Introduction
Pneumonia is an inflammatory condition of the lung
that involves lung parenchyma. Community-acquired pneumonia (CAP)
is one of several diseases that results in lung infections in
individuals who have not recently been hospitalized. CAP may be
caused by bacterial, viral, fungal or parasitic agents with the
additional complication of upper respiratory tract infections
(1,2). Furthermore, CAP is the most
frequently occurring infectious disease worldwide, with high
morbidity and mortality rates (3).
Timely diagnosis and optimized antibiotic treatment are critical
for reducing CAP morbidity and mortality. Early diagnosis and
recognition of the severity of CAP is required for early treatment
in order to increase the survival rate of CAP patients (4).
Growth arrest-specific protein 6 (Gas6) is a vitamin
K-dependent protein, which was initially described as a protein
expressed during growth arrest. Gas6 is also crucial for
phagocytosis of apoptotic cells (5–7). Axl
is the receptor tyrosine kinase (RTK) for Gas6 and belongs to a
subfamily of RTKs (8). Axl is
present in the endothelium and is capable of being cleaved and
released into circulation; it is crucial for endothelial activation
during inflammation. The soluble form of Axl (sAxl), which is
present in plasma, binds Gas6 and inhibits Axl-mediated cell
signaling. Numerous studies have demonstrated that the Gas6-Axl
system is capable of regulating cell survival, proliferation,
migration, adhesion and phagocytosis (5–8).
Gheita et al (8) indicated
that plasma concentrations of sAxl correlate positively with
systemic lupus erythematosus (SLE) and Behçet’s disease. Ekman
et al reported that Gas6 and sAxl correlate with numerous
inflammatory markers, suggesting a role in systemic inflammation,
including SLE and critical limb ischemia (CLI) diseases (5,6).
Therefore, the inflammation severity and survival rate of these
diseases may be indirectly predicted by sAxl levels, which may be
useful markers for inflammation severity. However, the correlation
between sAxl and pneumonia has not been examined. Therefore, the
plasma sAxl concentrations of CAP patients prior to and following
treatment with antibiotics and the normal controls were compared.
In addition, it was determined whether the severity correlated with
the expression of sAxl or was associated with CAP
susceptibility.
Materials and methods
Participants and diagnosis
This study was performed on a group of 121
individuals, comprised of 61 CAP patients and 60 healthy controls,
between February, 2009 and December, 2009. Venous blood samples
from CAP patients were obtained through routine venipuncture at
Chung Shan Medical University Hospital (Taichung, Taiwan), prior to
and following treatment with antibiotics. This study was approved
by the Chung Shan Medical University Hospital Institutional Review
Board and each patient provided informed consent. The demographic
characteristics, comorbidities, symptoms and signs of pneumonia,
laboratory results and previous antibiotic treatment of each
patient were recorded once they had been admitted. The diagnostic
criteria for CAP were based on the guidelines of the Infectious
Diseases Society of America/American Thoracic Society (9). The guidelines for CAP diagnosis
included a typical infiltration change on chest X-ray films within
one day of symptom occurrence and at least one clinical
manifestation, including a cough, thick yellow sputum, or a high
fever (>37.8°C); or at least two minor criteria, including
tachypnea, dyspnea, pleural pain, chest pain, confusion or
disorientation, lung consolidation, or white blood cell (WBC)
counts of >12000 cells/ml. Exclusion criteria included
outpatient status; transfer from another hospital or hospital
admission within the previous three weeks; other acute conditions,
including pulmonary edema, pulmonary embolism, or malignancy
appearing during follow-up; pneumonia caused by tuberculosis or
malignancy; severe immunocompromisation, including severe
neutropenia (WBC count <1.0×109 cells/l); organ or
bone marrow transplant and human immunodeficiency virus infection.
Pneumonia severity was assessed using the pneumonia severity index
(PSI) (10), acute physiology and
chronic health evaluation II (APACHE II) (11) and CURB-65 (12) tests.
Participants and blood specimen
collection
In total, 61 CAP patients and 60 healthy
individuals, to serve as a control group, were recruited. All CAP
patients were treated with empirical antimicrobial agents. Blood
samples were obtained from all CAP patients in order to test the
WBC, neutrophil cell count, C-reactive protein (CRP) concentration,
and plasma concentration of sAxl prior to and following treatment
with antibiotics. Blood samples for the control group were also
obtained and analyzed. The blood samples were placed in tubes
containing EDTA and were immediately centrifuged (3,000 × g, 10
min) and stored at −80°C. Depending on the severity of their
conditions, CAP patients were treated with effective and common
antibiotics, including cefuroxime, ceftizoxime, and clarithromycin.
Table I provides a summary of the
clinical data and demographics of the patients and controls.
 | Table ILaboratory data of controls and
patients with community-acquired pneumonia (CAP) prior to and
following treatmenta. |
Table I
Laboratory data of controls and
patients with community-acquired pneumonia (CAP) prior to and
following treatmenta.
| Clinical
variables | Controls (n=60) | Pre-treatment
(n=61) | Post-treatment
(n=61) | P-value UT/Cb | P-value UT/Tc |
|---|
|
|
|
|---|
| Median (range) | Median (range) | Median (range) |
|---|
| Age (years) | 59.38±11.45 | 59.52±20.46 | 0.963 | | |
| Gender |
| Male | 36 (60%) | 37 (60.7%) | 0.941 | | |
| Female | 24 (40%) | 24 (39.3%) | | | |
| CRP (mg/dl) | 0.30 (0.02–1.65) | 8.63
(0.69–27.40) | 0.94
(0.30–11.30) | 0.001 | 0.001 |
| WBC
(/mm3) | 5860
(3110–10190) | 10890
(3560–32480) | 8450
(3460–22340) | 0.001 | 0.001 |
| Neutrophils
(/mm3) | 3530 (1738–6046) | 8673
(1032–29686) | 5484
(1518–21155) | 0.001 | 0.001 |
| PSI score | | 79.03±38.91e | | | |
| CURB-65 scored | | 0.88 ± 0.85e | | | |
| APACHE II score | | 9.22 ± 5.57e | | | |
Measurement of WBCs, neutrophils and CRP
concentrations
Staff members who were unaware of the source of the
samples (blinded to the study) measured WBCs, neutrophils and CRP
concentrations by enzyme immunoassays in a clinical laboratory.
Measurement of plasma sAxl level by
enzyme-linked immunosorbent assay (ELISA)
ELISA was used to measure the plasma concentrations
of sAxl in all blood samples (Aviscera Bioscience, Santa Clara, CA,
USA). For each plasma sample, 100 μl was directly transferred to
the microtest strip wells of the ELISA plate and subsequently
incubated for 2 h at room temperature. Following four washing steps
to remove unbound protein, the detection antibody (anti-sAxl;
Aviscera Bioscience, Santa Clara, CA, USA) was added and the
reaction system was incubated for 2 h at room temperature. Antibody
binding (anti-sAxl) was detected with streptavidin-conjugated
horseradish peroxidase and developed with a substrate solution. The
reaction was stopped and the optical density was determined using a
microplate reader (Molecular Devices, Sunnyvale, CA, USA) set at
450 nm. sAxl concentrations were quantitated with a calibration
curve using a human sAxl standard. Each plasma sample was assayed
according to the manufacturer’s instructions, and the values were
within the linear portion of the standard curve.
Statistical analysis
Statistical analyses were performed using SPSS 15.0
statistical software (SPSS Inc., Chicago, IL, USA). All continuous
variables were expressed as the mean ± standard deviation. In order
to compare the untreated patients and the healthy controls, the
statistical differences between the demographic and clinical data
were analyzed using the Mann–Whitney U test for continuous
variables not following a parametric distribution. The Wilcoxon
signed-rank test was used to compare untreated and treated patients
for categorical variables. Linear regression analysis was used to
examine the correlation between the sAxl of all clinical and
laboratory variables of CAP patients. P<0.05 was considered to
indicate a statistically significant difference in the two-tailed
test.
Results
Demographic and clinical
characteristics
Table I provides a
summary of the demographic and clinical characteristics. The
analysis was based on a sample of 121 individuals; the age and
percentage of male participants did not differ significantly
between the CAP patients and the control group. The blood cell
counts of WBCs and neutrophils and CRP levels were significantly
elevated in patients with CAP prior to treatment, compared with the
healthy controls (P<0.001; Table
I) and patients with CAP following treatment (P<0.001;
Table I).
ELISA analysis
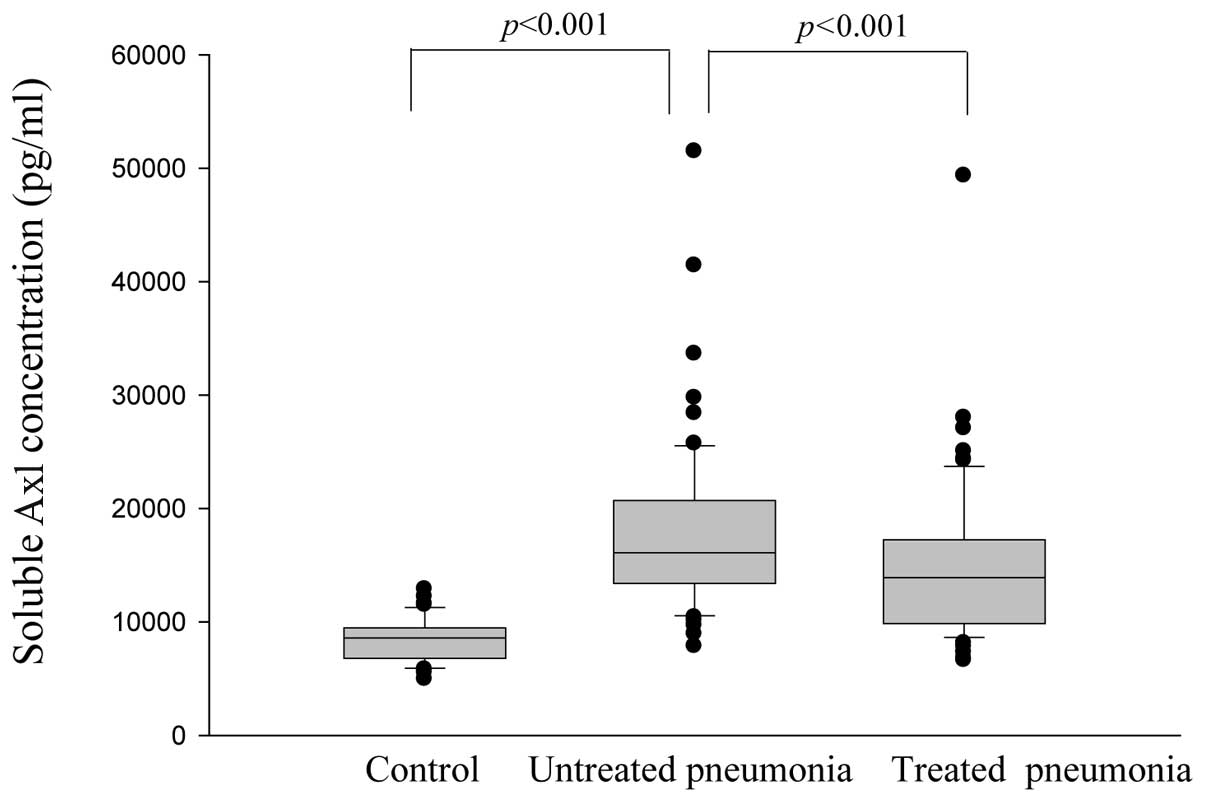
Fig. 1 demonstrates
the plasma-soluble Axl concentration levels (pg/ml) of 61 CAP
patients and 60 control participants obtained using ELISA analysis.
The plasma-soluble Axl concentration level was significantly
elevated in CAP patients prior to treatment (18,143.2±7,551.5
pg/ml) compared with the controls (8,328±1,909.4 pg/ml)
(P<0.001), and decreased significantly following treatment
(14,799.9±6,762.8 pg/ml) (P<0.001).
Correlation between plasma-soluble Axl
expression and WBC and neutrophil counts, and C-reactive protein
levels
No significant correlations were observed with
plasma-soluble Axl concentrations (Fig. 2). Fig.
3 reveals correlations among PSI, CURB-65, APACHE II scores,
and plasma-soluble Axl concentrations in CAP patients prior to
treatment. Significant correlations were observed between
plasma-soluble Axl concentrations and PSI (Spearman correlation
coefficients: r=0.350, P=0.006, n=61; Fig. 3A), CURB-65 (Spearman correlation
coefficients: r=0.640, P=0.028, n=61; Fig. 3B), and APACHE II (Spearman
correlation coefficients: r=0.313, P=0.014, n=61; Fig. 3C).
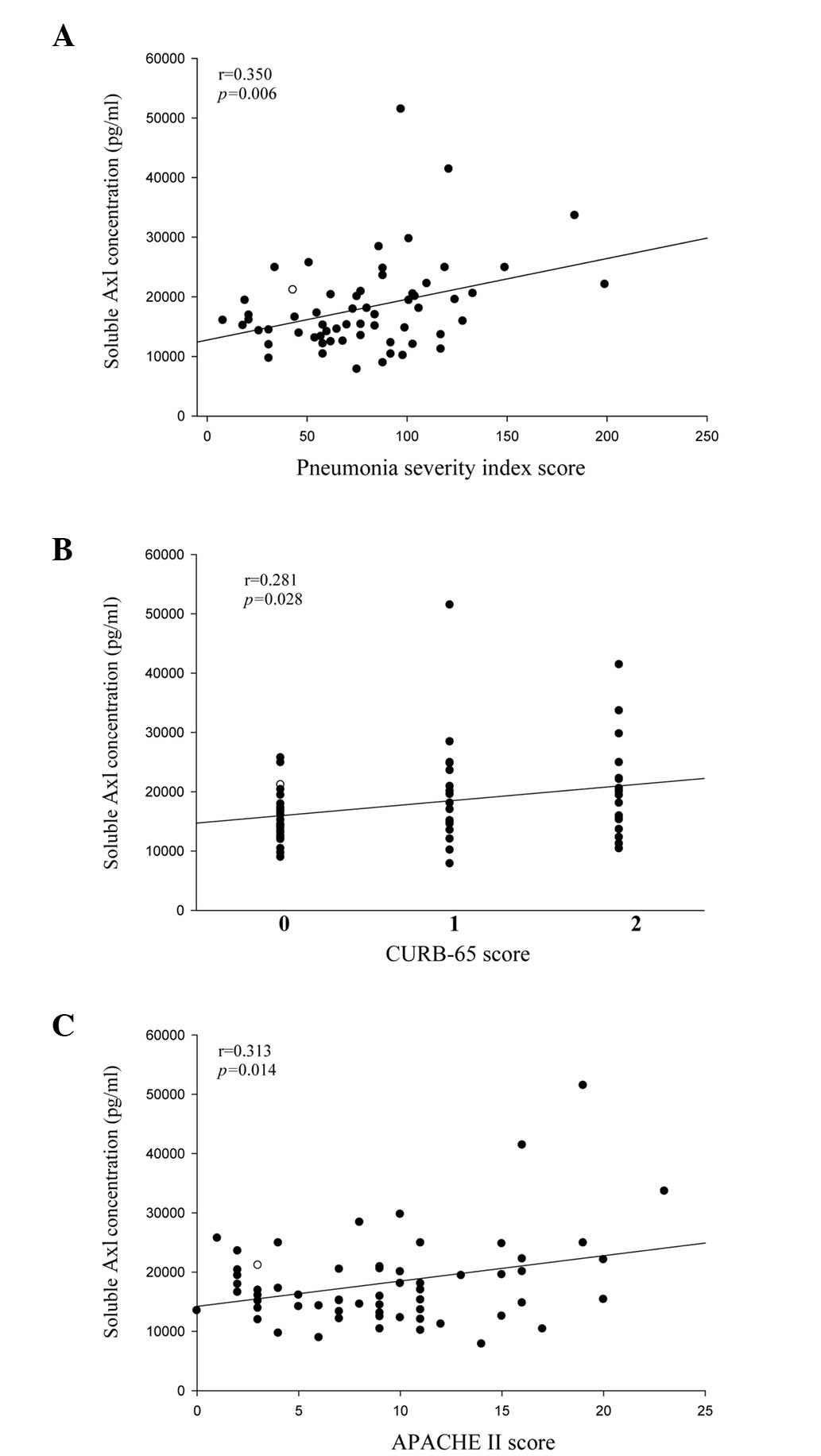 | Figure 3Correlations were observed among the
pneumonia severity index (PSI), CURB-65, acute physiology and
chronic health evaluation II (APACHE II) scores and plasma-soluble
Axl concentrations in community-acquired pneumonia (CAP) patients
prior to treatment. Significant correlations were observed between
plasma-soluble Axl concentrations and (A) PSI; Spearman correlation
coefficients: r=0.350, P=0.006, n=61, (B) CURB-65; Spearman
correlation coefficients: r=0.640, P=0.028, n=61, and (C) APACHE
II; Spearman correlation coefficients: r=0.313, P=0.014, n=61. |
Discussion
Axl (also known as UFO or Ark) is a 140-kD protein,
originally identified in human patients with chronic myelogenous
leukemia (13). Axl is a member of
the TAM family of receptor RTKs, consisting of Tyro3 (Sky), Axl,
and Mer (13–16). Axl is stimulated by Gas6 (product
of the growth arrest-specific gene 6) that was originally observed
as a protein expressed by growth-arrested fibroblasts (7,17).
The soluble form of Axl (sAxl) may be found in circulation. The Axl
receptor is expressed in a wide range of tissues and cell lines
(18). Overexpression of the Axl
receptor occurs in several human cancer types (16) and is crucial for the growth of
human gliomas (19) and gastric
cancer (20). Furthermore, several
studies have focused on the correlation between sAxl concentrations
and inflammation. Ekman et al indicated that sAxl correlates
with a number of inflammatory diseases, including SLE and CLI
(5,6). In addition, Ekman et al
(6) indicated that the sAxl
ligands and sAxl concentrations correlate with numerous
inflammatory markers in systemic inflammation response syndromes
and sepsis. Therefore, the number of studies on the correlation
between sAxl and inflammatory diseases (except pneumonia) have
increased.
In CAP patients, the correlation among sAxl
concentrations, number of WBCs, neutrophils, and CRP levels with
regard to severity remains unclear. Therefore, this study examined
the changes in the plasma concentration of sAxl, the number of WBCs
and neutrophils, and CRP levels in CAP patients. The results
revealed that the number of WBCs and neutrophils, and the levels of
CRP and sAxl decreased considerably following treatment with
antibiotics. However, the number of WBCs, neutrophils and levels of
CRP did not correlate with the sAxl levels in CAP patients prior to
treatment with antibiotics. This result is similar to that obtained
by Lee et al (21), which
demonstrated that CRP was not associated with the ligands of sAxl
in patients with chronic renal failure. However, Ekman et al
(22) indicated that the
concentrations of Gas6 and sAxl correlated with CRP in SLE patients
with varying degrees of disease activity. Therefore, the
correlation between the levels of sAxl and CRP may be controversial
in various disease types and various diseases have differing
correlations of sAxl and CRP levels. A greater number of samples
and experiments are required in order to verify this concept in
future studies.
The correlations between plasma sAxl levels and PSI,
CURB-65, APACHE II scores in CAP patients remain unclear. These
scoring systems are crucial in order to predict the mortality rate
of CAP patients as it represents the severity of the disease.
Therefore, the plasma sAxl concentrations of CAP patients were
further examined prior to treatment with antibiotics in order to
determine whether CAP severities correlated with the PSI, CURB-65
and APACHE II scores. The results demonstrated that significant
correlations of plasma sAxl concentrations with PSI, CURB-65 and
APACHE II score severity, were observed in CAP patients. However,
the number of WBCs and neutrophils, and the levels of CRP did not
correlate with the severity of CAP patients. Therefore, altered
plasma sAxl levels are a trend in inflammation severity and
endothelial dysfunction, and plasma sAxl levels may be used as a
diagnostic and prognostic serologic marker for CAP instead of the
number of WBCs, neutrophils and levels of CRP. This result is
similar to that obtained by Ekman et al (5), in which sAxl concentrations
correlated positively with the concentrations of known inflammatory
markers and predicted future mortality rates in CLI. To the best of
our knowledge, this is the first study on the correlation of CAP
severity with the expression of sAxl.
In conclusion, this study examined the correlation
between the plasma concentrations of sAxl and CAP. The results
provided valuable information with regard to the plasma
concentrations of sAxl in the assessment of CAP severity and
demonstrated that the sAxl concentration correlated significantly
with antibiotic treatment.
References
|
1
|
Kumar V, Abbas AK, Fausto N, et al:
Pathologic Basis of Disease. 8th ed. Elsevier Saunders;
Philadelphia, PA: pp. 710–711. 2009
|
|
2
|
Chiang TY, Shyu LY, Tsao TC, et al:
Elevated plasma matrix metalloproteinase-9 protein and its gene
polymorphism in patients with community-acquired pneumonia. Clin
Chem Lab Med. 50:449–454. 2011.PubMed/NCBI
|
|
3
|
Lee YT, Chen SC, Shyu LY, et al:
Significant elevation of plasma cathepsin B and cystatin C in
patients with community-acquired pneumonia. Clin Chim Acta.
413:630–635. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Houck PM, Bratzler DW, Nsa W, Ma A and
Bartlett JG: Timing of antibiotic administration and outcomes for
Medicare patients hospitalized with community-acquired pneumonia.
Arch Intern Med. 164:637–644. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ekman C, Gottsäter A, Lindblad B and
Dahlbäck B: Plasma concentrations of Gas6 and soluble Axl correlate
with disease and predict mortality in patients with critical limb
ischemia. Clin Biochem. 43:873–876. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ekman C, Linder A, Akesson P and Dahlbäck
B: Plasma concentrations of Gas6 (growth arrest specific protein 6)
and its soluble tyrosine kinase receptor sAxl in sepsis and
systemic inflammatory response syndromes. Crit Care. 14:R1582010.
View Article : Google Scholar
|
|
7
|
Hafizi S and Dahlbäck B: Gas6 and protein
S. Vitamin K-dependent ligands for the Axl receptor tyrosine kinase
subfamily. FEBS J. 273:5231–5244. 2006.PubMed/NCBI
|
|
8
|
Gheita TA, Bassyouni IH and Bassyouni RH:
Plasma concentrations of growth arrest specific protein 6 and the
soluble form of its tyrosine kinase receptor Axl in patients with
Systemic lupus erythematosus and Behçets disease. J Clin Immunol.
32:1279–1286. 2012.
|
|
9
|
Mandell LA, Wunderink RG, Anzueto A, et
al: Infectious Diseases Society of America/American Thoracic
Society consensus guidelines on the management ofcommunity-acquired
pneumonia in adults. Clin Infect Dis. 44:S27–S72. 2007. View Article : Google Scholar
|
|
10
|
Fine MJ, Auble TE, Yealy DM, et al: A
prediction rule to identify low-risk patients with
community-acquired pneumonia. N Engl J Med. 336:243–250. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Knaus WA, Draper EA, Wagner DP, et al:
APACHE II: a severity of disease classification system. Crit Care
Med. 13:818–829. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lim WS, van der Eerden MM, Laing R, et al:
Defining community acquired pneumonia severity on presentation to
hospital: an international derivation and validation study. Thorax.
58:377–382. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Melaragno MG, Wuthrich DA, Poppa V, et al:
Increased expression of Axl tyrosine kinase after vascular injury
and regulation by G protein-coupled receptor agonists in rats. Circ
Res. 83:697–704. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ekman C, Site DF, Gottsäter A, Lindblad B
and Dahlbäck B: Plasma concentrations of growth arrest specific
protein 6 and the soluble form of its tyrosine kinase receptor Axl
as markers of large abdominal aortic aneurysms. Clin Biochem.
43:110–114. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Robinson DR, Wu YM and Lin SF: The protein
tyrosine kinase family of the human genome. Oncogene. 19:5548–5557.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Linger RM, Keating AK, Earp HS and Graham
DK: TAM receptor tyrosine kinases: biologic functions, signaling,
and potential therapeutic targeting in human cancer. Adv Cancer
Res. 100:35–83. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Manfioletti G, Brancolini C, Avanzi G and
Schneider C: The protein encoded by a growth arrest-specific gene
(gas6) is a new member of the vitamin K dependent proteins related
to protein S, a negative coregulator in the blood coagulation
cascade. Mol Cell Biol. 13:4976–4985. 1993.
|
|
18
|
O’Bryan JP, Frye RA, Cogswell PC, et al:
Axl, a transforming gene isolated from primary human myeloid
leukemia cells, encodes a novel receptor tyrosine kinase. Mol Cell
Biol. 11:5016–5031. 1991.PubMed/NCBI
|
|
19
|
Vajkoczy P, Knyazev P, Kunkel A, et al:
Dominant-negative inhibition of the Axl receptor tyrosine kinase
suppresses brain tumor cell growth and invasion and prolongs
survival. Proc Natl Acad Sci USA. 103:5799–5804. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Sawabu T, Seno H, Kawashima T, et al:
Growth arrest-specific gene 6 and Axl signaling enhances gastric
cancer cell survival via Akt pathway. Mol Carcinog. 46:155–164.
2007. View
Article : Google Scholar : PubMed/NCBI
|
|
21
|
Lee IJ, Hilliard B, Swami A, et al: Growth
arrest-specific gene 6 (Gas6) levels are elevated in patients with
chronic renal failure. Nephrol Dial Transplant. 27:4166–4172. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ekman C, Jönsen A, Sturfelt G, Bengtsson
AA and Dahlbäck B: Plasma concentrations of Gas6 and sAxl correlate
with disease activity in systemic lupus erythematosus. Rheumatology
(Oxford). 50:1064–1069. 2011. View Article : Google Scholar : PubMed/NCBI
|