Introduction
The prognosis of patients with unresectable or
metastatic gastric cancer (GC) is poor and the median survival time
ranges between 6 and 12 months (1–12).
Cisplatin (CDDP) and 5-fluoropyrimidine (5-FU) are the most
frequently prescribed agents. Various chemotherapeutic agents have
been used in an attempt to improve patient survival. Oral
fluoropyrimidines (S-1 and capecitabine) plus CDDP were found to be
non-inferior to 5-FU plus CDDP (8,12).
Furthermore, docetaxel and trastuzumab achieved additional results
as first-line treatments in a phase III study (7,13).
Although irinotecan failed to demonstrate results as a first-line
treatment option in a TOP-003 trial (11), it was found to be non-inferior
compared to standard treatment in a first-line setting (5,9).
Peritoneal metastasis (PM) in GC is often the cause
of ascites and bowel obstruction. Chau et al (14) conducted a multivariate prognostic
factor analysis and identified four independent poor prognostic
factors, including PM; the patients were classified into good-,
moderate- and poor-risk groups, with highly significant differences
in survival among the groups.
In order to determine the association between PM and
poor prognosis, it is crucial to elucidate the clinical course of
the disease. It is, however, difficult to clearly define the
patients' clinical characteristics from the pooled data alone. In
addition, precise information associated with PM is seldom
collected. One of the reasons may be the differences among
individual doctors and other observers when classifying identical
adverse events. Furthermore, the clinical course of PM varies
widely between patients. Finally, following the termination of the
protocol treatment, follow-up monitoring is also terminated,
resulting in limited availability of information regarding events
(i.e., whether the patient is deceased or alive). Therefore, in
prospective trials, it is difficult to determine the clinical
characteristics over the period between chemotherapy initiation and
patient death.
We conducted a retrospective study to determine the
frequency of major events during and after palliative chemotherapy
in advanced GC patients with peritoneal dissemination.
Patients and methods
Inclusion criteria
The participants were recruited among patients who
received first-line chemotherapy for locally advanced or metastatic
disease at the Tochigi Cancer Center (TCC; Utsunomiya, Tochigi,
japan) and were selected according to the following criteria: i)
histologically confirmed gastric adenocarcinoma; ii) no history of
prior chemotherapy; iii) adequate bone marrow, hepatic and renal
function; and iv) absence of synchronous double cancer or other
serious illness.
Diagnositc criteria of
complications
The patient records were reviewed and the extracted
information included metastatic sites, treatments received,
developed complications and overall survival. The complications
were determined according to the following criteria: i) Bowel
obstruction, diagnostic imaging (air-fluid level formation) and/or
decompression tube insertion; ii) ascitic fluid collection, a large
amount of ascites and/or therapeutic drain insertion for ascites;
iii) obstructive jaundice, biliary drainage and/or jaundice with
imaging findings of biliary tree dilatation; iv) hydronephrosis,
diagnostic imaging and/or therapeutic insertion of ureteral
catheter(s); and v) thrombosis, recorded thrombotic event with
abnormal blood tests.
Results
Patient characteristics
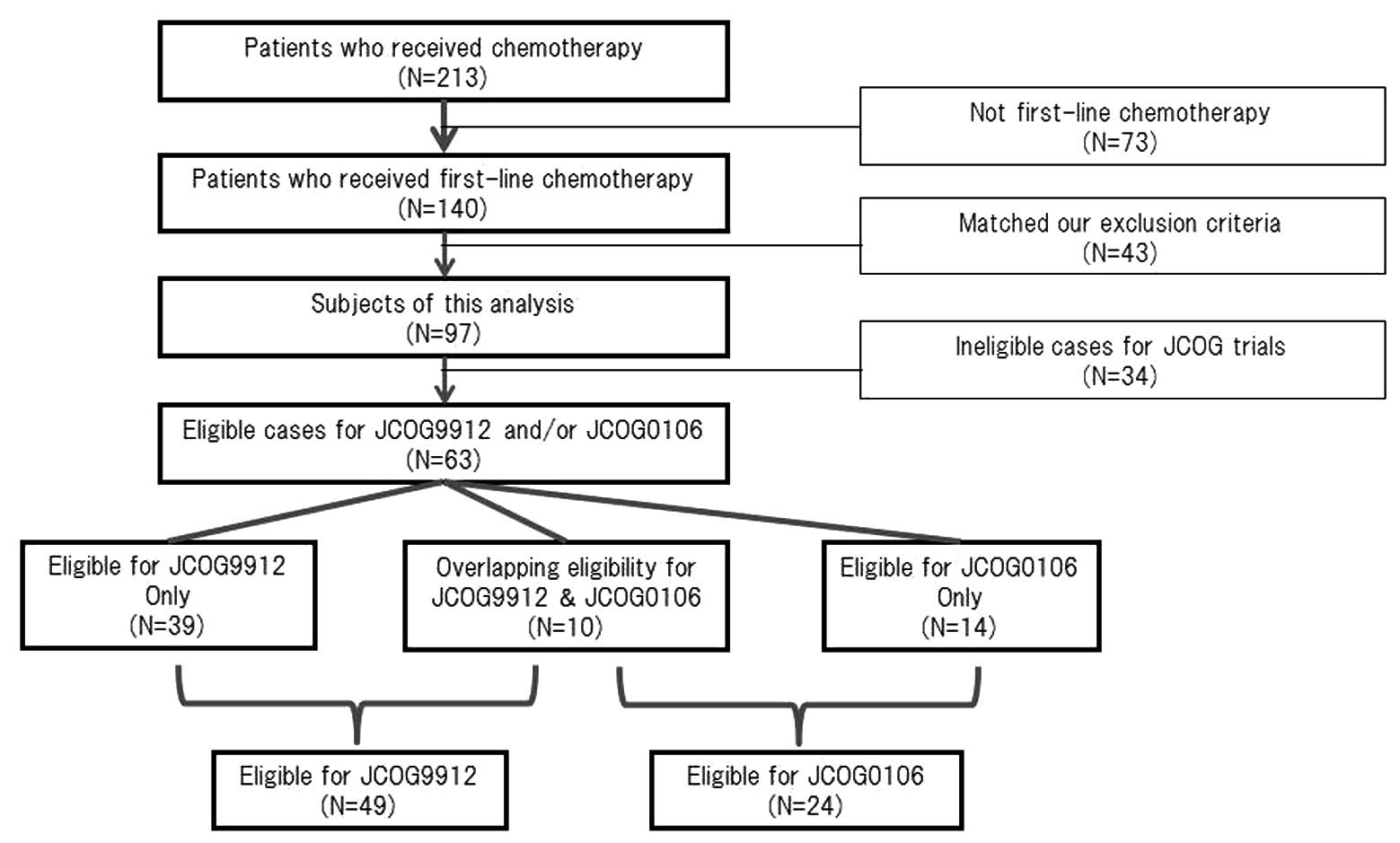
A total of 140 patients at TCC received first-line
chemotherapy. Of those patients, 43 were excluded as they matched
our exclusion criteria and the remaining 97 patients were reviewed
and included this analysis (Fig.
2).
The patient characteristics are summarized in
Table I. The patients included 67 men
and 30 women, with a median age of 65 years (range, 33–83 years). A
total of 43 patients had PM prior to chemotherapy, whereas the
remaining 54 patients did not have PM (non-PM).
 | Table I.Patient characteristics (n=97). |
Table I.
Patient characteristics (n=97).
| Characteristics | Patient no. |
| % |
|---|
| Age, years |
|
|
|
| Median
(range) |
| 65 (33–83) |
|
| Gender |
|
|
|
| Male | 67 |
| 69.0 |
|
Female | 30 |
| 31.0 |
| ECOG performance
status |
|
|
|
| 0 | 28 |
| 29.0 |
| 1 | 54 |
| 56.0 |
| 2 | 12 |
| 12.0 |
| 3 | 3 |
| 3.0 |
| Primary tumor |
|
|
|
| Yes | 44 |
| 45.0 |
| No | 53 |
| 55.0 |
| Histological
type |
|
|
|
|
Intestinal | 37 |
| 38.0 |
|
Diffuse | 51 |
| 53.0 |
|
Mixed | 9 |
| 9.0 |
| Metastatic site |
|
|
|
| Lymph
nodes | 46 |
| 47.0 |
|
Peritoneum | 43 |
| 44.0 |
|
Liver | 26 |
| 27.0 |
| Bone | 4 |
| 4.0 |
| Lung | 3 |
| 3.0 |
| Number of metastatic
sites |
|
|
|
| 1 | 1 |
| 1.0 |
| 2 | 66 |
| 68.0 |
| 3 | 30 |
| 31.0 |
Treatment regimens
The treatment regimens are outlined in Table II. The JCOG9912 and JCOG0106 trials
were conducted during the period of our analysis and 30% of the
patients at TCC were also enrolled in those trials. The median
survival time was 11.7 months and the median follow-up period of
the survivors was 17.5 months (range, 1.4–43 months).
| Table II.Treatment regimens. |
Table II.
Treatment regimens.
| Regimens | Patient no. | % |
|---|
| First-line
(n=97) |
| S-1 | 30 | 31.0 |
|
CPT/CDDP | 21 | 22.0 |
|
MTX/5-FU | 19 | 20.0 |
| 5-FU
continuous infusion | 16 | 16.0 |
|
Others | 11 | 11.0 |
| Multiple-line (n=59,
120 regimens) |
|
Paclitaxel (weekly) | 26 | 21.5 |
| Docetaxel
(tri-weekly) | 20 | 17.0 |
| S-1 | 18 | 15.0 |
|
CPT/CDDP | 15 | 12.5 |
|
MTX/5-FU | 12 | 10.0 |
| CPT | 12 | 10.0 |
|
Others | 17 | 14.0 |
Complications
As determined by our diagnostic criteria, the
following coexisting illnesses developed in our patients: bowel
obstruction, 28% (27/97), ascites, 26% (25/97), obstructive
jaundice, 10% (10/97), thrombosis, 7% (7/97) and hydronephrosis, 6%
(6/97) (Table III).
| Table III.Developed complications. |
Table III.
Developed complications.
| Complications | Patient no.
(n=97) | % |
|---|
| Bowel
obstruction | 27 | 28 |
| Ascites | 25 | 26 |
| Obstructive
jaundice | 10 | 10 |
| Thrombosis | 7 | 7 |
| Hydronephrosis | 6 | 6 |
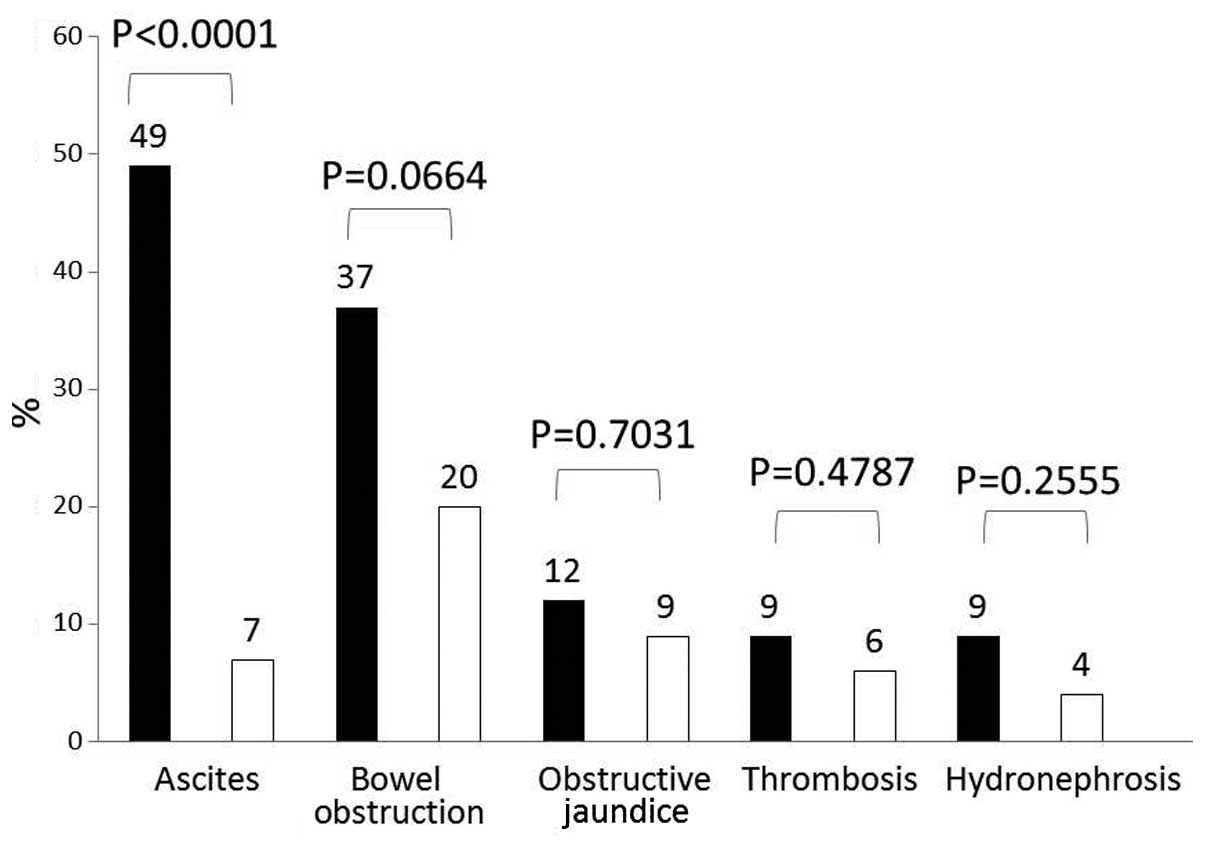
In total, 43 (44%) of our patients had GC with PM
(Fig. 1). Of these patients, 16 (37%)
developed bowel obstruction, whereas the prevalence of this
condition in non-PM patients was only 20% (P=0.0664). There was a
statistically significant difference between the two groups
regarding the development of ascites, with 21 (49%) of the PM
patients compared to only 4 (7%) of the non-PM patients (P=0.0001).
Obstructive jaundice (n=5, 12%), thrombosis (n=4, 9%) and
hydronephrosis (n=4, 9%) were also encountered more frequently
among patients with PM compared to those without PM.
Discussion
The findings of this retrospective study
demonstrated that <1/3 of the patients with advanced or
recurrent GC developed ascites or bowel obstruction, with a higher
frequency among patients with PM. However, development of
obstructive jaundice, thrombosis and hydronephrosis was observed in
<10% of the patients. There were no differences with regards to
metastatic sites.
In phase III trials of metastatic GC, the frequency
of patients with PM is ~20–30%. Although the rate of PM is very
similar between Western countries and Japan, there is a difference
in the frequency of non-target lesions according to the Response
Evaluation Criteria In Solid Tumors (RECIST) criteria (15). It is generally considered that the
majority of the patients with non-target lesions are patients with
PM. The rates of non-target lesions in Japanese trials are higher
compared to those in Western trials. One of the reasons for this
difference is the eligibility criteria; Japanese trials tend to
allow enrollment of patients with vey small metastases that cannot
be detected by imaging techniques, but are detectable only by
laparotomy. This may provide an explanation as to why patients with
PM in the JCOG9912 trial had a better outcome compared to the
patients enrolled in Western trials (1–16).
Although several other studies have described PM as
a prognostic factor for survival (16–18), the
Japanese Clinical Oncology Group (JCOG) indicated in the JCOG9912
trial that PM was not a significant factor (19). The JCOG0106 clinical trial, a phase
III, non-platinum comparison trial with eligibility limited only to
patients with PM (20), was conducted
during the same period by JCOG; patients with extensive PM were not
enrolled in this trial due to poor prognosis and the severe
toxicity. It is possible that certain investigators preferred to
enroll patients with moderate PM in the less toxic JCOG0106
trial.
The JCOG trials assigned patients with PM into two
different studies. However, 16% (10/63) of the eligible cases
included in the two JCOG trials overlapped (Fig. 2). Selection bias is one reason why the
prognostic index of JCOG differed from those of other analyses and
any evaluation of their results of a prognostic index should be
performed with caution.
Our data suggest unique trends of PM and the present
treatment strategy for PM appears to be reasonable. However, there
is currently no widely accepted specific treatment for PM; JCOG
failed to demonstrate a clear strategy in two trials limited only
to patients with PM (JCOG0106 and JCOG0407). Japanese investigators
are attempting to establish a PM limited strategy in one of two
manners: one group of investigators intends to achieve a survival
benefit by intraperitoneal direct infusional chemotherapy (21), similar to the treatment of ovarian
cancer, whereas another group is investigating non-platinum
systemic treatment with a paclitaxel-based regimen for PM-limited
disease (22).
An ongoing trial in cooperation with the West Japan
Oncology Group (WJOG) has already completed enrollment and is
partly considering the unique clinical course of PM. The WJOG4007
trial, comparing second-line treatment with irinotecan or
paclitaxel, is not limited to PM patients. Even if the prevalence
of PM is not extensive at the time of enrollment, it is expected
that ~1/3 of the patients will develop PM during cancer
progression. A proportion of the PM patients are likely to develop
bowel obstruction and would in turn lose their opportunity to
receive irinotecan, due to its poor elimination from the intestine
and liver. The majority of oncologists tend to avoid selecting
irinotecan as a first-line treatment for patients with PM due to
its characteristic excretion mechanism. However, certain
experienced gastrointestinal oncologists predict disease
progression and the development of PM and, therefore, prefer to use
irinotecan as early as possible, suggesting that, by using all
active chemotherapeutic agents, including irinotecan, patients may
achieve a survival benefit.
Our data did not elucidate at which timepoint the
complications occur. It is considered that disease progression in
cases with PM is closely associated with bowel obstruction and
ascites. In general, bowel obstruction and ascites represent
typical symptoms and clinical evidence of disease progression in GC
patients with PM. It is difficult to assess disease progression in
patients with small PM. Japanese investigators recently reported
that progression-free survival does not directly reflect on overall
survival in GC (23). There may be
several reasons for this and we hypothesized that one of the
possible explanations is the unique clinical characteristics of PM
in GC. The majority of the patients with PM do not have RECIST
target lesions; thus, it is very difficult to define a distinct
point of disease progression. When conducting control trials by
using progression-free survival as a primary endpoint in GC, we
must consider enrolling only patients who have target lesions,
while indirectly considering bowel obstruction and ascites as
progression events.
Our data also suggests that we should consider a
change of active regimens in patients with PM when there are
clinical symptoms of bowel obstruction and ascites without any
definitive progression of metastases on imaging. In the presence of
bowel obstruction and massive ascites, it is impossible to continue
with anticancer treatment, unless the patient's clinical condition
is reversed. The clinical characteristics of patients with PM of GC
are unique and it is crucial to consider PM as a predictive sign
and an important factor when making clinical decisions and
developing treatment strategies.
References
|
1
|
Wils JA, Klein HO, Wagener DJT, et al:
Sequential high-dose methotrexate and fluorouracil combined with
doxorubicin – a step ahead in the treatment of advanced gastric
cancer: a trial of the european organization for research and
treatment of cancer gastrointestinal tract cooperative group. J
Clin Oncol. 9:827–831. 1991.PubMed/NCBI
|
|
2
|
Vanhoefer U, Rougier P, Wilke H, et al:
Final results of a randomized phase III trial of sequential
high-dose methotrexate, fluorouracil and doxorubicin versus
infusional fluorouracil and cisplatin in advanced gastric cancer: a
trial of the european organization for research and treatment of
cancer gastrointestinal tract cancer cooperative group. J Clin
Oncol. 18:2648–2657. 2000.PubMed/NCBI
|
|
3
|
Ohtsu A, Shimada Y, Shirao K, et al:
Randomized phase III trial of fluorouracil alone versus
fluorouracil plus cisplatin versus uracil and tegafur plus
mitomycin in patients with advanced gastric cancer: JCOG study
9205. J Clin Oncol. 21:54–59. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Webb A, Cunningham D, Scarffe JH, et al:
Randomized trial comparing epirubicin, cisplatin and fluorouracil
versus fluorouracil, doxorubicin and methotrexate in advanced
esophagogastric cancer. J Clin Oncol. 15:261–267. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Dank M, Zaluski J, Barone C, et al:
Randomized phase III study comparing irinotecan combined with
5-fluorouracil and folinic acid to cisplatin combined with
5-fluorouracil in chemotherapy naive patients with advanced
adenocarcinoma of the stomach or esophagogastric junction. Ann
Oncol. 19:1450–1457. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Cunningham D, Starling N, Rao S, et al:
Capecitabine and oxaliplatin for advanced esophagogastric cancer. N
Engl J Med. 358:36–46. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Van Cutsem E, Moiseyenko VM, Tjulandin S,
et al: V325 Study Group: Phase III study of docetaxel and cisplatin
plus fluorouracil compared with cisplatin and fluorouracil as
first-line therapy for advanced gastric cancer: a report of the
V325 Study Group. J Clin Oncol. 24:4991–4997. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ajani JA, Rodriguez W, Bodoky G, et al:
Multicenter phase III comparison of cisplatin/S-1 with
cisplatin/infusional fluorouracil in advanced gastric or
gastroesophageal adenocarcinoma study: the FLAGS trial. J Clin
Oncol. 28:1547–1553. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Boku N, Yamamoto S, Fukuda H, et al:
Fluorouracil versus combination of irinotecan plus cisplatin versus
S-1 in metastatic gastric cancer: a randomized phase 3 study.
Lancet Oncol. 10:1063–1069. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Koizumi W, Narahara H, Hara T, et al: S-1
plus cisplatin versus S-1 alone for first-line treatment of
advanced gastric cancer (SPIRITS trial): a phase III trial. Lancet
Oncol. 9:215–221. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Narahara H, Iishi H, Imamura H, et al:
Randomized phase III study comparing the efficacy and safety of
irinotecan plus S-1 with S-1 alone as first-line treatment for
advanced gastric cancer (study GC0301/TOP-002). Gastric Cancer.
14:72–80. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kang YK, Kang WK, Shin DB, et al:
Capecitabine/cisplatin versus 5-fluorouracil/cisplatin as
first-line therapy in patients with advanced gastric cancer: a
randomised phase III noninferiority trial. Ann Oncol. 20:666–673.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Bang YJ, Cutsem E, Feyereislova A, et al:
ToGA Trial Investigators: Trastuzumab in combination with
chemotherapy versus chemotherapy alone for treatment of
HER2-positive advanced gastric or gastro-oesophageal junction
cancer (ToGA): a phase 3, open-label, randomised controlled trial.
Lancet. 376:687–697. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Chau I, Norman AR, Cunningham D, Waters
JS, Oates J and Ross PJ: Multivariate prognostic factor analysis in
locally advanced and metastatic esophago-gastric cancer. Pooled
analysis from three multicenter, randomized, controlled trials
using individual patient data. J Clin Oncol. 22:2395–2403. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Therasse P, Arbuck SG, Eisenhauer EA, et
al: New guidelines to evaluate the response to treatment in solid
tumors. European Organization for Research and Treatment of Cancer,
National Cancer Institute of the United States, National Cancer
Institute of Canada. J Natl Cancer Inst. 92:205–216. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kim JG, Ryoo BY, Park YH, et al:
Prognostic factors for survival of patients with advanced gastric
cancer treated with cisplatin-based chemotherapy. Cancer Chemother
Pharmacol. 61:301–307. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Lee SS, Lee JL, Ryu MH, et al: Combination
chemotherapy with capecitabine (X) and cisplatin (P) as first line
treatment in advanced gastric cancer: experience of 223 patients
with prognostic factor analysis. Jpn J Clin Oncol. 37:30–37. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Lee J, Lim T, Uhm JE, et al: Prognostic
model to predict survival following first-line chemotherapy in
patients with metastatic gastric adenocarcinoma. Ann Oncol.
18:886–891. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Takahari D, Takashima A, Mizusawa J, et
al: Prognostic factors in Japanese patients with advanced gastric
cancer using the data from JCOG9912 study. Proc ASCO. abstract no.
4059. 2011.
|
|
20
|
Shirao K, Boku N, Yamada Y, Yamaguchi K,
Doi T, Takiuchi H, et al: Randomized phase III study of
5-fluorouracil continuous infusion (5FUci) versus methotrexate and
5-FU sequential therapy (MF) in gastric cancer with peritoneal
metastasis (JCOG0106). Proc ASCO. abstract no. 4545. 2009.
|
|
21
|
Ishigami H, Kitayama J, Kaisaki S,
Hidemura A, Kato M, Otani K, et al: Phase II study of weekly
intravenous and intraperitoneal paclitaxel combined with S-1 for
advanced gastric cancer with peritoneal metastasis. Ann Oncol.
21:67–70. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Matsubara J, Shimada Y, Takashima A, et
al: A phase i study of bolus 5-fluorouracil and leucovorin combined
with weekly paclitaxel (FLTAX) as first-line therapy for advanced
gastric cancer. Jpn J Clin Oncol. 38:540–546. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Fuse N: Progression-free survival as
surrogate endpoint of overall survival in patients with
advanced/recurrent gastric cancer: individual patient data analysis
on 4,102 patients from 20 randomized trials. Proc JSCO: Plenaly.
1:2011.
|