Introduction
Cervical cancer is the most common cancer type
amongst women in Sub-Saharan Africa, with an age-standardized
incidence rate of 34.8 per 105 females (1). Cervical cancer is also the leading
cause of cancer-associated mortality amongst women in this region,
with 22.5 per 105 women dying from the disease annually
(1). It is well-established that
infection with oncogenic Human Papilloma Viruses (HPV) is the main
cause of cervical cancer (2,3). The
high incidence of cervical cancer in Africa is likely due to a
combination of factors. These include lack of awareness of the
disease and its causes, as well as challenges in implementing
regular HPV Papanicolaou (Pap)-smear screenings and HPV
vaccinations, which have only recently been introduced into the
South African health care system (4–6).
While a large number of women are infected with the HPV virus, not
all of them develop cervical cancer (7). Heritability studies have shown that
susceptibility to cervical cancer may be genetic (8) and recent studies have reported an
association between cervical cancer and genes involved in DNA
damage repair, including APE1, XRCC2, XRCC3, ERCC1, ERCC2, ERCC4
and ATM (9–12).
Enhanced chromosomal radiosensitivity is associated
with defects in genes involved in DNA damage repair (13). A possible inherited basis for
radiosensitivity was first indicated by studies on patients with
rare genetic syndromes, including Ataxia Telangiectasia and
Nijmegen breakage syndrome (13).
These patients were shown to display chromosomal radiosensitivity
not only by clinical observations, but also by in vitro
assays (14). Patients with these
syndromes have germline mutations in genes involved in DNA damage
repair and also display predisposition to numerous cancer types.
Their increased chromosomal radiosensitivity encouraged
investigations demonstrating an enhanced in vitro
chromosomal radiosensitivity in patients with various cancer types,
including breast, head and neck and prostate cancer (15–18).
Mutations in DNA repair genes not only lead to increased
chromosomal radiosensitivity in these patients but may also
predispose them to the development of cancer (13,17,19,20).
The chromosomal radiosensitivity of lymphocytes of cervical cancer
patients has been investigated in vitro using a variety of
cytogenetic assays, however, results have been inconclusive
(21–24).
A well-established method to measure chromosomal
radiosensitivity is the micronucleus (MN) assay, which quantifies
residual chromosomal damage resulting from mis-or non-repaired
double-strand breaks after exposure to radiation. This assay can be
performed on lymphocytes, which are an attractive model for
radiosensitivity studies, as they are easily obtainable through
venepuncture. MN scoring in this assay can be automated with an MN
scoring module of the Metafer 4 platform. The MNScore micronucleus
software module allows automated screening of binucleate cells and
the subsequent scoring of MN in these cells (25). In this system, various scoring
methods can be utilized that involve varying degrees of visual
validation of automated scoring to correct for false positive and
false negative MN and reject unsuitable cells (26,27).
The benefits and challenges of using the MN assay with the Metafer
4 platform have been documented elsewhere (26–32).
A study performed by our group (33) has previously shown that individuals
infected with human immunodeficiency virus (HIV) are more
chromosomally radiosensitive than HIV-negative individuals. In
South Africa, ~5.7 million people are HIV-positive (34). HIV, HPV and cervical cancer are
epidemiologically associated and in 1993, invasive cervical
carcinoma was classified as an acquired immune deficiency
syndrome-defining illness by the United States Centers for Disease
Control and Prevention (35).
Rates of HPV infection increase with decreasing CD4-cell count
(36) and studies have shown that
HPV infection still persists in a high proportion of patients
receiving highly active anti-retroviral therapy (37). Due to the high rate of HIV in
Africa and its association with cervical cancer, it is likely that
a significant proportion of cervical cancer patients seeking
treatment are HIV-positive.
The aim of the present study was to investigate the
in vitro chromosomal radiosensitivity in South African
cervical cancer patients by means of the MN assay using a
case-control study design. Concurrently, various scoring methods
were evaluated when using the MN assay with the Metafer 4 platform.
Due to the high rate of HIV in South Africa and its association
with cervical cancer, the effect of the HIV infection status on
chromosomal radiosensitivity of patients was also assessed.
Patients and methods
Study population
Blood samples were obtained via venepuncture from a
total of 35 cervical cancer patients (mean age, 46 years) and 20
healthy female controls (mean age, 41 years). Among the patients
with cervical cancer, 15 were infected with HIV (mean age, 43
years) and 20 were HIV-negative (mean age, 49 years). Patients were
recruited from the public Charlotte Maxeke Johannesburg Academic
Hospital (CMJAH; Johannesburg, South Africa), where they underwent
a curative hysterectomy or radiotherapy. Clinical information on
the patients was obtained from questionnaires and hospital files.
None of the patients had received any chemotherapy or radiotherapy
prior to sample collection. The tumors of all patients were
squamous cell carcinoma. The majority of the patients had
late-stage disease, five had early-stage disease and the disease
stage was unknown for one patient. The healthy controls were staff
members at CMJAH. All blood donors provided written informed
consent and the study was approved by the Human Research Ethics
Committee of University of Witwatersrand (Johannesburg, South
Africa; no. M110230).
Irradiation and micronucleus assay
Lymphocyte cultures were established by adding 0.5
ml heparinized blood to 4.5 ml RPMI-1640 medium (BioWhittaker,
Walkersville, MD, USA) supplemented with 13% foetal bovine serum
(Gibco-BRL, Invitrogen Life Technologies, Inc., New York, NY, USA)
and antibiotics (50 U/ml penicillin and 50 mg/ml streptomycin;
Gibco-BRL) in tissue culture flasks (25 cm2). The medium
was pre-warmed to 37°C and gassed (5% CO2/95% air). The
cells were exposed to irradiation at the Radiation Oncology Unit of
CMJAH. Culture flasks were placed in a Phantom-water tank
(PolyScience, Warrington, PA, USA) at room temperature and
irradiated with X-rays using a 6 MV photon beam from a medical
linear accelerator (Siemens Healthcare, Erlangen, Germany). Culture
flasks were placed 100 cm away from the radiation source with an
angle of 90 degrees. The field size at the depth of the sample was
10×10 cm. Samples were irradiated with 2 Gray (Gy) and 4 Gy at a
dose rate of ~1.33 Gy/min. A 0 Gy dose was used for the
sham-irradiated control. For each irradiation dose, two co-cultures
were set up. Immediately after irradiation, the lymphocytes were
stimulated with 100 µl phytohaemagglutinin (1-mg/ml stock
solution; Sigma-Aldrich, St Louis, MO, USA) and 23 h later, 20
µl cytochalasin B (stock solution of 1.5 mg/ml;
Sigma-Aldrich) was added to block cytokinesis. Cells were harvested
at 70 h after stimulation using a cold (4°C) hypotonic shock with 7
ml 0.075 M KCl (Merck, Darmstadt, Germany). This was followed by
fixation in methanol/acetic acid/Ringer's solution (0.9% NaCl)
(4:1:5) (Merck) at 4°C overnight. Subsequently, cells were fixed
another three times with methanol/acetic acid (4:1) (Merck). Cell
suspensions were dropped onto coded slides and stored at 4°C
overnight. Slides were mounted with vectashield containing DAPI
(Vector Laboratories, Brussels, Belgium) prior to automatized
scanning using the Metafer 4 platform (MetaSystems, Altlussheim,
Germany) (28,32).
Scoring
Microscopic analysis was performed with the Metafer
4 platform connected to a motorized Zeiss AxioImager M1 microscope
(Zeiss, Gottingen, Germany). The MetaSystems MNScore software
module identifies binucleated cells and displays them in an image
gallery with the quantified MN count per cell (28,32).
The present study used the parameters of the classifier of Willems
et al (32) with minor
adjustments. The system allows for the use of three different
scoring methods, involving varying degrees of visual validation of
automated scores. The first is the 'fully-automated' scoring
method, in which MN counts are obtained directly by the MNScore
module (32). The second is a
'semi-automated' scoring method which has been discussed in other
publications (26,27,38).
In the present study, this scoring method, which only corrects
false positive MN, was referred to as semi-automated A. For
additional validation, the present study introduced a third scoring
method, referred to as semi-automated B. In this method, every
binucleated (BN) cell (with and without MN) was observed in the
image gallery and false negative MN were corrected, in addition to
the false positive MN corrected in semi-automated A. For each
sample, 'fully-automated', 'semi-automated A' and 'semi-automated
B' MN scores were determined by two experienced scorers. The
average number of BN cells per data-point was 1,600. Data-points
(per patient/per irradiation dose) with <500 BN were not
included. All results were normalized to the MN frequency in 1,000
BN cells.
The nuclear division index (NDI) was also calculated
according to the following formula: NDI = (N1 + 2N2 + 3N3 +
4N4)/Ntotal, with N1-N4 being the number of cells with 1–4 nuclei
and Ntotal the total number of cells scored (Ntotal = 500).
Statistical analysis
Statistical analysis was performed using Graphpad
Prism 6 (GraphPad Inc., La Jolla, CA, USA). Differences between
means of MN counts in the various groups were tested for
significance with the Mann-Whitney U-test. This statistical test
was used as it is a non-parametric, distribution-free test that is
suitable for the comparison of groups with small sizes where no
underlying distribution can be assumed. Values are expressed as the
mean MN of a patient group/irradiation dose. P<0.05 was
considered to indicate a statistically significant difference
between values.
Results
Establishment of an MN scoring method for
assessing chromosomal radiosensitivity of cervical cancer patients
vs. that of healthy controls
MN frequencies of cervical cancer patients were
compared to those of healthy controls using the three different
scoring methods of the Metafer 4 system. Radiation-induced MN
yields were calculated by subtracting spontaneous MN yields from MN
yields in irradiated cells. Spontaneous MN values and
radiation-induced values for 2 Gy and 4 Gy are listed in Table I. Using the automated and
'semi-automated A' scoring method, no significant differences were
detected between patients and controls. According of the results
obtained with the 'semi-automated B' scoring method, patients with
cervical cancer had clearly higher MN values compared to those of
controls for all radiation doses tested; the difference between the
groups was significant at 2 Gy (P=0.0075) and 4 Gy (P=0.0059).
 | Table ISpontaneous and radiation-induced
chromosomal radiosensitivity values for controls (n=20) and
cervical cancer patients (n=35) determined by micronucleus assay
and evaluated using three scoring methods. |
Table I
Spontaneous and radiation-induced
chromosomal radiosensitivity values for controls (n=20) and
cervical cancer patients (n=35) determined by micronucleus assay
and evaluated using three scoring methods.
| Group | Automated
| Semi-Automated A
| Semi-Automated B
|
|---|
| 0 Gy | 2 Gy | 4 Gy | 0 Gy | 2 Gy | 4 Gy | 0 Gy | 2 Gy | 4 Gy |
|---|
| Controls |
| Mean | 56 | 125 | 323 | 10 | 115 | 317 | 13 | 155 | 454 |
| SEM | 8 | 8 | 13 | 1 | 5 | 11 | 1 | 6 | 9 |
| Patients |
| Mean | 66 | 144 | 320 | 12 | 124 | 327 | 14 | 179a | 506a,b |
| SEM | 7 | 9 | 14 | 1 | 4 | 10 | 1 | 5 | 12 |
HIV-positive cervical cancer patients
have increased chromosomal radiosensitivity compared with that of
HIV-negative cervical cancer patients and healthy controls
To investigate whether the HIV status affects the
chromosomal radiosensitivity of cervical cancer patients, the group
of cervical cancer patients was divided into HIV-positive and
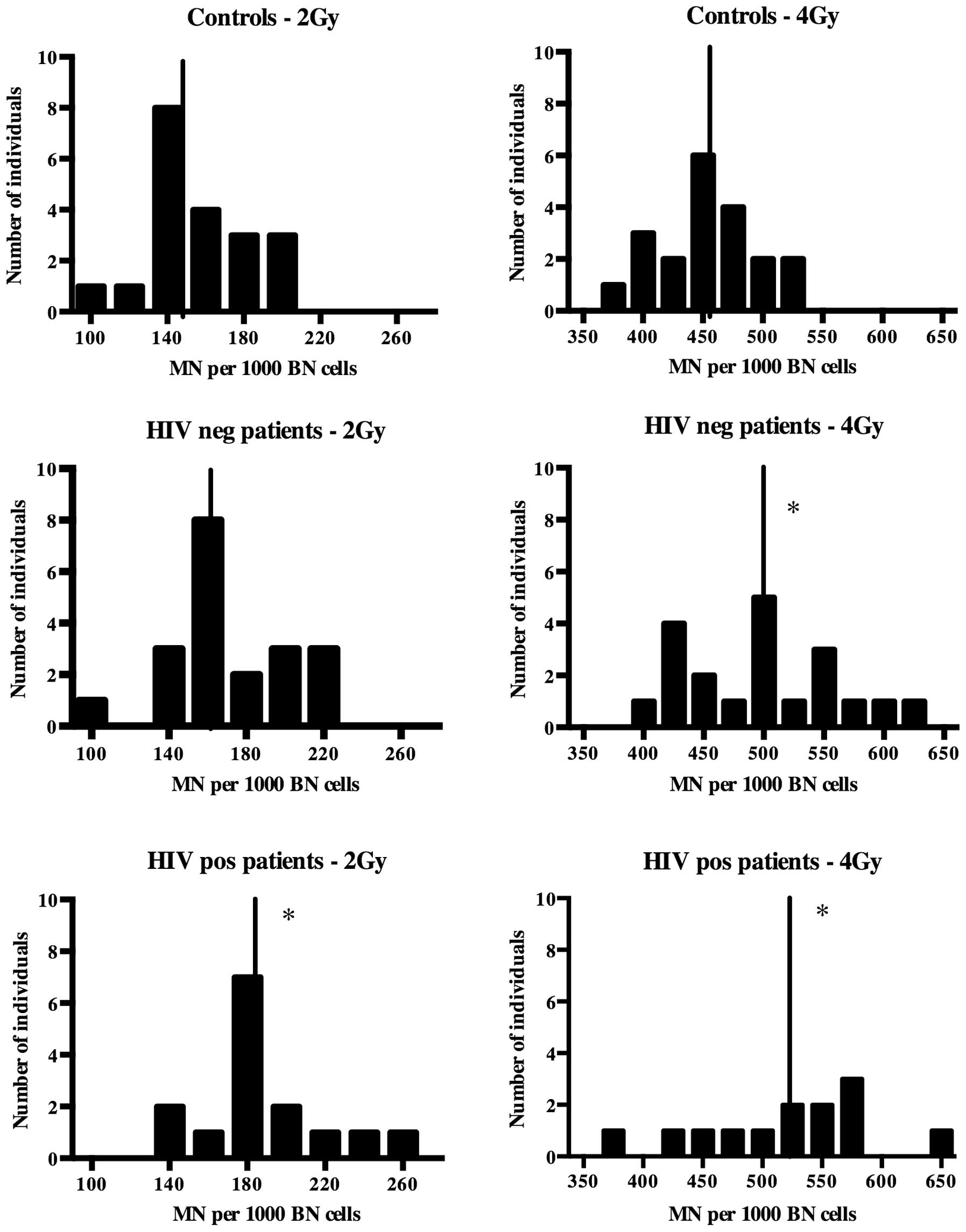
HIV-negative patients. Based on the results shown in Table I, the 'semi-automated B' scoring
method was used to compare HIV-positive and HIV-negative patients
to controls. The MN values of healthy controls, HIV-positive
patients and HIV-negative patients are presented in Fig. 1. The HIV-negative patients had
clearly higher MN scores and therefore a higher chromosomal
radiosensitivity compared to those of the controls; however, the
difference was only significant at 4 Gy (P=0.037). For 2 Gy, there
was no significant difference between HIV-negative cancer patients
and controls (P=0.060), while there was a clear shift towards
higher MN values in the patient group (Fig. 1).
In the HIV-positive patient group, two samples with
insufficient BN measured at 4 Gy were excluded from the analysis.
Although differences were not statistically significant, the
HIV-positive patients had higher MN values than the HIV-negative
patients. The HIV-positive patients had significantly higher
radiation-induced MN values than the healthy controls at 2 Gy
(P=0.006) and 4 Gy (P=0.008).
HIV-positive cervical cancer patients
have lower NDIs than HIV-negative cervical cancer patients and
healthy controls
To evaluate the quality of the MN assay in the
groups of the present study, the nuclear division index was
calculated. The healthy controls had NDIs of 2.170, 2.073 and 1.668
at 0, 2 and 4 Gy, respectively, while the cancer patients had NDIs
of 2.117, 1.883 and 1.535 at these radiation doses, respectively.
The differences in NDI were statistically significant between the
two groups at 2 and 4 Gy (P=0.0091 and P=0.0182, respectively). The
HIV-positive cancer patients had the lowest NDIs among all groups.
The NDIs for HIV-positive versus HIV-negative patients were 2,074;
1,842; 1,529 vs 2,160; 1,928; 1,535. The NDI of the HIV-positive
group was lower than the other groups, but not significantly.
Discussion
The aim of the present study was to compare the
chromosomal radiosensitivity of South African cervical cancer
patients with that of healthy controls using the MN assay. The
development of the MNScore software module by MetaSystems has
allowed for the automation of MN scoring (25). The system has been documented in
several biodosimetric and cancer-associated studies and allows for
the application of various scoring methods that involve varying
degrees of visual validation of automated scores (26–32).
The presence of apoptotic nuclei and a wide range in cell size have
been mentioned as factors impairing the efficiency of the Metafer
system (26,29). Another challenge noted is that the
system 'may fail to identify all MN if they are close or attached
to the main nuclei or if there are more than one MN in the same BN
cell' (29). The majority of the
patient group in the present study had late-stage cervical cancer,
which may have contributed to apoptosis and variation in cell size;
furthermore, the doses of irradiation administered in vitro
may have resulted in multiple MN. For these reasons, the present
study included a 'semi-automated B' scoring method as an extra
validation step to correct for false positive as well as false
negative MN in all BN cells detected. While 'semi-automated B'
scoring using the Metafer platform is more time-consuming than
'semi-automated A' scoring, it is more rapid than manual scoring
under a microscope. Furthermore, the Metafer system has additional
benefits, including the less subjective BN screening and the
generation of a full image gallery, which can be archived as a
'virtual slide' that can be re-analyzed whenever necessary. The
Metafer platform has been used in two similar population studies on
breast and prostate cancer populations (30,31).
Using the automated scoring only, Varga et al (30,31)
were able to clearly distinguish between breast cancer patients and
controls but not between prostate cancer patients and controls. To
the best of our knowledge, Metafer scoring has not previously been
used to investigate a cervical cancer population. In the present
study, when cervical cancer patients were compared to controls
using the 'fully-automated' and 'semi-automated A' method, no
differences were observed between patients and controls. However,
the 'semi-automated B' scoring method determined significantly
higher MN values for the patient group as compared to those of the
control group at 2 and 4 Gy. At the 4 Gy dose, a significant
percentage of BN had multiple MN, which was missed by the
'fully-automated' and 'semi-automated A' scoring methods. Another
reason for the inaccuracy of the 'fully-automated' and
'semi-automated A' methods may have been the high level of cell
debris that was noted on the slides of the cancer patients, which
was a possible result of increased apoptosis due to elevated
radiosensitivity or other types of cellular stress associated with
late-stage disease. The lower yield of binucleated cells in the
cancer group, which may have also been a result of apoptosis or
cellular stress, was reflected by the significantly lower NDI
compared to that in the healthy control group. All of these
circumstances may have resulted in false positive MN that may have
affected the automated scoring.
The results of the present study indicated an
increased chromosomal radiosensitivity in patients with cervical
cancer compared to that of controls. Previous studies on the
chromosomal radiosensitivity of lymphocytes of cervical cancer
patients have been inconclusive. In a study by Ban et al
(22) using the MN assay, patients
were found to have lower MN frequencies than controls. However, the
blood samples of a large proportion of the patients were taken
after or during radiotherapy treatment. This resulted in high
spontaneous MN values, which affected the radiation-induced MN
values. It was also suggested by the authors that the lower MN
values determined in cervical cancer patients may be the result of
an adaptive response of the patients to clinical therapy. Encheva
et al (39), who performed
a similar study to the present one, compared MN values of
lymphocytes from 40 gynecological cancer patients (23 with cervical
and 17 with endometrial cancer combined into one group) to those of
10 healthy control subjects. The lymphocytes from the combined
gynecological cancer patients and the controls had similar MN
values after exposure to a dose of 1.5 Gy in vitro. The
inclusion of 17 patients with endometrial cancer makes it difficult
to draw conclusions on the chromosomal radiosensitivity of cervical
cancer patients alone. The present study was performed on a cohort
of patients with cervical cancer, mainly at the late stage.
It is widely accepted that inherited genes have a
role in cervical cancer susceptibility, as only a fraction of women
with HPV infection develop cervical cancer, and the disease shows
familial clustering (40).
HPV-induced cervical carcinogenesis is a complex, multi-faceted
process that has yet to be fully elucidated (7). While numerous studies on cervical
cancer have focused on genes involved in the immune response
(41–43), cervical cancer-associated genes
involved in DNA damage repair are also an area of interest. Recent
studies have shown associations with genes involved in DNA damage
repair and a risk for cervical cancer (9–12,44).
In addition, studies have shown that Fanconi Anemia (FA) patients,
who have deficient DNA damage repair mechanisms, are more
susceptible to HPV-positive head and neck squamous cell carcinomas
compared to non-FA patients with the same lesions (45). Park et al (46) reported an association between HPV
and the FA pathway. Defects in DNA damage-response genes are known
to affect chromosomal radiosensitivity (47). The increased chromosomal
radiosensitivity observed in the present study suggested deficient
DNA damage response signaling, which may have had a role in the
genesis of cervical cancer. The exact role of DNA damage repair
genes in the development and progression of cervical cancer remains
to be fully elucidated. Evidence from a study using retroviruses
showed that when a virus was integrated into the host's genome, a
double-strand break (DSB) was formed, causing a DNA damage response
similar to that observed when cells were exposed to ionizing
radiation (48). If these DSB are
not repaired and the integration process is not properly regulated,
it can result in genomic instability, which can lead to
carcinogenesis (12). It was also
reported that the preferential targets of HPV integration are
common fragile sites (49). DNA
damage repair genes, including ATR, BRCA1, CHK1, have been shown to
have a role in fragile site stability and expression (50–53).
There may be a link between compromised DNA damage repair, fragile
site stability and susceptibility to HPV integration and subsequent
carcinogenesis.
A previous study by our group showed that
HIV-positive individuals were more radiosensitive than non-infected
individuals (33). HIV infection
is common in Africa and the epidemiological link between HIV and
cervical cancer implies that a large number of women seeking
treatment (often radiotherapy) of the disease are HIV-positive. For
this reason, the present study examined a group of HIV-positive
cervical cancer patients as part of the study cohort. In two of the
HIV-positive patients, the number of BN after the 4 Gy dose was too
low for the evaluation of the MN score. This was likely due to HIV
infection, which affects the CD4 count, in combination with the
late-stage cervical cancer, causing cells to not withstand the
cytotoxicity of a dose as high as 4 Gy. HIV-positive cervical
cancer patients had higher MN values than HIV-negative cervical
cancer patients, despite the differences not being significant.
This suggested that HIV infection enhanced the radiosensitivity of
cervical cancer patients. The MN values of HIV-positive patients
were significantly higher than those of the healthy controls at 2
Gy and 4 Gy. These results were consistent with those of Baeyens
et al (33).
The present study showed that when using the Metafer
system on cancer populations with advanced disease or HIV, the
'semi-automated B' scoring method yields the most reliable results.
This technique may also be useful for the assessment of the
radiosensitivity of population groups with other types of cancer.
The results also showed that cervical cancer patients had higher MN
values than those of the controls, suggesting increased chromosomal
radiosensitivity. The findings of the present study confirmed that
cervical cancer patients seeking radiotherapy who are HIV-positive
may form a distinct group that requires individualized treatments.
It may be useful to follow up the in vitro data with the
clinical response of cervical cancer patients with HIV infection
undergoing radiotherapy. Evidence suggested that these patients
suffer from increased radiation-induced side-effects; however,
further investigation is required to confirm this (54–56).
From the results of the present study, it can be deduced that when
performing studies in developing countries, factors such as the HIV
status should be considered. Further studies are required to
investigate the link between chromosomal radiosensitivity, DNA
damage repair genes and the underlying mechanisms of susceptibility
to HPV-induced carcinogenesis. Such studies may identify a marker
for increased cervical cancer risk in women with HPV infection and
may assist in the identification of individuals requiring regular
pap-smears, which may reduce medical expenses in resource-limited
countries such as South Africa.
Acknowledgments
The present study was supported by the iThemba
Laboratory for Accelerated Based Science (LABS), Nuclear
Technologies in Medicine and the Biosciences Initiative [NTeMBI; a
national technology platform developed and managed by the South
African Nuclear Energy Corporation (NECSA)], the 'Competitive
Support for Unrated Researchers' grant (no. 78798) of the National
Research Foundation, South Africa and the 'VLIR Own Initiative
Programme' between Belgium and South Africa (no. ZEIN2011 pr387).
The authors wish to thank all donors who participated in the
present study.
References
|
1
|
IARC: International agency for research on
cancer: GLOBOCAN report. 2012.
|
|
2
|
Bosch FX, Lorincz A, Muñoz N, Meijer CJ
and Shah KV: The causal relation between human papillomavirus and
cervical cancer. J Clin Pathol. 55:244–265. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Walboomers JM, Jacobs MV, Manos MM, Bosch
FX, Kummer JA, Shah KV, Snijders PJ, Peto J, Meijer CJ and Muñoz N:
Human papillomavirus is a necessary cause of invasive cervical
cancer worldwide. J Pathol. 189:12–19. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Anorlu RI: Cervical cancer: the
sub-Saharan African perspective. Reprod Health Matters. 16:41–49.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sitas F, Parkin DM, Chirenje M, Stein L,
Abratt R and Wabinga H: Part II: Cancer in indigenous
africans-causes and control. Lancet Oncol. 9:786–795. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
DOHSA: South African department of health;
2014
|
|
7
|
Woodman CB, Collins SI and Young LS: The
natural history of cervical HPV infection: Unresolved issues. Nat
Rev Cancer. 7:11–22. 2007. View
Article : Google Scholar
|
|
8
|
Magnusson PK, Lichtenstein P and
Gyllensten UB: Heritability of cervical tumours. Int J Cancer.
88:698–701. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wang M, Chu H, Wang S, Wang M, Wang W, Han
S and Zhang Z: Genetic variant in APE1 gene promoter contributes to
cervical cancer risk. Am J Obstet Gynecol. 209:360 e1–7. 2013.
View Article : Google Scholar
|
|
10
|
Pérez LO, Crivaro A, Barbisan G, Poleri L
and Golijow CD: XRCC2 R188H (rs3218536), XRCC3 T241 M (rs861539)
and R243H (rs77381814) single nucleotide polymorphisms in cervical
cancer risk. Pathol Oncol Res. 19:553–558. 2013. View Article : Google Scholar
|
|
11
|
Bajpai D, Banerjee A, Pathak S, Jain SK
and Singh N: Decreased expression of DNA repair genes (XRCC1,
ERCC1, ERCC2 and ERCC4) in squamous intraepithelial lesion and
invasive squamous cell carcinoma of the cervix. Mol Cell Biochem.
377:45–53. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Oliveira S, Ribeiro J, Sousa H, Pinto D,
Baldaque I and Medeiros R: Genetic polymorphisms and cervical
cancer development: ATM G5557A and p53bp1 C1236 G. Oncol Rep.
27:1188–1192. 2012.
|
|
13
|
Jeggo P and Lavin MF: Cellular
radiosensitivity: How much better do we understand it? Int J Radiat
Biol. 85:1061–1081. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Huo YK, Wang Z, Hong JH, Chessa L, McBride
WH, Perlman SL and Gatti RA: Radiosensitivity of
ataxia-telangiectasia, X-linked agammaglobulinemia and related
syndromes using a modified colony survival assay. Cancer Res.
54:2544–2547. 1994.PubMed/NCBI
|
|
15
|
Jones LA, Scott D, Cowan R and Roberts SA:
Abnormal radio-sensitivity of lymphocytes from breast cancer
patients with excessive normal tissue damage after radiotherapy:
chromosome aberrations after low dose-rate irradiation. Int J
Radiat Biol. 67:519–528. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Parshad R, Sanford KK and Jones GM:
Chromatid damage after G2 phase x-irradiation of cells from
cancer-prone individuals implicates deficiency in DNA repair. Proc
Natl Acad Sci USA. 80:5612–5616. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Baeyens A, Thierens H, Claes K, Poppe B,
Messiaen L, De Ridder L and Vral A: Chromosomal radiosensitivity in
breast cancer patients with a known or putative genetic
predisposition. Br J Cancer. 87:1379–1385. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Riches AC, Bryant PE, Steel CM, Gleig A,
Robertson AJ, Preece PE and Thompson AM: Chromosomal
radiosensitivity in G2-phase lymphocytes identifies breast cancer
patients with distinctive tumour characteristics. Br J Cancer.
85:1157–1161. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Terzoudi GI, Jung T, Hain J, Vrouvas J,
Margaritis K, Donta-Bakoyianni C, Makropoulos V, Angelakis P and
Pantelias GE: Increased G2 chromosomal radiosensitivity in cancer
patients: The role of cdk1/cyclin-B activity level in the
mechanisms involved. Int J Radiat Biol. 76:607–615. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Scott D, Spreadborough A, Levine E and
Roberts SA: Genetic predisposition in breast cancer. Lancet.
344:14441994. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Baria K, Warren C, Roberts SA, West CM and
Scott D: Chromosomal radiosensitivity as a marker of predisposition
to common cancers? Br J Cancer. 84:892–896. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ban S, Konomi C, Iwakawa M, Yamada S, Ohno
T, Tsuji H, Noda S, Matui Y, Harada Y, Cologne JB and Imai T:
Radiosensitivity of peripheral blood lymphocytes obtained from
patients with cancers of the breast, head and neck or cervix as
determined with a micronucleus assay. J Radiat Res. 45:535–541.
2004. View Article : Google Scholar
|
|
23
|
Bozsakyová E, Wsólová L and Chalupa I:
Spontaneous and gamma-ray-induced sister chromatid exchanges in
patients with carcinoma of cervix uteri. Int J Radiat Biol.
81:177–185. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Gabelova A, Farkasova T, Gurska S,
Machackova Z, Lukacko P and Witkovsky V: Radiosensitivity of
peripheral blood lymphocytes from healthy donors and cervical
cancer patients; the correspondence of in vitro data with the
clinical outcome. Neoplasma. 55:182–191. 2008.PubMed/NCBI
|
|
25
|
Schunck C, Johannes T, Varga D, Lörch T
and Plesch A: New developments in automated cytogenetic imaging:
Unattended scoring of dicentric chromosomes, micronuclei, single
cell gel electrophoresis and fluorescence signals. Cytogenet Genome
Res. 104:383–389. 2004. View Article : Google Scholar
|
|
26
|
Bolognesi C, Balia C, Roggieri P, et al:
Micronucleus test for radiation biodosimetry in mass casualty
events: Evaluation of visual and automated scoring. Radiation
Measurements. 46:169–175. 2011. View Article : Google Scholar
|
|
27
|
Baeyens A, Swanson R, Herd O, Ainsbury E,
Mabhengu T, Willem P, Thierens H, Slabbert JP and Vral A: A
semi-automated micronucleus-centromere assay to assess low-dose
radiation exposure in human lymphocytes. Int J Radiat Biol.
87:923–931. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Varga D, Johannes T, Jainta S, Schuster S,
Schwarz-Boeger U, Kiechle M, Patino Garcia B and Vogel W: An
automated scoring procedure for the micronucleus test by image
analysis. Mutagenesis. 19:391–397. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Fenech M, Kirsch-Volders M, Rossnerova A,
Sram R, Romm H, Bolognesi C, Ramakumar A, Soussaline F, Schunck C
and Elhajouji A: HUMN project initiative and review of validation,
quality control and prospects for further development of automated
micronucleus assays using image cytometry systems. Int J Hyg
Environ Health. 216:541–552. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Varga D, Michel I, Patino-Garcia B, Paiss
T, Vogel W and Maier C: Radiosensitivity detected by the
micronucleus test is not generally increased in sporadic prostate
cancer patients. Cytogenet Genome Res. 111:41–45. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Varga D, Hoegel J, Maier C, Jainta S,
Hoehne M, Patino-Garcia B, Michel I, Schwarz-Boeger U, Kiechle M,
Kreienberg R and Vogel W: On the difference of micronucleus
frequencies in peripheral blood lymphocytes between breast cancer
patients and controls. Mutagenesis. 21:313–320. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Willems P, August L, Slabbert J, Romm H,
Oestreicher U, Thierens H and Vral A: Automated micronucleus (MN)
scoring for population triage in case of large scale radiation
events. Int J Radiat Biol. 86:2–11. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Baeyens A, Slabbert JP, Willem P, Jozela
S, Van Der Merwe D and Vral A: Chromosomal radiosensitivity of HIV
positive individuals. Int J Radiat Biol. 86:584–592. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
STATSSA: Statistics South Africa: Mid-year
population estimates South Africa. 2013.
|
|
35
|
CDC: Centre for disease control:
Classification system for HIV infection and expanded surveillance
case definition for AIDS among adolescents and adults. 1993.
|
|
36
|
Firnhaber C, Van Le H, Pettifor A, Schulze
D, Michelow P, Sanne IM, Lewis DA, Williamson AL, Allan B, Williams
S, et al: Association between cervical dysplasia and human
papillomavirus in HIV seropositive women from Johannesburg South
Africa. Cancer Causes Control. 21:433–443. 2010. View Article : Google Scholar :
|
|
37
|
Heard I, Schmitz V, Costagliola D, Orth G
and Kazatchkine MD: Early regression of cervical lesions in
HIV-seropositive women receiving highly active antiretroviral
therapy. AIDS. 12:1459–1464. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Thierens H, Vral A, Vandevoorde C,
Vandersickel V, de Gelder V, Romm H, Oestreicher U, Rothkamm K,
Barnard S, Ainsbury E4, et al: Is a semi-automated approach
indicated in the application of the automated micronucleus assay
for triage purposes? Radiat Prot Dosimetry. 159:87–94. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Encheva E, Deleva S, Hristova R,
Hadjidekova V and Hadjieva T: Investigating micronucleus assay
applicability for prediction of normal tissue intrinsic
radiosensitivity in gynecological cancer patients. Rep Pract Oncol
Radiother. 17:24–31. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Magnusson PK, Sparén P and Gyllensten UB:
Genetic link to cervical tumours. Nature. 400:29–30. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Chen D, Hammer J, Lindquist D, Idahl A and
Gyllensten U: A variant upstream of HLA-DRB1 and multiple variants
in MICA influence susceptibility to cervical cancer in a Swedish
population. Cancer Med. 3:190–198. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Jiang J, Li N, Shen Y, Liu J, Liu L, Du J,
Lei Y, Wen Y, Yang L, Guo L, et al: Genetic variants in HLA-DP/DQ
contribute to risk of cervical cancer: A two-stage study in Chinese
women. Gynecol Oncol. 129:401–405. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Chen D, Juko-Pecirep I, Hammer J, Ivansson
E, Enroth S, Gustavsson I, Feuk L, Magnusson PK, McKay JD, Wilander
E and Gyllensten U: Genome-wide association study of susceptibility
loci for cervical cancer. J Natl Cancer Inst. 105:624–633. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Wang SS, Gonzalez P, Yu K, Porras C, Li Q,
Safaeian M, Rodriguez AC, Sherman ME, Bratti C, Schiffman M, et al:
Common genetic variants and risk for HPV persistence and
progression to cervical cancer. PLoS One. 5:e86672010. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Kutler DI, Wreesmann VB, Goberdhan A,
Ben-Porat L, Satagopan J, Ngai I, Huvos AG, Giampietro P, Levran O,
Pujara K, et al: Human papillomavirus DNA and p53 polymorphisms in
squamous cell carcinomas from Fanconi anemia patients. J Natl
Cancer Inst. 95:1718–1721. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Park JW, Pitot HC, Strati K, Spardy N,
Duensing S, Grompe M and Lambert PF: Deficiencies in the Fanconi
anemia DNA damage response pathway increase sensitivity to
HPV-associated head and neck cancer. Cancer Res. 70:9959–9968.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Iarmarcovai G, Bonassi S, Botta A, Baan RA
and Orsière T: Genetic polymorphisms and micronucleus formation: a
review of the literature. Mutat Res. 658:215–33. 2008. View Article : Google Scholar
|
|
48
|
Skalka AM and Katz RA: Retroviral DNA
integration and the DNA damage response. Cell Death Differ.
12(Suppl 1): 971–978. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Thorland EC, Myers SL, Gostout BS and
Smith DI: Common fragile sites are preferential targets for HPV16
integrations in cervical tumors. Oncogene. 22:1225–1237. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Casper AM, Nghiem P, Arlt MF and Glover
TW: ATR regulates fragile site stability. Cell. 111:779–789. 2002.
View Article : Google Scholar
|
|
51
|
Arlt MF, Xu B, Durkin SG, Casper AM,
Kastan MB and Glover TW: BRCA1 is required for common-fragile-site
stability via its G2/M checkpoint function. Mol Cell Biol.
24:6701–6709. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Durkin SG, Arlt MF, Howlett NG and Glover
TW: Depletion of CHK1, but not CHK2, induces chromosomal
instability and breaks at common fragile sites. Oncogene.
25:4381–4388. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Glover TW, Arlt MF, Casper AM and Durkin
SG: Mechanisms of common fragile site instability. Hum Mol Genet.
14(Spec No. 2): R197–R205. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Housri N, Yarchoan R and Kaushal A:
Radiotherapy for patients with the human immunodeficiency virus:
Are special precautions necessary? Cancer. 116:273–283. 2010.
View Article : Google Scholar
|
|
55
|
Shrivastava SK, Engineer R, Rajadhyaksha S
and Dinshaw KA: HIV infection and invasive cervical cancers,
treatment with radiation therapy: Toxicity and outcome. Radiother
Oncol. 74:31–35. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Gichangi P, Bwayo J, Estambale B, Rogo K,
Njuguna E, Ojwang S and Temmerman M: HIV impact on acute morbidity
and pelvic tumor control following radiotherapy for cervical
cancer. Gynecol Oncol. 100:405–411. 2006. View Article : Google Scholar
|