Introduction
Primary mediastinal large B cell lymphoma (PMLBCL)
is a distinct subtype of aggressive B cell lymphoma, accounting for
2–3% of all non-Hodgkin's lymphomas, and predominantly occurring in
women and 30–39-year-old patients (1,2).
PMLBCL was originally classified as a subtype of diffuse large B
cell lymphoma. However, in 2008, PMLBCL was identified as a
distinctive entity by the World Health Organization owing to its
unique clinical and biological features (3). PMLBCL originates in the mediastinal
region, and usually forms a bulky mass that leads to local
compression and infiltration of the lungs, pleura and pericardium.
Common symptoms of PMLBCL include cough, dyspnea, dysphagia, airway
compromise, great vessel compromise and superior vena cava syndrome
(1,4).
The standard first-line therapy for patients with
PMLBCL is unclear because of the lack of randomized trials. The
recommended standard treatments of PMLBCL are currently: Rituximab,
cyclophosphamide, doxorubicin, vincristine and prednisolone
(R-CHOP); rituximab, etoposide, doxorubicin, cyclophosphamide,
vincristine, prednisolone and bleomycin (R-VACOP-B); rituximab,
methotrexate, doxorubicin, cyclophosphamide, vincristine,
prednisolone and bleomycin (R-MACOP-B); dose-dense CHOP; and
dose-adjusted etoposide, prednisone, vincristine cyclophosphamide,
doxorubicin and rituximab (DA-EPOCH-R). Consolidative radiotherapy
(RT) is recommended for patients receiving R-CHOP and R-V/MACOP-B
regimens. For patients achieving a complete metabolic response
after more intensive regimens, such as DA-EPOCH-R, consolidative RT
may be excluded (5,6). However, as this recommendation is
based on a small phase II study, the omission of consolidative RT
requires investigation in large randomized trials (7).
At present, there is no consensus on prognostic
models in PMLBCL. A retrospective study of patients in the British
Columbia Cancer Agency lymphoma database showed that poor
performance status was the only factor predicting poor survival in
patients treated with CHOP or V/MACOP-B regimens (8). However, a multicenter retrospective
study conducted by Todeschini et al (9) showed that the achievement of complete
remission and treatment with a V/MACOP-B regimen contributed to
improved survival. In the rituximab era, a retrospective study
conducted by Yang et al (10) found that the inclusion of rituximab
in the induction chemotherapy regimen was independently associated
with superior overall survival (OS), and age >60 years was
independently associated with poor OS. A multicenter retrospective
study conducted by Aoki et al (11) showed that for patients receiving
R-CHOP without consolidative RT, stage III/IV disease and the
presence of pleural or pericardial effusion were associated with
inferior progression-free survival (PFS). In addition, patients
without pleural or pericardial effusion and with low International
Prognostic Index (IPI) scores had higher OS and PFS rates compared
with those with pleural or pericardial effusion and high IPI
scores. In another multicenter retrospective study, conducted by
Zhou et al (12), it was
reported that patients with IPI >1, stage III–IV disease, Ki-67
expression ≥70% and maximum standardized uptake values of positron
emission tomography imaging at diagnosis of >11.6 had
significantly poorer survival. By contrast, patients with higher
lymphocyte/monocyte ratios and multiple myeloma 1 protein
expression had significantly improved survival. The factors
identified to affect survival and treatment response vary among
studies. Therefore, the present study was designed to assess the
factors that affect OS and PFS in patients with PMLBCL at a single
institute in Taiwan.
Materials and methods
Patients
The lymphoma registry at Linkou Chang Gung Memorial
Hospital (Taipei, Taiwan) between January 2004 and June 2020 was
screened. All patients with a diagnosis of PMLBCL were included and
patients with a diagnosis of other types of lymphoma were excluded.
The medical records of patients newly diagnosed with PMLBCL were
retrospectively reviewed. The study was conducted in accordance
with the principles of the Declaration of Helsinki. The Chang Gung
Medical Foundation Institutional Review Board approved the study
protocol (ref. no. 202100653B0).
Demographic and clinical data
Patients diagnosed with PMLBCL based on biopsy
specimens of lymph nodes or mediastinal masses were included
(13). The data collected included
age, sex, Eastern Cooperative Oncology Group (ECOG) performance
status (14), disease stage, the
presence of B symptoms (fever, weight loss and sweats), serum
lactate dehydrogenase (LDH) levels, mediastinal mass size, IPI
(15), first-line treatment
modality, treatment response and survival status. Disease stage was
determined using the Ann Arbor system, and a maximum mediastinal
mass diameter larger than one-third of the thoracic diameter or
>10 cm was defined as bulky disease (16). Intensive chemotherapy was defined as
DA-EPOCH-R, R-MACOP-B or similar regimens, whereas less intensive
chemotherapy was defined as R-CHOP or similar regimens. OS was
defined as the time from diagnosis to death from any cause. PFS was
defined as the time from diagnosis to disease progression or death,
whichever occurred first. Treatment response was assessed according
to the Lugano Classification (17).
Statistical analysis
Descriptive statistics are used for baseline
characteristics, which are expressed as count (percentage) or
median (range). Survival curves were estimated using the
Kaplan-Meier method and compared using the log-rank test based on
sex (male vs. female), disease stage (stage I/II vs. III/IV), age
(≤60 vs. >60 years), IPI score (≤1 vs. >1), treatment
modality (low- vs. high-intensity chemotherapy; with vs. without
consolidative RT) and treatment response (complete response
achieved vs. not achieved). P<0.05 was considered to indicate a
statistically significant difference. Data analyses were performed
using IBM SPSS Statistics 26 software (IBM Corp.).
Results
Patient characteristics
A total of 72 patients were included in the
analysis. The median age of the patients was 28 years (range, 17–78
years), and most of the patients (90.3%) were ≤60 years old. The
study included 34 female and 38 male patients (female-to-male
ratio, 0.89). The majority of the patients had an ECOG performance
status 0–1 (88.9%), early disease (stages I–II, 75%), elevated
levels of serum LDH (69.4%), bulky disease (79.2%) and low-risk
disease (IPI scores 0–1; 87.5%). There were 23 (31.9%) patients
with B symptoms. Regarding initial therapy, 47 (66.2%) patients
received intensive chemotherapy (DA-EPOCH-R, R-MACOP-B or similar
regimens) and 24 (33.8%) received less intensive chemotherapy
(R-CHOP or similar regimens). In addition, more than half of the
patients (56.9%) received consolidative RT. After initial therapy,
57 (83.8%) patients achieved a complete response (Table I). A total of 15 patients had
relapsed or refractory disease.
 | Table I.Demographic and clinical
characteristics of the 72 patients. |
Table I.
Demographic and clinical
characteristics of the 72 patients.
| Characteristic | n (%)a |
|---|
| Median (range) age,
years | 28 (17–78) |
| Age, years |
|
| ≤60 | 65 (90.3) |
|
>60 | 7 (9.7) |
| Sex |
|
|
Female | 34 (47.2) |
|
Male | 38 (52.8) |
| ECOG performance
status |
|
|
0-1 | 64 (88.9) |
|
2-4 | 8 (11.1) |
| Stage |
|
|
I–II | 54 (75) |
|
III–IV | 18 (25) |
| B symptoms | 23 (31.9) |
| Elevated LDH | 50 (69.4) |
| Bulky disease | 57 (79.2) |
| IPI |
|
|
0-1 | 63 (87.5) |
| 2 | 8 (11.1) |
|
3-5 | 1 (1.4) |
|
Chemotherapyb |
|
| High
intensity | 47 (66.2) |
| Low
intensity | 24 (33.8) |
| Radiotherapy |
|
|
Yes | 41 (56.9) |
| No | 31 (43.1) |
| Complete
responsec | 57 (83.8) |
Overall survival
The mean OS for the entire cohort was 171.40 months
[95% confidence interval (CI): 154.56, 188.23]. Regarding sex,
female patients had a mean OS of 192.78 months (95% CI: 177.70,
207.86) and 5-year OS rate of 93.8%, while male patients had a mean
OS of 152.31 months (95% CI: 124.82, 179.80) and 5-year OS rate of
72.8% (P=0.017; Fig. 1A). Regarding
age, patients aged ≤60 years had a mean OS of 180.00 months (95%
CI: 164.43, 195.56) and 5-year OS rate of 87.0%. However, patients
aged >60 years had a mean OS of only 80.57 months (95% CI:
16.69, 144.45) and a 5-year OS rate of 42.9%. These results
indicate that younger patients had significantly improved OS
compared with older patients (P<0.001; Fig. 1B). Regarding disease stage, patients
with stage I–II disease had a mean OS of 178.78 months (95% CI:
161.34, 196.21) and 5-year OS rate of 86.7%, while patients with
stage III–IV disease had a mean OS of 149.35 months (95% CI:
108.71, 189.99) and 5-year OS rate of 70.7%. The difference between
the early and advanced disease groups was not found to be
significant (P=0.129; Fig. 1C).
When patients were analyzed according to their IPI scores, patients
with an IPI score ≤1 had a mean OS of 179.08 months (95% CI:
162.95, 195.20) and 5-year OS rate of 86.7%. By contrast, patients
with an IPI score >1 had a mean OS of 102.44 months (95% CI:
49.36, 155.53) and 5-year OS rate of 55.6%. A significant
difference was identified between the two groups (P=0.008; Fig. 1D).
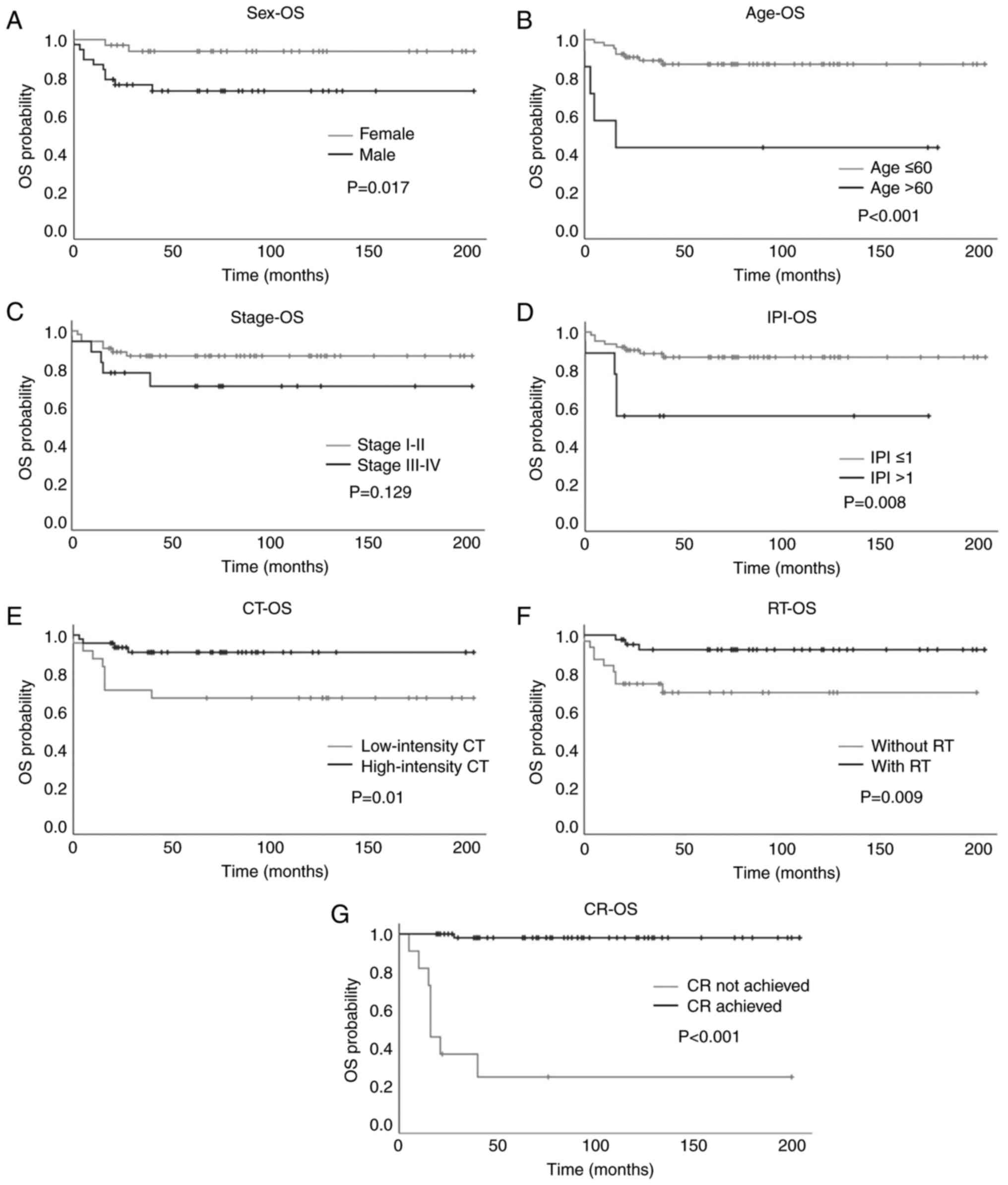 | Figure 1.Kaplan-Meier plots of OS in patients
with primary mediastinal large B-cell lymphoma based on various
prognostic factors. (A) Sex, (B) age, (C) stage, (D) IPI, (E)
intensity of CT, (F) with or without RT and (G) achievement of CR.
OS, overall survival; IPI, International Prognostic Index; CT,
chemotherapy; RT, radiotherapy; CR, complete response. |
With regard to treatment modality, patients treated
with high-intensity chemotherapy had significantly longer OS than
those treated with low-intensity chemotherapy [mean OS, 186.75
months (95% CI: 170.59, 202.91) vs. 140.92 months (95% CI: 105.13,
176.70); 5-year OS rate, 90.9 vs. 66.7%, respectively; P=0.01;
Fig. 1E]. Patients who received
consolidative RT had significantly longer OS than those who did not
[mean OS, 189.94 months (95% CI: 174.64, 205.24) vs. 143.23 months
(95% CI: 111.94, 174.51); 5-year OS rate, 92.3 vs. 69.6%,
respectively; P=0.009, Fig. 1F].
Patients who achieved a complete response had significantly longer
OS than those who did not [mean OS, 200.48 months (95% CI: 193.65,
207.31) vs. 62.33 months (95% CI: 13.47, 111.20); 5-year OS rate,
98.0 vs. 24.2%, respectively; P<0.001; Fig. 1G]. These results indicated that
female sex, age ≤60 years, IPI score ≤1, treatment with
high-intensity chemotherapy and consolidative RT, and achievement
of a complete response were significantly associated with improved
OS (Table II).
| Table II.Prognostic factors for
progression-free survival and overall survival. |
Table II.
Prognostic factors for
progression-free survival and overall survival.
| First author/s,
year |
Progression/event-free survival | Overall
survival | (Refs.) |
|---|
| Present study | Female, age ≤60
years, stage I–II disease, with radiotherapy, CR achievement | Female, age ≤60
years, IPI ≤1, high-intensity chemotherapy, with radiotherapy, CR
achievement | - |
| Savage et
al, 2006 | - | ECOG ≤1 | (8) |
| Todeschini et
al, 2004 | CR achievement,
V/MACOP-B chemotherapy | CR achievement,
V/MACOP-B chemotherapy | (9) |
| Yang et al,
2015 | - | Rituximab
induction, age ≤60 years | (10) |
| Aoki et al,
2014 | Without pleural or
pericardial effusion, IPI <3 | Without pleural or
pericardial effusion, IPI <3 | (11) |
| Zhou et al,
2020 | IPI ≤1, stage I–II
disease, Ki-67 expression <70%, higher lymphocyte/monocyte
ratios, MUM1 expression | IPI ≤1, Ki-67
expression <70%, age ≤60 years, maximum standardized uptake
values of positron emission tomography imaging ≤11.6, higher
lymphocyte/monocyte ratios, MUM1 expression | (12) |
Progression-free survival
The mean PFS for the entire cohort was 159.77 months
(95% CI: 140.65, 178.90). Regarding sex, female patients had a mean
PFS of 180.82 months (95% CI: 159.67, 202.18) and 5-year PFS rate
of 88.2%, whereas male patients had a mean PFS of 141.03 months
(95% CI: 111.53, 170.52) and 5-year PFS rate of 68.4% (P=0.044;
Fig. 2A). Regarding age, patients
aged ≤60 years had a mean PFS time of 167.30 months (95% CI: 148.5,
186.06) and 5-year PFS rate of 81.5%. By contrast, patients aged
>60 years had a mean PFS of 79.57 months (95% CI: 15.06, 144.08)
and 5-year PFS rate of 42.9%. A significant difference in PFS was
identified between patients younger and older than 60 years
(P=0.011; Fig. 2B). Regarding
disease stage, patients with stage I–II disease had a mean PFS of
170.83 months (95% CI: 151.04, 190.63) and 5-year PFS rate of
83.3%, while patients with stage III–IV disease had a mean PFS of
126.56 months (95% CI: 81.68, 171.44) and 5-year PFS rate of 61.1%.
The patients with early disease had a significantly longer PFS than
those with advanced disease (P=0.045; Fig. 2C). In terms of IPI score, patients
with an IPI score ≤1 had a mean PFS of 166.18 months (95% CI:
146.92, 185.45) and 5-year PFS rate of 80.9%, while those with an
IPI score >1 had a mean PFS of 98.78 months (95% CI: 43.04,
154.52) and 5-year PFS rate of 55.6%. No significant difference in
PFS was detected between the two groups (P=0.069; Fig. 2D).
 | Figure 2.Kaplan-Meier plots of PFS in patients
with primary mediastinal large B-cell lymphoma based on various
prognostic factors. (A) Sex, (B) age, (C) stage, (D) IPI, (E)
intensity of CT, (F) with or without RT and (G) achievement of CR.
PFS, progression-free survival; IPI, International Prognostic
Index; CT, chemotherapy; RT, radiotherapy; CR, complete
response. |
With regards to treatment modality, no significant
difference in PFS was detected between patients treated with
high-intensity chemotherapy and those treated with low-intensity
chemotherapy [mean PFS, 170.58 months (95% CI: 149.47, 191.69) vs.
136.71 months (95% CI: 98.62, 174.80); 5-year PFS rate, 82.9 vs.
66.7%; P=0.1, respectively; Fig.
2E]. Patients who received consolidative RT had longer PFS than
those who did not [mean PFS, 180.49 months (95% CI: 161.17, 199.80)
vs. 83.94 months (95% CI: 62.51, 105.36); 5-year PFS rate, 87.7 vs.
64.5%, respectively; P=0.013; Fig.
2F]. Patients who achieved a complete response had longer PFS
than those who did not [mean PFS, 197.47 months (95% CI: 188.58,
206.36) vs. 4.0 months (95% CI: 0.87, 7.13); 5-year PFS rate, 96.5
vs. 0%, respectively; P<0.001; Fig.
2G]. In summary, female sex, early-stage disease, age ≤60
years, treatment with consolidative RT and achievement of a
complete response were found to have a significant association with
longer PFS (Table II).
Discussion
In the present study, several factors were found to
be associated with PMLBCL prognosis, including age, sex, disease
stage, IPI, chemotherapy intensity and initial response. While
other risk factors are well known, male sex has not been reported
as a poor prognostic factor in the literature. Notably, no female
predominance of PMLBCL was observed in the present study, unlike in
other patient populations (2).
There was a slightly higher number of male patients than female
patients in the present study. Interestingly, sex was found to
create a difference in patient outcomes; male patients had
significantly worse OS and PFS than female patients. In addition,
among the 15 patients with relapsed or refractory disease, 11 were
males. As other prognostic factors such as age, stage, IPI, and
treatment intensity were balanced between male and female patients
in the present study (data not shown), this indicates that the poor
prognosis for male patients did not result from common clinical or
demographic factors. Although a scientific explanation for such sex
differences is lacking, sex differences in cancer prognosis are not
a novel issue. For example, male sex has been considered a poor
risk factor for Hodgkin's lymphoma for decades without proper
pathophysiological explanations (18). Several hypotheses can be proposed
for sex as a prognostic factor for PMLBCL. Firstly, drug metabolism
may differ between male and female patients; for example, the
pharmacokinetic differences in rituximab between male and female
patients are well known (19).
Additionally, androgen receptor expression in lymphomas and the
effects of hormones on lymphoma growth have been demonstrated in
previous studies (20,21). These findings highlight the
biological nature of sex differences in lymphomas. However, further
studies are required to clarify the underlying pathophysiology. In
clinical practice, based on the above findings, it is suggested
that sex should be considered when designing a prognostic system
specific for PMLBCL.
Age is a common prognostic factor for lymphomas.
Compared with other types of diffuse large B-cell lymphoma (DLBCL),
PMLBCL predominantly occurs in young individuals. The age
distribution observed in the present study was consistent with
this. Age was demonstrated to be a major prognostic factor, as the
OS and PFS durations were significantly shorter in patients aged
>60 years than in younger patients. This may be due to elderly
patients being unable to tolerate intensive chemotherapy. Indeed,
in the present study, only one of the seven elderly patients who
received R-MACOP-B had progressive disease and succumbed before
completing the protocol. The remaining elderly patients were
treated with R-CHOP or less-intensive regimens. A large
population-based study of the Surveillance, Epidemiology and End
Results (SEER) database analyzed 426 cases of PMLBCL, and the
results of multivariate analysis showed that the OS of patients
>60 years was significantly reduced compared with that of
patients aged 18–39 years [hazard ratio (HR)=3.568 (95% CI: 2.653,
4.798); P=0.005] (2). Another
single-center retrospective study in which 48 cases of PMLBCL were
analyzed also showed that age >60 years was an independent
prognostic factor for OS, with an HR of 16.697 (95% CI: 1.106,
252.022; P=0.042) (10). As the
predominant age of patients with PMLBCL is <60 years, a cutoff
age of 60 years may not be a proper predictor of survival. In a
retrospective study of 153 patients with PMLBCL, univariate
analysis showed that age >40 years was associated with poor
survival; however, this association was not observed by
multivariate analysis (8). Another
study based on the SEER database analyzed 474 patients with PMLBCL
who were aged <60 years, and univariate analysis showed that age
(18–39 vs. 40–59 years) was not significantly associated with OS
(22). Therefore, whether age is an
appropriate prognostic factor for survival requires further
investigation. Despite the risk of an unfavorable prognosis in
elderly patients treated with high-intensity chemotherapy, a cure
can be achieved in some of such patients. Among the elderly
patients who received low-intensity treatment, three had
relapse-free survival. The two elderly long-term survivors both
underwent RT. While the number of patients was small, such an
experience suggests that low-intensity treatment and consolidative
RT are tolerable for elderly patients, resulting in potentially
more favorable outcomes.
The present study showed that patients with stage
III/IV PMLBCL had worse PFS than those with stage I/II disease, but
no significant difference in OS. This indicates that patients with
advanced disease are prone to relapse and that salvage therapies
are beneficial for OS. As relapse is not common, there is no
consensus regarding the standard treatment for refractory/relapsed
PMLBCL (rrPMLBCL). However, a systematic review investigated
published guidelines and real-world treatment patterns for
rrPMLBCL. It revealed that only four guidelines for the treatment
of rrPMLBCL recommend rituximab plus chemotherapy protocols with or
without consolidative RT followed by high-dose chemotherapy and
autologous stem cell transplantation. Regarding real-world
treatment strategies, chemotherapy alone or in combination with
rituximab followed by high-dose treatment and stem cell
transplantation has been used in the majority of published studies
(23). Owing to the frequent
expression of programmed cell death-1 (PD-1) ligand 1 and 2 in
PMLBCL, it has been proposed that PMLBCL may be susceptible to PD-1
inhibition. In the phase IB KEYNOTE-013 and phase II KEYNOTE-170
trials, the objective response rate of adults with rrPMLBCL
receiving pembrolizumab, a PD-1 inhibitor, was 48 and 45%,
respectively, and the incidence of treatment-related adverse events
was 24 and 23%, respectively (24).
Several multicenter trials evaluating pembrolizumab for the
treatment of rrPMLBCL are ongoing (25).
The IPI utilizes five clinicopathological
parameters, namely age, stage, pretreatment serum concentrations of
LDH, ECOG performance status and the involvement of extranodal
sites, and has been shown to predict prognosis in patients with
newly diagnosed DLBCL (15). Since
the age, stage and possibility of extranodal involvement of PMLBCL
are very different from those of DLBCL, the prognostic value of IPI
in PMLBCL is not as powerful as that in DLBCL (26,27).
Although the present study showed that an IPI score >1 was
associated with inferior OS, the number of cases in the high- and
low-IPI groups was not well balanced, as there were only nine
patients in the high-IPI group. Therefore, it is not recommended
that the IPI should be a standard prognostic tool for PMLBCL, as it
is in other types of DLBCL. However, a novel prognostic system for
PMLBCL, based on the risk factors identified in the present and
previous studies, may be constructed to determine the prognosis of
patients more accurately. This system should be evaluated and
validated in subsequent large-scale cohorts or prospective
studies.
The role of RT in the treatment of PMLBCL remains
controversial. There are concerns regarding the late toxicity of
mediastinal irradiation, including cardiovascular diseases and
secondary malignancies. However, RT was shown to be significantly
associated with survival benefits in two retrospective
population-based studies performed using the SEER and National
Cancer Databases. However, these studies also found that in the
USA, approximately half of the patients in the post-rituximab era
did not receive RT (28,29). The UNFOLDER trial included 134
patients with PMLBCL receiving R-CHOP who were randomized to
receive R-CHOP-14 or R-CHOP-21 with or without RT for bulky or
extranodal involvement. The results showed that 3-year event-free
survival was superior in patients receiving RT (94 vs. 78%;
P=0.007). No significant differences in the OS and PFS rates were
detected between the RT and no-RT groups. The authors concluded
that the benefits of RT were observed only in patients who showed a
partial response to R-CHOP (30).
Based on these findings and clinical experience, it is proposed
that the cornerstone of successful treatment is the achievement of
a complete response. Therefore, the administration of
high-intensity chemotherapy is recommended after the initial
diagnosis if the patient is able to tolerate the regimen. A
complete response can often be achieved, and RT may not be
necessary. By contrast, when patients receive only low-intensity
chemotherapy, a complete response is not achieved or is equivocal.
It is recommended that RT should be administered immediately since
disease progression is often rapid in patients receiving
low-intensity chemotherapy.
The current study has several limitations. Firstly,
this was a single-center retrospective study with a small sample
size, which might have been susceptible to selection bias.
Secondly, the patients were mostly <60 years old, and with
disease stage I/II and IPI score ≤1. Therefore, the number of
patients was not balanced between the groups being compared.
Finally, a multivariate analysis was not performed because of the
small number of patients. Therefore, whether the analyzed variables
are independent prognostic factors for survival requires further
investigation. In conclusion, age, sex, stage, IPI and type of
chemotherapy were identified as prognostic factors for PMLBCL. The
achievement of a CR after frontline treatment appears to be the key
to success; therefore, high-intensity chemotherapy is recommended.
Male patients had significantly worse outcomes than female
patients, for reasons that are not yet clear. The IPI is not an
ideal tool for the prognostication of PMLBCL due to the unique
clinical features of young age, early stage and rare extranodal
lesions. It is proposed that a novel prognostic tool specific for
PMLBCL should be designed, in which the impact of sex is
considered.
Acknowledgements
Not applicable.
Funding
This study was supported by Chang Gung Memorial Hospital (grant
no. CORPG3G0821).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
HJS and HC designed the study. HJS wrote the
manuscript. MCK, TLL, HWK, JHW, YSH, CWO and YJS contributed to the
acquisition and analysis of clinical data. MCK supervised the
conduction of the clinical study and performed the data analysis.
HJS and HC confirm the authenticity of all the raw data. All
authors read and approved the final version of the manuscript.
Ethics approval and consent to
participate
This study was reviewed and approved by the Chang
Gung Medical Foundation Institutional Review Board (approval no.
202100653B0). The study was exempt from the requirement for written
informed consent.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
PMLBCL
|
primary mediastinal large B-cell
lymphoma
|
|
OS
|
overall survival
|
|
PFS
|
progression-free survival
|
|
IPI
|
International Prognostic Index
|
|
RT
|
radiotherapy
|
|
ECOG
|
Eastern Cooperative Oncology Group
|
|
R-CHOP
|
rituximab, cyclophosphamide,
doxorubicin, vincristine and prednisolone
|
|
R-VACOP-B
|
rituximab, etoposide, doxorubicin,
cyclophosphamide, vincristine, prednisolone and bleomycin
|
|
R-MACOP-B
|
rituximab, methotrexate, doxorubicin,
cyclophosphamide, vincristine, prednisolone and bleomycin
|
|
DA-EPOCH-R
|
dose-adjusted etoposide, prednisone,
vincristine, cyclophosphamide, doxorubicin and rituximab
|
|
LDH
|
lactate dehydrogenase
|
|
rrPMLBCL
|
refractory/relapsed PMLBCL
|
|
PD-1
|
programmed cell death-1
|
|
DLBCL
|
diffuse large B-cell lymphoma
|
References
|
1
|
Martelli M, Ferreri A, Di Rocco A,
Ansuinelli M and Johnson PWML: Primary mediastinal large B-cell
lymphoma. Crit Rev Oncol Hematol. 113:318–327. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Liu PP, Wang KF, Xia Y, Bi XW, Sun P, Wang
Y, Li ZM and Jiang WQ: Racial patterns of patients with primary
mediastinal large B-cell lymphoma: SEER analysis. Medicine
(Baltimore). 95:e40542016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Jaffe ES, Harris NL, Stein H and Isaacson
PG: Classification of lymphoid neoplasms: The microscope as a tool
for disease discovery. Blood. 112:4384–4399. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yu Y, Dong X, Tu M and Wang H: Primary
mediastinal large B cell lymphoma. Thorac Cancer. 12:2831–2837.
2021. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Zelenetz AD, Gordon LI, Wierda WG,
Abramson JS, Advani RH, Andreadis CB, Bartlett N, Byrd JC, Fayad
LE, Fisher RI, et al: Diffuse Large B-cell lymphoma version 1.2016.
J Natl Compr Canc Netw. 14:196–231. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Vitolo U, Seymour JF, Martelli M,
Illerhaus G, Illidge T, Zucca E, Campo E and Ladetto M; ESMO
Guidelines Committee, : Extranodal diffuse large B-cell lymphoma
(DLBCL) and primary mediastinal B-cell lymphoma: ESMO Clinical
Practice Guidelines for diagnosis, treatment and follow-up. Ann
Oncol. 27 (Suppl 5):v91–v102. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Dunleavy K, Pittaluga S, Maeda LS, Advani
R, Chen CC, Hessler J, Steinberg SM, Grant C, Wright G, Varma G, et
al: Dose-adjusted EPOCH-rituximab therapy in primary mediastinal
B-cell lymphoma. N Engl J Med. 368:1408–1416. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Savage KJ, Al-Rajhi N, Voss N, Paltiel C,
Klasa R, Gascoyne RD and Connors JM: Favorable outcome of primary
mediastinal large B-cell lymphoma in a single institution: The
British Columbia experience. Ann Oncol. 17:123–130. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Todeschini G, Secchi S, Morra E, Vitolo U,
Orlandi E, Pasini F, Gallo E, Ambrosetti A, Tecchio C, Tarella C,
et al: Primary mediastinal large B-cell lymphoma (PMLBCL):
Long-term results from a retrospective multicentre Italian
experience in 138 patients treated with CHOP or MACOP-B/VACOP-B. Br
J Cancer. 90:372–376. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Yang SH, Hsiao LT, Chiou TJ, Yang CF, Yu
YB, Liu CY, Gau JP, Liu JH, Chen PM and Tzeng CH: Rituximab
induction therapy, survival benefits, and the increasing selection
of radiotherapy as the postinduction treatment in patients with
primary mediastinal large B-cell lymphoma. J Chin Med Assoc.
78:400–407. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Aoki T, Izutsu K, Suzuki R, Nakaseko C,
Arima H, Shimada K, Tomita A, Sasaki M, Takizawa J, Mitani K, et
al: Prognostic significance of pleural or pericardial effusion and
the implication of optimal treatment in primary mediastinal large
B-cell lymphoma: A multicenter retrospective study in Japan.
Haematologica. 99:1817–1825. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Zhou H, Xu-Monette ZY, Xiao L, Strati P,
Hagemeister FB, He Y, Chen H, Li Y, Manyam GC, Li Y, et al:
Prognostic factors, therapeutic approaches, and distinct
immunobiologic features in patients with primary mediastinal large
B-cell lymphoma on long-term follow-up. Blood Cancer J. 10:492020.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Harris NL, Jaffe ES, Stein H, Banks PM,
Chan JK, Cleary ML, Delsol G, De Wolf-Peeters C, Falini B, Gatter
KC, et al: A revised European-American classification of lymphoid
neoplasms: A proposal from the International Lymphoma Study Group.
Blood. 84:1361–1392. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Oken MM: Toxicity and response criteria of
the Eastern Cooperative Oncology Group. Am J Clin Oncol. 5:649–655.
1982. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
International Non-Hodgkin's Lymphoma
Prognostic Factors Project, . A predictive model for aggressive
non-Hodgkin's lymphoma. N Engl J Med. 329:987–994. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Olweny CL: Cotswolds modification of the
Ann Arbor staging system for Hodgkin's disease. J Clin Oncol.
8:15981990.PubMed/NCBI
|
|
17
|
Cheson BD, Fisher RI, Barrington SF,
Cavalli F, Schwartz LH, Zucca E, Lister TA; Alliance Australasian
Leukaemia and Lymphoma Group; Eastern Cooperative Oncology Group;
European Mantle Cell Lymphoma Consortium, ; et al: Recommendations
for initial evaluation, staging, and response assessment of Hodgkin
and non-Hodgkin lymphoma: The Lugano classification. J Clin Oncol.
32:3059–3068. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Hasenclever D and Diehl V: A prognostic
score for advanced Hodgkin's disease. International prognostic
factors project on advanced Hodgkin's disease. N Engl J Med.
339:1506–1514. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Pfreundschuh M, Muller C, Zeynalova S,
Kuhnt E, Wiesen MH, Held G, Rixecker T, Poeschel V, Zwick C, Reiser
M, et al: Suboptimal dosing of rituximab in male and female
patients with DLBCL. Blood. 123:640–646. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Mostaghel EA, Martin PS, Mongovin S, Frayo
S, Zhang A, Edlefsen KL, Press OW and Gopal AK: Androgen receptor
expression in mantle cell lymphoma: Potential novel therapeutic
implications. Exp Hematol. 49:34–38.e32. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Talaber G, Yakimchuk K, Guan J, Inzunza J
and Okret S: Inhibition of estrogen biosynthesis enhances lymphoma
growth in mice. Oncotarget. 7:20718–20727. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Jiang S, Zhen H and Jiang H: Role of
radiation therapy in younger and older adults with primary
mediastinal large B cell lymphoma in rituximab Era: A U.S.
Population-based analysis. J Adolesc Young Adult Oncol. 8:623–627.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Takyar J, Raut M, Borse R, Balakumaran A
and Sehgal M: Relapsed/refractory primary mediastinal large B-cell
lymphoma: A structured review of epidemiology, treatment guidelines
and real-world treatment practices. Expert Rev Hematol. 13:275–287.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Armand P, Rodig S, Melnichenko V,
Thieblemont C, Bouabdallah K, Tumyan G, Özcan M, Portino S,
Fogliatto L, Caballero MD, et al: Pembrolizumab in relapsed or
refractory primary mediastinal large B-cell lymphoma. J Clin Oncol.
37:3291–3299. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Tomassetti S, Chen R and Dandapani S: The
role of pembrolizumab in relapsed/refractory primary mediastinal
large B-cell lymphoma. Ther Adv Hematol. 10:20406207198415912019.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Hamlin PA, Portlock CS, Straus DJ, Noy A,
Singer A, Horwitz SM, Oconnor OA, Yahalom J, Zelenetz AD and
Moskowitz CH: Primary mediastinal large B-cell lymphoma: Optimal
therapy and prognostic factor analysis in 141 consecutive patients
treated at Memorial Sloan Kettering from 1980 to 1999. Br J
Haematol. 130:691–699. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Romaguera JE, Rodriguez Diaz-Pavon J,
Carias L, Hagemeister FB, McLaughlin P, Rodriguez MA, Sarris AH,
Younes A, Preti A, Bachier C, et al: Use of the international
prognostic index and the tumor score to detect poor-risk patients
with primary mediastinal large B-cell lymphoma: A study of 37
previously untreated patients. Leuk Lymphoma. 28:295–306. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Jackson MW, Rusthoven CG, Jones BL, Kamdar
M and Rabinovitch R: Improved survival with radiation therapy in
stage I–II primary mediastinal B cell lymphoma: A surveillance,
epidemiology, and end results database analysis. Int J Radiat Oncol
Biol Phys. 94:126–132. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Jackson MW, Rusthoven CG, Jones BL, Kamdar
M and Rabinovitch R: Improved survival with combined modality
therapy in the modern era for primary mediastinal B-cell lymphoma.
Am J Hematol. 91:476–480. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Held G, Thurner L, Poeschel V, Berdel C,
Ott G, Schmidt C, Viardot A, Borchmann P, Shpilberg O, Nickelsen M,
et al: Role of radiotherapy and dose-densification of R-CHOP in
primary mediastinal B-cell lymphoma: A subgroup analysis of the
unfolder trial of the German Lymphoma Alliance (GLA). J Clin Oncol.
38 (Suppl 15):S80412020. View Article : Google Scholar
|














