Introduction
In recent years, cervical cancer has become the
third most common female cancer and in 2008 there were ~529,000 new
cases worldwide (1). Cervical
squamous cell carcinoma (CSCC) is the most common pathological type
of cervical cancer followed by cervical adenocarcinoma and
adenosquamous carcinoma (2). The
association between human papillomavirus (HPV) infection and the
occurrence of cervical cancer has been verified by numerous studies
(3,4). HPV types 16, 18, 58, 33, 52, 45, 31
and 35 are the most common types in cervical cancer patients from
Asia (5). However, the prognostic
value of HPV in cervical cancer remains controversial. Certain
studies have demonstrated an association between HPV 18-related
cervical cancer and a poor prognosis (6,7).
However, in previous studies, HPV-positive cervical cancer patients
demonstrated a more favorable prognosis than HPV-negative patients
(8,9). Whereas certain authors were unable to
find any significance between HPV types and their prognosis
(10). Thus, the aim of the
present study was to identify potent molecular markers associated
with the prognosis of CSCC.
Growth-regulated oncogene-1 (GRO-1) is a member of
the CXC chemokine family which contains an ELR motif (Glu-Leu-Arg)
at the NH2 terminal and is important in angiogenesis (11). Overexpression of the GRO gene was
initially identified in transformed Chinese hamster cells (12). An elevated expression of GRO-1 was
detected in numerous malignancies (13,14).
Hepatocyte growth factor (HGF) was first identified as a type of
mitogen extracted from hepatectomized rats in 1984 (15). The HGF/c-Met signaling pathway
composed of HGF and its functional receptor c-Met promotes
tumorigenesis, progression and tumor cell invasion (16). Platelet-derived growth factor-AA
(PDGF-AA) is a member of the PDGF family which can promote the
production of angiogenic factors, resulting in tumor angiogenesis
(17). E-selectin is a member of
the selectin family which is a family of cellular adhesion
molecules contributing to cell-cell adhesion and is associated with
tumor progression and metastasis. Soluble E-selectin (sE-selectin)
can be used as a biomarker in the serum to detect and monitor the
occurrence and development of cancer (18).
The roles of serum levels of GRO-1, HGF, PDGF-AA and
sE-selectin as biomarkers have not yet been elucidated compared
with the important roles of high-risk HPV in CSCC. Studies on these
four factors in cervical cancer are rare. The aim of the present
study was to analyze the clinical significance and prognostic value
of these four factors and high-risk HPV infection in CSCC.
Materials and methods
Patients
A total of 292 females with CSCC, 43 females with
cervical intraepithelial neoplasia (CIN) and 91 healthy age-matched
females were recruited for physical examination from the Jiangsu
Cancer Hospital (Nanjing, China) between February 2010 and March
2013. In total, 292 cases with CSCC were histopathologically
confirmed as CSCC for the first time and did not undergo any
treatment prior to collecting the specimens. All the CSCC patients
were staged on the basis of the latest International Federation of
Gynecology and Obstetrics (FIGO) staging. The characteristics of
all the cases are shown in Table
I.
 | Table ICharacteristics of all the cases. |
Table I
Characteristics of all the cases.
| Patients with | |
|---|
|
| |
|---|
| Characteristic | CSCC n (%) | CIN n (%) | Healthy controls n
(%) |
|---|
| Age, median
(range) | 48 (27–84) | 45 (29–61) | 43 (33–72) |
| FIGO Stage or CIN
classification |
| I | 40 (13.70) | 12 (29.91) | |
| II | 108 (36.99) | 18 (41.86) | |
| III | 115 (39.38) | 13 (30.23) | |
| IV | 29 (9.93) | | |
| Metastasis |
| Positive | 29 (9.93) | | |
| Negative | 263 (90.07) | | |
| Grading |
| 1 | 43 (14.73) | | |
| 2 | 147 (50.34) | | |
| 3 | 102 (34.93) | | |
| Pelvic nodal
status |
| Positive | 150 (51.37) | | |
| Negative | 142 (48.63) | | |
| Tumor size |
| >4 cm | 144 (49.32) | | |
| ≤4 cm | 148 (50.68) | | |
| Total number | 292 (100) | 43 (100) | 91 (100) |
Collection of the specimens
Fasting blood (3 ml) specimens were obtained from
335 patients and 91 healthy females. The blood specimens were
immediately transferred into the test tubes and then centrifuged at
1,000 × g for 10 min and the serum was extracted. The serum samples
were stored at −80°C until detection.
A routine gynecological examination was performed on
292 females with CSCC and 43 females with CIN. The cervical
secretions were washed using sterile physiological cotton balls and
then cervical scrapings were collected from the squamous cell
junction of the cervical canal using cotton swabs. Subsequently,
they were placed in sterile glass tubes and stored at −20°C until
use.
The present study was approved by the Ethics
Committee of Jiangsu Cancer Hospital and written informed consent
was obtained from all the participants in accordance with the
ethical standards laid down in the 1964 Declaration of Helsinki and
its later amendments.
Luminex xMAP technology
Serum levels of GRO-1, HGF, PDGF-AA and sE-selectin
were quantified using Luminex xMAP technology. The Human
Cytokine/Chemokine kit (cat no. MPXHCYTO60KPMX42) was used for the
detection of GRO-1 and PDGF-AA, and Human Circulating Cancer
Biomarker Magnetic Bead Panel 1 (cat no. HCCBP1MAG-58K) was used
for the detection of HGF. Levels of sE-selectin were determined
with Human Cardiovascular Disease (CVD) Panel 1 (cat no.
HCVD1-67AK). All the kits were supplied by Millipore (Billerica,
MA, USA) while the FLEXMAP 3D™ system was purchased from Luminex
Corporation (Austin, TX, USA).
The main experimental steps were as follows (in
strict accordance with the manufacturer’s instructions): Firstly,
standard and quality controls were prepared in accordance with the
manufacturer’s instructions, then 25 μl serum and 25 μl beads
(Millipore) were added to the plate, following being incubated for
agitation overnight at 4°C. Subsequently, 25 μl of rabbit anti-rat
monoclonal antibodies were added into each well followed by
incubation for 1 h at 20–25°C. Streptavidin-phycoerythrin (25 μl)
was added to the well and the plate followed by incubation for 30
min at 20–25°C. Following being washed twice, 100 μl of sheath
fluid (Millipore) was added to every well. Finally, the median
fluorescence intensity data was analyzed on the Luminex analyzer
(FLEXMAP 3D™ system; Luminex Corporation) and the final
concentrations of the four factors were calculated using the
weighted 5-parameter logistic method.
DNA extraction and quantitative
polymerase chain reaction (qPCR)
The steps for DNA extraction of cervical scrapings
were as follows: Firstly, the cervical scrapings were mixed with
1.5 ml sterile saline in a glass tube, then all the liquid was
transferred into a 1.5 ml microcentrifuge tube to be centrifuged at
12,000 × g for 10 min. The supernatant was removed and the
precipitate was digested using proteinase K (Omega Bio-Tek Inc.,
Norcross, GA, USA). Finally, DNA was extracted using chloroform. A
Real quality RQ-HPV HR kit (AB ANALITICA, Padova, Italy) was used
to identify and quantify the HPV DNA type (16, 18/45, 31 and
33/52/58/67) on the ABI 7300 Real-Time PCR system (Applied
Biosystems, Foster City, CA, USA) and β-globin served as the
internal control. qPCR was conducted in a 20 μl volume containing
10 μl AB Real Time mix (AB ANALITICA), 0.4 μl primer mix, 0.8 μl
probe mix, 6.8 μl H2O and 2 μl DNA. The PCR program
comprised 40 cycles of 2 min at 50°C, 3 min at 95°C, 15 sec at 94°C
and 40 sec at 57°C. When the quantitative value of HPV was ≥100
gene copies, the result was positive for this type of HPV,
otherwise the result was negative. All the experiments were
repeated three times.
Statistical analysis
The concentrations of GRO-1, HGF, PDGF-AA and
sE-selectin were not normally distributed, thus the Mann-Whitney U
test and Kruskal-Wallis test were used in the present study, while
the χ2 test was used to compare the positive rate of HPV
between the groups. The correlations between the biomarkers were
analyzed using Spearman’s rank correlation coefficient. The areas
under the receiver operating characteristic curves (AUROC) were
used to evaluate the diagnostic accuracy. Youden’s index [Youden’s
index = sensitivity + specificity) −1] is an indicator of
authenticity of diagnostic tests and the optimal cut-off values
were calculated when the Youden index was maximum. Overall survival
time (OS) was calculated from the day of diagnosis to mortality due
to cervical cancer or the latest follow-up, while progression-free
survival (PFS) was calculated from the day of diagnosis to the
initial disease progression or mortality from cervical cancer or
the latest follow-up. The Kaplan-Meier survival curves and the
log-rank test were used to compare the differences between groups.
Multivariate Cox regression analysis was used to screen out the
independent prognostic variables. The median (25–75 percentiles)
was used to describe the measurement data and P<0.05 was
considered to indicate a statistically significant difference. All
the above statistical analyses was performed using SPSS version
21.0 (IBM, Armonk, NY, USA).
Results
Concentrations of GRO-1, HGF, PDGF-AA and
sE-selectin in CSCC patients, CIN patients and the healthy
controls
The serum levels of GRO-1, HGF and sE-selectin in
patients with CSCC significantly increased compared with the CIN
patients and the healthy controls [GRO-1: 748.43 (501.49–1088.23
pg/ml) vs. 620.07 (386.60–846.58 pg/ml) and 564.91 (376.34–899.03
pg/ml), P<0.0001; HGF: 724.35 (501.68–1049.35 pg/ml) vs. 555.68
(409.21–711.13 pg/ml) and 476.27 (356.36–834.40 pg/ml),
P<0.0001; sE-selectin: 22176.68 (13767.43–34829.97 pg/ml) vs.
17214.00 (10854.60–25306.98 pg/ml) and 18276.34 (9028.38–26154.20
pg/ml), P<0.0001] and no significant difference was identified
between the CIN patients and the healthy controls (P>0.05). No
statistical difference was identified in the serum levels of
PDGF-AA among the three groups [13311.48 (8952.06–19040.87 pg/ml)
vs. 12220.30 (7623.88–18438.83 pg/ml) and 11224.32
(8756.27–17643.22 pg/ml), P=0.21] (Fig. 1).
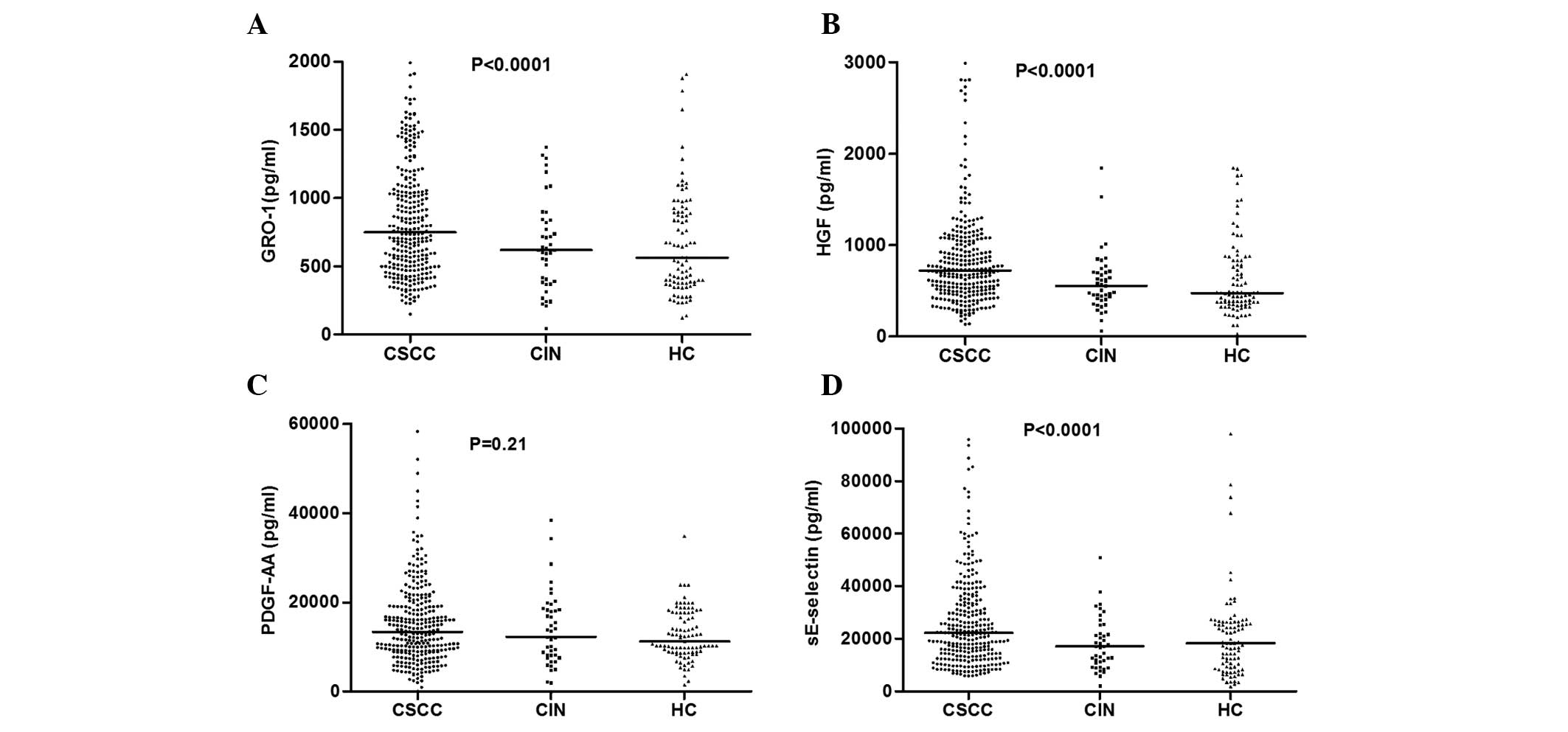 | Figure 1Concentrations of GRO-1, HGF, PDGF-AA
and sE-selectin in CSCC patients, CIN patients and HCs. Each point
represents an individual and the horizontal lines show the median
values. (A)-Concentration of GRO-1 in the three groups.
(B)-Concentration of HGF in the three groups. (C)-Concentration of
PDGF-AA in the three groups. (D)-Concentration of sE-selectin in
the three groups. CSCC, cervical squamous cell carcinoma; CIN,
cervical intraepithelial neoplasia; HC, healthy controls; GRO-1,
growth-regulated oncogene-1; HGF, hepatocyte growth factor;
PDGF-AA, platelet-derived growth factor-AA; sE-selectin, soluble
E-selectin. |
Positive rate of HPV types between the
CSCC patients and the CIN patients
HPV infection was identified in 205 out of 292
(70.21%) of the CSCC patients as well as 22 out of 43 (51.16%) of
the CIN patients. A significant difference was found between the
two groups (χ2=6.22, P=0.013). Table II shows the distribution of the
HPV types in the HPV-positive patients. It was revealed that HPV 16
was the most common genotype in the CSCC patients (50.24%) and the
CIN patients (45.45%) infected with HPV 16 only. In addition, HPV
16 was the most common genotype in the CSCC patients (66.34%) and
the CIN patients (59.09%) in the overall prevalence (Table II).
| Table IIPrevalence of HPV types in the
HPV-positive patients. |
Table II
Prevalence of HPV types in the
HPV-positive patients.
| HPV type | CSCC patients n
(%) | CIN patients n
(%) |
|---|
| 16 | 103 (50.24) | 10 (45.45) |
| 18/45 | 17 (8.29) | 5 (22.73) |
| 31 | 11 (5.37) | 0 (0.00) |
| 33/52/58/67 | 35 (17.07) | 4 (18.18) |
| 16, 18/45 | 4 (1.95) | 0 (0.00) |
| 16, 31 | 4 (1.95) | 0 (0.00) |
| 16,
33/52/58/67 | 25 (12.20) | 3 (13.64) |
| 18/45,
33/52/58/67 | 4 (1.95) | 0 (0.00) |
| 31,
33/52/58/67 | 2 (0.98) | 0 (0.00) |
| Total infection
number | 205 (100) | 22 (100) |
Association between HPV infection and
clinicopathological characteristics in CSCC patients
As demonstrated in Table III, HPV infection was not
associated with age, FIGO stage, metastasis, grading, pelvic lymph
node metastasis or tumor size of the CSCC patients (P>0.05).
| Table IIIAssociation between HPV and
clinicopathological characteristics in 292 cervical squamous cell
carcinoma patients. |
Table III
Association between HPV and
clinicopathological characteristics in 292 cervical squamous cell
carcinoma patients.
| Characteristic | Patients (n) | HPV positive n
(%) | HPV negative n
(%) | χ2 | P-value |
|---|
| Age (years) |
| ≤45 | 175 | 121 (69.14) | 54 (30.86) | 0.236 | 0.627 |
| >45 | 117 | 84 (71.79) | 33 (28.21) | | |
| FIGO stage |
| I+II | 148 | 99 (66.89) | 49 (33.11) | 1.575 | 0.209 |
| III+IV | 144 | 106 (73.61) | 38 (26.39) | | |
| Metastasis |
| Positive | 29 | 20 (68.97) | 9 (31.03) | 0.024 | 0.878 |
| Negative | 263 | 185 (70.34) | 78 (29.66) | | |
| Grading |
| 1 | 43 | 29 (67.44) | 14 (32.56) | 0.249 | 0.883 |
| 2 | 147 | 103 (70.07) | 44 (29.93) | | |
| 3 | 102 | 73 (71.57) | 29 (28.43) | | |
| Pelvic lymph
node |
| Positive | 150 | 105 (70.00) | 45 (30.00) | 0.006 | 0.937 |
| Negative | 142 | 100 (70.42) | 42 (29.58) | | |
| Tumor size |
| >4 cm | 144 | 99 (68.75) | 45 (31.25) | 0.288 | 0.592 |
| ≤4 cm | 148 | 106 (71.62) | 42 (28.38) | | |
Association between serum levels of
GRO-1, HGF, PDGF-AA and sE-selectin with clinicopathological
variables and HPV infection in CSCC patients
The serum levels of GRO-1 were closely associated
with FIGO stage (P=0.001), metastasis (P<0.0001), pathological
grading (P<0.0001) and pelvic lymph node metastasis (P=0.003).
The serum levels of HGF were significantly correlated with FIGO
stage (P=0.02), pathological grading (P<0.0001), pelvic lymph
node metastasis (P<0.0001), tumor size (P<0.0001) and HPV
infection (P=0.039). The concentrations of PDGF-AA in the serum
were associated with FIGO stage (P=0.004), pathological grading
(P=0.021) and pelvic lymph node metastasis (P<0.0001), and the
concentrations of sE-selectin were correlated with age
(P<0.0001), FIGO stage (P<0.0001) and tumor size (P=0.001)
(Table IV).
| Table IVAssociation between the
concentrations of GRO-1, HGF, PDGF-AA and sE-selectin with
clinicopathological variables and HPV infection in CSCC
patients. |
Table IV
Association between the
concentrations of GRO-1, HGF, PDGF-AA and sE-selectin with
clinicopathological variables and HPV infection in CSCC
patients.
| GRO-1 (pg/ml) | HGF (pg/ml) | PDGF-AA
(pg/ml) | sE-selectin
(pg/ml) |
|---|
|
|
|
|
|
|---|
| Variable | Median (Q1–Q3) | P-value | Median (Q1–Q3) | P-value | Median (Q1–Q3) | P-value | Median (Q1–Q3) | P-value |
|---|
| Age (years) |
| ≤45 | 706.15 | 0.405 | 703.61 | 0.673 | 12232 | 0.507 | 25100.07 | <0.0001 |
|
(498.34–1064.77) | |
(491.28–1050.43) | |
(8924.25–18981.15) | |
(16334.44–39911.36) | |
| >45 | 797.84 | | 730.04 | | 14546.64 | | 17570.96 | |
|
(511.44–1101.05) | |
(533.35–1055.83) | |
(8975.73–20086.15) | |
(10854.60–26670.43) | |
| FIGO stage |
| I+II | 681.68 | 0.001 | 684.94 | 0.02 | 11836.83 | 0.004 | 18567.66 | <0.0001 |
|
(487.51–997.52) | |
(463.36–906.66) | |
(7667.91–17829.22) | |
(12063.41–27413.10) | |
| III+IV | 854.89 | | 745.29 | | 15079.25 | | 25514.91 | |
|
(512.11–1377.29) | |
(541.90–1106.87) | |
(9654.05–21567.82) | |
(16552.68–41161.57) | |
| Metastasis |
| Negative | 725.37 | <0.0001 | 718.67 | 0.53 | 13666.55 | 0.473 | 21492.66 | 0.051 |
|
(498.34–1032.68) | |
(497.93–1046.13) | |
(9071.68–19012.58) | |
(13322.53–33429.15) | |
| Positive | 1454.65 | | 745.29 | | 10304.72 | | 29365.53 | |
|
(673.72–1813.78) | |
(514.75–1187.60) | |
(7024.07–23145.85) | |
(17768.34–42434.70) | |
| Grading |
| 1 | 684.23 | <0.0001 | 548.78 | <0.0001 | 12730.83 | 0.021 | 19027.79 | 0.815 |
|
(486.09–1015.88) | |
(386.06–671.97) | |
(7640.13–16155.14) | |
(14464.74–29145.96) | |
| 2 | 680.07 | | 651.76 | | 12621.99 | | 21882.43 | |
|
(471.20–1021.78) | |
(474.78–883.24) | |
(8755.05–18273.21) | |
(13322.53–36253.62) | |
| 3 | 932.37 | | 954.13 | | 15745.92 | | 23168.46 | |
|
(639.76–1280.61) | |
(743.85–1163.76) | |
(9749.88–22532.62) | |
(14012.20–35245.75) | |
| Pelvic lymph
node |
| Positive | 854.06 | 0.003 | 867.08 | <0.0001 | 16083.24 | <0.0001 | 22472.31 | 0.528 |
|
(539.70–1177.40) | |
(556.12–1149.30) | |
(9376.87–21631.17) | |
(14012.20–37642.05) | |
| Negative | 673.11 | | 609.31 | | 11382.93 | | 21492.66 | |
|
(455.37–1020.08) | |
(424.11–801.47) | |
(7905.86–15881.62) | |
(13483.41–32109.79) | |
| Tumor size |
| >4 cm | 797.41 | 0.115 | 881.21 | <0.0001 | 13486.61 | 0.79 | 25100.07 | 0.001 |
|
(507.29–1202.84) | |
(574.39–1208.60) | |
(8770.29–20453.72) | |
(15987.78–39849.31) | |
| ≤4 cm | 703.19 | | 646.29 | | 13104.19 | | 19585.97 | |
|
(496.78–1029.21) | |
(427.27–829.08) | |
(9086.33–18808.46) | |
(12373.51–29530.70) | |
| HPV type |
| Positive | 756.01 | 0.454 | 739.56 | 0.039 | 13407.86 | 0.883 | 22472.31 | 0.595 |
|
(491.82–1060.47) | |
(523.15–1080.69) | |
(9046.62–18981.15) | |
(14382.01–35777.81) | |
| Negative | 737.38 | | 649.94 | | 12999.18 | | 21882.43 | |
|
(557.53–1203.25) | |
(464.98–907.68) | |
(8816.01–21652.84) | |
(12529.74–33429.15) | |
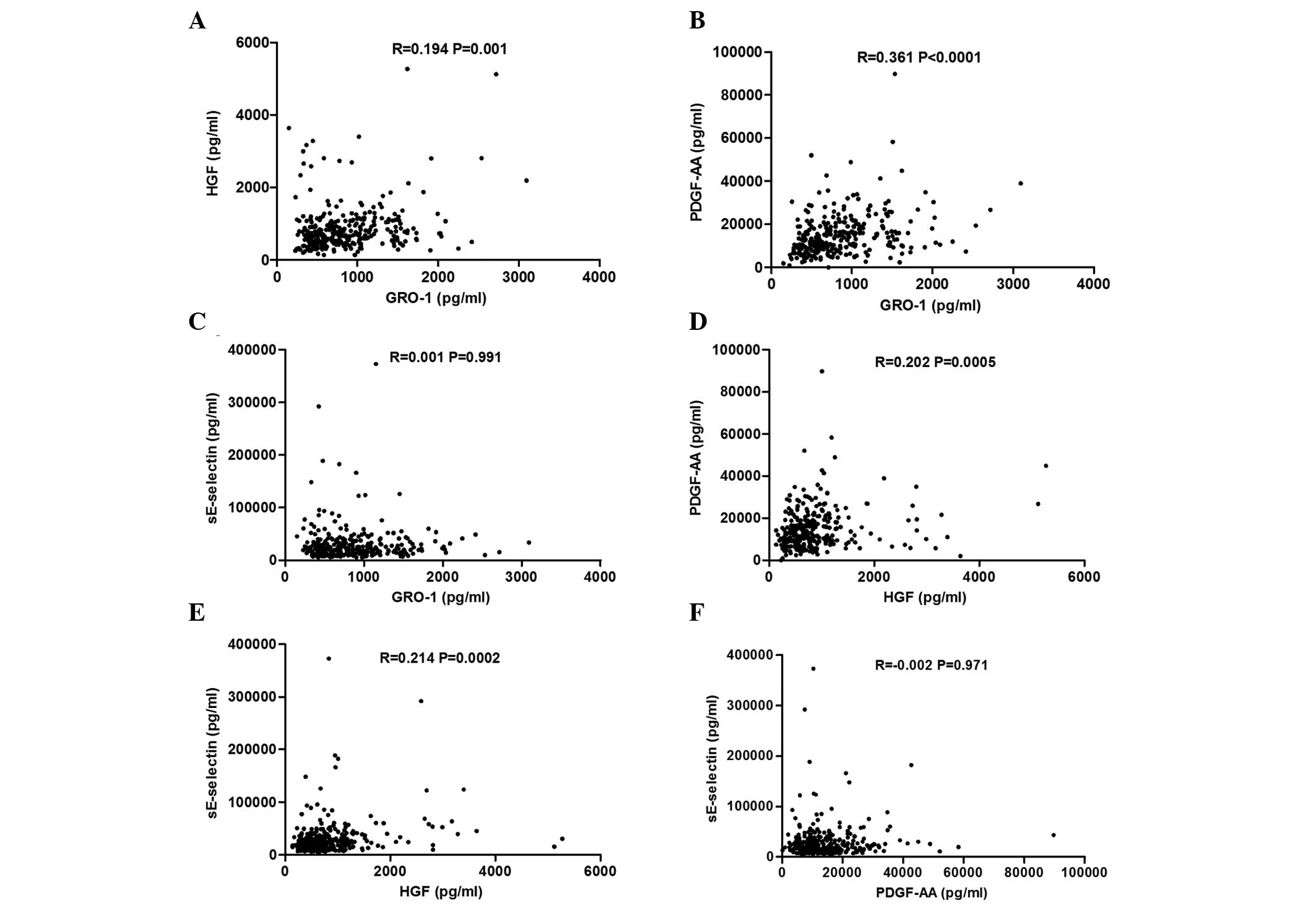
Correlations between GRO-1, HGF, PDGF-AA
and sE-selectin in patients with CSCC
Fig. 2 shows that
there were several positive correlations of the serum levels of HGF
with the other three factors: Serum levels of HGF correlated with
GRO-1 (R=0.194, P=0.001), PDGF-AA (R=0.202, P=0.0005) and
sE-selectin (R=0.214, P=0.0002). The concentration of PDGF-AA was
correlated with GRO-1 (R=0.361, P<0.0001), while no association
of sE-selectin with GRO-1 (R=0.001, P=0.991) and PDGF-AA (R=−0.002,
P=0.971) was identified.
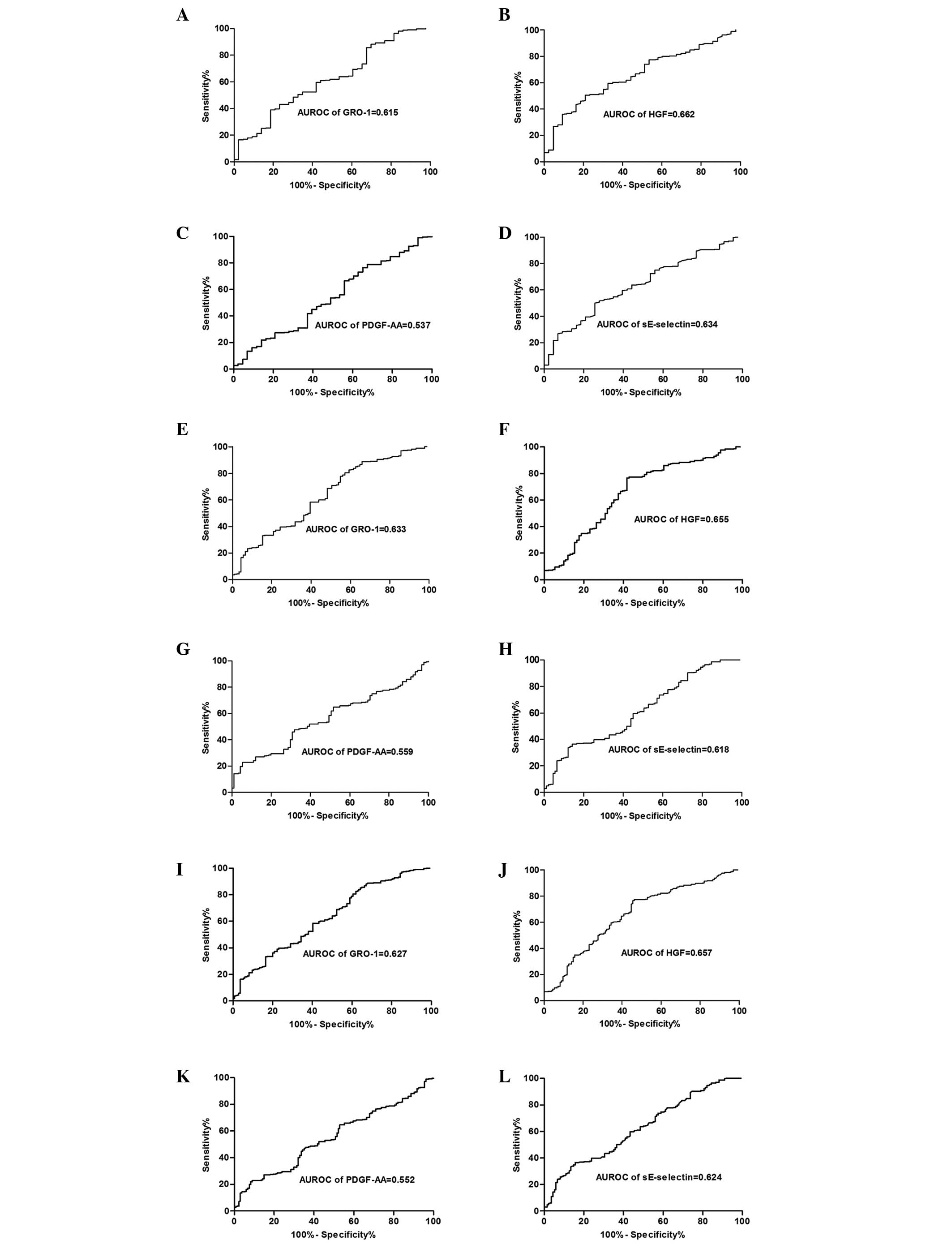
Diagnostic value of serum levels of
GRO-1, HGF, PDGF-AA and sE-selectin in the CSCC patients
AUROC of GRO-1, HGF, PDGF-AA and sE-selectin for
discriminating the CSCC patients from the CIN patients were 0.615
(95% CI: 0.525–0.705), 0.662 (95% CI: 0.583–0.741), 0.537 (95% CI:
0.442–0.631) and 0.634 (95% CI: 0.551–0.718), respectively, while
the AUROC of HGF for discriminating the CSCC patients from the
healthy controls was 0.655 (95% CI: 0.586–0.723) compared with
0.633 (95% CI: 0.566–0.700) for GRO-1, 0.559 (95% CI: 0.497–0.622)
for PDGF-AA and 0.618 (95% CI: 0.552–0.684) for sE-selectin. In
addition, the AUROC of GRO-1, HGF, PDGF-AA and sE-selectin for
discriminating the CSCC patients from the CIN patients and the
healthy controls were 0.627 (95% CI: 0.570–0.684), 0.657 (95% CI:
0.600–0.714), 0.552 (95% CI: 0.495–0.609) and 0.624 (95% CI:
0.567–0.680), respectively (Fig.
3). The results demonstrated that serum levels of HGF obtained
the highest diagnostic value compared with the other three factors.
Table V shows the sensitivity and
specificity of the optimal cut-off values.
| Table VSensitivity and specificity of the
optimal cut-off values in different screening groups. |
Table V
Sensitivity and specificity of the
optimal cut-off values in different screening groups.
| Group | GRO-1 | HGF | PDGF-AA | sE-selectin |
|---|
| CSCC vs CIN |
| Cut-off point
(pg/ml) | 902.27 | 717.72 | 8287.73 | 22176.68 |
| Sensitivity
(%) | 39.04 | 50.68 | 78.77 | 50.00 |
| Specificity
(%) | 81.40 | 79.07 | 32.56 | 74.42 |
| CSCC vs healthy
controls |
| Cut-off point
(pg/ml) | 466.89 | 494.00 | 19898.33 | 27399.83 |
| Sensitivity
(%) | 80.48 | 76.71 | 22.95 | 36.64 |
| Specificity
(%) | 42.86 | 58.24 | 94.51 | 85.71 |
| CSCC vs CIN and
healthy controls |
| Cut-off point
(pg/ml) | 407.58 | 494.00 | 19898.33 | 27399.83 |
| Sensitivity
(%) | 88.01 | 76.71 | 22.95 | 36.64 |
| Specificity
(%) | 32.84 | 54.48 | 91.04 | 84.33 |
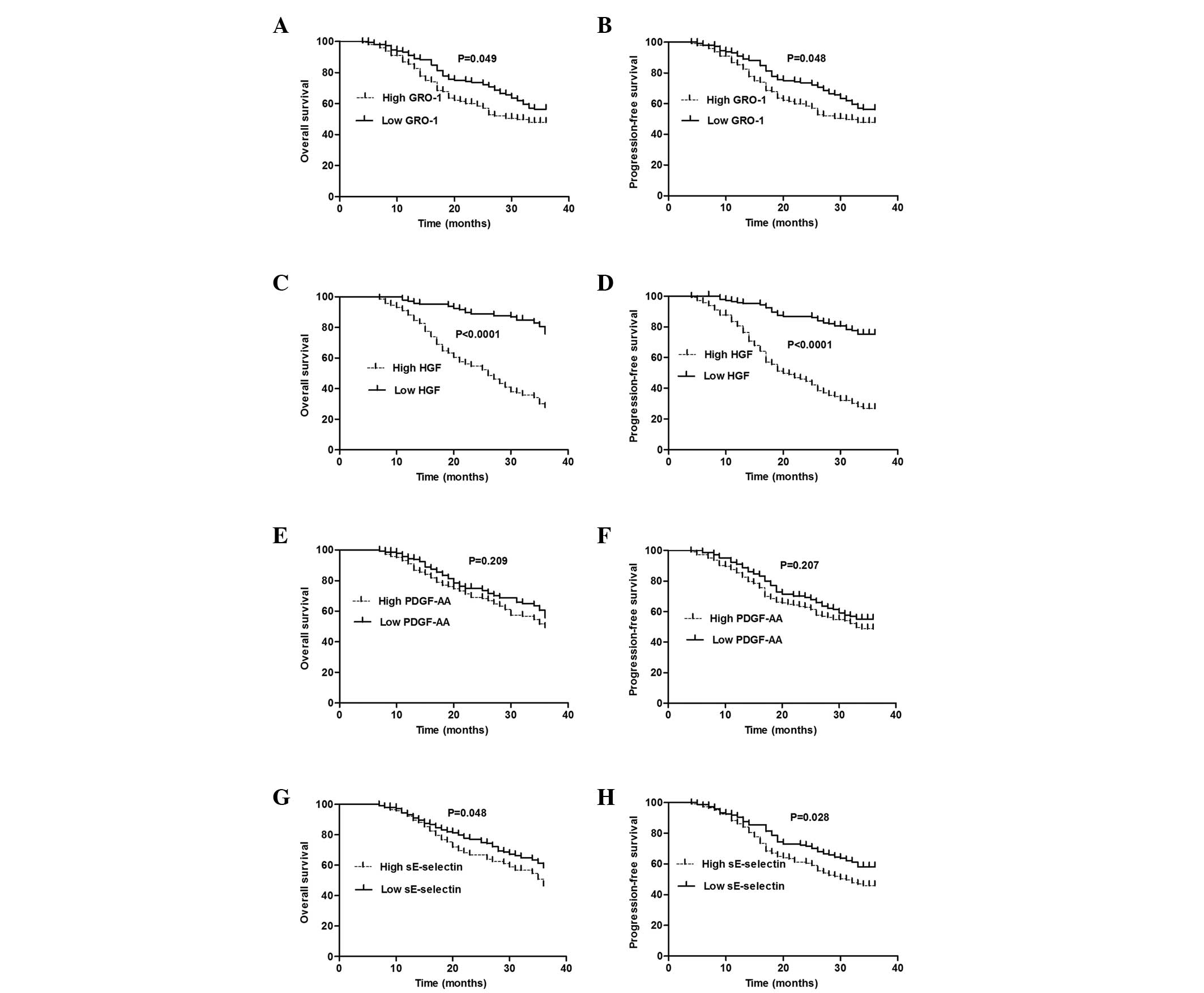
Prognostic value of GRO-1, HGF, PDGF-AA,
sE-selectin and HPV in CSCC patients
The median values of GRO-1, HGF, PDGF-AA and
sE-selectin were used as the cut-off points. The log-rank analysis
demonstrated that patients with a low expression of GRO-1
(<748.43 pg/ml) had significantly longer OS and PFS than those
with a high expression of GRO-1 (>748.43 pg/ml; OS, P=0.049;
PFS, P=0.048), and that patients with a high expression of HGF
(>724.35 pg/ml) had significantly shorter OS and PFS than those
with a low expression of HGF (<724.35 pg/ml; OS, P<0.0001;
PFS, P<0.0001). The analysis also indicated significant
differences in OS and PFS between patients with a high
(>22176.68 pg/ml) and low expression (<22176.68 pg/ml) of
sE-selectin (OS, P=0.048; PFS, P=0.028). However, no differences in
OS and PFS between patients with a high (>13311.48 pg/ml) and
low expression (<13311.48 pg/ml) of PDGF-AA (OS, P=0.209; PFS,
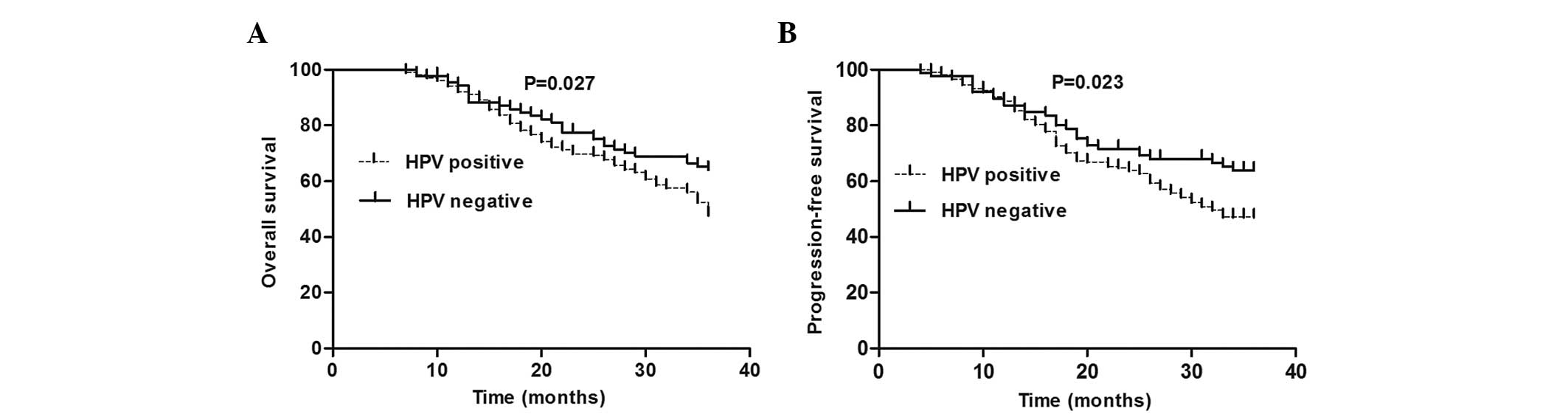
P=0.207) were identified (Fig. 4).
Furthermore, HPV-positive patients had shorter OS and PFS compared
with the HPV-negative patients (OS, P=0.027; PFS, P=0.023)
(Fig. 5). Table VI indicated that only the
expression of HGF in the serum (P<0.0001), FIGO stage
(P<0.0001) and pelvic lymph node metastasis (P=0.001) were
independent prognostic factors in CSCC patients, while high-risk
HPV infection did not show any statistical significance in the
multivariate Cox analysis.
| Table VIMultivariate Cox regression in
cervical squamous cell carcinoma patients. |
Table VI
Multivariate Cox regression in
cervical squamous cell carcinoma patients.
| OS | PFS |
|---|
|
|
|
|---|
| Risk factor | P-value | HR | 95% CI | P-value | HR | 95% CI |
|---|
| Age: >45 vs ≤45
years | 0.277 | 1.235 | 0.844–1.808 | 0.237 | 1.258 | 0.860–1.840 |
| FIGO stage: III+IV
vs I+II | <0.0001 | 2.616 | 1.727–3.961 | <0.0001 | 2.540 | 1.683–3.835 |
| Metastasis:
Positive vs negative | 0.911 | 0.967 | 0.534–1.752 | 0.985 | 0.994 | 0.548–1.804 |
| Grading: 3 vs
1+2 | 0.316 | 0.816 | 0.549–1.214 | 0.293 | 0.808 | 0.544–1.202 |
| Pelvic nodal
status: Positive vs negative | 0.001 | 1.950 | 1.320–2.881 | 0.001 | 1.982 | 1.342–2.927 |
| Tumor size: >4
cm vs ≤4 cm | 0.676 | 0.923 | 0.633–1.345 | 0.668 | 0.921 | 0.631–1.343 |
| GRO-1 (pg/ml): High
vs low levels | 0.554 | 1.117 | 0.774–1.614 | 0.627 | 1.095 | 0.759–1.579 |
| HGF (pg/ml): High
vs low levels | <0.0001 | 5.640 | 3.596–8.846 | <0.0001 | 5.279 | 3.368–8.276 |
| PDGF-AA (pg/ml):
High vs low levels | 0.187 | 0.776 | 0.533–1.130 | 0.206 | 0.785 | 0.540–1.142 |
| sE-selectin
(pg/ml): High vs low levels | 0.695 | 0.929 | 0.643–1.342 | 0.977 | 0.995 | 0.690–1.433 |
| HPV: Positive vs
negative | 0.301 | 1.251 | 0.819–1.910 | 0.260 | 1.276 | 0.835–1.948 |
Discussion
GRO-1, also termed CXCL1, has been extensively
investigated in cancer in recent years (11–14).
It is highly expressed in numerous types of carcinomas, including
oropharyngeal cancer (19),
colorectal cancer (13) and
gastric cancer (14). Ogata et
al (13) demonstrated that the
expression of GRO-1 is associated with tumor size, staging, lymph
node metastasis and invasion depth in colorectal cancer using
immunohistochemistry. Jung et al (14) detected the serum levels of GRO-1 in
gastric cancer and found that its high expression was correlated
with tumor stage and lymph node metastasis. However, studies
investigating this factor in CSCC are extremely rare. In the
present study, the serum levels of GRO-1 in CSCC patients were
significantly higher than patients with CIN and the healthy
controls. In addition, the serum levels were associated with FIGO
stage, metastasis, pathological grading and pelvic lymph node
metastasis. In addition, the concentration of GRO-1 in patients
whose tumor size was >4 cm was higher than those in patients
whose tumor size was ≤4 cm, however, no difference was observed
between them, and this may be due to the small sample size. The
present study also could not verify the association between age and
GRO-1. This result is consistent with several previous studies
(13,14). Overall, detecting the serum levels
of GRO-1 in CSCC patients may be useful for predicting the state of
tumor load and the progression of the disease.
Several studies have indicated that the expression
of HGF mainly secreted by stromal cells is elevated in various
types of carcinoma (20,21), including cervical cancer (22). Certain studies have demonstrated
that overexpression of HGF is associated with the progression and
metastasis of hepatocellular carcinoma (20). Another study emphasized the
important role of HGF and c-MET in the progression and invasion of
esophageal squamous cell carcinoma (23). Nakamura et al (24) reported that HGF antagonists or
inhibitors of c-MET were able to inhibit tumor growth and
metastasis. The results from the present study demonstrated that
serum levels of HGF in CSCC patients were significantly increased
compared with the CIN patients and healthy controls, and that the
serum levels were correlated with FIGO stage, pathological grade,
pelvic lymph node metastasis and tumor size. These findings suggest
that the expression of HGF is associated with infiltration and
tumor metastasis. Therefore, inhibiting the HGF/c-MET signaling
pathway may be a potential therapeutic treatment for CSCC. In the
present study, it was also observed that the serum levels of HGF in
patients with metastasis were higher than those without metastasis,
however, no statistical significance was observed between them. In
addition, no correlation between HGF and age was found. Aune et
al (25) demonstrated that
preoperative serum HGF level is not associated with age, which is
consistent with the results from the present study.
Several studies have demonstrated that the
upregulation of PDGF in numerous carcinomas is able to promote
lymph node metastasis and tumor cell proliferation (26,27).
Importantly, it can promote the formation of tumor blood vessels
and lymph vessels (28,29). Therefore, PDGF may stimulate the
growth and metastasis of tumors by angiogenesis and
lymphangiogenesis. It is well established that vascular endothelial
growth factor (VEGF) is important in neoplasm angiogenesis. As a
member of the PDGF family, PDGF-AA is an important autocrine
regulator, which can regulate the expression of VEGF, thus PDGF-AA
may be a more potent therapeutic target for inhibiting angiogenesis
in tumors than VEGF (30). In the
present study, it was observed that the concentrations of PDGF-AA
in the serum of CSCC patients were correlated with FIGO stage,
pathological grading and lymph node metastasis, and these results
were in accordance with the above-mentioned studies. However, the
results from the present study demonstrated that the serum levels
of PDGF-AA were not associated with metastasis or tumor size and no
association of PDGF-AA between the CSCC patients and the other two
groups was found. The reasons for these results are diverse.
Although PDGF-AA is a potent angiogenic factor, tumor angiogenesis
is a multistep process including numerous growth factors and
cytokines and every step may lead to different outcomes. The
present study also verified that serum levels of PDGF-AA were not
associated with age, which is consistent with a former study
(26).
Previous studies have demonstrated that sE-selectin
is highly expressed in colorectal cancer and is closely associated
with the progression, recurrence and metastasis of cancer (31,32).
It was observed that the serum levels of sE-selectin were
significantly increased in CSCC patients and were correlated with
FIGO stage and tumor size. These findings suggested that the levels
of sE-selectin can predict tumor invasion and progression. No
association was found between sE-selectin and metastasis and
certain studies also failed to demonstrate an association between
sE-selectin and lymph node metastasis (33). Other studies indicated that
sE-selectin is not able to predict the metastasis of colorectal
cancer (34). Therefore, this
requires further investigation. It was also observed that the
levels of sE-selectin were significantly associated with age, which
is in accordance with a previous study (35). This may owe to a more active
metabolic activity in young patients. No significant correlation
was identified between sE-selectin and grading.
In the analysis of high-risk HPV infection in CSCC
patients, a higher rate of infection was found in the CSCC patients
compared with the CIN patients illustrating that HPV infection is
closely associated with the occurrence of cervical cancer (3,4).
However, no significance was found between HPV infection and
clinicopathological variables, which is consistent with the study
by Bachtiary et al (36).
The association between HPV and the four biomarkers was also
analyzed and only the serum levels of HGF in HPV-positive patients
were higher than HPV-negative patients. Walker et al
(37) clarified that the
overexpression of HGF is closely associated with cervical HPV
infection.
The association between serum levels of GRO-1, HGF,
PDGF-AA and sE-selectin in patients with CSCC was investigated in
the present study, and it was revealed that HGF was associated with
the other three factors, and PDGF-AA was associated with GRO-1.
Certain studies have demonstrated that HGF can enhance the
generation of GRO-1 and VEGF in vitro (38) and another study indicated that
serum levels of HGF in head and neck squamous cell carcinoma can
regulate the expression of PDGF-A (39). There were correlations between two
of either GRO-1, HGF and PDGF-AA in the present study, which
suggests that they have a common role in angiogenesis (11,17,40),
while no association was found between sE-selectin and GRO-1 and
PDGF-AA. Studies investigating this issue are rare and thus further
investigation is required.
The diagnostic value of the four biomarkers in CSCC
patients was also analyzed. HGF obtained the highest diagnostic
value although the diagnostic value of all four factors was not
significantly high. Hashem et al (41) reported the diagnostic value of HGF
in prostate cancer, thus the detection of HGF in the serum of
cervical cancer may provide aided diagnostic value.
Finally, the prognostic value of GRO-1, HGF,
PDGF-AA, sE-selectin and HPV was examined in patients with CSCC.
The results indicated that patients with a low expression of GRO-1,
HGF and sE-selectin had significantly longer OS and PFS than those
with high expression of the three factors. Furthermore, the
HPV-positive patients had shorter OS and PFS compared with the
HPV-negative patients, but only the levels of HGF, FIGO stage and
pelvic lymph node metastasis were independent prognostic factors in
the multivariate Cox analysis. Cheng et al (42) reported that GRO-1 may be a
promising adverse prognostic molecular marker, and Miyake et
al (43) confirmed the poor
prognostic value of GRO-1 in bladder cancer. Numerous studies have
demonstrated the prognostic value of sE-selectin in colorectal
cancer (31,34). Our findings suggested that GRO-1
and sE-selectin may have an impact on the prognosis of CSCC
patients by affecting FIGO stage or lymph node metastasis, thus
GRO-1 and sE-selectin were not independent prognostic risk factors.
Madsen et al (44) failed
to verify the prognostic value of PDGF-AA in ovarian cancer.
However, another study indicated the adverse prognosis of PDGF-AA
in pancreatic cancer (26), thus
the prognostic value of PDGF-AA in CSCC requires further
investigation. However, the prognostic value of HPV remains
controversial (6–10). Studies have reported the prognostic
value of HGF in patients with head and neck squamous cell carcinoma
and verified that the high expression of HGF was closely associated
with a poor prognosis (45). Aune
et al (25) demonstrated
its adverse prognostic significance in ovarian cancer. In cervical
cancer, the prognostic value of the HGF receptor was clarified by
Baykal et al (46),
therefore, in addition to these traditional prognostic indicators,
including FIGO stage and pelvic lymph node metastasis, the
pre-treatment serum levels of HGF may be a predictor of tumor
progression in certain early stage cervical carcinomas.
In conclusion, HGF may be a potential prognostic
tumor marker rather than high-risk HPV types in patients with CSCC,
therefore, detecting the serum levels of HGF may be useful for
predicting the prognosis of CSCC patients.
References
|
1
|
Ferlay J, Shin HR, Bray F, et al:
Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int
J Cancer. 127:2893–2917. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Wang SS, Sherman ME, Hildesheim A, Lacey
JV Jr and Devesa S: Cervical adenocarcinoma and squamous cell
carcinoma incidence trends among white women and black women in the
United States for 1976–2000. Cancer. 100:1035–1044. 2004.PubMed/NCBI
|
|
3
|
Walboomers JM, Jacobs MV, Manos MM, et al:
Human papillomavirus is a necessary cause of invasive cervical
cancer worldwide. J Pathol. 189:12–19. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Castellsagué X: Natural history and
epidemiology of HPV infection and cervical cancer. Gynecol Oncol.
110:S4–S7. 2008.
|
|
5
|
Bao YP, Li N, Smith JS and Qiao YL; ACCPAB
members. Human papillomavirus type distribution in women from Asia:
a meta-analysis. Int J Gynecol Cancer. 18:71–79. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Schwartz SM, Daling JR, Shera KA, et al:
Human papillomavirus and prognosis of invasive cervical cancer: a
population-based study. J Clin Oncol. 19:1906–1915. 2001.PubMed/NCBI
|
|
7
|
Kang WD, Kim CH, Cho MK, et al: HPV-18 is
a poor prognostic factor, unlike the HPV viral load, in patients
with stage IB-IIA cervical cancer undergoing radical hysterectomy.
Gynecol Oncol. 121:546–550. 2011. View Article : Google Scholar
|
|
8
|
Riou G, Favre M, Jeannel D, Bourhis J, Le
Doussal V and Orth G: Association between poor prognosis in
early-stage invasive cervical carcinomas and non-detection of HPV
DNA. Lancet. 335:1171–1174. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Higgins GD1, Davy M, Roder D, et al:
Increased age and mortality associated with cervical carcinomas
negative for human papillomavirus RNA. Lancet. 338:910–913. 1991.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Barreto CL, Martins DB, de Lima Filho JL
and Magalhães V: Detection of human Papillomavirus in biopsies of
patients with cervical cancer, and its association with prognosis.
Arch Gynecol Obstet. 288:643–648. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Belperio JA, Keane MP, Arenberg DA, et al:
CXC chemokines in angiogenesis. J Leukocyte Biol. 68:1–8. 2000.
|
|
12
|
Anisowicz A, Bardwell L and Sager R:
Constitutive overexpression of a growth-regulated gene in
transformed Chinese hamster and human cells. Proc Natl Acad Sci
USA. 84:7188–7192. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ogata H, Sekikawa A, Yamagishi H, et al:
GROα promotes invasion of colorectal cancer cells. Oncol Rep.
24:1479–1486. 2010.
|
|
14
|
Jung JJ, Noh S, Jeung HC, et al: Chemokine
growth-regulated oncogene 1 as a putative biomarker for gastric
cancer progression. Cancer Sci. 101:2200–2206. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Nakamura T, Nawa K and Ichihara A: Partial
purification and characterization of hepatocyte growth factor from
serum of hepatectomized rats. Biochem Biophys Res Commun.
122:1450–1459. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Cecchi F, Rabe DC and Bottaro DP:
Targeting the HGF/Met signalling pathway in cancer. Eur J Cancer.
46:1260–1270. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Ferrara N and Kerbel RS: Angiogenesis as a
therapeutic target. Nature. 438:967–974. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Gogali A, Charalabopoulos K, Zampira I, et
al: Soluble adhesion molecules E-cadherin, intercellular adhesion
molecule-1, and E-selectin as lung cancer biomarkers. Chest.
138:1173–1179. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Allen C, Duffy S, Teknos T, et al: Nuclear
factor-κB-related serum factors as longitudinal biomarkers of
response and survival in advanced oropharyngeal carcinoma. Clin
Cancer Res. 13:3182–3190. 2007.
|
|
20
|
Ogunwobi OO, Puszyk W, Dong HJ and Liu C:
Epigenetic upregulation of HGF and c-Met drives metastasis in
hepatocellular carcinoma. PloS One. 8:e637652013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Tyan SW, Kuo WH, Huang CK, et al: Breast
cancer cells induce cancer-associated fibroblasts to secrete
hepatocyte growth factor to enhance breast tumorigenesis. PLoS One.
6:e153132011. View Article : Google Scholar
|
|
22
|
Horn LC, Hommel N, Roschlau U, Bilek K,
Hentschel B and Einenkel J: Peritumoral stromal remodeling, pattern
of invasion and expression of c-met/HGF in advanced squamous cell
carcinoma of the cervix uteri, FIGO stages III and IV. Eur J Obstet
Gynecol Reprod Biol. 163:76–80. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Grugan KD, Miller CG, Yao Y, et al:
Fibroblast-secreted hepatocyte growth factor plays a functional
role in esophageal squamous cell carcinoma invasion. Proc Natl Acad
Sci USA. 107:11026–11031. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Nakamura T, Sakai K, Nakamura T and
Matsumoto K: Anti-cancer approach with NK4: bivalent action and
mechanisms. Anticancer Agents Med Chem. 10:36–46. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Aune G, Lian AM, Tingulstad S, et al:
Increased circulating hepatocyte growth factor (HGF): a marker of
epithelial ovarian cancer and an indicator of poor prognosis.
Gynecol Oncol. 121:402–406. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Rahbari NN, Schmidt T, Falk CS, et al:
Expression and prognostic value of circulating angiogenic cytokines
in pancreatic cancer. BMC cancer. 11:2862011. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Willenberg A, Saalbach A, Simon JC and
Anderegg U: Melanoma cells control HA synthesis in peritumoral
fibroblasts via PDGF-AA and PDGF-CC: impact on melanoma cell
proliferation. J Invest Dermatol. 132:385–393. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Suzuki S, Dobashi Y, Hatakeyama Y, et al:
Clinicopathological significance of platelet-derived growth factor
(PDGF)-B and vascular endothelial growth factor-A expression, PDGF
receptor-β phosphorylation, and microvessel density in gastric
cancer. BMC cancer. 10:6592010.PubMed/NCBI
|
|
29
|
Donnem T, Al-Saad S, Al-Shibli K, Busund
LT and Bremnes RM: Co-expression of PDGF-B and VEGFR-3 strongly
correlates with lymph node metastasis and poor survival in
non-small-cell lung cancer. Ann Oncol. 21:223–231. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Shikada Y, Yonemitsu Y, Koga T, et al:
Platelet-derived growth factor-AA is an essential and autocrine
regulator of vascular endothelial growth factor expression in
non-small cell lung carcinomas. Cancer Res. 65:7241–7248. 2005.
View Article : Google Scholar
|
|
31
|
Ferroni P, Roselli M, Spila A, et al:
Serum sE-selectin levels and carcinoembryonic antigen
mRNA-expressing cells in peripheral blood as prognostic factors in
colorectal cancer patients. Cancer. 116:2913–2921. 2010. View Article : Google Scholar
|
|
32
|
Dymicka-Piekarska V and Kemona H: Does
colorectal cancer clinical advancement affect adhesion molecules
(sP-selectin, sE-selectin and ICAM-1) concentration? Thromb Res.
124:80–83. 2009. View Article : Google Scholar
|
|
33
|
Mantur M, Snarska J, Koper O, et al: Serum
sICAM, sVCAM and sE-selectin levels in colorectal cancer patients.
Folia Histochem Cytobiol. 47:621–625. 2009.PubMed/NCBI
|
|
34
|
Uner A, Akcali Z and Unsal D: Serum levels
of soluble E-selectin in colorectal cancer. Neoplasma. 51:269–274.
2004.PubMed/NCBI
|
|
35
|
Nash MC, Wade AM, Shah V and Dillon MJ:
Normal levels of soluble E-selectin, soluble intercellular adhesion
molecule-1 (sICAM-1), and soluble vascular cell adhesion molecule-1
(sVCAM-1) decrease with age. Clin Exp Immunol. 103:167–170. 1996.
View Article : Google Scholar
|
|
36
|
Bachtiary B, Obermair A, Dreier B, et al:
Impact of multiple HPV infection on response to treatment and
survival in patients receiving radical radiotherapy for cervical
cancer. Int J Cancer. 102:237–243. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Walker F, Kermorgant S, Daraï E, et al:
Hepatocyte growth factor and c-Met in cervical intraepithelial
neoplasia overexpression of proteins associated with oncogenic
human papillomavirus and human immunodeficiency virus. Clin Cancer
Res. 9:273–284. 2003.
|
|
38
|
Dong G, Lee TL, Yeh NT, et al: Metastatic
squamous cell carcinoma cells that overexpress c-Met exhibit
enhanced angiogenesis factor expression, scattering and metastasis
in response to hepatocyte growth factor. Oncogene. 23:6199–6208.
2004. View Article : Google Scholar
|
|
39
|
Worden B, Yang XP, Lee TL, et al:
Hepatocyte growth factor/scatter factor differentially regulates
expression of proangiogenic factors through Egr-1 in head and neck
squamous cell carcinoma. Cancer Res. 65:7071–7080. 2005. View Article : Google Scholar
|
|
40
|
Carmeliet P and Jain RK: Angiogenesis in
cancer and other diseases. Nature. 407:249–257. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Hashem M and Essam T: Hepatocyte growth
factor as a tumor marker in the serum of patients with prostate
cancer. J Egypt Natl Canc Inst. 17:114–120. 2005.PubMed/NCBI
|
|
42
|
Cheng WL, Wang CS, Huang YH, et al:
Overexpression of CXCL1 and its receptor CXCR2 promote tumor
invasion in gastric cancer. Ann Oncol. 22:2267–2276. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Miyake M, Lawton A, Goodison S, et al:
Chemokine (CXC) ligand 1 (CXCL1) protein expression is increased in
aggressive bladder cancers. BMC cancer. 13:3222013. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Madsen CV, Steffensen KD, Olsen DA, et al:
Serial measurements of serum PDGF-AA, PDGF-BB, FGF2, and VEGF in
multiresistant ovarian cancer patients treated with bevacizumab. J
Ovarian Res. 5:232012. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Rischin D, Fisher R, Oliner K, et al:
Prognostic significance of interleukin-8 (IL-8) and hepatocyte
growth factor (HGF) in patients with head and neck squamous cell
carcinoma (HNSCC) treated with chemoradiation on a phase III trial.
J Clin Oncol (Meeting Abstracts). 28:55092010.
|
|
46
|
Baykal C and Ayhan A, Al A, Yüce K and
Ayhan A: Overexpression of the c-Met/HGF receptor and its
prognostic significance in uterine cervix carcinomas. Gynecol
Oncol. 88:123–129. 2003. View Article : Google Scholar : PubMed/NCBI
|