Introduction
123I-metaiodobenzylguanidine
(123I-MIBG), a physiological analogue of noradrenaline,
is actively transported into noradrenaline granules at sympathetic
nerve terminals by a noradrenaline transporter and allows the
quantification of cardiac sympathetic innervation in
vivo(1). In Parkinson’s
disease (PD), neuronal damage in the areas associated with motor
functions, particularly the superordinate centers of the
somatomotor, visceromotor and limbic systems, has been reported
(2). In particular, structures
such as the dorsal motor nucleus of the vagal nerve and
intermediate reticular zone are involved in the early stages, while
the substantia nigra and other nuclear grays of the midbrain and
forebrain become the focus of initially slight, and then severe,
pathological changes in the late stages (2). These findings are consistent with
cardiac sympathetic denervation shown by means of myocardial
123I-MIBG scintigraphy, indicating an impairment of the
nigrostriatal dopaminergic and myocardial sympathetic systems in
the majority of the patients with PD, even in the earliest clinical
stage of the disease (3).
In total, 50% of PD patients complain of slowness of
movement at presentation (4). The
symptoms of PD involve the initiation and execution of movements,
particularly sequential and volitional actions (4). Approximately 40% of patients are
likely to complain of tremulousness of the hand at rest, which
improves with action and 80% of patients have an asymmetrical 3–5
Hz rest tremor evident on examination (5). The two subtypes of PD have different
courses, which are concordant with the differences in brain
biochemical abnormalities (5), and
it has been reported that PD progresses more rapidly in akinetic
rigid-type (ART) patients than in tremor dominant-type (TDT)
patients (6). Previous studies
suggested that 123I-MIBG cardiac uptake is increased in
PD patients with bradykinesia as compared with tremor patients
(7). Additionally, Spiegel et
al found that at all Hoen & Yahr (H&Y) stages,
myocardial MIBG uptake was significantly higher in TDT patients
than in ART patients (8).
In this study, 123I-MIBG myocardial
uptake was compared in patients with different subtypes of PD in
order to assess the correlation between the clinical phenotype and
sympathetic denervation. Moreover, the results concerning the PD
population were evaluated in comparison with those of a control
group (CG).
Materials and methods
Patients
The study involved 53 patients with PD [31 males and
22 females, mean age 62±10 years; 19 H&Y stage 1, 9 stage 1.5,
15 stage 2 and 10 at stage 3]. A clinical examination was conducted
by an experienced neurologist (P.S.) and PD was diagnosed using
United Kingdom Parkinson’s Disease Society Brain Bank (UKPDSBB)
criteria (9). The motor part of
the UKPDSBB criteria was used to assess the severity of disease
(10). On the basis of the
predominant motor features in UPDRS III motor examination section
score, patients were subtyped into one of two clinical groups, ART
and TDT, following the methods described in previous studies
(11–14). The Mini Mental State Examination
(MMSE) did not reveal any cognitive deficit. Nineteen patients had
TDT and 34 had ART. A ‘tremor score’ and a ‘non-tremor score’ were
calculated for each patient (11,15).
The data concerning the clinical subtypes of patients with PD are
shown in Table I. The tremor score
was derived from the sum of UPDRS items 20 (tremor at rest) and 21
(action or postural tremor of hands) divided by 7 (the number of
the single subitems included). The non-tremor score was derived
from the sum of UPDRS items 18 (speech), 19 (facial expression), 22
(rigidity), 27 (arising from the chair), 28 (posture), 29 (gait),
30 (postural stability) and 31 (body bradykinesia and hypokinesia)
divided by 12 (the number of the single subitems included). The
patient was classified as tremor-dominant type when the tremor
score was at least twice the non-tremor score. An age-matched
control group (CG) of 18 patients was recruited (8 males and 10
females, mean age 62.4±16.3 years). The CG patients underwent a
123I-MIBG scintigraphy for a suspected adrenal mass,
which was then revealed to be negative on image evaluation. Prior
to their inclusion in our study, the subjects were evaluated for
the absence of clinical signs of PD by an experienced neurologist
(A.S.). Exclusion criteria for the PD and CG patients included
diabetes, a history of neuropathy, previous relevant cardiac
disease or any other medical condition that potentially affected
the autonomic nervous system or the myocardial 123I-MIBG
uptake. None of the subjects were undergoing treatment with drugs
that have been previously reported to affect 123I-MIBG
uptake at the sympathetic terminals (15,16).
Informed consent was obtained in all cases from the patients
themselves or from their families, in accordance with the
Declaration of Helsinki. This study was approved by the ethics
committee of the University of Tor Vergata.
 | Table IGeneral overview of the PD population
examined. |
Table I
General overview of the PD population
examined.
| Population
(n=53) | TDT (n=19) | ART (n=34) |
|---|
| Gender |
| Males | 31 | 10 | 21 |
| Females | 22 | 9 | 13 |
| Disease duration
(months ± SD) | 50.7±60.6 | 66.1±68.2 | 41.4±54.7 |
| UPDRS III (mean ±
SD) | 23.3±11.1 | 18.2±6.6 | 26.3±12.3 |
| Hoehn & Yahr
score |
| 1 | 19 | 7 | 12 |
| 1.5 | 9 | 4 | 5 |
| 2 | 15 | 6 | 9 |
| 3 | 10 | 2 | 8 |
Data acquisition
Each PD patient was intravenously injected in 60 sec
with 111 MBq of 123I-MIBG (Amersham, Eindhoven, The
Netherlands) and 185–200 MBq was injected in CG patients in 5 min.
The radio-labeled compound was administered at the same time of the
day under the same experimental conditions in each patient.
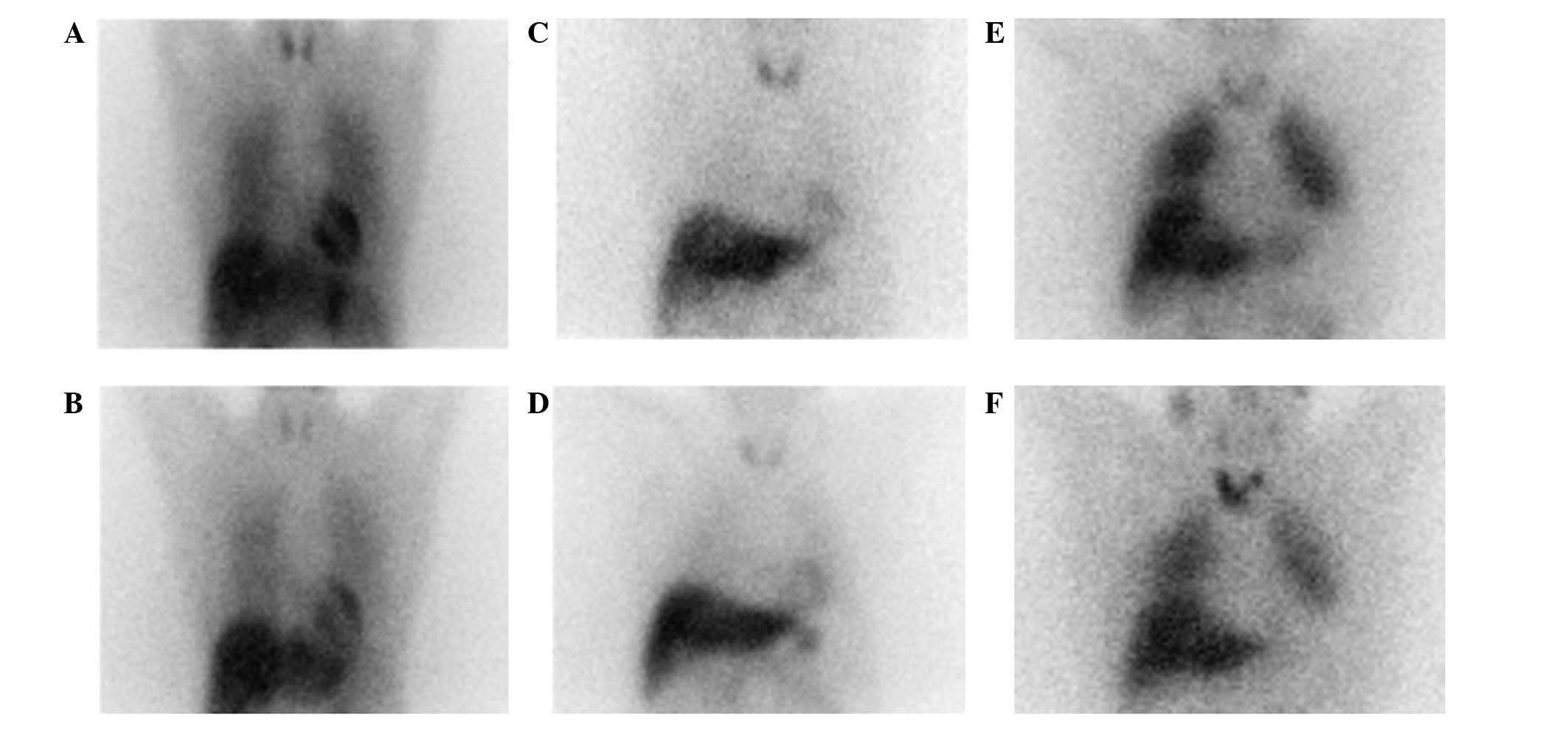
Data were collected by means of a dual head
gamma-camera (Millennium VG; General Electric Medical Systems,
Milwaukee, WI, USA) equipped with low-energy high-resolution
parallel-hole collimators with static planar images in a 128×128
matrix. Images were captured 30 min (early images) and 4 h (delayed
images) after the injection of the radio-labeled compound (Fig. 1). A region of interest (ROI) was
manually drawn over the myocardium, including the left ventricular
cavity. ROIs were then set over the upper mediastinum and a
heart-to-mediastinum (H/M) count-ratio was calculated, which was
defined as the average counts/pixel in the myocardium, divided by
that of the upper mediastinum (1).
Statistical analysis
The means and standard deviation were calculated for
age, UPDRS III score, H&Y grade, disease duration and the
results of the semi-quantitative analysis for the early and delayed
H/M count-ratio. To detect differences in the cardiac sympathetic
innervation between the subgroups (semi-quantitative analysis,
non-parametric data) a Mann-Whitney U test was used. Differences in
early and delayed H/M in the PD subgroups (ART and TDT) and CG
patients were analyzed by means of a Wilcoxon matched-pairs test.
The Spearman’s correlation was used to determine the relationship
among UPDRS motor scores, H&Y stage, age at examination and
early and delayed H/M count-ratio. Multiple regression analysis was
applied to observe the effect of disease duration. The Chi-square
test was used to assess differences in the H&Y stage and
disease phenotype. An unpaired t-test was used to assess
differences between age, disease duration, UPDRS and disease
phenotype. A hypothesis was considered valid when P≤0.05.
Results
Patient characteristics and analysis of
early and delayed H/M count-ratio
Differences in age, gender, disease duration and
H&Y stage between ART and TDT patients were not significant.
Patient characteristics are shown in Table I.
The results of the semi-quantitative analysis of the
early and delayed H/M count-ratio are shown in Table II. A reduced 123I-MIBG
myocardial uptake was detected in PD patients as compared to CG
patients in early (P=0.0026) and delayed images (P=0.0040). The H/M
ratio was lower in ART patients as compared to CG patients only in
early images (P=0.0017), while no statistically significant
differences were observed in delayed acquisitions (P=0.0691). A
lower H/M ratio was detected in TDT patients as compared to the CG
ones in both the early and delayed images (P=0.0016; P=0.0002). A
significant decrease in the H/M ratio was found between delayed
images as compared to that of the early images in TDT patients
(P=0.0040), CG patients (P=0.0175) and in the entire PD population
(P=0.0012), while no statistically significant differences were
found when comparing early and delayed H/M ratio in ART patients
(P=0.1043). No statistically significant differences were detected
when comparing early H/M count ratios in TDT and ART patients
(P=0.1727), while 123I-MIBG myocardial uptake was
significantly lower in delayed images in TDT (P=0.0167) compared to
ART patients (Fig. 2).
| Table IIEarly and delayed H/M ratio of the
123I-MIBG myocardial uptake in clinical PD subtypes and
the CG patients. |
Table II
Early and delayed H/M ratio of the
123I-MIBG myocardial uptake in clinical PD subtypes and
the CG patients.
| CG | PD | TDT | ART | Comparison | P-value |
|---|
| Early H/M | 1.97±0.28 | 1.68±0.36 | 1.59±0.34 | 1.72±0.36 | PD vs. CG | 0.0026 |
| | | | | TDT vs. CG | 0.0016 |
| | | | | ART vs. CG | 0.0017 |
| | | | | TDT vs. ART | 0.1727 |
| Delayed H/M | 1.88±0.27 | 1.58±0.36 | 1.43±0.38 | 1.66±0.33 | PD vs. CG | 0.0040 |
| | | | | TDT vs. CG | 0.0002 |
| | | | | ART vs. CG | 0.0691 |
| | | | | TDT vs. ART | 0.0167 |
Effects on UPDRS score
The UPDRS score was higher in ART patients as
compared with TDT patients (P=0.0192). The early and delayed H/M
ratio of PD patients was not associated with UPDRS (r=−0.1236,
P=0.4297; r=−0.0057, P=0.9708). Early and delayed
123I-MIBG myocardial uptake was not correlated with
UPDRS in ART (r=−0.3132, P=0.1117; r=−0.2128, P=0.2865) and TDT
patients (r=0.07985, P=0.7688; r=0.04546, P=0.8672). The H/M ratio
was not associated with H&Y stage in PD patients in early
(r=−0.2411, P=0.0821) or delayed (r=−0.1969, P=0.1577) scans.
123I-MIBG myocardial uptake was also not correlated with
the H&Y stage in the early (r=−0.1909, P=0.2794) and delayed
images (r=−0.1491, P=0.4002) in ART patients. No correlation was
found between H&Y stage and early (r=−0.4047, P=0.0856) and
delayed (r=−0.4352, P=0.0626) H/M ratios in TDT patients.
Correlation of 123I-MIBG
myocardial uptake and disease duration
123I-MIBG myocardial uptake was
significantly correlated with disease duration in early
(r2=0.1894, P=0.0028) and delayed images
(r2=0.1795, P=0.0037) in PD patients. The same
correlation was found with this parameter when considering the ART
population in early (r2=0.2651, P=0.0051) and delayed
images (r2=0.2193, P=0.0120). No significant
relationships were detected with disease duration in the TDT
population in either the early (r2=0.0916; P=0.2375) or
delayed (r2=0.0983; P=0.2204) image set.
Correlation of 123I-MIBG
myocardial uptake and age
No significant correlation was found when
considering 123I-MIBG myocardial uptake and age in PD
patients at examination in early (r=−0.1506, P=0.2817) and delayed
images (r=−0.2430, P=0.0796). The same results were obtained in the
CG in the early (r=−0.2687, P=0.2970) and delayed images
(r=−0.2221, P=0.3916). Considering the single subsets of the PD
population, no significant correlations were found with aging in
early (r=−0.1905, P=0.2806) and delayed (r=−0.2700, P=0.1225)
images and with the H/M ratio of ART patients and TDT patients in
early (r=0.0537, P=0.8272) and delayed images (r=−0.04178,
P=0.8652).
Discussion
One of the key findings of the present study was the
reduction of 123I-MIBG myocardial uptake in PD patients
as compared to the CG patients. This finding was more marked for
the delayed compared to the early images (Figs. 1 and 2), in agreement with several previous
studies (4,7,8,16–20).
The use of 123I-MIBG has been suggested as a useful
marker in the diagnosis of PD (19) and as a sensitive tool in the early
detection of silent autonomic dysfunction (18). Being an analogue of noradrenaline
(8), 123I-MIBG uptake
reflects presynaptic sympathetic integrity, while a reduced
myocardial uptake of this tracer is consistent with cardiac
sympathetic dysfunction or denervation (21). Nevertheless, Matsui et al
demonstrated that there were no significant correlations between
orthostatic hypotension or constipation and cardiac
123I-MIBG uptake, indicating that not all components of
the autonomic nervous system are uniformly affected in PD (19).
In the population of this study, a strong
contribution to the lower H/M count-ratio in PD patients as
compared with the CG was due to the TDT patients. When the single
ART population was analyzed, only the early, but not the delayed,
H/M ratio was lower than the CG.
In the comparison between TDT and ART, the TDT group
showed markedly reduced H/M values in the delayed images (Figs. 1 and 2). Moreover, TDT patients showed a
reduction of the H/M ratio in the delayed images as compared to the
early images, while no differences were found in the ART patients.
These latter findings are consistent with an increased wash-out of
123I-MIBG in the myocardium of TDT patients (18), and together with previously
mentioned results, indicate a more extensive involvement of the
cardiac sympathetic system (due to denervation, a reduced uptake by
storage vesicles, abnormalities in reuptake function, and increased
norepinephrine release or an increased catecholamine turnover) in
PD patients with the tremulous phenotype (22).
Previous studies have shown that in the early stage
of PD the dopaminergic system is more severely impaired in ART
compared to the other subgroups of patients, in particular when
compared to TDT (11,12). To the best of our knowledge, only a
few studies have evaluated the 123I-MIBG myocardial
uptake in different Parkinson’s phenotypes (7,8,20).
In their study, Spiegel et al found that myocardial
123I-MIBG uptake was significantly less impaired in TDT
patients than in ART patients at the same stage of the disease
(8). Similar results were
demonstrated by Saiki et al when comparing a tremor
phenotype population of PD with a phenotype characterized by
postural instability gait difficulty, which could correspond to the
ART phenotype (20). A significant
correlation was found when comparing the early and delayed H/M
ratio with the severity of hypokinesia and rigidity, a finding
showing that the H/M ratio was negatively associated with the
severity of these clinical features (8), whereas no correlations have been
found with the severity of the resting tremor (8). By contrast, Suzuki et al did
not find such a correlation in their population where
123I-MIBG myocardial uptake was correlated only with the
severity of bradykinesia but not with tremor or rigidity (7). In our study, 123I-MIBG
myocardial uptake was significantly lower in TDT patients when
compared to ART patients (P=0.0167), findings that are in contrast
with those of other studies (7,8,20).
These discrepancies may be due to the different disease duration in
these two subgroups. Even if differences in disease duration
between TDT and ART patients did not reach statistical
significance, TDT patients showed a longer disease duration than
ART, which potentially affected our results. However, while the H/M
ratio was significantly associated with disease duration in ART
patients, no such correlation was found in TDT patients, supporting
the hypothesis that a longer illness duration does not correlate
with a worsening of the sympathetic system in this last group.
Moreover, no difference was detected beween ART and TDT patients in
H&Y stage, with TDT patients scoring better than ART patients
in UPDRS III, reflecting a lower disability level in these patients
(9).
No significant correlations were found in either
early or delayed images with H&Y stage and UPDRS motor score in
PD patients. Additionally, no statistically significant
relationships were evident when comparing the single populations of
ART or TDT patients with these aspects of the disease. The lack of
a clear relationship of 123I-MIBG myocardial uptake with
disease severity detectable by means of UPDRS and H&Y stage has
been previously described (8,19).
In their study performed on a pool of 143 patients, Suzuki et
al hypothesized that 61.3% of the variation in the observed
early H/M ratio and 68.2% of that in the delayed H/M ratio could be
explained by their linear relationship with disease duration,
gender, H&Y stages and the clinical features of their
population (7). Nevertheless,
their data indicated no such correlation with clinical disease
severity of PD (H&Y stage) and 123I-MIBG myocardial
uptake (7). A comparison of both
early and delayed H/M ratios of PD patients with disease duration
yielded a lower H/M ratio in patients with a longer disease
duration. In our population, the mean disease duration was
50.7±60.6 months, which was lower as compared to that reported in
previously published studies in which the same relationship was
found and the disease duration was 86.4±73.2 months (18). This finding suggests that cardiac
sympathetic dysfunction occurs relatively early in PD and the
longer the disease duration, the lower the myocardial
123I-MIBG uptake and the more sympathetic degeneration
occurred. In their study, Kashihara et al found that
123I-MIBG myocardial uptake was lower in patients with a
long history of PD and the duration of the illness was inversely
correlated with the H/M ratio (18). Our data suggest that myocardial
sympathetic impairment detectable in PD remains with a worsening in
the disease course over time (23). However, such a correlation is
controversial (24). It has been
shown that disease duration was not significantly correlated with
either the early or delayed H/M ratio in a pool of 88 patients with
PD, while both age at examination and age at onset were negatively
correlated (17). Hamada et
al suggested that a later onset of the disease rather than the
length of disease duration may be associated with a lower
123I-MIBG uptake in PD. Our results are slightly
different from those of Hamada et al when considering
disease duration and the number of subjects examined, and it is
possible that a larger standard deviation in our data may play a
role in these discrepancies (17).
Of note, no significant differences were detected in
cardiac 123I-MIBG uptake in terms of aging in either CG
or PD patients. This observation is in agreement with a previous
study reporting a reduced 123I-MIBG uptake in the
inferior heart regions in older patients, but no significant
decrease in the whole myocardium with age (1).
In this study, the planar H/M values for
quantification in the CG (early 1.97±0.28, and delayed 1.88±0.27)
were similar to the values reported by Somsen et al and
Merlet et al in healthy volunteers (1,25).
Morozumi et al reported higher values of early and delayed
H/M ratios; 2.80±0.25 and 3.02±0.47, respectively (26). Differences in these measurements
have already been explained with the ROI size for the upper
mediastinum and the matrix size used (1). In particular, the small ROI used by
Morozumi et al for non-specific mediastinal uptake is less
affected by non-specific lung uptake leading to a lower mediastinal
count density and a larger variability with a larger SD for late
H/M (26). Notably, in the CG,
differences in the early and delayed H/M ratios were statistically
significant (Fig. 1). This finding
is in agreement with other studies that reported a decrease in H/M
ratio from early and delayed images in normal subjects (17,27,28).
Nevertheless, several studies reported a stability or an increase
in the H/M ratio over time (1,20,25).
A high interindividual and within-subject variability in
123I-MIBG uptake has been shown and may explain the
differences with the previously mentioned studies (1).
In conclusion, the results of the present study have
shown that the cardiac sympathetic system is more severely impaired
in TDT than in ART patients. Thus, in contrast to the other
movement symptoms of PD, tremor is caused by separate mechanisms
and is anatomically different from rigidity and bradykinesia
(29,30). Therefore, resting tremor is
comparatively less affected by dopamine than other motor symptoms,
and the evidence of lesser efficacy of dopaminergic therapy on PD
tremor than on other main symptoms emphasizes the contribution of
non-dopaminergic mechanisms (12).
The scintigraphic findings in TDT are possibly associated with a
greater autonomic impairment in these patients with
123I-MIBG molecular imaging being capable of improving
therapeutic planning. However, more studies on this subject are
required.
References
|
1
|
Somsen GA, Verberne HJ, Fleury E and
Righetti A: Normal values and within-subject variability of cardiac
I-123 MIBG scintigraphy in healthy individuals: Implications for
clinical studies. J Nucl Cardiol. 11:126–133. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Braak H, Ghebremedhin E, Rüb U, Bratzke H
and Del Tredici K: Stages in the development of Parkinson’s
disease-related pathology. Cell Tissue Res. 318:121–134. 2004.
|
|
3
|
Kline RC, Swanson DP, Wieland DM, et al:
Myocardial imaging in man with I-123 meta-iodobenzylguanidine. J
Nucl Med. 22:129–132. 1981.PubMed/NCBI
|
|
4
|
Spiegel J, Möllers MO, Jost WH, et al:
FP-CIT and MIBG scintigraphy in early Parkinson’s disease. Mov
Disord. 20:552–561. 2005.
|
|
5
|
Ahlskog JE: Diagnosis and differential
diagnosis of Parkinson’s disease and parkinsonism. Parkinsonism
Relat Disord. 7:63–70. 2000.
|
|
6
|
Quinn N: Parkinsonism-recognition and
differential diagnosis. Br Med J. 310:447–452. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Suzuki M, Urashima M, Oka H, Hashimoto M
and Taira K: Cardiac sympathetic denervation in
bradykinesia-dominant Parkinson’s disease. Neuroreport.
18:1867–1870. 2007.PubMed/NCBI
|
|
8
|
Spiegel J, Hellwig D, Farmakis G, et al:
Myocardial sympathetic degeneration correlates with clinical
phenotype of Parkinson’s disease. Mov Disord. 22:1004–1008.
2007.PubMed/NCBI
|
|
9
|
Hughes A, Daniel SE, Kilford L and Lees
AJ: Accuracy of clinical diagnosis of idiopatic Parkinson’s
disease: a clinico-pathological study of 100 cases. J Neurol
Neurosurg Psychiatry. 55:181–184. 1992.
|
|
10
|
Fahn S and Elton RL; members of the UPDRS
Development Committee. Unified Parkinson’s disease rating scale.
Macmillan Healthcare Information; Florhan Park HJ: 1987
|
|
11
|
Spiegel J, Hellwing D, Samnick S, et al:
Striatal FP-CIT uptake differs in the subtypes of early Parkinson’s
disease. J Neural Transm. 114:331–335. 2007.PubMed/NCBI
|
|
12
|
Schillaci O, Chiaravalloti A, Pierantozzi
M, et al: Different patterns of nigrostriatal degeneration in
tremor type versus the akinetic-rigid and mixed types of
Parkinson’s disease at the early stages: molecular imaging with
123I-FP-CIT SPECT. Int J Mol Med. 28:881–886. 2011.PubMed/NCBI
|
|
13
|
Lewis SJG, Foltynie T, Blackwell AD,
Robbins TW, Owen AM and Barker RA: Heterogeneity of Parkinson’s
disease in the early clinical stages using a data driven approach.
J Neurol Neurosurg Psychiatry. 76:343–348. 1995.
|
|
14
|
Kang GA, Bronstein JM, Masterman DL, et
al: Clinical characteristics in early Parkinson’s disease in a
central California population-based study. Mov Disord.
20:1133–1142. 1995.
|
|
15
|
Solanki KK, Bomanji J, Moyes J, Mather SJ,
Trainer PJ and Britton KE: A pharmacological guide to medicines
which interfere with the biodistribution of radiolabelled
meta-iodobenzylguanidine (MIBG). Nucl Med Commun. 14:513–521. 1992.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Courbon F, Brefel-Courbon C, Thalamas C,
et al: Cardiac MIBG scintigraphy is a sensitive tool for detecting
cardiac sympathetic denervation in Parkinson’s disease. Mov Disord.
18:890–897. 2003.
|
|
17
|
Hamada K, Hirayama M, Watanabe H, et al:
Onset age and severity of motor impairment are associated with
reduction of myocardial 123I-MIBG uptake in Parkinson’s disease. J
Neurol Neurosurg Psychiatry. 74:423–426. 2003.PubMed/NCBI
|
|
18
|
Kashihara K, Ohno M, Kawada S and Okumura
Y: Reduced cardiac uptake and enhanced washout of 123I-MIBG in pure
autonomic failure occurs conjointly with Parkinson’s disease and
dementia with lewy bodies. J Nucl Med. 47:1099–1101.
2006.PubMed/NCBI
|
|
19
|
Matsui H, Nishinaka K, Oda M, Komatsu K,
Kubori T and Udaka F: Does cardiac metaiodobenzylguanidine (MIBG)
uptake in Parkinson’s disease correlate with major autonomic
symptoms? Parkinsonism Relat Disord. 12:284–288. 2006.
|
|
20
|
Saiki S, Hirose G, Sakai K, et al: Cardiac
123I-MIBG scintigraphy can assess the disease severity and
phenotype of PD. J Neurol Sci. 220:105–111. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Hakusui S, Yasuda T, Yanagi T, et al: A
radiological analysis of heart sympathetic functions with
meta-[123I]iodobenzylguanidine in neurological patients with
autonomic failure. J Auton Nerv Syst. 49:81–84. 1994.PubMed/NCBI
|
|
22
|
Pace L, Betocchi S, Losi MA, et al:
Sympathetic nervous function in patients with hypertrophic
cardiomyopathy assessed by [123I]-MIBG: relationship with left
ventricular perfusion and function. Q J Nucl Med Mol Imaging.
48:20–25. 2004.
|
|
23
|
Sawada H, Hoeda T, Yamamoto K, et al:
Diagnostc accuracy of cardiac metaiodobenzylguanidine scintigraphy
in Parkinson disease. Eur J Neurol. 16:174–182. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Blin J, Dubois B, Bonnet AM, Vidailhet M,
Brandabur M and Agid Y: Does ageing aggravate parkinsonian
disability? J Neurol Neurosurg Psychiatry. 54:780–782. 1991.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Merlet P, Benvenuti C, Moyse D, et al:
Prognostic value of MIBG imaging in idiopathic dilated
cardiomyopathy. J Nucl Med. 40:917–923. 1999.PubMed/NCBI
|
|
26
|
Morozumi T, Kusuoka H, Fukuchi K, et al:
Myocardial iodine- 123-metaiodobenzylguanidine images and autonomic
nerve activity in normal subjects. J Nucl Med. 38:49–52.
1997.PubMed/NCBI
|
|
27
|
Kobayashi S, Tateno M, Morii H, Utsumi K
and Saito T: Decreased cardiac MIBG uptake, its correlation with
clinical symptoms in dementia with Lewy bodies. Psychiatry Res.
174:76–80. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Yoshita M, Taki J, Yokoyama K, et al:
Value of 123I-MIBG radioactivity in the differential diagnosis of
DLB from AD. Neurology. 66:1850–1854. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Carr J: Tremor in Parkinson’s disease.
Parkinsonism Relat Disord. 8:223–234. 2002.
|
|
30
|
Rivlin-Etzion M, Marmor O, Heimer G, Raz
A, Nini A and Bergman H: Basal ganglia oscillations and
pathophysiology of movement disorders. Curr Opin Neurobiol.
16:629–637. 2006. View Article : Google Scholar : PubMed/NCBI
|