Introduction
Malignant adnexal masses are rare during pregnancy.
The imaging characteristics of such masses have been even less
frequently reported. The sonographic appearance of benign adnexal
masses may be misdiagnosed as malignancy and further research is
required to determine whether sonographic findings may distinguish
these lesions from malignant tumors during pregnancy (1–3). The aim
of this study was to describe the preoperative sonographic
characteristics of 4 consecutive patients with lesions misdiagnosed
as malignant and histologically diagnosed as benign
postoperatively.
Patients and methods
Cases
For this retrospective study, we collected cases of
pregnancy complicated by adnexal masses treated at the Obstetrics
and Gynecology Hospital of Fudan University (Shanghai, China)
between January, 2010 and January, 2014. All the patients had
undergone imaging using a transabdominal 13-MHz probe and we
selected a total of 4 cases with benign pelvic masses initially
misdiagnosed as ovarian cancer. This study was approved by the
Obstetrics and Gynecology Hospital of Fudan University
Institutional Review Board (Shanghai, China).
Results
Case 1
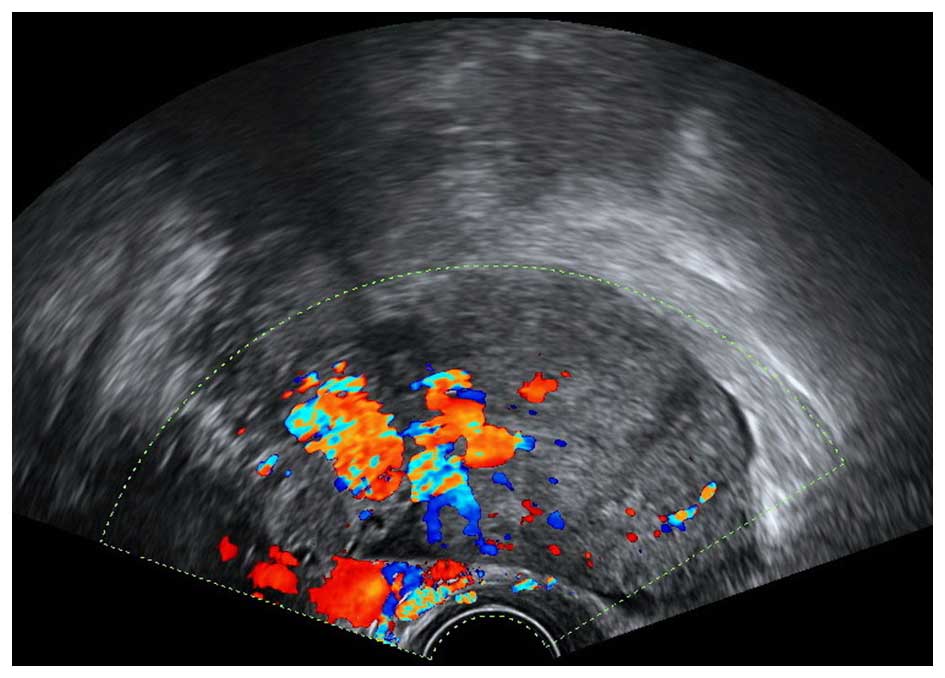
The patient was admitted at 23 weeks of gestation
for a heterogeneous adnexal mass, sized 8×7×6 cm, which was
discovered incidentally. Sonographically, there was a predominantly
solid lesion with a middle hypoechoic area on the left adnexa,
appearing to originate from the left ovary. Color Doppler
evaluation (MyLab 90 Systems; Esaote S.p.A., Genova, Italy)
demonstrated abundant arterial and venous flow (Fig. 1). We detected an accumulation of 1,000
ml of ascitic fluid. The fetus and the contralateral adnexa were
normal in appearance. The mass was diagnosed as malignant left
ovarian tumor on ultrasound. The carbohydrate antigen (CA) 125
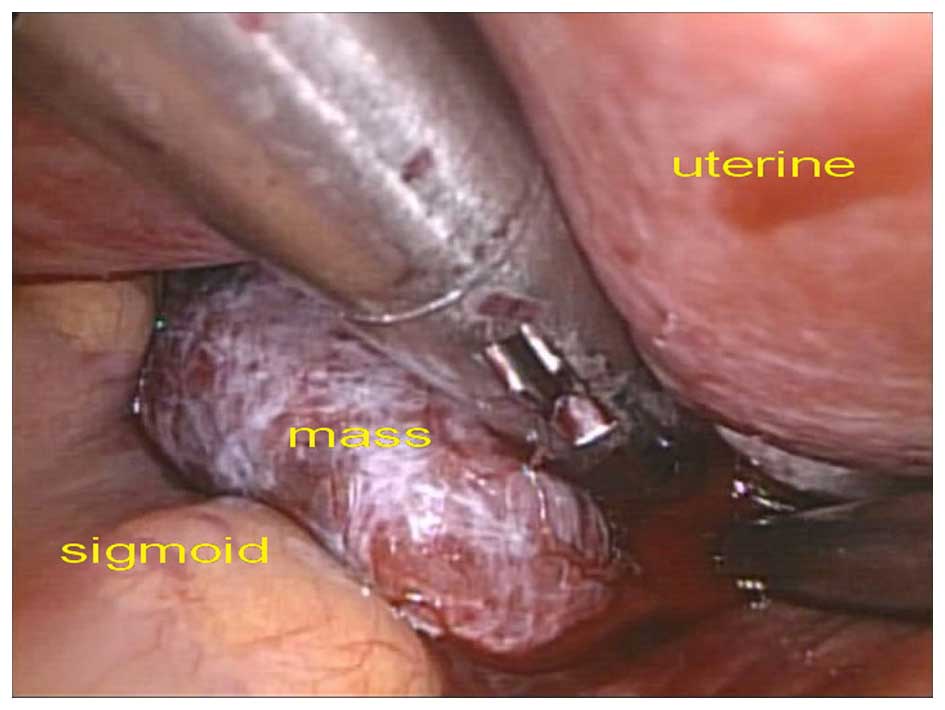
levels were increased to 2,443.1 U/ml (normal, <35 U/ml). During
laparoscopy a highly vascularized mass was identified at the
periphery of the left ovary. There was a 800-ml blood loss and the
patient received a transfusion intraoperatively (Fig. 2). The mass was diagnosed as luteoma of
pregnancy on frozen section analysis. However, on postoperative
pathological examination, the mass was definitively diagnosed as a
theca cell tumor with luteinization. The follow-up of the pregnancy
course was unremarkable and the patient delivered a 3,200-g infant
at 39 weeks.
Case 2
The patient was admitted at the 16th week of
gestation, with persistent mild lower abdominal pain. She had
undergone in vitro fertilization and embryo transfer and
laparoscopic right salpingostomy for ectopic pregnancy with a
uterine pregnancy at the 9th week. A transvaginal ultrasound
indicated the presence of an inhomogeneous, predominantly solid
lesion, sized 58×56×47 mm, on the left side of the uterus. Doppler
ultrasound revealed a blood vessel encircling the mass. The ovaries
were of normal morphology and size, with a normal double uterine
pregnancy. The ultrasound diagnosis was fallopian tube cancer. The
patient exhibited increased CA125 levels (256.1 U/ml). However, on
laparoscopy, we observed an obsolete ectopic pregnancy in the left
fallopian tube and salpingectomy was performed. The patient
underwent a caesarean section at the 34th week of gestation as a
result of pregnancy-induced hypertension syndrome and the birth
weight of the infants was 2,200 and 2,450 g.
Case 3
The patient was admitted during the 20th week of
gestation, asymptomatic. Ultrasonography revealed a left-sided
18×16×15-cm adnexal mass, with a heterogeneous echo. The patient
had increased CA125 (532.75 U/ml) and CA199 (13.87 U/ml) levels.
The fetus and the contralateral adnexa appeared to be normal. The
mass was diagnosed as ovarian cancer. A left adnexectomy was
performed by laparotomy. Frozen section examination revealed a
mature teratoma with abundant nervous tissue, which was
pathologically confirmed postoperatively. The patient delivered by
cesarean laparotomy at 40 weeks and the infant's weight was 3,250
g.
Case 4
The patient was admitted during the 22th week of
gestation, asymptomatic. A 15-cm adnexal mixed-echo mass was
detected attached to the uterine wall. On Doppler examination, the
mass exhibited abundant blood flow and a tangled bloodstream, and
was diagnosed as right ovarian cancer. The patient had elevated
CA125 levels (872.7 U/ml). However, the patient refused surgery;
she underwent caesarean section at the 39th week and the birth
weight of the infant was 3,050 g. Intraoperatively, a 16-cm mass
arising from the uterine isthmus was identified, surrounded by
dilated blood vessels; the mass was not excised. Both ovaries and
fallopian tubes were of normal appearance. After 1 year, the
patient was readmitted for the uterine mass. Laparoscopy was
performed and a uterine myoma with degeneration was pathologically
confirmed.
Discussion
Although adnexal masses complicating pregnancy are
significantly less common compared with non-pregnant patients,
benign masses, including benign teratoma (7–37%), serous
cystadenoma (5–28%) and mucinous cystadenoma (3–24%), endometrioma
(0.8–27%), paraovarian cysts (<5%) and leiomyoma (1–2.5%), may
be encountered. Ovarian cancers (including those of low malignant
potential) in pregnancy are very rare, accounting for ~1–8% in all
adnexal masses (4).
Adnexal masses identified as malignant tumors during
pregnancy are a serious finding, due to the increased risk of
obstetric complications and the difficulty in surgical
management.
Ultrasound evaluation is the usual method applied
for the diagnosis of adnexal masses (5). During pregnancy, the ultimate purpose of
an ultrasound examination is to assist the gynecologist in
determining whether those adnexal masses require observation or
surgical intervention.
Characteristics such as septation, solid components,
nodules, papillary components, or an average diameter of >5 cm
have been identified as predictors of malignancy. The 4 benign
cases in our study were consistent with the abovementioned
findings. It appears to be difficult to distinguish between benign
and malignant adnexal lesions during pregnancy. These difficulties
are due to the inhomogeneous echo and, particularly, the massively
increased pelvic blood flow. DePriest and DeSimone reported that
investigations with regard to blood flow on Doppler demonstrated
that Doppler examination did not further facilitate diagnosis
compared with gray-scale sonography alone, with a similar
false-positive rate of 49% for the prediction of malignancy
(6). Groszmann et al did not
identify any morphological or vascular flow characteristics that
were helpful in sonographically distinguishing benign decidualized
endometrioma from malignancy (7).
Undeniably, as a commonly used epithelial ovarian
cancer tumor marker, CA125, may be elevated during the first
trimester of pregnancy and postpartum in normal pregnancy (1). However, massively elevated CA125 levels
(1,000–10,000 U/ml) during the second trimester may mislead the
gynecologist to suspect malignancy (8). In our study, the CA125 levels were
increased above normal levels in all 4 cases.
A limitation of our study was the small sample size.
Although the data were from a single center, the results revealed
that abundant blood flow and heterogeneous echo of the adnexal
masses during pregnancy may not represent malignancy.
Acknowledgements
The present study was supported by the Science and
Technology Commission of Shanghai Municipality (grant no.
134119a8200).
References
|
1
|
Naqvi M and Kaimal A: Adnexal masses in
pregnancy. Clin Obstet Gynecol. 58:93–101. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Marret H, Lhommé C, Lecuru F, Canis M,
Lévèque J, Golfier F and Morice P: Guidelines for the management of
ovarian cancer during pregnancy. Eur J Obstet Gynecol Reprod Biol.
149:18–21. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Aggarwal P and Kehoe S: Ovarian tumours in
pregnancy: A literature review. Eur J Obstet Gynecol Reprod Biol.
155:119–124. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Hoover K and Jenkins TR: Evaluation and
management of adnexal mass in pregnancy. Am J Obstet Gynecol.
205:97–102. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Yacobozzi M, Nguyen D and Rakita D:
Adnexal masses in pregnancy. Semin Ultrasound CT MR. 33:55–64.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
DePriest PD and DeSimone CP: Ultrasound
screening for the early detection of ovarian cancer. J Clin Oncol.
21(Suppl): 194s–199s. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Groszmann Y, Howitt BE, Bromley B,
Feltmate CM and Benacerraf BR: Decidualized endometrioma
masquerading as ovarian cancer in pregnancy. J Ultrasound Med.
33:1909–1915. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Goh W, Bohrer J and Zalud I: Management of
the adnexal mass in pregnancy. Curr Opin Obstet Gynecol. 26:49–53.
2014. View Article : Google Scholar : PubMed/NCBI
|