Introduction
Screening of asymptomatic men based on the serum
level of prostate-specific antigen (PSA) coupled with the use of
ultrasound-guided random systematic prostate biopsy has
significantly improved the diagnostic accuracy and treatment of
prostate cancer (1). The incidence of
prostate cancer and its associated mortality rates have also
increased significantly in numerous countries, including Japan
(2). Despite significant progress in
the detection and treatment of prostate cancer, high relapse rates
(20–57%) following radical prostatectomy have been problematic, and
various neoadjuvant therapies have been examined with the aim of
reducing the rate of relapse (3–5). However,
numerous patients have locally advanced disease at diagnosis, and
therefore novel therapeutic options are required.
Treatment that involves a combination of surgery
with adjuvant therapy may conceivably improve the outcome of
patients who have a high risk of recurrence. Neoadjuvant therapy
prior to surgery has several advantages over adjuvant therapy, as
it targets presumed micro-metastases at an early stage and may
reduce locally advanced tumors, thus allowing more effective
surgical resection.
Gene therapy may offer a chance of surmounting the
drawbacks of current therapies by inducing cytotoxicity in
localized prostate cancer without serious morbidity or mortality,
and stimulating immune-mediated therapeutic activities that affect
not only the primary tumor but also metastases. Several protocols
of gene therapy for prostate cancer have been examined in
preclinical studies and clinical trials. Intraprostatic adenoviral
vector transduction of the herpes simplex virus-thymidine kinase
(HSV-tk) gene followed by intravenous ganciclovir (GCV)
administration is a cytotoxic gene therapy approach for prostate
cancer that has been tested extensively in preclinical studies and
phase I/II clinical trials at Baylor College of Medicine (Houston,
TX, USA) (6–8). The HSV-tk gene product, which
lacks the enzyme encoded in mammalian cells, efficiently
phosphorylates GCV, which is subsequently incorporated into newly
synthesized DNA during cellular division, causing termination of
DNA synthesis and cell death (9).
This in situ gene therapy approach involves the ‘bystander
effect,’ in which tumor cells close to HSV-tk-expressing
cells are also killed (10–12). Baylor College of Medicine has
demonstrated the safety of HSV-tk gene therapy for prostate
cancer.
Previous studies have reported that activated human
leukocyte antigen (HLA)-DR+ cluster of differentiation
8+ (CD8+) T cells are increased in patients
treated with adenoviral vector-mediated HSV-tk gene delivery
followed by GCV injection (8,13,14).
However, the details of the resulting immune responses were not
clear.
In the present study, the immune responses in
patients who were repeatedly administered GCV intravenously
following intraprostatic HSV-tk injection over a period of 2 weeks
were investigated. Central memory (CM) CD8+ T cells in
peripheral blood were clearly and efficiently increased during the
second round of HSV-tk + GCV treatment, and prostate cancer antigen
(PCa)-specific T cells were also increased.
Materials and methods
Patients
The study subjects were five patients with
clinically localized prostate cancer with a high risk of recurrence
who underwent prostate biopsy (Table
I). All the patients had a Kattan preoperative nomogram score
of 115, and provided study-specific informed consent prior to
enrollment in the phase I/II clinical trial, which was approved by
the Institutional Review Board of Kitasato University (Sagamihara,
Kanagawa, Japan) and the Ministry of Health, Labour and Welfare of
Japan.
 | Table I.Characteristics of the patients
treated with repeated HSV-tk + GCV injections. |
Table I.
Characteristics of the patients
treated with repeated HSV-tk + GCV injections.
| Patient | Age, years | PSA, ng/ml | Clinical stage | Gleason score |
|---|
| Pt1 | 70 | 13.7 | T2c | 3+3 |
| Pt2 | 63 | 6.6 | T2b | 3+5 |
| Pt3 | 60 | 44.1 | T2c | 4+3 |
| Pt4 | 68 | 7.8 | T2b | 4+3 |
| Pt5 | 71 | 28.9 | T2b | 3+3 |
Vector
The vector used was a serotype Ad5 adenovirus that
contained the HSV-tk gene and Rous sarcoma virus long
terminal repeat promoter in the region of the excised E1/E2
wild-type adenoviral genes. This replication-defective adenoviral
vector was constructed, as described previously (14). A clinical-grade preparation was made
by the Baylor Center for Cell and Gene Therapy, Gene Vector
Laboratory under good manufacturing practice conditions. All the
patients received 2×1011 viral particles of the vector
into the prostate using a transrectal approach under ultrasound
guidance.
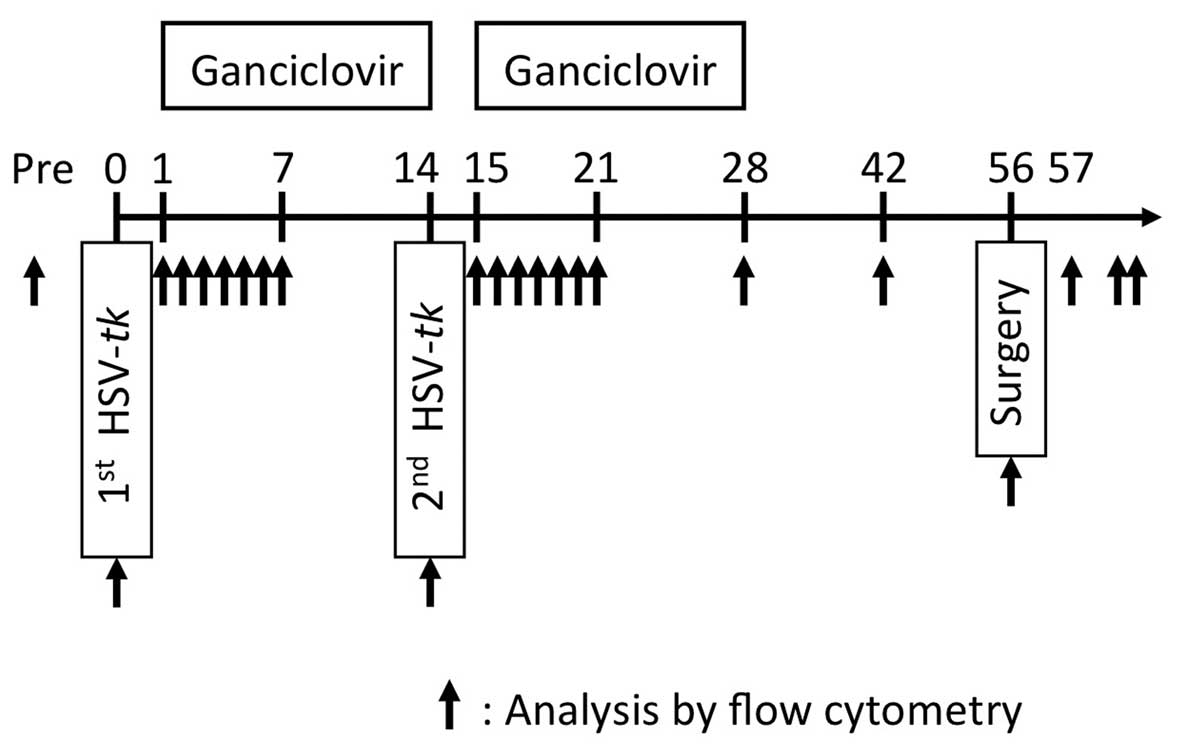
Treatment course
The five patients underwent repeated intraprostatic
injection of HSV-tk for 2 weeks with intravenous GCV. After a
further 4 weeks, four of the patients underwent radical
prostatectomy (Fig. 1). One patient
was switched to radiotherapy instead of radical prostatectomy due
to a prolonged activated partial thromboplastin time.
Lymphocyte immunophenotyping
Heparin-treated blood (100 µl) was incubated with
the following fluorescence-conjugated monoclonal antibodies (mAbs):
CD3/CD19 (cat. no. 349211), CD3/CD8 (cat. no. 340044), CD3/CD4
(cat. no. 340043), CD8/HLA-DR (cat. no. 349528), CD4/HLA-DR (cat.
no. 340771), CD3/HLA-DR (cat. no. 340573) [all fluorescein
isothiocyanate/phycoerythrin (FITC/PE); Becton, Dickinson and Co.,
San Jose, CA, USA], CD45RO (PE-Texas Red), CD62L (FITC) and CCR7
(PE) (Beckman Coulter, Inc., Brea, CA, USA). After incubation at
room temperature for 15 min, red blood cells were lysed with BD
FACS lysing solution (Becton, Dickinson and Co.). Forward light
scatter and side light scatter were set to distinguish the
lymphocyte, macrophage and granulocyte population from debris with
an EPICS XL flow cytometer (Beckman Coulter, Inc.). Multi-color
immunofluorescence analysis was performed using 10,000 lymphocytes
for each analysis.
Intracellular interferon (IFN)-γ
assay
Peripheral blood mononuclear cells (PBMC) were
stimulated with prostatic acid phosphatase (PAP) or NY-ESO-1
peptides that were 15 amino acids in length, overlapping by 11
amino acids at a concentration of 1 mg/ml (Miltenyi Biotec GmbH,
Bergisch Gladbach, Germany). Simultaneously, monesin (200 µM) was
added to block protein transport. After 16 h of incubation, the
peptide-stimulated PBMC were stained with anti-CD3 (FITC), anti-CD4
(PE-Vio770) and anti-CD8 (APC-Vio770) mAbs (Miltenyi Biotec GmbH).
For IFN-γ staining, the peptide-stimulated PBMCs were treated with
FACS Perm2 (Becton, Dickinson and Co.) and stained with anti-IFN-γ
(PE) mAb (Beckman Coulter, Inc.). IFN-γ-producing T cells were
analyzed using a MACSQuant flow cytometer (Miltenyi Biotec
GmbH).
Statistics
Statistical significance was analyzed using the
Mann-Whitney U test. P<0.05 was considered to indicate a
statistically significant difference.
Results
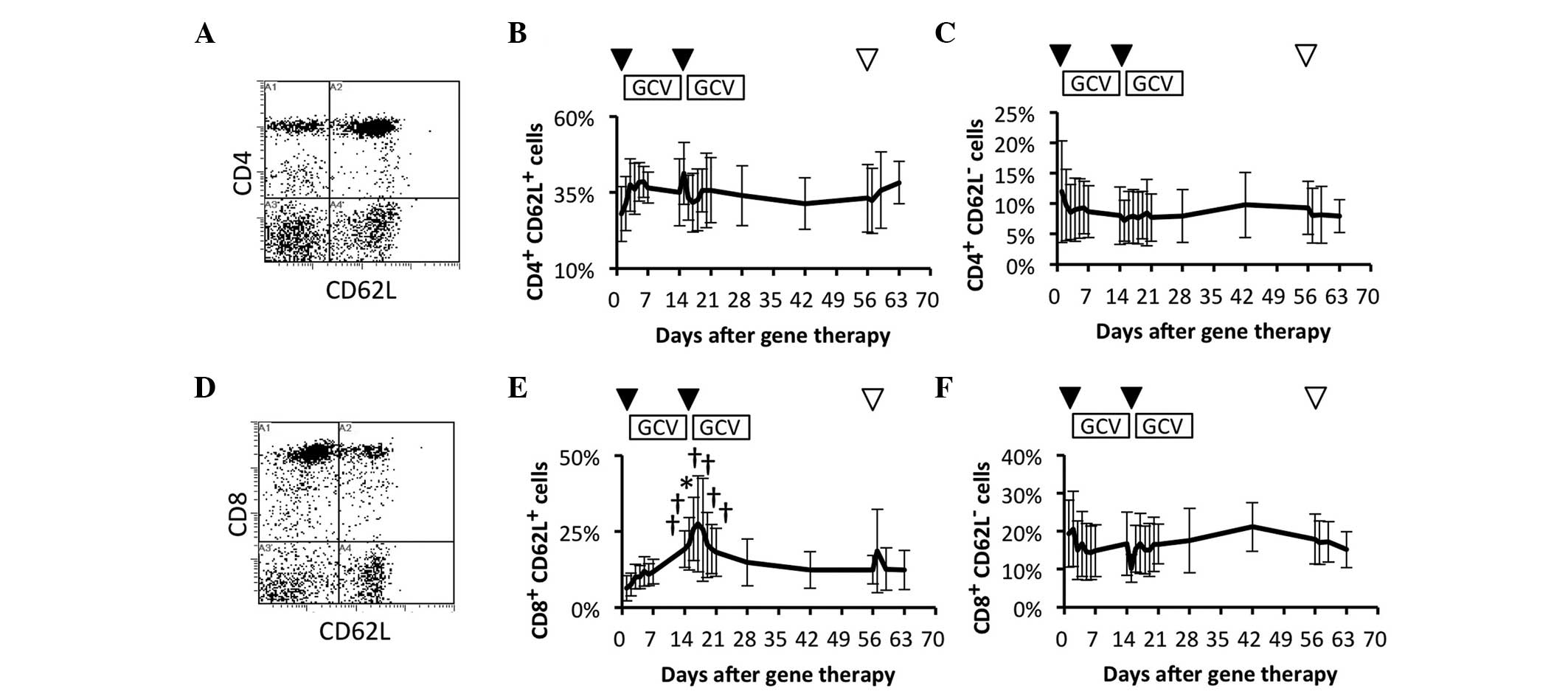
Comparison of circulating naïve and
effector T cell subsets
To study the efficacy of the immune system, whether
the frequency of naïve and effector cells in peripheral blood was
affected by the repeated HSV-tk + GCV treatment was investigated.
The frequency of naïve and effector cells were compared in the
circulating CD4+ T cell subsets prior and subsequent to
the HSV-tk + GCV treatment (Fig. 2A).
Naïve and a proportion of the memory T cell subsets
(CD4+ CD62L+) were immediately and slightly
increased following the 1st and 2nd HSV-tk vector injections, but
there were no significant increases in comparison to the frequency
of the CD4+ CD62L+ T cell subsets prior to
the treatment (Fig. 2B). In contrast
to the CD4+ CD62L+ T cell subsets, there was
no significant difference in the effector (CD4+
CD62L–) T cell subset during the observation period
(Fig. 2C). The frequency of naïve and
effector cells were also compared among the circulating
CD8+ T cell subsets prior and subsequent to the repeated
HSV-tk + GCV treatment (Fig. 2D).
Naïve and a proportion of memory T cell subsets (CD8+
CD62L+) were gradually increased following the 1st
HSV-tk + GCV treatment. This was followed by a significant increase
during the 2nd HSV-tk + GCV treatment, in comparison with the
frequency of CD8+ CD62L+ T cell subsets prior
to the treatment (Fig. 2E). In
contrast to the CD8+ CD62L+ T cell subsets,
the effector (CD8+CD62L–) T cell subset
showed no significant change during the observation period
(Fig. 2F). These results suggested
that naïve, and a proportion of memory CD8+ T cells,
were possibly affected by the repeated HSV-tk + GCV treatments.
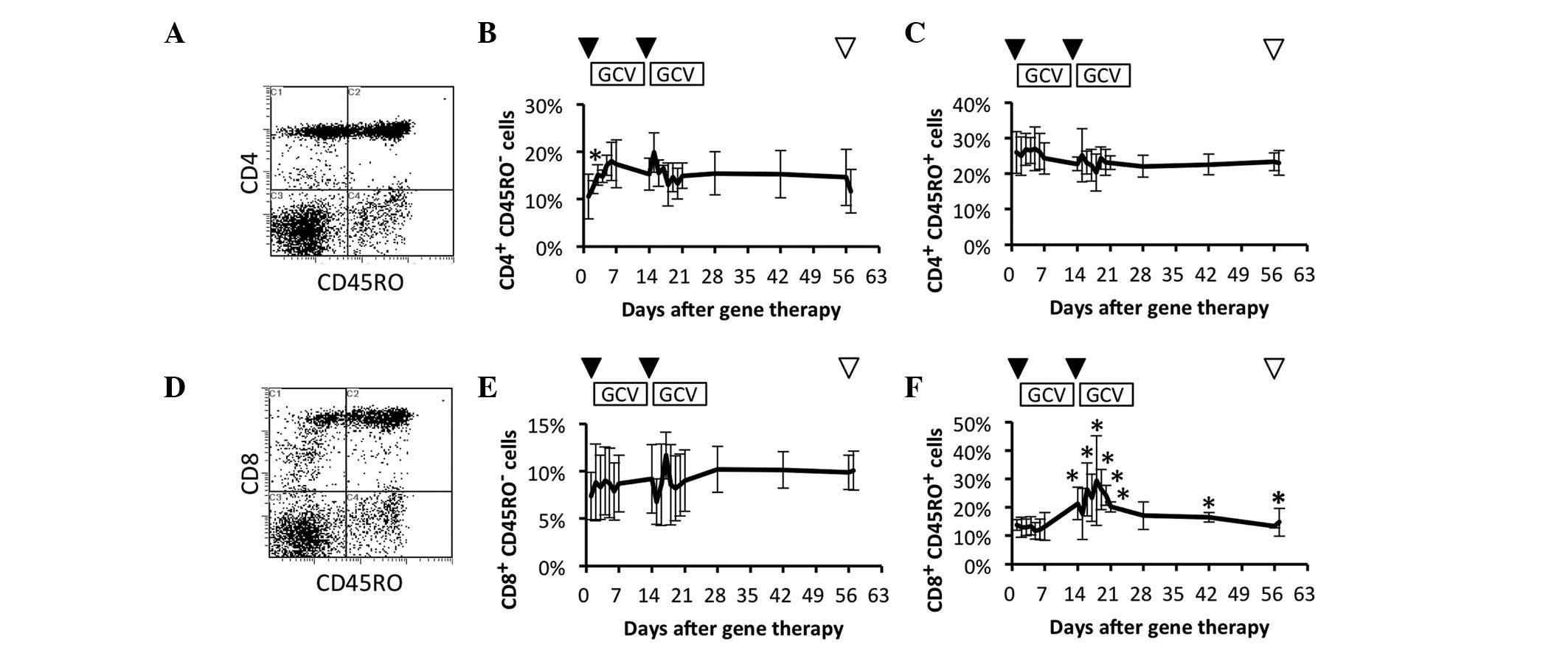
Comparison of circulating naïve and
memory T cell subsets
To clarify which of the naïve and memory T cell
subsets were effectively increased, these subsets were investigated
in patients who had received repeated HSV-tk + GCV treatment. The
frequencies of circulating naïve and memory CD4+ T cell
subsets were compared prior and subsequent to HSV-tk + GCV
treatment (Fig. 3A). The naïve T cell
(CD4+ CD45RO–) subset was significantly
increased on day 2 after the 1st HSV-tk vector injection in
comparison to the frequency prior to treatment (Fig. 3B). In contrast to the naïve
CD4+ T cell subset, the memory T cell subset
(CD4+ CD45RO+) showed no significant change
during the observation period (Fig.
3C). The frequencies of circulating naïve and memory
CD8+ T cell subsets were compared prior and subsequent
to the HSV-tk + GCV treatment (Fig.
3D). The naïve T cell (CD8+ CD45RO–)
subset showed no significant change during the observation period
(Fig. 3E). By contrast, the memory T
cell (CD8+ CD45RO+) subset was significantly
increased following the 2nd HSV-tk + GCV treatment in comparison to
the frequency of the naïve CD8+ T cell subset prior to
treatment. A significant increase of the CD8+
CD45RO+ T cell subset was further observed on days 42
and 56 after the 1st HSV-tk vector injection (Fig. 3F). These results suggested that memory
CD8+ T cells were clearly and more effectively increased
by repeated HSV-tk + GCV treatment.
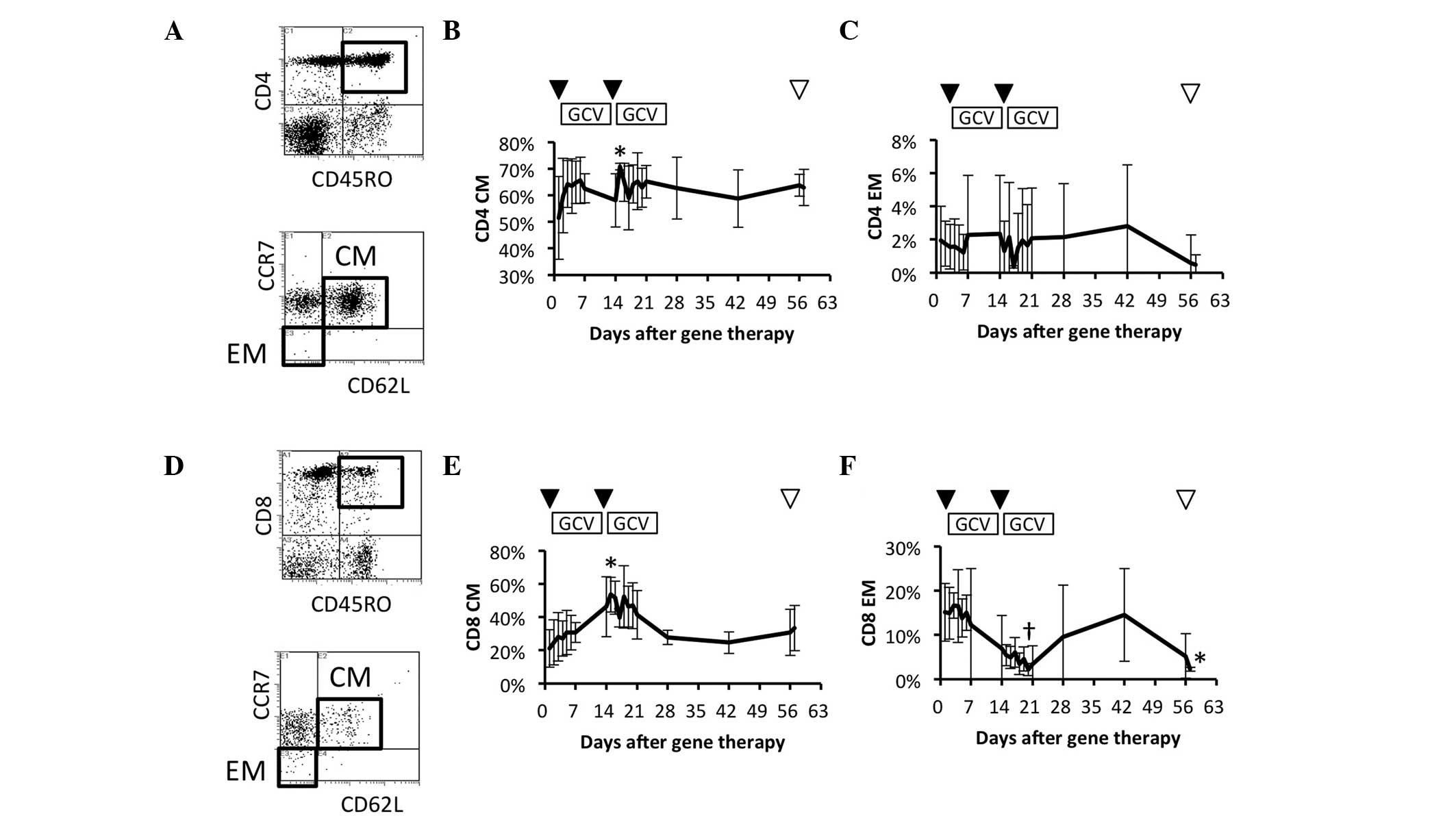
Comparison of circulating memory T
cell subsets
To further study the details of memory T cell
responses in patients who had received the repeated HSV-tk + GCV
treatment, the frequencies of the circulating CM
(CD45RO+ CD62L+ CCR7+) and
effector memory (EM) (CD45RO+ CD62L–
CCR7–) CD4+ T cell subsets were examined
(Fig. 4A). CM CD4+ T cells
increased gradually during the 1st HSV-tk + GCV treatment, and were
significantly increased on day 2 after the 2nd HSV-tk vector
injection (Fig. 4B). In contrast to
CM CD4+ T cells, the EM CD4+ T cell subset
showed no significant change during the observation period
(Fig. 4C). The frequency of
circulating CM (CD45RO+ CD62L+
CCR7+) and EM (CD45RO+ CD62L–
CCR7–) CD8+ T cell subsets were also compared
prior and subsequent to the repeated HSV-tk + GCV treatment
(Fig. 4D). CM CD8+ T cells
increased gradually during the 1st HSV-tk + GCV treatment, and
their frequency was maximal and most significant on day 2 after the
2nd HSV-tk vector injection, in comparison with the frequency prior
to treatment (Fig. 4E). By contrast,
the EM CD8+ T cell subset decreased gradually during the
2nd HSV-tk + GCV treatment, and showed the lowest frequency on day
7 after the 2nd HSV-tk vector injection (Fig. 4F). These results suggested that CM
CD4+ and CD8+ T cells were effectively
increased following repeated HSV-tk vector injection, whereas it
appeared that EM CD8+ T cells were induced to migrate
from blood vessels to the local environment.
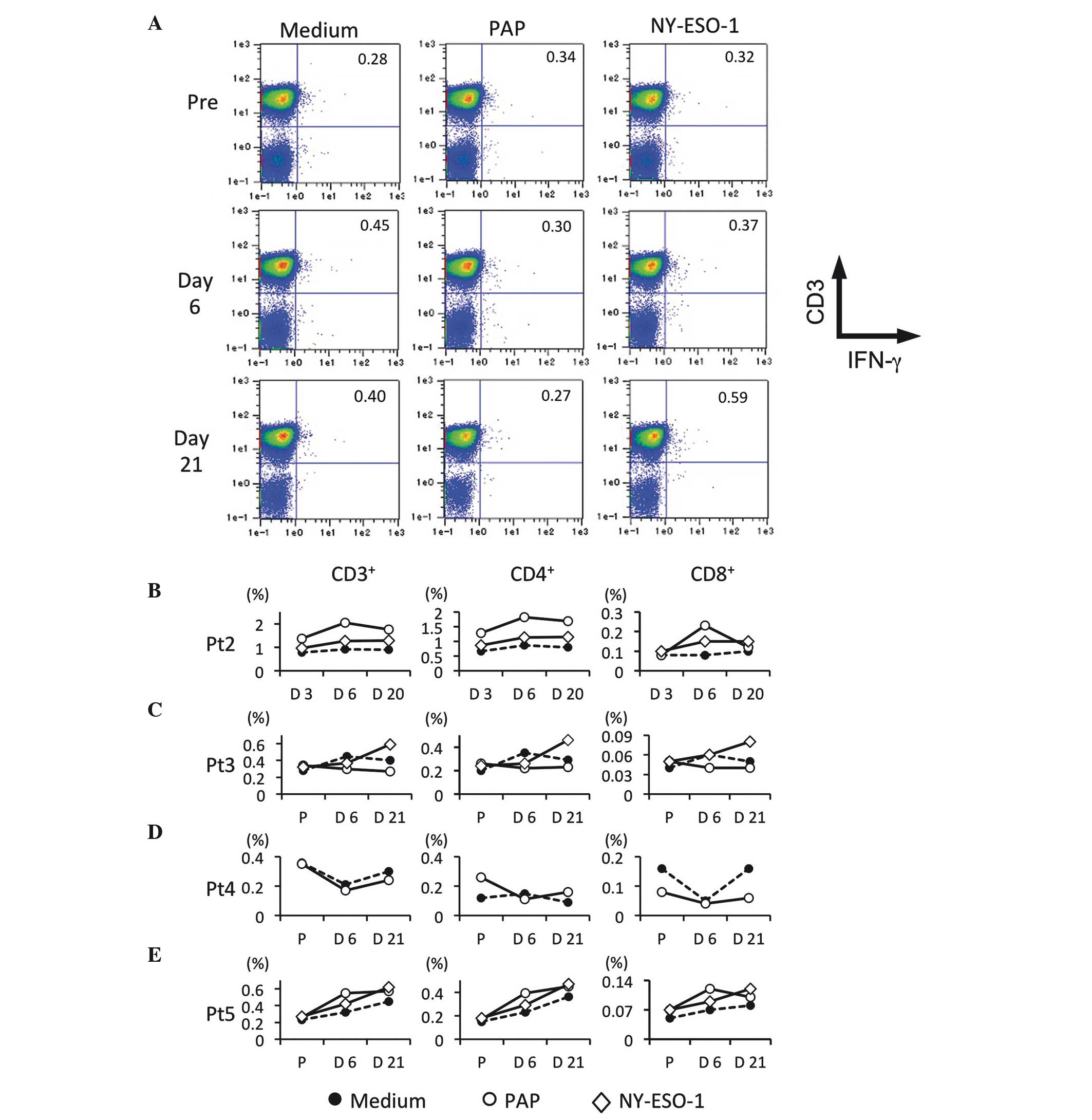
Detection of PCa-specific T cells
To study whether PCa-specific T cells were also
increased by repeated HSV-tk + GCV treatment, the IFN-γ-producing T
cells in patients following stimulation with PAP and
NY-ESO-1-overlapping peptides were detected. Fig. 5A shows representative flow-cytometric
data for tumor antigen-specific IFN-γ producing T cells prior and
subsequent to HSV-tk vector injection (Fig. 5A). In patient 2, PAP-specific T cells
were maximally increased on day 6 after the 1st HSV-tk vector
injection, whereas NY-ESO-1-specific T cells were slightly
increased (Fig. 5B). In patient 3,
NY-ESO-1-specific T cells were clearly increased following repeated
HSV-tk + GCV treatment, whereas PAP-specific T cells were slightly
increased on day 6 after the 1st HSV-tk vector injection in
comparison to PCa-specific T cells prior to treatment (Fig. 5C). In patient 4, PAP-specific T cells
were only examined, and no difference was observed prior and
subsequent to the treatment (Fig.
5D). In patient 5, an increase of PAP-specific T cells on day 6
after the 1st HSV-tk vector injection was observed, whereas
NY-ESO-1-specific T cells increased after the 2nd injection of
HSV-tk vector, in comparison to PCa-specific T cells prior to
treatment (Fig. 5E). Although
PAP-specific T cells were increased following the 1st injection of
HSV-tk vector, NY-ESO-1-specific T cells appeared to be increased
following the 2nd injection. These results suggested that PCa
antigen-specific T cells may be efficiently induced by repeated
treatment with HSV-tk + GCV.
Discussion
Gene therapy is a promising experimental approach
for prostate cancer. Numerous in vitro and animal studies
have shown that HSV-tk is effective against prostate cancer cell
lines and prostate tumors grown in animals (15–18).
However, its efficacy and immune responses in human prostate cancer
patients are not well defined. In the present study, the dynamics
of systemic T cell subsets and prostate cancer-derived
antigen-specific T cells were investigated, and it was identified
that they were efficiently increased in patients who received
repeated treatment with HSV-tk + GCV.
Several preclinical studies have shown that tumors
treated with HSV-tk + GCV contain areas of necrosis highlighted by
infiltration of macrophages, CD4+ and CD8+ T
cells (11,12,19,20).
Additionally, interleukin (IL)-1, IL-2, IL-6, IL-12, IFN-γ, tumor
necrosis factor-α and granulocyte macrophage colony-stimulating
factor are detectable in tumors following HSV-tk + GCV treatment
(19,21). Furthermore, previous studies have
indicated that circulating total CD8+ and activated
CD8+ T cells are significantly increased 2 weeks after
injection of HSV-tk vector (8,13,14). Our previous study reported the
dynamics of circulating lymphocyte subsets in patients who had
received repeated HSV-tk + GCV treatment (22). Total CD8+ and activated
CD8+ T cells were significantly and efficiently
increased by this type of treatment, particularly following the 2nd
round of treatment. However, it was not clear whether the increased
CD8+ T cells were specifically active against prostate
cancer antigens. Previous studies have utilized adenoviral vectors
for suicide gene delivery to prostate tumors as a form of
neoadjuvant therapy (14,23,24). These
increased CD8+ T cells possibly represent an immune
response to adenovirus. van der Linden et al (24) reported that adenovirus-specific
neutralizing antibody responses are clearly enhanced in patients
who received adenovirus-mediated suicide gene therapy. The study
further demonstrated that adenovirus-specific PBMC proliferation
and IFN-γ production occurred in vitro. By contrast, van der
Linden et al (24) also found
no correlation between anti-adenovirus antibody titers
(neutralizing antibody) and the PSA response. To the best of our
knowledge, the present study is the first to indicate that repeated
HSV-tk + GCV treatment can efficiently induce circulating CM
CD8+ T cells and PCa-specific T cell responses in human
patients. The high rate of relapse of prostate cancer following
surgery is clinically problematic. Although radical prostatectomy
is intended to be curative, the high recurrence rates of prostate
cancer may be due to minimal residual disease (MRD) following
surgery. To eliminate MRD, induction of memory T cells, which are
also involved in immunological surveillance for adaptive immunity,
may be important.
In the present study, circulating memory
CD8+ T cells were more effectively increased compared to
memory CD4+ T cells, whereas IFN-γ-producing
PCa-specific CD4+ T cells were more efficiently induced
compared to IFN-γ-producing PCa-specific CD8+ T cells.
PAP and NY-ESO-1 overlapping peptides were utilized to stimulate
PCa-specific T cells. These peptides were 15 amino acids in length,
overlapping by 11 amino acids. These overlapping peptides may be
presented more easily by the major histocompatibility complex
(MHC)-II on antigen-presenting cells compared to MHC-I. Cytopathic
and bystander effects appeared to be efficiently induced by this
repeated HSV-tk + GCV treatment. As a result, prostate
cancer-associated antigens may be released from cytopathic areas,
thus initiating PCa-specific T cell responses in patients.
In conclusion, the present study reported evidence
of systemic T cell responses following repeated HSV-tk + GCV
treatment. CM CD8+ T cells and PCa-specific T cells in
peripheral blood were enhanced following injection of the vector,
suggesting the potential for activation of components of the
cell-mediated immune response in the clinical trial. This
cell-mediated immune response may contribute to a reduction of
relapse rates in patients with prostate cancer. This repeated
treatment with HSV-tk + GCV is expected to be promising for
neoadjuvant therapy.
Acknowledgements
The present study was supported by a grant from the
Japanese Ministry of Education, Culture, Sports, Science and
Technology (Grant-In-Aid for Scientific Research C21592060), Japan
Science and Technology Agency and Asahi Kasei Pharma Urological
Academy.
Glossary
Abbreviations
Abbreviations:
|
HSV-tk
|
herpes simplex virus-thymidine
kinase
|
|
GCV
|
ganciclovir
|
|
CM
|
central memory
|
|
EM
|
effector memory
|
|
PAP
|
prostatic acid phosphatase
|
|
PCa
|
prostate cancer
|
References
|
1
|
Jones GW, Mettlin C, Murphy GP, et al:
Patterns of care for carcinoma of the prostate gland: Results of a
national survey of 1984 and 1990. J Am Coll Surg. 180:545–554.
1995.PubMed/NCBI
|
|
2
|
Center MM, Jemal A, Lortet-Tieulent J,
Ward E, Ferlay J, Brawley O and Bray F: International variation in
prostate cancer incidence and mortality rates. Eur Urol.
61:1079–1092. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ohori M, Wheeler TM, Kattan MW, Goto Y and
Scardino PT: Prognostic significance of positive surgical margins
in radical prostatectomy specimens. J Urol. 154:1818–1824. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Zietman AL, Edelstein RA, Coen JJ, Babayan
RK and Krane RJ: Radical prostatectomy for adenocarcinoma of the
prostate: The influence of preoperative and pathologic findings on
biochemical disease-free outcome. Urology. 43:828–833. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Namiki K and Rosser CJ: Neoadjuvant
therapy and prostate cancer: What a urologist should know. Curr
Opin Urol. 17:188–193. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Herman JR, Adler HL, Aguilar-Cordova E,
Rojas-Martinez A, Woo S, Timme TL, Wheeler TM, Thompson TC and
Scardino PT: In situ gene therapy for adenocarcinoma of the
prostate: A phase I clinical trial. Hum Gene Ther. 10:1239–1249.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Shalev M, Kadmon D, Teh BS, Butler EB,
Aguilar-Cordova E, Thompson TC, Herman JR, Adler HL, Scardino PT
and Miles BJ: Suicide gene therapy toxicity after multiple and
repeat injections in patients with localized prostate cancer. J
Urol. 163:1747–1750. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Miles BJ, Shalev M, Aguilar-Cordova E, et
al: Prostate-specific antigen response and systemic T cell
activation after in situ gene therapy in prostate cancer patients
failing radiotherapy. Hum Gene Ther. 12:1955–1967. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Thompson TC: In situ gene therapy for
prostate cancer. Oncol Res. 11:1–8. 1999.PubMed/NCBI
|
|
10
|
Freeman SM, Abboud CN, Whartenby KA,
Packman CH, Koeplin DS, Moolten FL and Abraham GN: The ‘bystander
effect’: Tumor regression when a fraction of the tumor mass is
genetically modified. Cancer Res. 53:5274–5283. 1993.PubMed/NCBI
|
|
11
|
Barba D, Hardin J, Sadelain M and Gage FH:
Development of anti-tumor immunity following thymidine
kinase-mediated killing of experimental brain tumors. Proc Natl
Acad Sci USA. 91:4348–4352. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Gagandeep S, Brew R, Green B, Christmas
SE, Klatzmann D, Poston GJ and Kinsella AR: Prodrug-activated gene
therapy: Involvement of an immunological component in the
‘bystander effect’. Cancer Gene Ther. 3:83–88. 1996.PubMed/NCBI
|
|
13
|
Ayala G, Wheeler TM, Shalev M, Thompson
TC, Miles B, Aguilar-Cordova E, Chakraborty S and Kadmon D:
Cytopathic effect of in situ gene therapy in prostate cancer. Hum
Pathol. 31:866–870. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Satoh T, Teh BS, Timme TL, et al: Enhanced
systemic T-cell activation after in situ gene therapy with
radiotherapy in prostate cancer patients. Int J Radiat Oncol Biol
Phys. 59:562–571. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hall SJ, Mutchnik SE, Chen SH, Woo SL and
Thompson TC: Adenovirus-mediated herpes simplex virus thymidine
kinase gene and ganciclovir therapy leads to systemic activity
against spontaneous and induced metastasis in an orthotopic mouse
model of prostate cancer. Int J Cancer. 70:183–187. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Hall SJ, Sanford MA, Atkinson G and Chen
SH: Induction of potent antitumor natural killer cell activity by
herpes simplex virus-thymidine kinase and ganciclovir therapy in an
orthotopic mouse model of prostate cancer. Cancer Res.
58:3221–3225. 1998.PubMed/NCBI
|
|
17
|
Hassan W, Sanford MA, Woo SL, Chen SH and
Hall SJ: Prospects for herpes-simplex-virus thymidine-kinase and
cytokine gene transduction as immunomodulatory gene therapy for
prostate cancer. World J Urol. 18:130–135. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Loimas S, Toppinen MR, Visakorpi T, Jänne
J and Wahlfors J: Human prostate carcinoma cells as targets for
herpes simplex virus thymidine kinase-mediated suicide gene
therapy. Cancer Gene Ther. 8:137–144. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Vile RG, Castleden S, Marshall J,
Camplejohn R, Upton C and Chong H: Generation of an anti-tumour
immune response in a non-immunogenic tumour: HSVtk killing in vivo
stimulates a mononuclear cell infiltrate and a Th1-like profile of
intratumoural cytokine expression. Int J Cancer. 71:267–274. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kianmanesh AR, Perrin H, Panis Y, Fabre M,
Nagy HJ, Houssin D and Klatzmann D: A ‘distant’ bystander effect of
suicide gene therapy: Regression of nontransduced tumors together
with a distant transduced tumor. Hum Gene Ther. 8:1807–1814. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Whartenby KA, Abboud CN, Marrogi AJ,
Ramesh R and Freeman SM: The biology of cancer gene therapy. Lab
Invest. 72:131–145. 1995.PubMed/NCBI
|
|
22
|
Satoh T, Kubo M, Tabata K, et al: Systemic
T-cell activation following neoadjuvant in situ gene therapy in
high-risk prostate cancer patients. J Urol. 187:e3232012.
View Article : Google Scholar
|
|
23
|
Ayala G, Satoh T, Li R, Shalev M, Gdor Y,
Aguilarcordova E, Frolov A, Wheeler T, Miles B and Rauen K:
Biological response determinants in HSV-tk + ganciclovir gene
therapy for prostate cancer. Mol Ther. 13:716–728. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
van der Linden RR, Haagmans BL,
Mongiat-Artus P, van Doornum GJ, Kraaij R, Kadmon D,
Aguilar-Cordova E, Osterhaus AD, van der Kwast TH and Bangma CH:
Virus specific immune responses after human neoadjuvant
adenovirus-mediated suicide gene therapy for prostate cancer. Eur
Urol. 48:153–161. 2005. View Article : Google Scholar : PubMed/NCBI
|