Introduction
As the development of therapeutics for ischemic
injury continues, brain imaging is taking an increasingly important
role in the initial evaluation of patients with acute stroke
(1). Exclusion of cerebral
hemorrhage by computed tomography (CT) or magnetic resonance
imaging (MRI) is necessary for any acute intervention in ischemic
stroke (1,2). At present, the American Heart
Association Stroke Council recommend the administration of
intravenous recombinant tissue plasminogen activator (rtPA) within
a 4.5-h thrombolytic therapy time window for patients with acute
ischemic stroke (2,3). Despite its potential effectiveness,
no objective assessment or quantitative criteria exist to evaluate
factors governing the 4.5-h time window. Intracranial hemorrhage
remains the major risk of intravenous rtPA treatment (2).
With the potential of rtPA treatment, interest in
using CT to identify the preliminary changes of ischemic brain
injury (early infarct signs) or arterial occlusion (hyperdense
vessel signs), which may affect treatment decisions is increasing.
In addition, sulcal effacement and loss of gray-white
differentiation in the cortical ribbon (particularly at the lateral
margins of the insula) or lentiform nucleus can often be detected
within 6 h in up to 82% of patients with large-vessel anterior
circulation occlusions (4). Such
symptoms often result in poorer outcomes (5). Standard MRI sequences (T1
weighted, T2 weighted and proton density) often do not
reveal changes resulting from acute ischemia (6,7). The
mismatch between magnetic resonance (MR), diffusion-weighted
imaging (DWI) and perfusion-weighted imaging (PWI) in the
visualization of the penumbra has been suggested to guide
thrombolytic therapy. However, several studies have indicated that,
at least under certain circumstances, the initial diffusion
abnormality is reversible and that visually thresholded perfusion
volumes overestimate the penumbra (8,9).
Sequential MRI studies performed on patients treated with
thrombolytic therapy have revealed that an MRI may visualize the
salvaged mismatch-defined penumbral tissue in smaller volumes of
infarction among patients with successful recanalization (9).
It is well known that diffusion MRI and proton MR
spectroscopy (MRS) can evaluate early metabolite alterations in
acute stroke in humans and animals (10). Several studies have demonstrated
that MRI is the modality of choice for studies of early stroke
brain injury in humans (11) and
in a rat middle cerebral artery occlusion (MCAO) model (12). MR-based DWI is sensitive to changes
in the magnitude and direction of water diffusion. Numerous studies
have demonstrated that the apparent diffusion coefficient (ADC), a
parameter derived from DWI, is reduced in the hyperacute phase of
an ischemic event, resulting from the influx of water from the
extracellular space into the intracellular space (13,14).
Proton MRS can provide information on the severity of ischemic
injury by measuring the levels of metabolites following cerebral
ischemia (15). In particular, a
decrease in N-acetyl-aspartate (NAA) has been observed to
correlate with neuronal loss and is a predictor of outcome
following stroke and traumatic brain injury (16). Recent studies on ischemic mice or
human patients with traumatic brain injury revealed that important
metabolite concentration changes occurred prior to the appearance
of abnormalities and which could not be detected by MRI (17), suggesting that MRS is better at
detecting early tissue damage or compromised cell function.
Following the progression of ischemic injury, proton MRS may be a
valuable tool for providing information on the timing and pattern
of acute metabolic changes, as increased quantities of lactate are
detected in the early stages of stroke and are prognostic (18).
In the present study, a rat model of MCAO was used
to continuously assess and quantify brain alterations at 1-h
intervals within the first 3 h after stroke onset using
multiparametric MRI. The early neurochemical changes in ischemic
brain tissue and their role in early ischemic damage in vivo
were further investigated.
Materials and methods
Animal model
Adult male Sprague-Dawley rats, aged 7–8 weeks old
and weighing 250–280 g, were used in all experiments. Rats were
obtained from the Shantou University Medical College Laboratory
Animal Center (Shantou, China). The animals were housed under
standard laboratory conditions with a 12-h light/dark cycle at a
room temperature of 24±1°C and a relative humidity of 45±5%. All
experimental procedures were approved by the Care of Experimental
Animals Committee of Shantou University (Shantou, China) and were
performed in accordance with their guidelines. Permanent middle
cerebral artery occlusion (pMCAO) was induced using a previously
described method of intraluminal vascular occlusion (19). Rats subjected to pMCAO were
subjected to a consistent and reproducible ischemic lesion in the
unilateral striatum and cortex. Briefly, a 20-mm incision was made
at the center of the neck and the right common carotid artery,
external carotid artery (ECA) and internal carotid artery (ICA)
were exposed under an operating microscope (SXP-1C; Shanghai
Medical Equipment Co., Shanghai, China). The ECA and ICA were
temporarily clamped using microsurgical clips. A 5-0 silk suture
was tied loosely at the origin of the ECA and ligated at the distal
end of the ECA. A length of 4-0 monofilament nylon suture
(18.5–19.5 mm), determined by the animal’s weight and with its tip
rounded by heating near a flame, was introduced into the ECA lumen
through a small puncture. The silk suture surrounding the ECA
origin was tightened around the intraluminal nylon suture to
prevent bleeding and the microsurgical clips were removed. The
nylon suture was gently advanced from the ECA into the lumen of the
ICA until it blocked the origin of the MCA. Immediately following
the occlusion, the rat was positioned in an animal holder equipped
with a birdcage radio frequency coil manufactured in house.
MRI and localized proton MR spectroscopy
acquisition
For in vivo MRI and 1H MRS,
animals were initially anesthetized using a chamber pervaded with
5% isoflurane (Sigma-Aldrich, St. Louis, MO, USA) in oxygen.
Subsequently, the mice were anesthetized through a mask by
spontaneous inhalation of 1.5–2.0% isoflurane and air using an
anesthesia unit. Anesthetized rats were placed in the prone
position with the head firmly fixed on a palate holder equipped
with an adjustable nose cone. MR imaging was performed on 12
animals using a 7.0 T horizontal DriveDrive 2 MR system (Agilent
Technologies, Santa Clara, CA, USA) with a 160-mm bore magnet and a
400 mT/m actively shielded gradient coil. For proton spectra signal
excitation and reception, a dedicated animal brain surface coil (20
mm, 157–350 MHz, Agilent Technologies) was used.
A scout view was initially obtained to verify the
animal’s position and the image quality. T2 weighted
images (sequence, rapid acquisition with a relaxation enhancement;
repetition time (TR)/echo time (TE), 2,000/48 ms; number of
acquisitions, 4; slice thickness, 1.0 mm; matrix, 192×192) were
obtained. Diffusion-weighted indices were acquired from a
multi-shot fast spin-echo trace sequence (TR, 3,000 ms; TE, 36 ms;
b, 1,000 s/mm2; Δ,14.65 ms; duration, 5 ms, average, 4;
matrix, 128×128). In vivo proton spectra volumes of interest
(VOI) were positioned in regions with ischemic lesions (3.5×3.5×3.5
mm) based on multi-slice axial diffusion-weighted images. The VOI
was adjusted to minimize intracranial lipid contamination.
Localized shimming in the VOI was performed automatically based on
three dimensional field mapping, leading to a water line width
ranging from 15 to 20 Hz. An ultra short echo time stimulated echo
acquisition pulse sequence was used for acquisition of the proton
spectra in the VOI (TR/mixing time/TE, 5,000/12.72/2.35 ms;
spectral width, 5,000 Hz; number of excitations, 160; scan time, 13
min). The water signal from the VOI was suppressed by variable
power radio frequency pulses with optimized relaxation delays. To
compensate for eddy currents, a water reference scan was acquired,
which also served as an internal reference for absolute
quantification.
In vivo proton spectra were analyzed using
the LCModel 6.3-1B software (LCModel Inc., Oakville, ON, Canada)
(20), which calculates the best
fit to the experimental spectrum as a linear combination of model
spectra (simulated spectra of brain metabolites). Raw data free
induction decays were used as the standard data input. The
water-suppressed time domain data were analyzed between 0.2 and 4.0
ppm without further T1 or T2 correction. The
following 17 metabolites were included in the basis set: Alanine
(Ala), aspartate (Asp), creatinine (Cr), γ-aminobutyric acid
(GABA), glucose (Glc), glutamate (Glu), glutamine (Gln),
glutathione (GSH), glycerophosphorylcholine (GPC),
phosphorylcholine (PCho), myo-ionositol (mIns), lactate (Lac),
N-acetyl aspartate (NAA), N-acetylaspartylglutamate
(NAAG), phosphocreatine (PCr), scyllo-inositol (Scy) and taurine
(Tau). In addition, macromolecules were also included in the basis
set. To obtain more reliable results, only the sums of metabolites
(NAA+NAAG, Glu+Gln, GPC+PCho and Cr+PCr) were estimated. The other
metabolites, including mIns and Tau, were individually
quantified.
The standard error estimates and Cramer Rao lower
bounds (CRLBs) were used to provide useful estimates of reliability
and uncertainty for each metabolite peak in the LCModel spectra
(20). CRLBs have been used to
provide acceptable reliability for estimates of fitting
uncertainty.
Statistical analysis
The SPSS software package version 12.01 (SPSS, Inc.,
Chicago, IL, USA) was used for statistical analysis. Data for each
metabolite were assessed for homogeneity of variance and a one-way
analysis of variance with a Bonferroni post hoc test was
used to compare the means of the metabolite ratios for each
time-point group. P<0.05 was considered to indicate a
statistically significant difference.
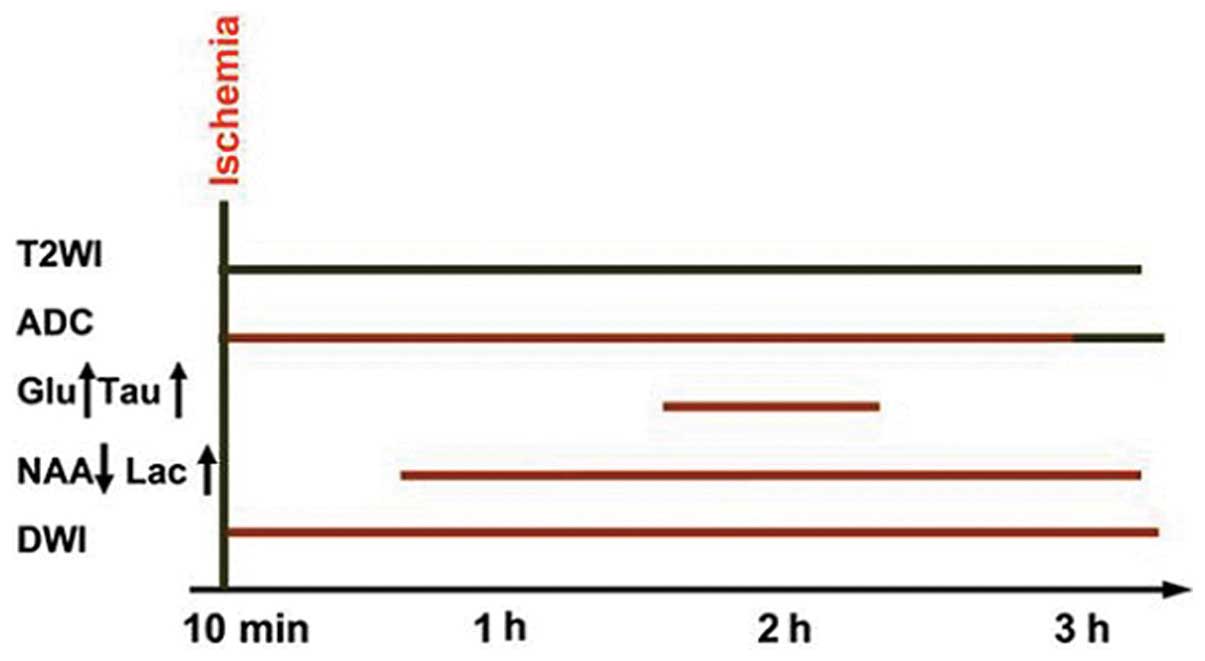
Results
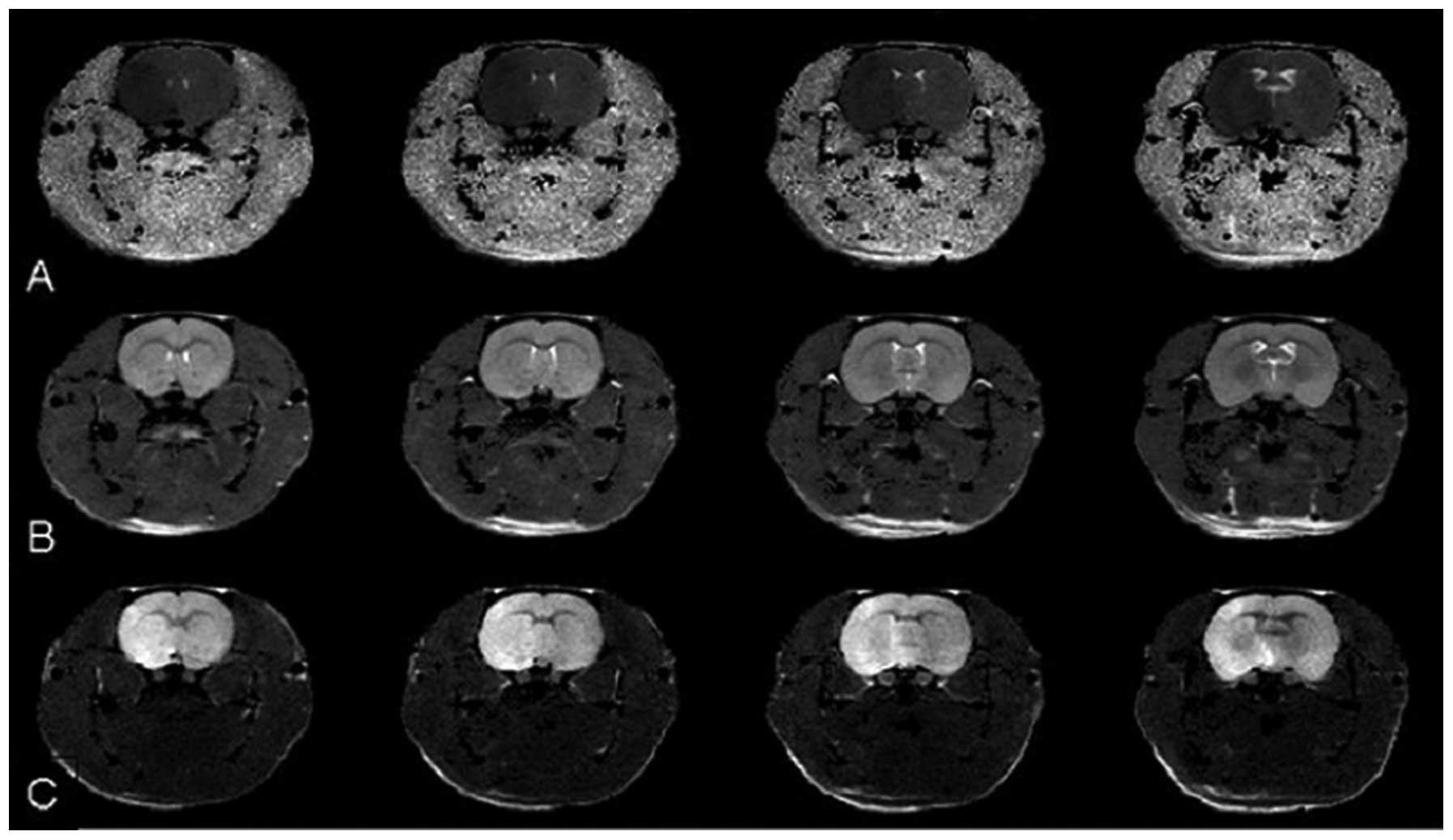
For all 20 MCAO rats, the infarct was not observable
by T2WI within 6 h from the onset of ischemia. However,
abnormal hyperintensity signals were observed by DWI in the
striatum and parietal cortex of all MCAO rats 10 min and 6 h after
the onset of ischemia. The ADC demonstrated abnormal, hypointense
signals in the same area and at the same time-point (Fig. 1). The baseline mean ADC was
(7.573±0.553)×10−4 mm2/sec, comparable to
values previously reported (21).
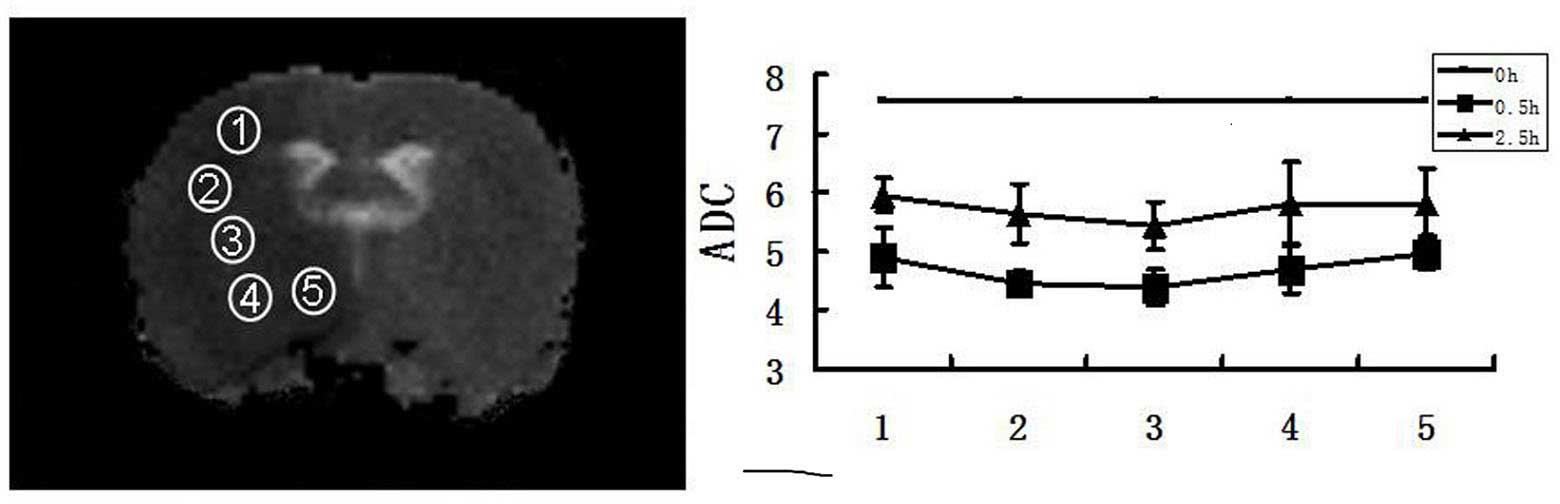
At 30 min after MCAO, the ADC decreased from
(4.7571±1.423)×10−4 to (5.7318±1.031)×10−4
mm2/sec. The ADC values increased gradually from the
center towards the periphery of the damaged areas at the 0.5 h and
2.5 h time-points. At 3 h after the onset of ischemia, the ADC
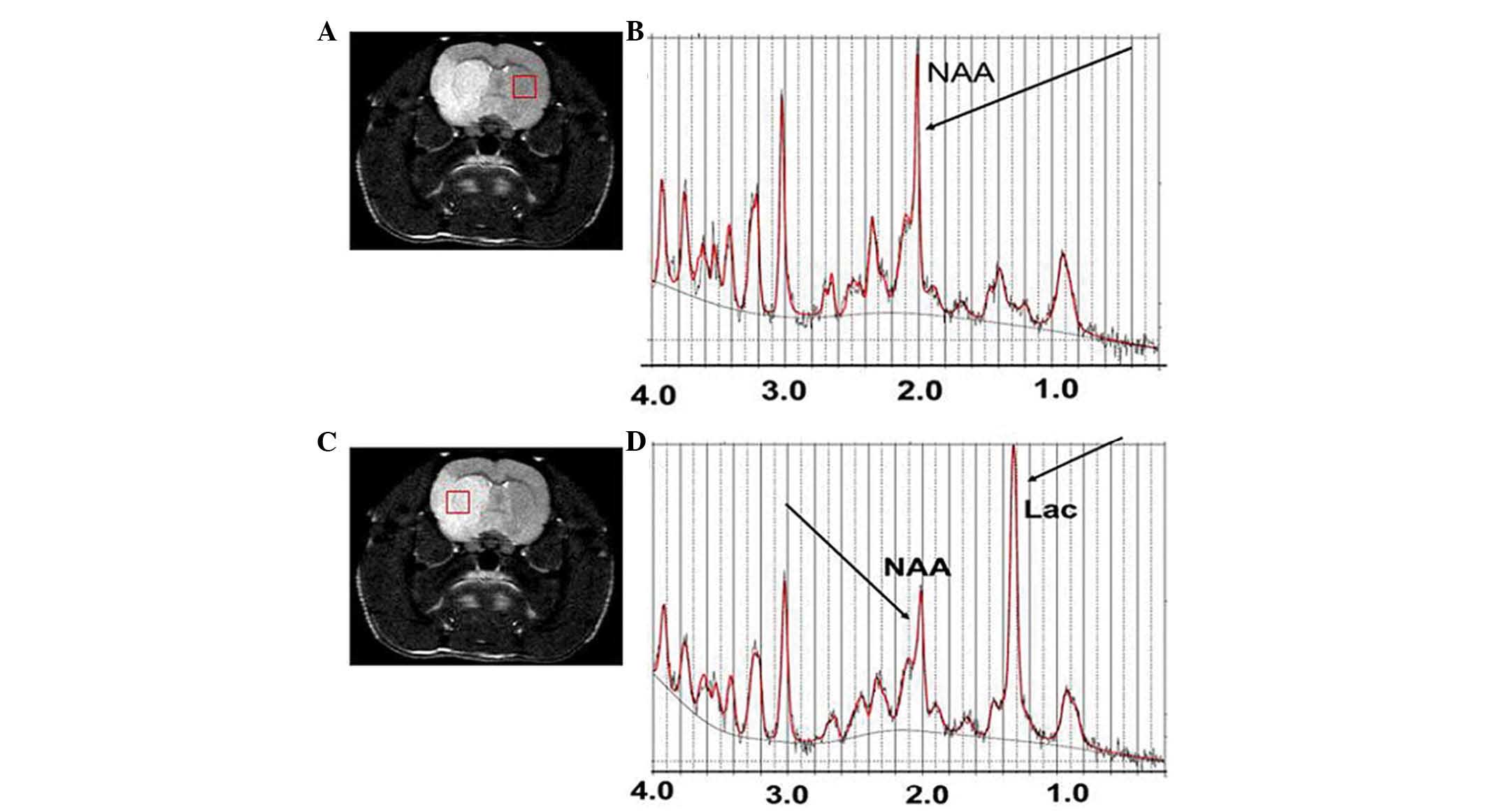
values were the same across all areas (Fig. 2). Typical water-suppressed proton
MR spectra of the rat brain from the region of the ischemic lesion
and the ipsilateral hemisphere (Fig.
3) represent the spectral quality consistently achieved in the
present study. Generally, short echo time localization methods
minimize T2 relaxation effects, which increases the
sensitivity and reliability of the metabolite quantification
(22). The high spectral
resolution allowed for unambiguous signal assignment. In addition
to the commonly observed 1H-MRS signals of the methyl
resonances of NAA, Cr and Cho, spectral patterns of other
metabolites, including Glu, Gln, GABA, mIns and Tau were
discernible in the 1H-MRS spectra with a CRLB ≤15% from
the two brain regions. The Lac peak was higher and the NAA peak
lower in the central damaged area than that on the contralateral
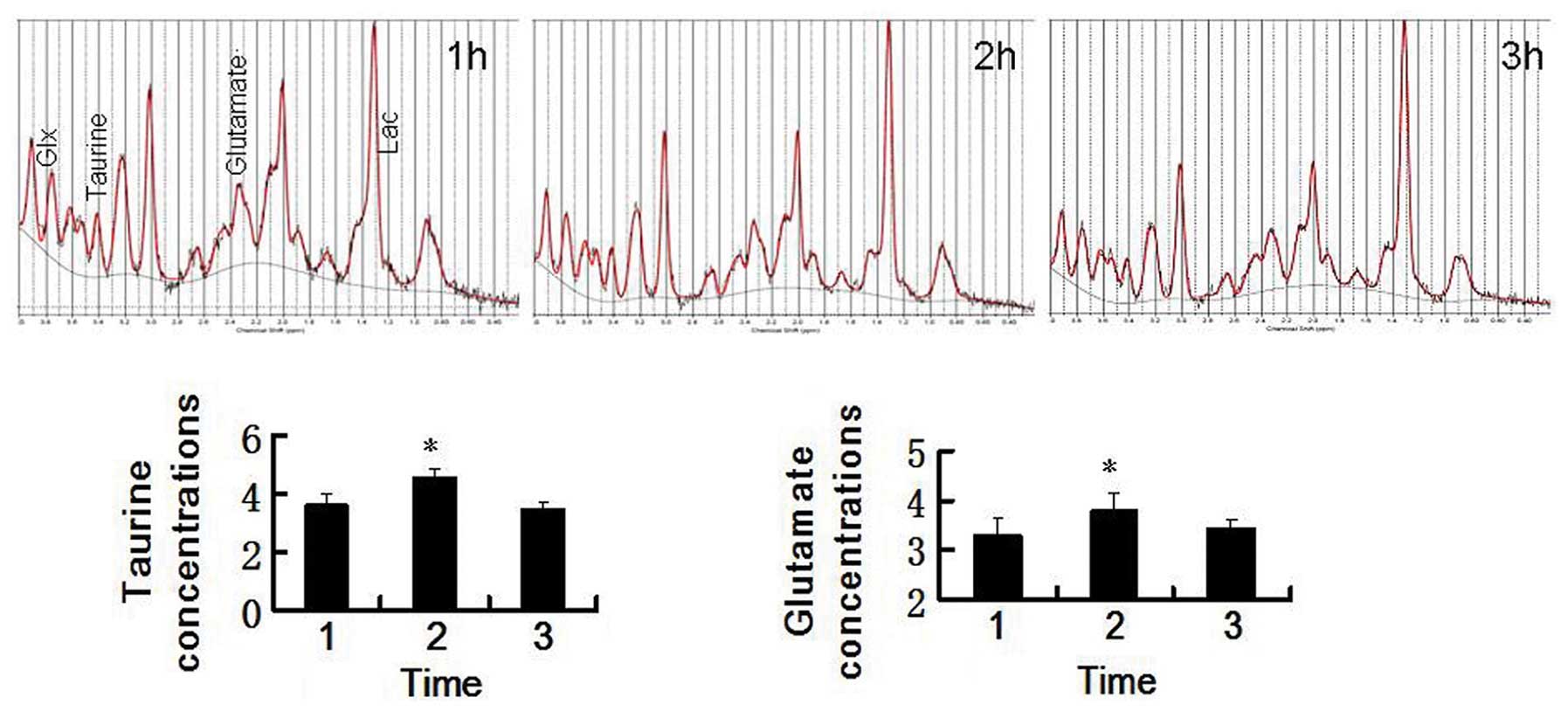
side at the 1 h time-point for all 12 MCAO rats (Fig. 3). 1H-MRS for each
time-point after the onset of ischemia are shown in Fig. 4. Within the first 2 h, the
concentrations of Glu and Tau increased gradually and then
decreased significantly in the following 3 h (Fig. 4).
Discussion
High DWI signal intensities in the right corpus
striatum and parietal cortex of the Sprague-Dawley rats were
observed following 30 min of middle cerebral artery occlusion in
the present study, but no intensity changes were observed in the
same regions by T2WI, even after 6 h of occlusion. The
present finding was consistent with that of a previous study
(23). DWI is a highly sensitive
and specific technique for the early diagnosis of acute cerebral
ischemia and is currently in use for the diagnosis and decisions on
therapy of patients with stroke. Signal intensity in DWIs exhibited
little change during the first hour after symptom onset and
decreased thereafter, but all lesions remained hyperintense
throughout the follow-up period. This pattern of signal intensity
on DWI was most likely the result of the effects of two factors:
Water diffusivity and intrinsic T2 properties
(T2 shine-through) of the tissue being examined
(24). Since the DWI signal
remained high for a long period (up to three days in the present
study), it is not ideal for estimating lesion age. However, the
combined interpretation of T2WI and DWI may be
insightful, as in cases where visual inspection of T2WI
shows normal results while DWI shows highly abnormal signals, the
stroke lesion age can be estimated as 6 h or less.
ADC is a parameter used for the quantitative
assessment of the extent and severity of cerebral ischemic injury
(13). A severe ADC decline in
energy-depleted tissue can be explained by anoxic depolarization
during MCAO, leading to an intracellular Na+
accumulation and water shift from the extracellular to the
intracellular space (cytotoxic edema). Quantitative ADC voxel
compartmental analysis revealed heterogeneity in the
spatial-temporal profile of the ischemic penumbra and infarction.
The ADC increased gradually from the center to the periphery of the
damaged area at the 0.5 h and 2.5 h time-points after permanent
MCAO. However, 3 h after the onset of ischemia, the ADC values were
equivalent across the entire region. The present results indicated
that an ADC map may provide useful information regarding the age of
ischemic lesions at 3 h. These results provided a novel method to
evaluate lesion age in a rat model of MCAO model, while previous
methods were not sufficient to adequately and accurately
characterize these conditions (14). Predictive algorithms also have the
potential to serve as promising metrics for screening thrombolytics
for acute ischemic stroke (4).
Glu is an excitatory neurotransmitter, which
stimulates postsynaptic neurons, whereas GABA and Tau are
inhibitory neurotransmitters that reduce the excitability of
neurons. The homeostasis of the metabolism of Glu and GABA is
usually dependent on the interaction between neurons and astrocytes
under physiological conditions. Previous studies revealed that the
concentrations of Glu, GABA and Tau decreased concurrently 4 and 8
h after MCAO, respectively (25,26).
In the present study, the extracellular content of excitatory amino
acids (Glu and Asp) and inhibitory amino acids (GABA and Tau)
reached a maximum in rats 1–2 h after MCAO and began to decrease 3
h after MCAO, which was consistent with a previous study (27). Increases in extracellular Glu may
lead to cell death by excitotoxicity, and therefore, it may be
vital to detect Glu in patients with stroke in order to make prompt
treatment decisions. The methods developed in the present study
provide tools for screening patients for thrombolytic therapy.
Combined analysis of DWI infarct size and location may provide
important information about when Glu and Tau are at their highest
levels, which may be used for selecting treatments for acute MCAO
ischemic stroke within 2 h of onset.
These MR-based findings provide a relatively
accurate method to predict the age of acute ischemic lesions in
animal models (Fig. 5). Indeed,
the final goal of our ongoing studies is to assess whether combined
T2WI, ADC and MRS can be used for early diagnosis and to
determine the onset time of acute ischemic stroke in human
patients. Further studies are required to extend the present
findings to humans. Precise knowledge of the onset time of
thrombolytic stroke is important, but there are difficult questions
based on the definition of acute ischemic stroke. The MR-based
methods described in the present study are more objective than
relying solely on the traditional image reading methods used by
radiologists to estimate acute ischemic stroke lesion age and to
select patients for treatment trials.
In conclusion, hyperacute cerebral infarction can be
sensitively and specifically detected with the application of ADC
on DWI and MRS. MR-based methods may also be used to quantitatively
assess the ischemic onset time of hyperacute ischemic stroke.
Objective and quantitative assessments of lesion age in hyperacute
ischemic stroke are useful parameters for the identification of
potential therapies in clinical trials and individualized
treatments for stroke patients.
Acknowledgments
The present study was supported in part by a grant
from The National Natural Science Foundation of China (grant no.
30930027) and a postdoctoral research fellowship from the Li Ka
Shing foundation.
References
|
1
|
Adams HP Jr, del Zoppo G, Alberts MJ, et
al: Guidelines for the early management of adults with ischemic
stroke. Circulation. 115:e478–e534. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Jauch EC, Saver JL, Adams HP, et al:
Guidelines for the early management of patients with acute ischemic
stroke a guideline for healthcare professionals from the american
heart association/American stroke association. Stroke. 44:870–947.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Cho KH, Ko SB, Kim DH, et al: Focused
update of Korean clinical practice guidelines for the thrombolysis
in acute stroke management. J Korean Stroke. 14:95–105. 2012.
View Article : Google Scholar
|
|
4
|
Moulin T, Cattin F, Crepin-Leblond T, et
al: Early CT signs in acute middle cerebral artery infarction
Predictive value for subsequent infarct locations and outcome.
Neurology. 47:366–375. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Von Kummer R, Allen KL, Holle R, et al:
Acute stroke: usefulness of early CT findings before thrombolytic
therapy. Radiology. 205:327–333. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Mohr JP, Biller J, Hilal SK, et al:
Magnetic resonance versus computed tomographic imaging in acute
stroke. Stroke. 26:807–812. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lee DH, Kang DW, Ahn JS, Choi CG, Kim SJ
and Suh DC: Imaging of the ischemic penumbra in acute stroke.
Korean J Radiol. 6:64–74. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sobesky J, Zaro Weber Oz, Lehnhardt F, et
al: Does the mismatch match the penumbra? Magnetic resonance
imaging and positron emission tomography in early ischemic stroke.
Stroke. 36:980–985. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kidwell CS, Alger JR and Saver JL: Beyond
mismatch evolving paradigms in imaging the ischemic penumbra with
multimodal magnetic resonance imaging. Stroke. 34:2729–2735. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hacke W, Albers G, Al-Rawi Y, et al: The
desmoteplase in acute ischemic stroke trial (DIAS) a phase II
MRI-based 9-h window acute stroke thrombolysis trial with
intravenous desmoteplase. Stroke. 36:66–73. 2005. View Article : Google Scholar
|
|
11
|
Kertesz A, Black SE, Nicholson L and Carr
T: The sensitivity and specificity of MRI in stroke. Neurology.
37:1580. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Baird AE and Warach S: Magnetic resonance
imaging of acute stroke. J Cerebr Blood F Metab. 18:583–609. 1998.
View Article : Google Scholar
|
|
13
|
Warach S, Gaa J, Siewert B, Wielopolski P
and Edelman RR: Acute human stroke studied by whole brain echo
planar diffusion-weighted magnetic resonance imaging. Ann Neurol.
37:231–241. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kim Jh, Na DG, Chang KH, et al: Serial MR
analysis of early permanent and transient ischemia in rats:
diffusion tensor imaging and high b value diffusion weighted
imaging. Korean J Radiol. 14:307–315. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Parsons MW, Barber PA, Desmond PM, et al:
Acute hyperglycemia adversely affects stroke outcome: a magnetic
resonance imaging and spectroscopy study. Ann neurol. 52:20–28.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Gillard JH, Barker PB, Van Zijl C, Bryan
RN and Oppenheimer SM: Proton MR spectroscopy in acute middle
cerebral artery stroke. AJNR. 17:873–886. 1996.PubMed/NCBI
|
|
17
|
Berthet C, Lei H, Gruetter R and Hirt L:
Early predictive biomarkers for lesion after transient cerebral
ischemia. Stroke. 42:799–805. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Cvoro V, Wardlaw JM, Marshall I, et al:
Associations between diffusion and perfusion parameters, N-acetyl
aspartate and lactate in acute ischemic stroke. Stroke. 40:767–772.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Longa EZ, Weinstein PR, Carlson S and
Cummins R: Reversible middle cerebral artery occlusion without
craniectomy in rats. Stroke. 20:84–91. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Provencher SW: Automatic quantitation of
localized in vivo 1H spectra with LCModel. NMR Biomed. 14:260–264.
2001. View
Article : Google Scholar : PubMed/NCBI
|
|
21
|
Neumann-Haefelin T, Kastrup A, de
Crespigny A, et al: Serial MRI after transient focal cerebral
ischemia in rats: dynamics of tissue injury, blood-brain barrier
damage and edema formation. Stroke. 31:1965–1972; discussion
1972–1963. 2000. View Article : Google Scholar
|
|
22
|
Pfeuffer J, Provencher SW and Gruetter R:
Water diffusion in rat brain in vivo as detected at very largeb
values is multicompartmental. MAGMA. 8:98–108. 1999.PubMed/NCBI
|
|
23
|
Sicard KM, Henninger N, Fisher M, Duong TQ
and Ferris CF: Differential recovery of multimodal MRI and behavior
after transient focal cerebral ischemia in rats. J Cerebr Blood F
Met. 26:1451–1462. 2006. View Article : Google Scholar
|
|
24
|
Le Bihan D, Breton E, Lallemand D, Grenier
P, Cabanis E and Laval-Jeantet M: MR imaging of intravoxel
incoherent motions: application to diffusion and perfusion in
neurologic disorders. Radiology. 161:401–407. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Pascual JM, Carceller F, Roda JM and
Cerdán S: Glutamate, glutamine and GABA as substrates for the
neuronal and glial compartments after focal cerebral ischemia in
rats. Stroke. 29:1048–1057. 1998. View Article : Google Scholar
|
|
26
|
al-Nazhan S, Andreasen JO, al-Bawardi S
and al-Rouq S: Evaluation of the effect of delayed management of
traumatized permanent teeth. J Endod. 21:391–393. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Graham SH, Chen J, Sharp FR and Simon RP:
Limiting ischemic injury by inhibition of excitatory amino acid
release. J Cerebr Blood F Metab. 13:88–97. 1993. View Article : Google Scholar
|