Introduction
Esophageal cancer (EC) has a high incidence
worldwide (1) and carries a poor
prognosis. EC develops mainly in individuals aged >50 years, and
the number of older patients with EC in Japan is increasing
concomitantly with the aging of the population. Older patients
frequently have comorbidities, cognitive decline, polypharmacy and
social issues (2). The currently
available treatment modalities for EC include endoscopic submucosal
dissection (ESD), esophagectomy, radiotherapy, chemotherapy,
chemoradiotherapy (CRT) and best supportive care (BSC) (3). ESD was developed for superficial EC
restricted to the mucosal layer (T1a) (3). Despite the increasing number of older
patients with EC, the majority of clinical trials have involved
only, or mostly, younger patients (4). Although some studies have focused on
older patients (5), these involved a
relatively limited number of subjects and a single arm (6,7). In
addition, older patients have high rates of morbidity and mortality
(8,9). Therefore, an optimal treatment modality
for older patients with EC has yet to be established.
Older patients have been defined as those aged
>70, 75 or 80 years, depending on the study in question
(6–11). A multicenter questionnaire survey
indicated that most institutions consider EC patients aged >75
or 80 years as older patients (12).
In the present study, older patients were defined as those who were
at least 75 years old.
Patients and methods
Patients
Data on EC patients diagnosed at the Niigata
University Medical and Dental Hospital (Niigata, Japan) between
January 2007 and December 2017 were retrospectively collected using
a hospital-based cancer registry and electronic medical records.
The study protocol was approved by the Ethics Review Committee of
the School of Medicine of Niigata University (Niigata, Japan;
approval no. 2485). All procedures performed in studies involving
human participants were in accordance with the ethical standards of
the Institutional and National Research Committee and the 1964
Declaration of Helsinki and its later amendments, or comparable
ethical standards. Patient informed consent was not applicable, as
this study was retrospective and data were collected only from
medical records. All patients were informed of the opportunity to
opt out of this study through the internet home page of Niigata
University School of Medicine. The collected data included age at
diagnosis, sex, tumor histology, cancer stage (TNM), treatment
modality and prognosis. The Union for International Cancer Control
guidelines, version 7 (13), were
used for TNM staging. The patient population was divided into
younger and older patients, with 75 years at the time of EC
diagnosis as the cut-off.
Statistical analysis
The Chi-squared or Fisher's exact tests were used to
evaluate the significance of the differences between the two
groups. Disease-specific survival duration was defined as the
period from the date of diagnosis to that of death due to EC.
Patients who died from causes other than EC were censored at the
date of death. Surviving patients were censored on the date of
their last visit to the hospital. Survival curves were drawn using
the Kaplan-Meier method and were compared by log-rank tests.
P<0.05 was considered to indicate a statistically significant
difference. Statistical analyses were performed using IBM version
22.0 (IBM Corp.).
Results
Patient characteristics
A total of 990 patients with EC who visited Niigata
University Medical and Dental Hospital between January 2007 and
December 2017 were identified. The patient characteristics are
summarized in Table I. Of these
patients, 359 (36.3%) were aged 75 years or older, and 631 patients
(63.7%) were aged <75 years. The median age was 71 years in the
entire population, 66 years in the younger group and 79 years in
the older group. The majority of the EC patients in both groups had
squamous cell carcinoma (90.1%) and early-stage EC (stage 0 or I).
The frequency of adenocarcinoma was significantly higher
(P<0.01), and the rates of different stages were significantly
different (P<0.01) in the older compared with the younger
group.
 | Table I.Characteristics of patients with
esophageal cancer. |
Table I.
Characteristics of patients with
esophageal cancer.
| Characteristics | Total (n=990) | Age ≤74 years
(n=631) | Age ≥75 years
(n=359) | P-value |
|---|
| Median age | 71 (33–91) | 66 (33–74) | 79 (75–91) | <0.01 |
| Sex |
|
|
| 0.8 |
| Male | 853 | 545 | 308 |
|
|
Female | 137 | 86 | 51 |
|
| Histology |
|
|
| <0.01 |
| Squamous
cell carcinoma | 897 | 588 | 309 |
|
|
Adenocarcinoma | 69 | 32 | 37 |
|
|
Others | 24 | 11 | 13 |
|
| Stage |
|
|
| <0.01 |
| 0 | 285 | 205 | 80 |
|
| I | 441 | 270 | 171 |
|
| II | 50 | 33 | 17 |
|
| III | 113 | 84 | 29 |
|
| IV | 64 | 39 | 25 |
|
|
Unknown | 37 | 0 | 37 |
|
Treatment modality
Treatment modalities were classified according to
the main treatment, as precise classification of treatment
modalities would be overly complicated. The majority of the
patients underwent ESD (n=629, 63.5%) followed by surgery (n=144,
14.5%) and CRT (n=108, 10.9%) (Table
II). Older patients were more likely to undergo radiotherapy
alone (n=24, 6.7%) or BSC (n=48, 22%) compared with younger
patients (P<0.01). The complete multidisciplinary treatment
modalities in stage I and II/III cases are presented in Table III. Among younger patients with
stage I EC treated by ESD (n=207), 38 (18.4%) also received
chemotherapy/radiotherapy, as advanced-stage EC was detected by
histological analysis of ESD specimens. By contrast, only 8 (6.5%)
of the older patients with stage I EC (n=124) underwent
chemotherapy/radiotherapy after ESD. A total of 38 (14.1%) younger
patients and 14 (8.2%) older patients underwent surgery
with/without additional treatment for stage I disease. Of the
younger (n=65) and older (n=21) patients with stage II/III EC who
underwent surgery, 46 (71.0%) and 10 (47.6%), respectively,
received chemotherapy or/and radiotherapy before or after surgery.
Among 10 older patients treated with chemotherapy after surgery, 2
succumbed to treatment-related adverse effects of severe bone
marrow suppression.
| Table II.Main treatment modality for each stage
of esophageal cancer. |
Table II.
Main treatment modality for each stage
of esophageal cancer.
|
|
| Patients |
|
|---|
|
|
|
|
|
|---|
| Stage | Modality | Total (n=990) | Age ≤74 years
(n=631) | Age ≥75 years
(n=359) | P-value |
|---|
| All |
| N | % | N | % | N | % | <0.01 |
|
| ESD | 629 | 63.5 | 411 | 65.1 | 218 | 60.7 |
|
|
| Surgerya | 144 | 14.5 | 103 | 16.3 | 41 | 11.4 |
|
|
| CRT | 108 | 10.9 | 81 | 12.8 | 27 | 7.5 |
|
|
| RT | 36 | 3.6 | 12 | 1.9 | 24 | 6.7 |
|
|
| Chemotherapy | 13 | 1.3 | 12 | 1.9 | 1 | 0.3 |
|
|
| BSC | 60 | 6.1 | 12 | 1.9 | 48 | 22 |
|
| 0 |
|
|
|
|
|
|
| <0.01 |
|
| ESD | 274 | 96.5 | 202 | 98.5 | 72 | 90 |
|
|
|
Surgerya | 1 | 0.4 | 0 | 0 | 1 | 1.3 |
|
|
| CRT | 2 | 0.7 | 1 | 0.5 | 1 | 1.3 |
|
|
| BSC | 8 | 2.8 | 2 | 1 | 6 | 7.5 |
|
| I |
|
|
|
|
|
|
| <0.01 |
|
| ESD | 331 | 75.1 | 207 | 76.7 | 124 | 72.5 |
|
|
|
Surgerya | 52 | 11.8 | 38 | 14.1 | 14 | 8.2 |
|
|
| CRT | 31 | 7 | 20 | 7.4 | 11 | 6.4 |
|
|
| RT | 13 | 2.9 | 2 | 0.7 | 11 | 6.4 |
|
|
| Chemotherapy | 2 | 0.5 | 2 | 0.7 | 0 | 0 |
|
|
| BSC | 12 | 2.7 | 1 | 0.4 | 11 | 6.4 |
|
| II/III |
|
|
|
|
|
|
| <0.05 |
|
|
Surgerya | 86 | 52.8 | 65 | 55.5 | 21 | 45.7 |
|
|
| CRT | 50 | 30.7 | 40 | 34.2 | 10 | 21.7 |
|
|
| RT | 11 | 6.7 | 3 | 2.6 | 8 | 17.4 |
|
|
| Chemotherapy | 5 | 3.1 | 4 | 3.4 | 1 | 2.2 |
|
|
| BSC | 11 | 6.7 | 5 | 4.3 | 6 | 13 |
|
| IV |
|
|
|
|
|
|
| <0.01 |
|
|
Surgerya | 8 | 12.5 | 3 | 0.1 | 5 | 20 |
|
|
| CRT | 26 | 40.6 | 21 | 53.8 | 5 | 20 |
|
|
| RT | 11 | 17.2 | 6 | 1.5 | 5 | 20 |
|
|
| Chemotherapy | 5 | 7.8 | 5 | 1.3 | 0 | 0 |
|
|
| BSC | 14 | 21.9 | 4 | 0.1 | 10 | 40 |
|
| Unknown | ESD | 13 | 35.1 | 0 | 0 | 13 | 35.1 | <0.01 |
|
| BSC | 24 | 64.9 | 0 | 0 | 24 | 64.9 |
|
| Table III.Multidisciplinary treatment in stage
I and II/III. |
Table III.
Multidisciplinary treatment in stage
I and II/III.
|
|
| Patients |
|
|---|
|
|
|
|
|
|---|
| Stage | Treatment
modalities | Total | Aged ≤74 years | Aged ≥75 years | P-value |
|---|
| I |
|
|
|
| <0.05 |
|
| ESD alone | 281 | 169 | 116 |
|
|
| ESD + CRT | 41 | 33 | 6 |
|
|
| ESD + RT | 7 | 5 | 2 |
|
|
|
Surgerya
alone | 34 | 24 | 10 |
|
|
|
Surgerya
+ chemotherapy | 2 | 2 | 0 |
|
|
|
Surgerya
+ CRT | 15 | 12 | 3 |
|
|
|
Surgerya
+ RT | 1 | 0 | 1 |
|
|
| CRT | 31 | 20 | 11 |
|
|
| RT | 13 | 2 | 11 |
|
|
| Chemotherapy | 2 | 2 | 0 |
|
|
| BSC | 12 | 1 | 11 |
|
| II/III |
|
|
|
| <0.01 |
|
|
Surgerya
alone | 29 | 19 | 11 |
|
|
|
Surgerya
+ chemotherapy | 49 | 38 | 10 |
|
|
|
Surgerya
+ CRT | 8 | 8 | 0 |
|
|
| CRT | 50 | 40 | 10 |
|
|
| RT | 11 | 3 | 8 |
|
|
| Chemotherapy | 5 | 4 | 1 |
|
|
| BSC | 11 | 5 | 6 |
|
Although patients with stage IV EC in both groups
received various treatment modalities, 40% of the older patients
(n=25) underwent BSC (P<0.01). Patients with EC of unknown stage
were only found in the older group, and 24 (65%) of those opted for
BSC.
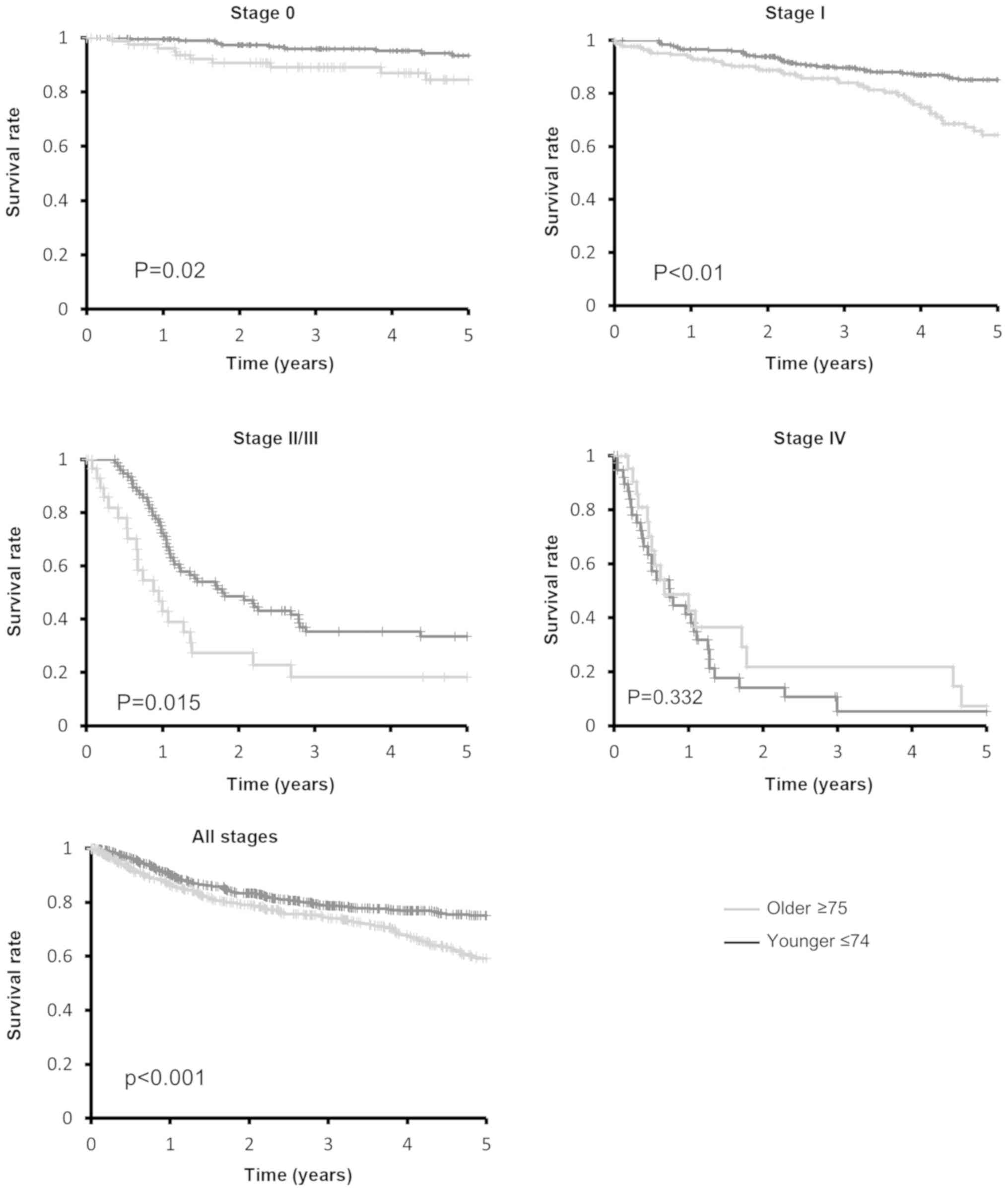
Disease-specific survival
Disease-specific survival rather than overall
survival was analyzed, due to the shorter life expectancy of the
older patients. The median follow-up time was 39.6 months (range,
1–120 months). The 5-year disease-specific survival rate was 59.1%
in the older group and 75.2% in the younger group at all stages
(Fig. 1). The disease-specific
survival duration of the older patients was significantly shorter
compared with that of the younger patients (P<0.001); moreover,
the disease-specific survival rate of the older patients decreased
markedly after 3.5 years. The disease-specific survival duration of
the older patients with stage 0, I or II/III EC was significantly
shorter compared with that of the younger patients with stage 0, I
or II/III EC (Fig. 1). The
disease-specific survival rate of the older patients with stage I
EC decreased considerably after 3.5 years, similar to the older
group as a whole. The survival curves differed markedly between
older and younger patients with stage I and II/III EC compared with
those with stage 0 EC. No difference in survival was observed
between older and younger patients with stage IV disease.
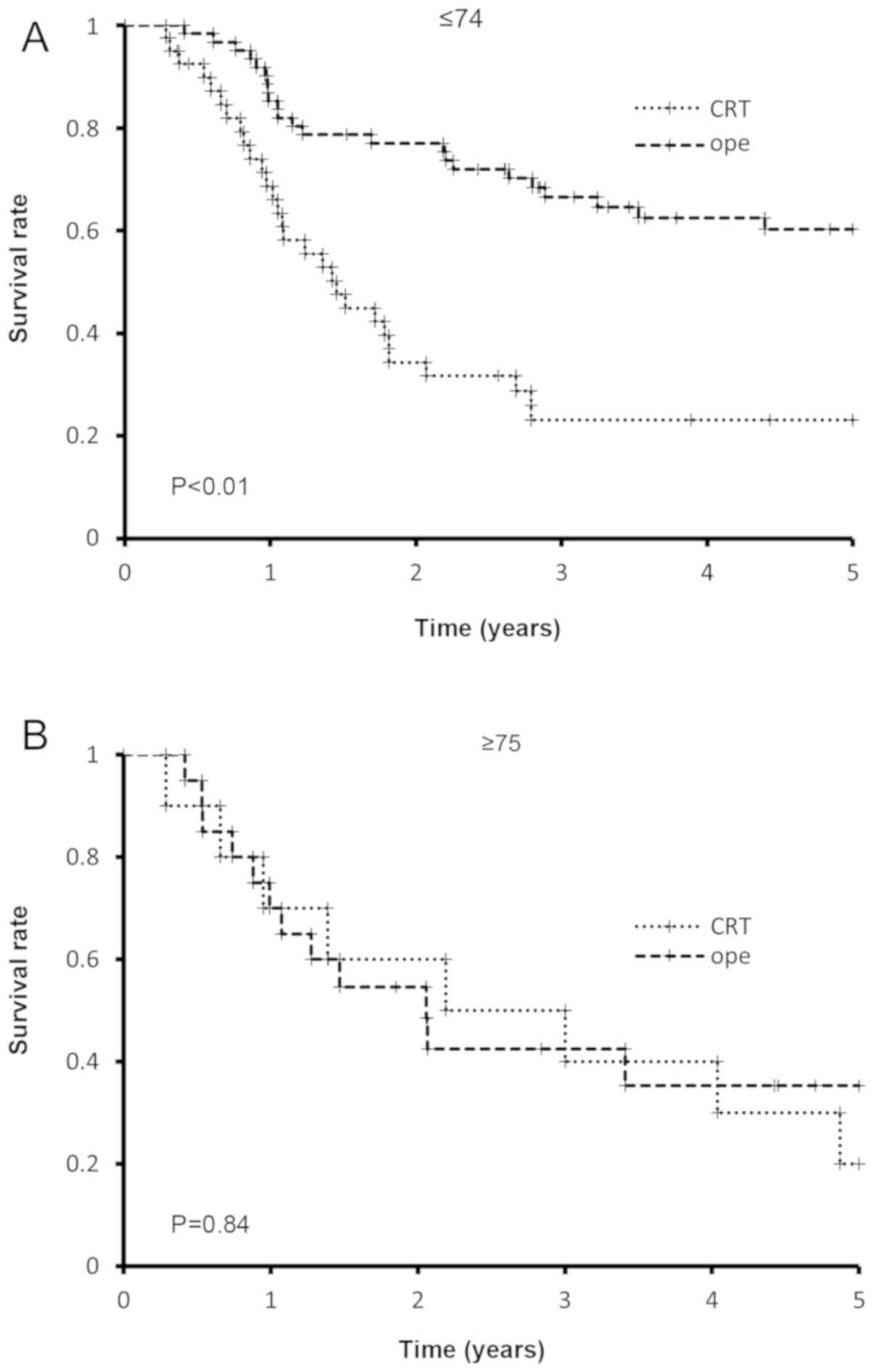
In older patients with stage II/III EC, the
disease-specific survival rate did not differ significantly between
patients who underwent surgery and those who received CRT; by
contrast, in the younger group, patients who received surgery
exhibited a significantly higher survival rate and duration
compared with those who were treated with CRT (Fig. 2). Older patients who underwent
surgery had a poorer prognosis compared with younger patients. A
total of 3 older patients died from adverse events due to
chemotherapy for stage II/IIII (2 cases) and IV (1 case) disease;
no treatment-related deaths were reported among younger
patients.
Discussion
In the present study, the clinicopathological
characteristics and treatment modalities and outcomes of 990
patients diagnosed with EC in our institution were reviewed.
Compared with younger patients with stage I EC, older patients with
stage I EC less frequently received additional treatment following
ESD (6.5% of the older vs. 18.4% of the younger patients). Compared
with younger patients with stage II/III EC, older patients with
stage II/II EC less frequently received perioperative
chemotherapy/radiotherapy (47.6 vs. 71.0%, respectively) and
definitive CRT (21.7 vs. 34.2%, respectively). Among the older
patients, 13% selected BCS compared with 2% of the younger
patients. Older patients had a significantly shorter
disease-specific survival duration compared with younger patients,
specifically for stage I and II/III disease.
Two large studies involving EC patients in the
United States and Taiwan (14,15)
reported 5-year survival rates of <20%. In addition, older
patients (≥70 years of age) were less likely to undergo surgery
or/and radiotherapy, and had a lower survival rate. In the US
study, 33.1 and 24.0% of the older and younger patients,
respectively, opted for BSC (14).
These survival rates are lower compared with those reported in the
present study, likely because the majority of our patients had
early-stage EC, were treated with ESD, and only 13% of the older
patients selected BSC.
ESD can completely remove superficial EC and EC
confined to the lamina propria mucosae, and is only indicated for
Tis and T1a (3,16). Patients diagnosed with T1a (m3) or
T1b, i.e., tumor invasion of the muscularis mucosae or submucosal
layer, respectively, require adjuvant therapy after ESD.
In a retrospective analysis in an adjuvant treatment
setting, both the 3-year relapse-free survival and overall survival
rates of patients with T1a (m3) or T1b EC after ESD were
significantly improved by adjuvant treatments (17). ESD followed by CRT for stage I
[m3(T1a) + T1b] is reportedly effective and safe, and improves the
prognosis compared with definitive CRT (18). In the present study, 6.5 and 18.4% of
the older and younger patients, respectively, with stage I EC
received adjuvant therapy. This low rate of adjuvant treatment may
partially explain the marked decrease in the survival rate after
3.5 years among older patients (Fig.
1). Of the 8 older patients who received adjuvant therapy after
ESD, 2 (25%) experienced grade 3 or 4 adverse effects of
neutropenia, but recovered. Therefore, adjuvant treatments after
ESD should be considered for older patients with T1a (m3) and T1b
EC. The low rate of surgical treatment (8.2 vs. 14.1%) may also
explain the worse prognosis of the older patients.
The prognosis of the older patients with stage
II/III EC did not differ significantly between those who underwent
surgery and those treated with CRT (Fig.
2). Older patients with EC who received surgery had a poorer
prognosis compared with younger patients (Fig. 2). Esophagectomy is a viable
alternative treatment option for patients aged >80 years, if the
surgical indication is strictly determined (19). In a prior study, the poor prognosis
of older patients (aged ≥75 years) who underwent surgery was
suggested to be due to the low rate of neoadjuvant chemotherapy
(6). Indeed, in the present study,
half of the older patients did not receive perioperative therapy,
and of the 21 older patients who received adjuvant therapy after
surgery, 2 succumbed to treatment-related adverse events. However,
the lack of precise data regarding treatment-related complications
and cause of death in older patients is a limitation of the present
study. CRT is reportedly effective without major toxicity in older
patients with locally advanced EC (20). Therefore, CRT may be considered as
the optimal treatment strategy for older patients with locally
advanced EC.
Although 54 and 20% of the younger and older
patients, respectively, with stage IV EC were treated with CRT, the
median survival duration was 10 months in both groups. CRT should
only be considered for patients with tumor-induced esophageal
stenosis. Novel and effective treatment modalities for treating
metastatic EC, such as immune-checkpoint drugs (21), are required.
In this context, it may be hypothesized that the
main explanation for the poorer prognosis in older patients is the
more conservative approach to treatment. In addition, the higher
frequency of multiple comorbidities among older patients may also
partially explain the poorer prognosis in older compared with that
in younger patients with EC. However, there was a lack of
information regarding comorbidities among EC patients in the
present study. Lack of disease-free survival data was also a
limitation of this study. A more precise analysis is required to
fully elucidate the exact causes of poorer prognosis among older
patients.
In conclusion, the poor prognosis of older patients
(aged ≥75 years) with stage I EC may be improved with
multidisciplinary treatment after ESD. Although the optimal
treatment for older EC patients with stage II/III disease may be
CRT at present, more efficient and safer treatment modalities, such
as immune checkpoint drugs, are urgently needed.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during the present
study are included in this published article.
Authors' contributions
YM contributed to the drafting of this manuscript.
YM, KK, TS, QZ, KS and MM contributed to the collection and
analysis of the data. MM and YS contributed to conception, design
and editing of the manuscript. All authors have read and approved
the final version of this manuscript for publication.
Ethics approval and consent to
participate
This study was approved by the Ethics Review
Committee of the School of Medicine of Niigata University (no.
2485).
Patient consent for publication
This was a retrospective observational study,
carried out by the opt-out method of School of Medicine of Niigata
University website.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
EC
|
esophageal cancer
|
|
ESD
|
endoscopic submucosal dissection
|
|
CRT
|
chemoradiotherapy
|
|
BSC
|
best supportive care
|
References
|
1
|
Global Burden of Disease Cancer
Collaboration, ; Fitzmaurice C, Dicker D, Pain A, Hamavid H,
Moradi-Lakeh M, MacIntyre MF, Allen C, Hansen G, Woodbrook R, et
al: The global burden of cancer 2013. JAMA Oncol. 1:505–527. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
van Deudekom FJ, Klop HG, Hartgrink HH,
Boonstra JJ, Lips IM, Slingerland M and Mooijaart SP: Functional
and cognitive impairment, social functioning, frailty and adverse
health outcomes in older patients with esophageal cancer, a
systematic review. J Geriatr Oncol. 9:560–568. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sohda M and Kuwano H: Current status and
future prospects for esophageal cancer treatment. Ann Thorac
Cardiovasc Surg. 23:1–11. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yang H, Liu H, Chen Y, Zhu C, Fang W, Yu
Z, Mao W, Xiang J, Han Y, Chen Z, et al: Neoadjuvant
chemoradiotherapy followed by surgery versus surgery alone for
locally advanced squamous cell carcinoma of the esophagus
(NEOCRTEC5010): A phase III multicenter, randomized, open-label
clinical trial. J Clin Oncol. 36:2796–2803. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Shapiro J, van Lanschot JJB, Hulshof MCCM,
van Hagen P, van Berge Henegouwen MI, Wijnhoven BPL, van Laarhoven
HWM, Nieuwenhuijzen GAP, Hospers GAP, Bonenkamp JJ, et al:
Neoadjuvant chemoradiotherapy plus surgery versus surgery alone for
oesophageal or junctional cancer (CROSS): Long-term results of a
randomised controlled trial. Lancet Oncol. 16:1090–1098. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tapias LF, Muniappan A, Wright CD,
Gaissert HA, Wain JC, Morse CR, Donahue DM, Mathisen DJ and Lanuti
M: Short and long-term outcomes after esophagectomy for cancer in
elderly patients. Ann Thorac Surg. 95:1741–1748. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Xu C, Xi M, Moreno A, Shiraishi Y, Hobbs
BP, Huang M, Komaki R and Lin SH: Definitive chemoradiation therapy
for esophageal cancer in the elderly: Clinical outcomes for
patients exceeding 80 years old. Int J Radiat Oncol Biol Phys.
98:811–819. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Markar SR, Karthikesalingam A, Thrumurthy
S, Ho A, Muallem G and Low DE: Systematic review and pooled
analysis assessing the association between elderly age and outcome
following surgical resection of esophageal malignancy. Dis
Esophagus. 26:250–262. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Steyerberg EW, Neville B, Weeks JC and
Earle CC: Referral patterns, treatment choices, and outcomes in
locoregional esophageal cancer: A population-based analysis of
elderly patients. J Clin Oncol. 25:2389–2396. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Miyata H, Yamasaki M, Makino T, Miyazaki
Y, Takahashi T, Kurokawa Y, Nakajima K, Takiguchi S, Mori M and
Doki Y: Clinical outcome of esophagectomy in elderly patients with
and without neoadjuvant therapy for thoracic esophageal cancer. Ann
Surg Oncol. 22 (Suppl 3):S794–S801. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Morita M, Otsu H, Kawano H, Kumashiro R,
Taketani K, Kimura Y, Saeki H, Ando K, Ida S, Oki E, et al:
Advances in esophageal surgery in elderly patients with thoracic
esophageal cancer. Anticancer Res. 33:1641–1647. 2013.PubMed/NCBI
|
|
12
|
Hamamoto Y, Akutsu Y, Nagashima F,
Hironaka S, Ito Y, Kato K, Hara H, Tsubosa Y, Nakagawa S, Daiko H,
et al: Multicenter questionnaire survey on patterns of care for
elderly patients with esophageal squamous cell carcinoma by the
Japan Esophageal Oncology Group. Jpn J Clin Oncol. 46:111–115.
2016.PubMed/NCBI
|
|
13
|
Talsma K, van Hagen P, Grotenhuis BA,
Steyerberg EW, Tilanus HW, van Lanschot JJ and Wijnhoven BP:
Comparison of the 6th and 7th Editions of the UICC-AJCC TNM
Classification for Esophageal Cancer. Ann Surg Oncol. 19:2142–2148.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zeng Y, Liang W, Liu J, He J, Ng CSH, Liu
CC, Petersen RH, Rocco G, D'Amico T, Brunelli A, et al: Esophageal
cancer in elderly patients: A population-based study. J Thorac Dis.
10:448–457. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Chen MF, Yang YH, Lai CH, Chen PC and Chen
WC: Outcome of patients with esophageal cancer: A nationwide
analysis. Ann Surg Oncol. 20:3023–3030. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Oyama T: Esophageal ESD: Technique and
prevention of complications. Gastrointest Endosc Clin N Am.
24:201–212. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Ikeda A, Hoshi N, Yoshizaki T, Fujishima
Y, Ishida T, Morita Y, Ejima Y, Toyonaga T, Kakechi Y, Yokosaki H
and Azuma T: Endoscopic submucosal dissection (ESD) with additional
therapy for superficial esophageal cancer with submucosal invasion.
Intern Med. 54:2803–2813. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kawaguchi G, Sasamoto R, Abe E, Ohta A,
Sato H, Tanaka K, Maruyama K, Kaizu M, Ayukawa F, Yamana N, et al:
The effectiveness of endoscopic submucosal dissection followed by
chemoradiotherapy for superficial esophageal cancer. Radiat Oncol.
10:312015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Morita M, Egashira A, Yoshida R, Ikeda K,
Ohgaki K, Shibahara K, Oki E, Sadanaga N, Kakeji Y and Maehara Y:
Esophagectomy in patients 80 years of age and older with carcinoma
of the thoracic esophagus. J Gastroenterol. 43:345–351. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Tougeron D, Di Fiore F, Thureau S, Berbera
N, Iwanicki-Caron I, Hamidou H, Paillot B and Michel P: Safety and
outcome of definitive chemoradiotherapy in elderly patients with
oesophageal cancer. Br J Cancer. 99:1586–1592. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Janjigian YY, Bendell J, Calvo E, Kim JW,
Ascierto PA, Sharma P, Ott PA, Peltola K, Jaeger D, Evans J, et al:
CheckMate-032 study: Efficacy and safety of nivolumab and nivolumab
plus ipilimumab in patients with metastatic esophagogastric cancer.
J Clin Oncol. 36:2836–2844. 2018. View Article : Google Scholar : PubMed/NCBI
|