Introduction
Malignant bowel obstruction (MBO) is a disease with
a poor prognosis, particularly in patients with advanced bowel or
gynecological cancers. Although it may occur at any stage, it is
most commonly associated with end-stage cancer (1). Retrospective reviews demonstrated
that 10–50% of patients with advanced cancer stage will develop MBO
during the course of their disease and suffer from intractable
abdominal pain, nausea and vomiting, which result in a poor quality
of life (QOL), mental and emotional problems (2). Multimodality treatments, including
surgery, palliative radiotherapy, chemotherapy and total parenteral
nutrition formulas, may be used to relieve the symptoms in patients
with MBO; however, there is currently no consensus regarding the
optimal treatment strategy and no strong evidence supporting the
efficacy of any treatment in improving QOL and prolonging
survival.
Materials and methods
Patient records
In order to evaluate the clinical presentation,
treatment options and survival of MBO patients, we searched the
TSGH database of cancer registries for MBO cases between January,
1995 and December, 2008 and analyzed the clinicopathological
characteristics and the association between treatments and
prognosis or QOL. The clinical information and diagnostic results
were extracted from the medical records, including demographic
data, clinical manifestations, physical examination, radiological
findings, laboratory results and pathology reports. Non-malignant
causes of obstruction, such as adhesions from previous surgery,
hernia, volvulus, inflammatory bowel disease, fecal impaction and
bowel ischemia were excluded from this study.
Functional status
The change in patients’ functional status following
treatment was evaluated according to the Eastern Cooperative
Oncology Group (ECOG) performance status, with a decrease in the
ECOG score reflecting the improvement of the symptoms following
treatment. Clinicopathological data from 27 MBO patients (16 males
and 11 females) treated in our hospital, with a median age of 69.3
years (range, 36–92 years) were retrospectively analyzed. Survival
was calculated with the Kaplan-Meier method and the groups were
compared using the log-rank test (3,4).
Results
Cases
Among the 27 MBO patients, the primary malignant
tumors included 15 colorectal cancers, 5 gastric, 2 duodenal, 2
bladder, 1 ovarian, 1 pancreatic and 1 pseudomyxoma peritonei. The
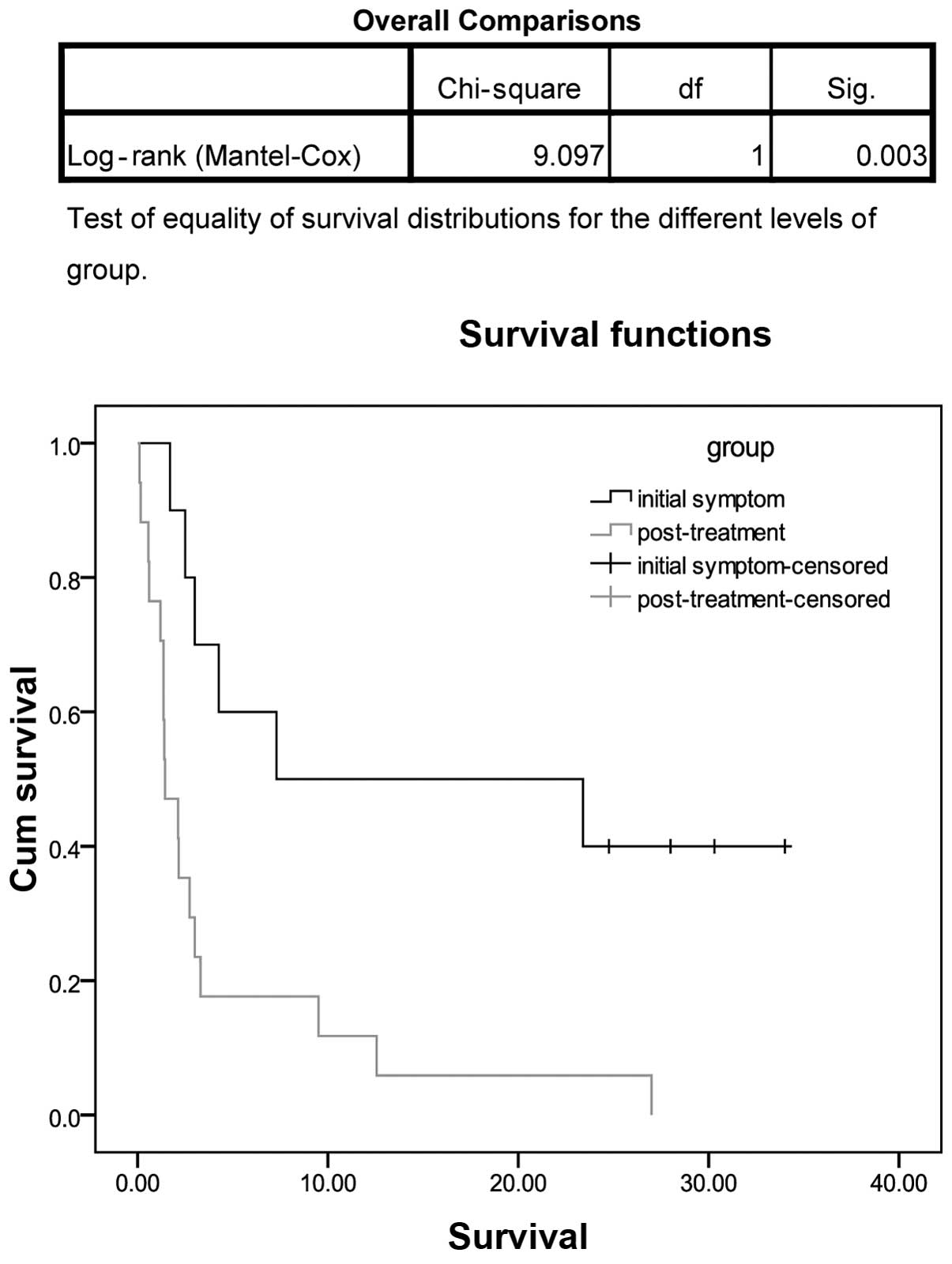
MBO patients were classified as the initial symptom (IS) and
post-treatment of primary cancer (PT) groups, according to the time
of onset of the MBO symptoms. The clinical characteristics of the
IS (n=10) and PT groups (n=17) are summarized in Table I. According to the statistical
analysis, the overall survival time was significantly higher in the
IS group compared with that in the PT group (P=0.003, Fig. 1).
 | Table I.Malignant bowel obstruction (MBO):
Initial symptom vs. post-treatment of primary cancer groups. |
Table I.
Malignant bowel obstruction (MBO):
Initial symptom vs. post-treatment of primary cancer groups.
| Characteristics | MBO patient groups
|
|---|
| Initial symptom
(n=10) | Post-treatment
(n=17) |
|---|
| Age (years) | | |
| Range | 45–92 | 36–85 |
| Median | 74.1 | 66.5 |
| Gender | | |
| Male | 5 | 11 |
| Female | 5 | 6 |
| Stage | | |
| III | 3 | 6 |
| IV | 5 | 8 |
| ECOG score | | |
| 0–2 | 5 | 2 |
| 3–4 | 5 | 15 |
| Primary cancer | | |
| Colorectal | 8 | 7 |
| Other | 2 | 10 |
| Treatment | | |
| Surgery | 7 | 3 |
| Chemotherapy | 3 | 10 |
| Outcome | | |
| Overall RR (%) | 50 | 17.6 |
| Survival time
(months) | 15.92 | 4.15 |
SI group
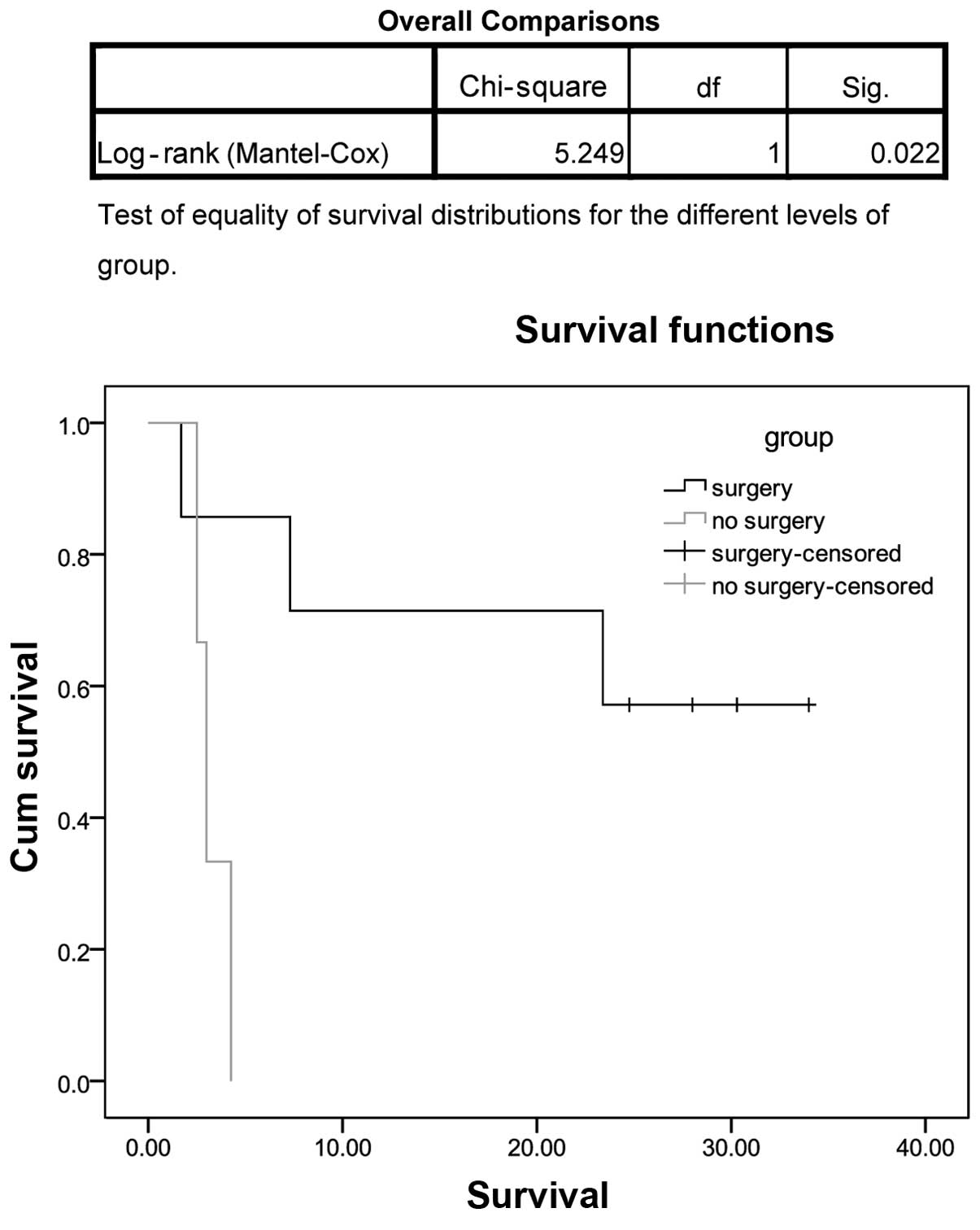
The clinical characteristics of the IS group are
summarized in Table II. Of the 10
patients in this group, 7 underwent surgery, whereas 3 did not
receive surgical treatment. The overall survival time of the
patients who received surgical treatment was significantly higher
compared with that in the no surgical treatment group (P=0.022,
Fig. 2). Of the 7 patients who
received surgical treatment, 6 exhibited an improvement in the ECOG
performance status, although the difference was not statistically
significant (P=0.206). There may be a trend indicating that the
survival time of colorectal cancer patients receiving surgery and
concurrent treatment is higher compared with those receiving
surgery alone (P=0.538); however, the results require further
analysis, taking into consideration the severity of the disease,
age and number of cases.
| Table II.Malignant bowel obstruction as the
initial symptom. |
Table II.
Malignant bowel obstruction as the
initial symptom.
| Case no. | Gender | Age (years) | Primary cancer | Stage | Treatment | Survival time
a (months) | ECOG score
(peri-treatment) | Hospice (days) |
|---|
| 4 | M | 73 | Colon | IV | Exp. lap. with
Hartmann’s, end S-colostomy and wedge of seg 2 | 30.3 | 2 to 1 | - |
| 5 | M | 76 | S-colon | IV | Colostomy + CPT-11,
Erbitux, UFUR, Oxalip, 5-FU | 23.4 | 3 to 2 | - |
| 9 | F | 92 | R-S colon | II | Exp. lap. with T-loop
colostomy | 1.7 | 4 to 4 | - |
| 11 | F | 81 | R-colon | IIIc | Exp. lap. with
Hartmann’s | 28 | 2 to 1 | - |
| 12 | M | 81 | S-colon | IIIb | AR and protective
T-loop colostomy | 7.3 | 2 to 1 | 8 |
| 15 | M | 45 | Stomach | IV | Oxalip + HDFL
(8)b | 4.26 | 4 to 4 | - |
| 17 | F | 83 | D-colon | IIb | T-loop colostomy and
left hemicolecotmy + UFUR, Xeloda | 24.76 | 2 to 1 | - |
| 19 | M | 81 | S-colon | IIIB | Exp. lap. with AR +
5-FU (4)b, Oxalip +
5-FU (2)b | 34 | 2 to 1 | - |
| 20 | F | 74 | Duodenum | IV | 5-FU (10)b | 3 | 4 to 4 | - |
| 22 | F | 55 | Colon | IV | HDFL (2)b, Oxalip + HDFL (2)b, Erbitux, Xeloda and
CPT-11 | 2.5 | 3 to 4 | - |
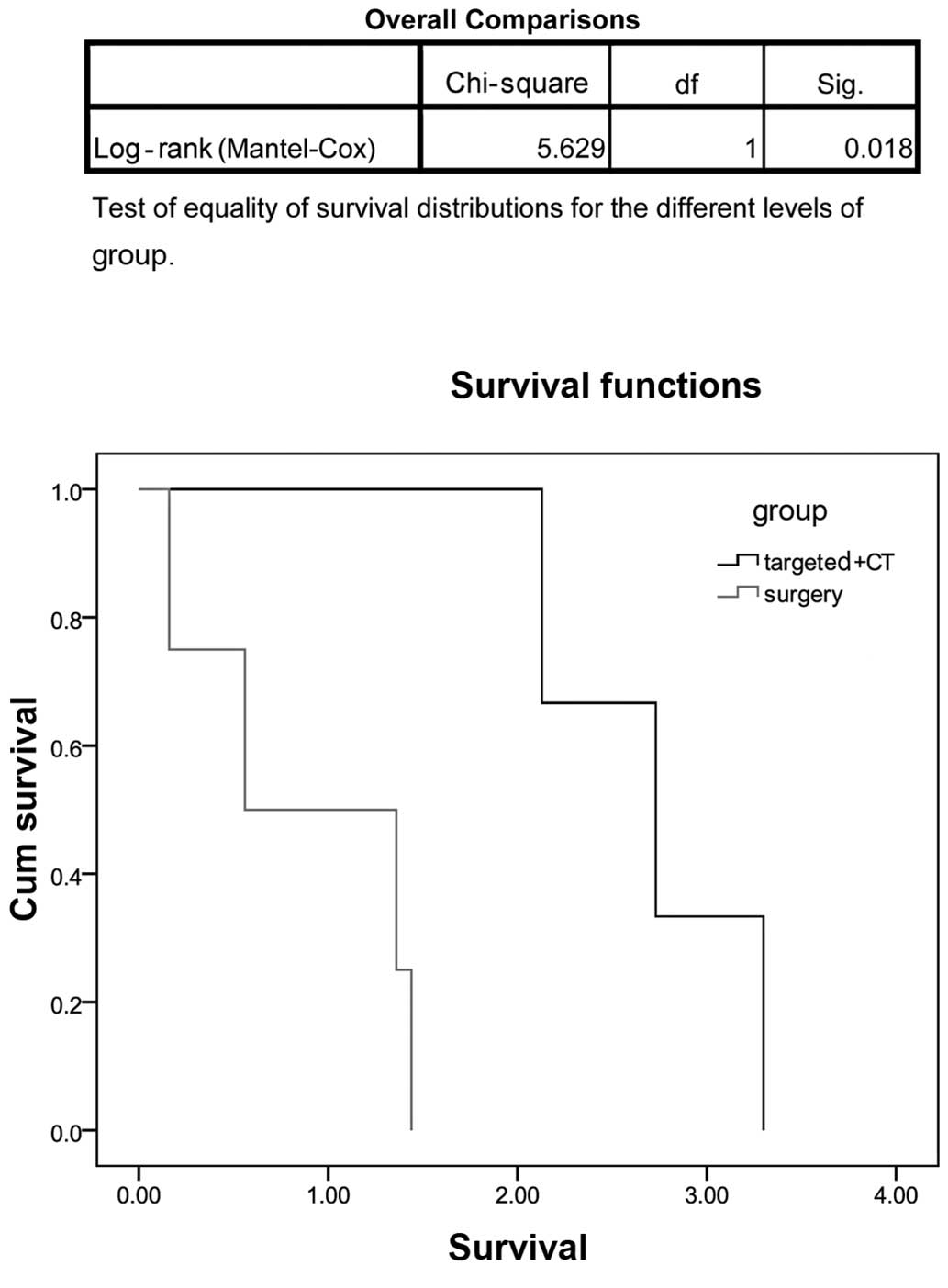
PT group
The clinical characteristics of the PT group are
summarized in Table III. The mean
survival time of the patients in this group was shorter compared
with the IS group. The mean survival time of colorectal cancer
patients receiving targeted therapy and chemotherapy was longer
compared with that of the patients who received surgery alone or
conservative treatment (2.72 vs. 0.69 months, respectively;
P=0.018, Fig. 3) and the patients’
functional status exhibited a more significant improvement in the
former group (ECOG score from 4 to 3). The mean survival time of
gastric cancer patients receiving targeted therapy + chemotherapy
was longer compared with those receiving chemotherapy alone,
although the difference was not statistically significant
(P=0.182), which may be due to the smaller number of cases. We also
observed that cancers which responded well to chemotherapy, such as
ovarian and colorectal cancers, were associated with longer
survival.
| Table III.Post-treatment malignant bowel
obstruction (MBO). |
Table III.
Post-treatment malignant bowel
obstruction (MBO).
| Case no. | Gender | Age (years) | Primary cancer | Stage | Treatment | MBO treatment | Survival time
(months) | ECOG score (Tx) | Hospice (days) |
|---|
| 1 | F | 81 | R-colon | III | APR + colostomy +
CCRT | Exp. lap. with loop
jejunostomy | 1.44 | 4 to 4 | - |
| 2 | M | 85 | Colon | IV | Nil | Nil | 0.56 | 4 to 4 | 17 |
| 3 | F | 69 | TCC | III | Nephroureterectomy +
removal of bladder cuff, R’t+CCRT (Toxol weekly) | Gemzar +vinblastin;
MTX + vinblastin | 1.2 | 4 to 4 | - |
| 6 | F | 64 | Ovary | IIIc | Debulking+Phyxol+
carboplatin+Doxil, Caelyx+Hycamptin | Carboplatin
(11)a+ Hycamptin
(2)a | 12.56 | 2 to 1 | 60 |
| 7 | F | 46 | Stomach | IV | Cisplatin+5-FU | 5-FU (3)a | 3 | 4 to 3 | 9 |
| 8 | M | 36 | D-S colon | III | Exp. lap. with
bisegmentectomy, left hemicolectomy | 5-FU (5)a; Oxalip+ 5-FU (2)a; Erbitux (8)a | 3.3 | 4 to 3 | - |
| 10 | M | 72 | Duodenum | II | Whipple
resection+5-FU (11)a | conservative | 0.1 | 4 to 4 | - |
| 13 | M | 66 | Stomach | IV | HDFU (4)a | Taxotere
(1)a | 1.4 | 4 to 4 | 18 |
| 14 | M | 67 | R-S colon | IIa | Neoadjuvant CCRT,
s/p oral UFUR+exp. lap. with LAR | Nil | 0.16 | 4 to 4 | - |
| 16 | M | 77 | Pseudomyxoma
peritonei | | Exp. lap. with
removal of tumor | Nil | 0.6 | 4 to 4 | - |
| 18 | M | 84 | Colon | IIB | Op+LDFL and liver
metastasis s/p weekly HDFL, Campto with HDFL, Oxalip with HDFL,
Erbitux with HDFL | Xeloda,
Erbitux | 2.73 | 4 to 3 | 16 |
| 21 | M | 70 | T-colon | IIIc | Right
hemicolectomy+5-FU +Eloxatin (6 months) | FOLFORI (4)a | 2.13 | 4 to 3 | - |
| 23 | M | 71 | S-colon | IV | Hartmann’s
procedure and lobectomy of liver | Nil | 1.36 | 4 to 4 | 23 |
| 24 | F | 46 | Stomach | IV | Exp.
lap.+TAH+BSO, | 5-FU | 2.16 | 4 to 3 | - |
| 25 | M | 57 | Pancreas | IV | Major surgery | 5-FU | 9.5 | 2 to 1 | - |
| 26 | M | 63 | TCC | IV | Nephroureterectomy
and removal of bladder cuff, R’t | Exp. lap. with
lysis of adhesions+jejunojejunostomy+end ileostomy+decompression of
small intestine | 1.36 | 4 to 4 | - |
| 27 | F | 78 | Stomach | IV | Subtotal
gastrectomy + FOLFOX | AR+colostomy, HDFL;
Phyxol+Avastin; Irino+HDFL+Avastin, with daily oral UFUR | 27 | 4 to 2 | - |
Hospice patients
The clinical characteristics of MBO patients under
hospice care are summarized in Table
IV. A total of 7 patients received hospice care. The MBO
symptoms in the terminal stage of cancer were intractable abdominal
pain, abdominal fullness, nausea, vomiting and constipation. Under
hospice care, the pain scores of all 7 patients decreased and the
symptoms causing discomfort were improved.
| Table IV.Palliative care of malignant bowel
obstruction. |
Table IV.
Palliative care of malignant bowel
obstruction.
| Case no. | Gender | Age | Primary cancer | Stage | Symptoms | ECOG (hospice) | Pain | TPN | NG | Hospice (days) |
|---|
| 12 | M | 81 | S-colon | IIIb | Abdominal fullness,
nausea and vomiting | 4 | 9 to 4 | N | Y | 8 |
| 2 | M | 85 | Colon | IV | Abdominal
fullness | 4 | 6 to 2 | N | N | 17 |
| 6 | F | 64 | Ovary | IIIc | Abdominal fullness,
nausea and vomiting | 3 | 5 to 3 | N | N | 60 |
| 7 | F | 46 | Stomach | IV | Constipation and
shortness of breath | 4 | 6 to 2 | N | Y | 9 |
| 13 | M | 66 | Stomach | IV | Abdominal fullness
and constipation | 4 | 7 to 4 | N | Y | 18 |
| 18 | M | 84 | Colon | IIB | Abdominal
fullness | 4 | 5 to 3 | N | Y | 16 |
| 23 | M | 71 | S-colon | IV | Abdominal pain and
fullness | 3 | 3 to 2 | N | Y | 23 |
Discussion
MBO is a common palliative care problem, encountered
in 5–51% of patients with ovarian cancer, 10–28% of patients with
colorectal cancer and 3–15% of patients with other types of cancer
(1,2,5–8). In
our study, the type of cancer most commonly responsible for MBO was
found to be colorectal adenocarcinoma (55%). The differences in
incidence may be attributed to the differences in clinical
environment, admission criteria, diagnostic standards and clinical
assessment.
Although MBO is a common problem in clinical
practice, achieving a consensus on its management is difficult, as
the treatment selection maybe be affected by the location and
degree of obstruction, cancer stage, patient’s functional status,
survival time and co-morbidity (2,5–8).
Furthermore, it may also be affected by the lack of a definitive
diagnosis, therapeutic goals and large clinical studies assessing
the effects of different treatment plans on symptom relief and QOL
improvement.
MBO patients may be classified into IS and PT groups
according to the time of onset of the MBO symptoms and the patients
of the IS group were considered more suitable for surgery,
exhibited better ECOG scores and longer mean survival time compared
with those in the PT group.
Woolfson et al demonstrated in a
non-randomized study in 1997 that surgery did not significantly
affect survival time and QOL (9).
However, in our study, the overall survival time of the patients in
the IS group who received surgical treatment was significantly
longer compared with that of the no surgical treatment group. Thus,
our results suggested that surgical treatment is suitable for IS
group patients.
In the PT group, the mean survival time of
colorectal cancer patients who received targeted therapy and
chemotherapy was longer compared with that of patients who received
surgery alone or conservative treatment and the patients’
functional status exhibited a more significant improvement in the
former group. Thus, palliative chemotherapy may be of value for
this group of patients and may be considered a viable option when
discussing the therapeutic plan with the patient and the family
members.
The most common symptoms of MBO in the terminal
stages of cancer are intractable abdominal pain, abdominal
fullness, nausea, vomiting and constipation. Previous studies have
predominantly focused on approaches to the management and
resolution of intestinal obstruction, with little consideration for
QOL (10). Under palliative care,
the pain scores exhibit a marked decrease and the symptoms are
improved. Thus, medical care personnel are always questioned
regarding hospice care interventions in terminal cancer
patients.
Multimodality treatment strategies, which currently
include surgical treatment, palliative radiotherapy, chemo-therapy
and total parenteral nutrition formulas, may be used to relieve the
symptoms in patients with MBO; however, there is no consensus
regarding the optimal treatment strategy and no strong evidence
supporting the efficacy of any treatment in improving QOL and
prolonging survival. Thus, it is crucial for physicians in
palliative care to accurately assess the patient’s clinical
condition, anticipated survival time, risk of mortality and
morbidity. The physicians should also communicate with the patient
and the family members prior to making therapeutic plan decisions.
Furthermore, educational interventions for patients and their
family members should focus on the primary goals of MBO management
in the palliative care setting. Patients with MBO from metastastic
intra-abdominal disease may bear a significant physical and
psychological burden, with a highly compromised QOL at the time of
diagnosis; however, with adequate treatment, an improvement may be
quickly achieved.
Targeted therapy for prolonging survival requires
further investigations. Our previous studies have had certain
limitations, such as limited number of cases, lack of QOL
evaluation, heterogeneity, different types of cancer and different
forms of treatment (11).
There were also important limitations to the present
study. Although this was not a randomized trial, the patient
characteristics in the two groups were significantly different.
Furthermore, the number of patients and duration of follow-up were
limited. A longer follow-up period may help stabilize the trends
and enable more reliable conclusions.
In conclusion, the primary cause of MBO in our study
was adenocarcinoma of the colon. The overall survival time was
significantly higher in the IS group and improved QOL was achieved
in patients receiving surgical treatment. The mean survival time of
colorectal cancer patients receiving targeted therapy and
chemotherapy was longer compared with those receiving surgery alone
or conservative treatment and their functional status exhibited a
more significant improvement. In addition, for end-stage cancer
patients with MBO, hospice care was effective in reducing pain
scores and relieving the symptoms of the disease.
Acknowledgements
This study was supported by a grant
from Tri-Service General Hospital (no. TSGH-C100-177), Taiwan,
R.O.C.
References
|
1.
|
Ripamonti C and Mercadante S:
Pathophysiology and management of malignant bowel obstruction.
Oxford Textbook of Palliative Medicine. Doyle D, Hanks G, Cherny NI
and Calman K: 3rd edition. New York Oxford University Press; NY:
pp. 496–507. 2004
|
|
2.
|
Ripamonti CI, Easson AM and Gerdes H:
Management of malignant bowel obstruction. Eur J Cancer.
44:1105–1115. 2008. View Article : Google Scholar
|
|
3.
|
Kaplan EL and Meier P: Nonparametric
estimation from incomplete observations. J Am Stat Assoc.
53:457–481. 1958. View Article : Google Scholar
|
|
4.
|
Peto R and Pike MC: Conservatism of the
approximation sigma (O-E)2-E in the logrank test for survival data
or tumor incidence data. Biometrics. 29:579–584. 1973. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Weber C and Zulian GB: Malignant
irreversible intestinal obstruction: the powerful association of
octreotide to corticosteroids, antiemetics, and analgesics. Am J
Hosp Palliat Care. 26:84–88. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Wong TH and Tan YM: Surgery for the
palliation of intestinal obstruction in advanced abdominal
malignancy. Singapore Med J. 50:1139–1144. 2009.PubMed/NCBI
|
|
7.
|
Davis MP and Nouneh C: Modern management
of cancer-related intestinal obstruction. Curr Oncol Rep.
2:343–350. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Selby D, Wright F, Stilos K, et al: Room
for improvement? A quality-of-life assessment in patients with
malignant bowel obstruction. Palliat Med. 24:38–45. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Sun A, Bae K, Gore EM, et al: Phase III
trial of prophylactic cranial irradiation compared with observation
in patients with locally advanced non-small-cell lung cancer:
neurocognitive and quality-of-life analysis. J Clin Oncol.
29:279–286. 2011. View Article : Google Scholar
|
|
10.
|
Thaker DA, Stafford BC and Gaffney LS:
Palliative management of malignant bowel obstruction in terminally
ill patient. Indian J Palliat Care. 16:97–100. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Chouliara Z, Kearney N, Stott D,
Molassiotis A and Miller M: Perceptions of older people with cancer
of information, decision making and treatment: a systemic review of
selected literature. Ann Oncol. 15:1596–1602. 2004. View Article : Google Scholar : PubMed/NCBI
|