Introduction
Prostate cancer is the most common cancer among men
in Western countries. The 5-year survival rate of localized and
regional prostate cancer is ~100%, whereas that of metastatic
prostate cancer is only 27–28% (1).
As serum prostate-specific antigen (PSA) screening has become
widespread, the proportion of cases presenting with lymph node
involvement or advanced disease has decreased considerably
(2). However, ~20% of patients
present with metastatic disease. Metastatic prostate cancer usually
involves the pelvic lymph nodes, bones, and lungs (2), with bone pain being a common symptom in
SUCH patients. However, there are other rare manifestations of
metastatic prostate cancer. HereIN, we present a rare case of
prostate cancer metastasis initially presenting as chylothorax.
Case report
A 64-year-old Asian man visited the emergency room
with dyspnea. The patient's medical history was unremarkable, with
the exception of being a current smoker with a 20 pack-year
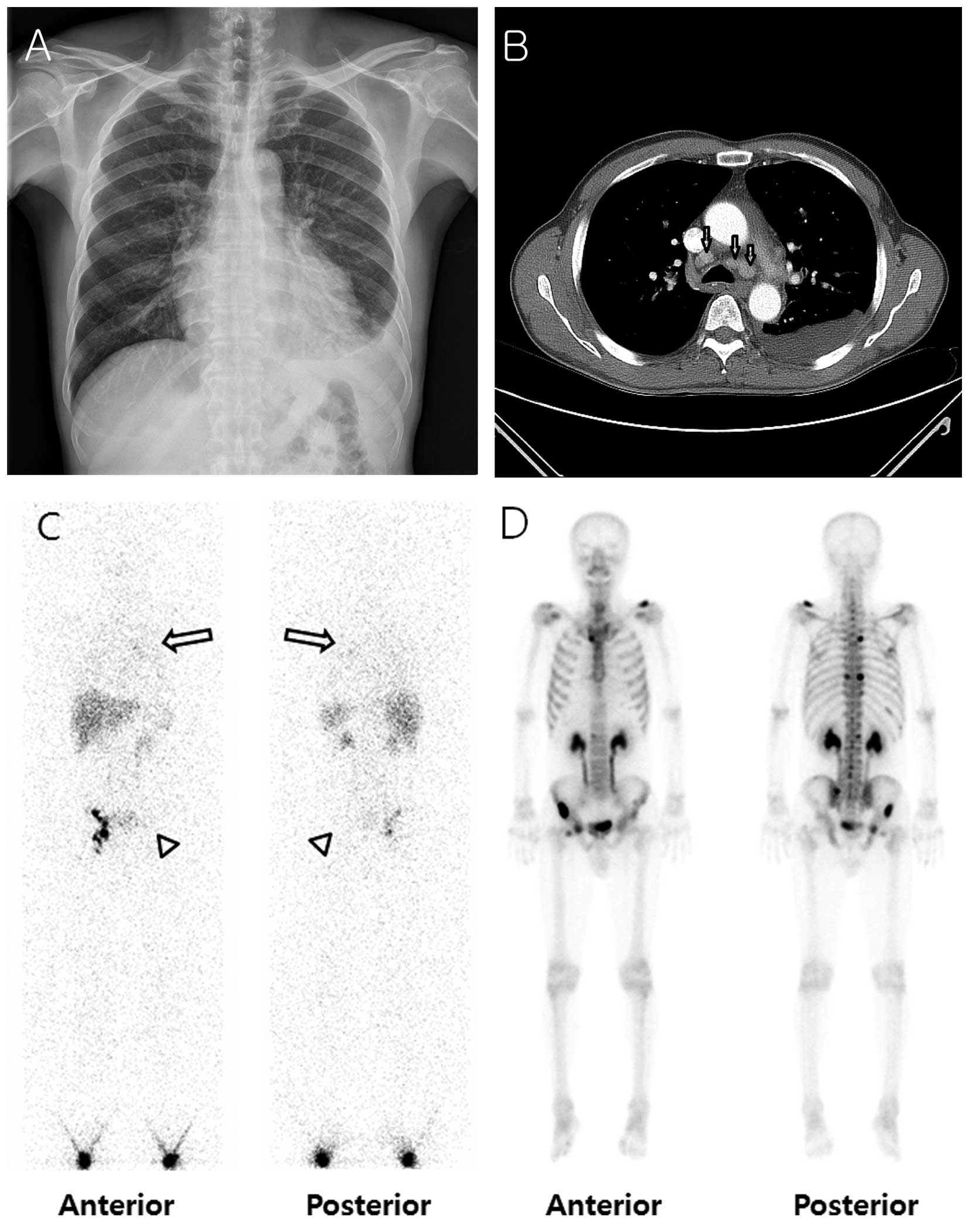
history. Radiographic images, including computed tomography scan of
the chest, revealed a left pleural effusion, pericardial effusion,
and enlarged lymph nodes in the left supraclavicular/posterior
neck/axillary area, right upper paratracheal area, subcarinal area,
and bilateral lower paratracheal areas (Fig. 1A and B). Thoracentesis was performed
and fluid analysis revealed a chylothorax, in which the
triglyceride level was 244 mg/dl (normal range, <50 mg/dl).
Whole-body lymphoscintigraphy revealed faint tracer accumulation
activity in the medial portion of the left hemithorax, where the
pleural effusion was present (Fig.
1C). Considering that the patient had never received thoracic
surgery or experienced trauma, malignancy was suspected. Pleural
fluid cytology revealed numerous mononuclear leukocytes and some
reactive mesothelial cells, but did not show any evidence of
malignancy. The serum PSA level was elevated to 194.6 ng/ml (normal
range, 0–3 ng/ml).
A prostate biopsy revealed adenocarcinoma of the
prostate gland. A bone scan was performed for staging, which
revealed multiple bone metastases (Fig.
1D). Therefore, the chylothorax was considered to have resulted
from thoracic duct obstruction by enlarged lymph node metastasis
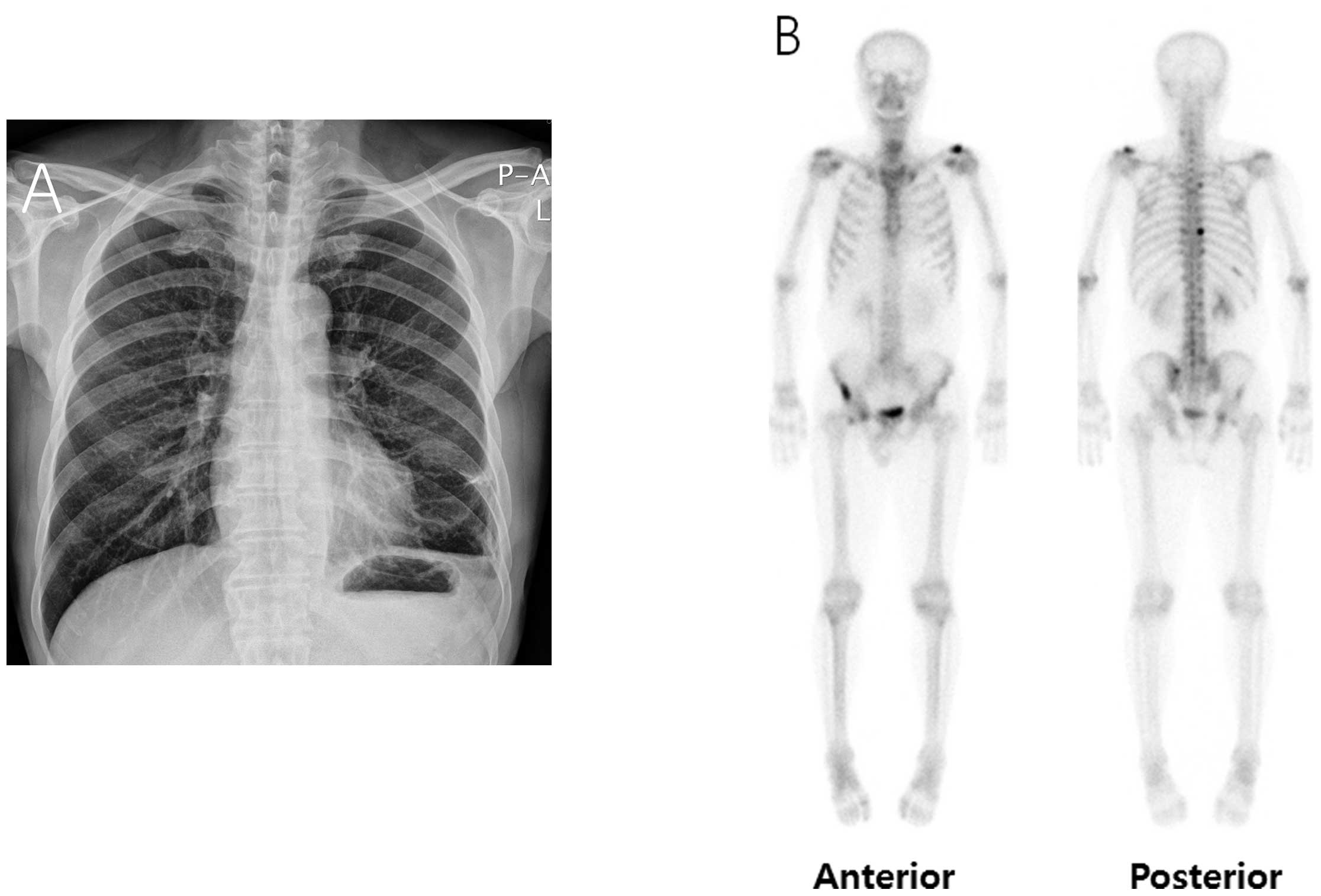
from prostate cancer. Androgen deprivation therapy (ADT) was
initiated, with simultaneous administration of goserelin and
anti-androgen. After 3 months, the amount of pleural effusion had
decreased (Fig. 2A) and the serum PSA
level decreased from 194.6 to 31.68 ng/ml following ADT. A bone
scan performed 8 months after the initiation of ADT revealed that
the intensities of multiple bone uptakes had decreased
significantly when compared to the initial scan (Fig. 2B). The patient is undergoing regular
follow-up at our outpatient clinic for 1 year after diagnosis and
has not reported experiencing any further discomfort.
Discussion
In Korea, among males aged ≥65 years, prostate
cancer is the fourth most common type of cancer and its incidence
is increasing with advancing age. The crude mortality of prostate
cancer is 2.8/10,000 and the 5-year relative survival rate by year
of diagnosis from 2007–2011 was 92%, indicating that it is a highly
treatable cancer (3).
There is some controversy regarding the efficacy of
serum PSA screening. Randomized trials have demonstrated that serum
PSA screening reduces metastatic prostate cancer incidence and
disease-related mortality (4).
However, other STUDIEs have reported that, due to the unnecessary
biopsies following false-positive serum PSA results, cancer
risk-adapted serum PSA screening is required (5). In the United States, the proportion of
patients presenting with metastatic disease decreased from 17% in
1988–1990 to 4% in 1996-1998, while the proportion presenting with
stage T1 tumors conversely increased from 14 to 51% (6).
As stated above, metastatic prostate cancer usually
involves the pelvic lymph nodes, bones and lungs (2) and it may present as a skin lesion,
endobronchial mass, ascites, or renal mass. Table I summarizes some of the rare
manifestations of prostate cancer (7–19).
Although our patient was not the first case of metastatic prostate
cancer presenting as chylothorax, initial presentation of prostate
cancer as chylothorax is quite rare (18,19).
 | Table I.Review of cases of rare manifestations
from metastatic prostate cancer. |
Table I.
Review of cases of rare manifestations
from metastatic prostate cancer.
| Authors | Presentation | Onset of
manifestation | Age, years | Treatment | Outcome | REFS. |
|---|
| Mak et al | Skin | Late | 73 | Radiotherapy | Pain relief | (7) |
| Garai et
al | Endobronchial
mass | Initial | 84 | Not stated | Not stated | (8) |
| Ani et al | Ascites | Initial | 57 | ADT | PR | (9) |
| Sakata et
al | Kidney | Late | 67 | Nephrectomy | PR | (10) |
| Ibinaiye et
al | Kidney | Initial | 55 | ADT | PR | (11) |
| Grenader et
al | Brain | Initial | 70 | Radiotherapy +
ADT | PR | (12) |
| Rahmathulla et
al | Brain | Initial | 70 | Surgical
resection | PR | (13) |
| Patel et
al | Pituitary gland | Late | 66 | Radiotherapy | PR | (14) |
| Kaswala et
al | Small bowel | Late | 42 | Chemotherapy | Not stated | (15) |
| Kusaka et
al | Testis | Late | 56 | Radiotherapy +
ADT | PR | (16) |
| Mortensen et
al | Testis | Late | 89 | Bilateral
orchiectomy | Not stated | (17) |
| Tabba et
al | Chylothorax | Late | 69 | Chemotherapy | PR | (18) |
| Quinonez et
al | Chylothorax | Late | 78 | Bilateral orchiectomy
+ chemotherapy | PR | (19) |
| PRESENT case | Chylothorax | Initial | 64 | ADT | PR |
|
Lymphoscintigraphy, which functionally assesses the
lymphatic transport and regional lymph nodes, is an easy,
non-invasive method for detecting abnormalities in the lymphatic
system, including leakages such as chylothorax, chyloperitoneum and
chyluria. Positive findings include tracer activity at the site
where lymphatic fluid is accumulated, as seen in our case (20,21). ADT
is the mainstay of treatment for patients with metastatic prostate
cancer. Luteinizing hormone-releasing hormone agonists have become
the standard of care in hormonal therapy, as these agents have the
potential of reversibility and enable the use of intermittent
androgen deprivation (22). Moreover,
with ADT, patients avoid the physical and psychological discomfort
associated with orchiectomy (23).
Intermittent androgen deprivation alternates androgen blockade with
treatment cessation, in order to allow hormonal recovery between
the treatment cycles, thus potentially improving the tolerability
and quality of life. Hence, for older patients, intermittent
androgen deprivation may generally be applied (24).
In summary, chylothorax is an uncommon condition. If
there is no history of chest/neck injury or surgery, exclusion of
malignancy is crucial. Despite its low probability, prostate cancer
with mediastinal lymph node metastasis may result in chylothorax.
Therefore, when we evaluate the causes of non-traumatic
chylothorax, prostate cancer should be considered, and serum PSA
screening is recommended to exclude this possibility.
References
|
1
|
Siegel R, Ma J, Zou Z and Jemal A: Cancer
statistics, 2014. CA Cancer J Clin. 64:9–29. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Elkin M and Mueller HP: Metastases from
cancer of the prostate; Autopsy and roentgenological findings.
Cancer. 7:1246–1248. 1954. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Jung KW, Won YJ, Kong HJ, Oh CM, Lee DH
and Lee JS: Cancer statistics in Korea: Incidence, mortality,
survival and prevalence in 2011. Cancer Res Treat. 46:109–123.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Schröder FH, Hugosson J, Roobol MJ,
Tammela TL, Ciatto S, Nelen V, Kwiatkowski M, Lujan M, Lilja H,
Zappa M, et al: Screening and prostate-cancer mortality in a
randomized European study. N Engl J Med. 360:1320–1328. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Loeb S: Guideline of guidelines: Prostate
cancer screening. BJU Int. 114:323–325. 2014.PubMed/NCBI
|
|
6
|
Crawford ED: Epidemiology of prostate
cancer. Urology. 62(6 Suppl 1): 3–12. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Mak G, Chin M, Nahar N and De Souza P:
Cutaneous metastasis of prostate carcinoma treated with
radiotherapy: A case presentation. BMC Res Notes. 7:5052014.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Garai S and Pandey U: Prostate cancer
presenting as an endobronchial mass: A case report with literature
review. Int J Surg Pathol. 18:554–556. 2010.PubMed/NCBI
|
|
9
|
Ani I, Costaldi M and Abouassaly R:
Metastatic prostate cancer with malignant ascites: A case report
and literature review. Can Urol Assoc J. 7:E248–E250. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Sakata R, Iwasaki A, Kobayashi M, Osaka K,
Fujikawa A, Tsuchiya F and Ishizuka E: Renal metastasis from
prostatic adenocarcinoma: A case report. ACTA UROLOGICA JAPONICA.
57:683–687. 2011.(In Japanese). PubMed/NCBI
|
|
11
|
Ibinaiye PO, Mbibu H, Shehu SM, David SO
and Samaila MO: Renal metastasis from prostate adenocarcinoma: A
potential diagnostic pitfall. Ann Afr Med. 11:230–233. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Grenader T, Shavit L, Lossos A, Pizov G
and Wygoda M: Brain metastases: A rare initial presentation of
prostate cancer. Int Urol Nephrol. 39:537–539. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Rahmathulla G, Prayson RA and Weil RJ:
Rare presentation of metastatic prostate adenocarcinoma as a
meningioma mimic. J Neurol Surg Rep. 75:e81–e83. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Patel N, Teh BS, Powell S, Lu HH, Amato R
and Butler EB: Rare case of metastatic prostate adenocarcinoma to
the pituitary. Urology. 62:3522003. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kaswala DH, Patel N, Jadallah S and Wang
W: Metastatic prostate cancer to the duodenum: A rare case. J
Family Med Prim Care. 3:166–168. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kusaka A, Koie T, Yamamoto H, Hamano I and
Yoneyama T, Hashimoto Y, Ohyama C, Tobisawa Y and Yoneyama T:
Testicular metastasis of prostate cancer: A case report. Case Rep
Oncol. 7:643–647. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Mortensen MA, Engvad B, Geertsen L,
Svolgaard N and Lund L: Metastasis in testis from prostate cancer.
Ugeskr Laeger. 176:V101306322014.(In Danish). PubMed/NCBI
|
|
18
|
Tabba M and Inaty H: A rare case of
chylothorax attributed to metastatic prostate carcinoma. J Pulmon
Resp Med. S142013.
|
|
19
|
Quinonez A, Halabe J, Avelar F, Lifshitz
A, Moreno J and Berumen AH: Chylothorax due to metastatic prostatic
carcinoma. Br J Urol. 63:325–327. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Pui MH and Yueh TC: Lymphoscintigraphy in
chyluria, chyloperitoneum and chylothorax. J Nucl Med.
39:1292–1296. 1998.PubMed/NCBI
|
|
21
|
Prevot N, Tiffet O, Avet J Jr, Quak E,
Decousus M and Dubois F: Lymphoscintigraphy and SPECT/CT using
99mTc filtered sulphur colloid in chylothorax. Eur J Nucl Med Mol
Imaging. 38:17462011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
McLeod DG: Hormonal therapy: Historical
perspective to future directions. Urology. 61(2 Suppl 1): 3–7.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Seidenfeld J, Samson DJ, Hasselblad V,
Aronson N, Albertsen PC, Bennett CL and Wilt TJ: Single-therapy
androgen suppression in men with advanced prostate cancer: A
systematic review and meta-analysis. Ann Intern Med. 132:566–577.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Abrahamsson PA: Potential benefits of
intermittent androgen suppression therapy in the treatment of
prostate cancer: A systematic review of the literature. Eur Urol.
57:49–59. 2010. View Article : Google Scholar : PubMed/NCBI
|