Introduction
Worldwide, hepatocellular carcinoma (HCC) is the
fifth most frequent cancer among men and the seventh among women.
It frequently occurs in East Asia and Africa because of the high
incidence of hepatitis infection in these regions (1). To address this disease, various
treatment methods, curative and non-curative, have been developed
based on factors such as liver function, tumor burden, and tumor
size. For patients with single or up to three nodules of HCC, local
treatment such as surgery or radiofrequency ablation (RFA) is the
standard choice.
HCC is frequently comorbid in the cirrhotic liver
with chronic hepatitis B or C virus (HBV or HCV) infections that
cause HCC recurrence even after curative local treatment has been
performed and local control have been achieved. A 2011 report
indicated that the risk of HCC recurrence in the liver within five
years after liver resection or RFA amounts to 70% (1). This recurrence pattern has two types,
multicentric and intrahepatic (2),
which force HCC patients to receive repeated treatments every few
months or years.
Proton beam therapy (PBT) is a radiotherapy
characterized by ultra-precise delivery of high dose radiation that
limits off-target energy. HCC is one of the diseases to which PBT
is often applied for treatment (3–5). PBT was
started in our facility in 1983 and the current facility has been
dedicated to clinical research and practice since 2002. We have
since treated approximately 1400 HCC patients using proton beams
and have demonstrated that PBT has the ability to achieve excellent
local control of HCC without severe toxicity in several scientific
reports (6–8). Among those patients, a total of 160
patients have subsequently received repeated PBT as of 2017 and the
maximum number of treatment courses delivered has been 4 times in 3
of those patients. Although local treatment effect has been
demonstrated in many reports, intrahepatic recurrence is as
important an issue for PBT as other local treatments. In cases of
single or few recurrent tumors, PBT is one of the local treatment
options. However, as the number of treatments increase, cumulative
dosages elevate and overlap of dose distribution in many organs
would cause various clinical issues such as liver dysfunction,
digestive tract/skin ulcers, and bile duct stenosis. However, in
spite of the importance of this issue, it is poorly understood how
repeated PBT affects the prognosis and treatment-derived side
effects to the various organs from past studies of PBT. For this
reason, we here describe the long-term treatment outcomes in
patients who each received the maximum number of 4 courses of
repeated PBT. The present study was approved by Institutional
Research Committee of the University of Tsukuba (approval no.
H28-101).
Case 1
A 60-year-old man with HCV infection had HCC with a
maximum diameter of 1.2 cm in S4. PBT was performed using the
respiratory-gating technique with an irradiation dose of 66 gray
relative biological effectiveness [Gy (RBE)] in 10 fractions over
22 days. A second PBT round for a new 2.2 cm diameter tumor in S7
was performed 12 months later [66 Gy (RBE)] in 10 fractions over 14
days). The third PBT course for a new 1.5 cm diameter tumor in S3
was performed 10 months after the second PBT round [72.6 Gy (RBE)]
in 22 fractions over 31 days). A fourth and final PBT course for a
new 1.6 cm diameter tumor in S5 was performed 21 months after the
third PBT round [66 Gy (RBE)] in 10 fractions over 14 days)
(Fig. 1A). Note that we took great
care to minimize irradiation field overlap during all courses in
all patients. The total liver volume was 1286 cm3 at the
first PBT while the irradiated liver volumes {an absolute volume of
>1.0 Gy (RBE) delivery [V1.0 Gy (RBE)]} over the four
treatments were 90, 176, 115 and 442 cm3, respectively
(Fig. 1B). Serum concentrations of
aspartate aminotransferase (AST), alanine aminotransferase (ALT),
albumin (Alb) and total bilirubin (T. Bil) showed no significant
changes during follow up (Fig. 1C).
The Child-Pugh classification remained class A and no acute or late
treatment-related toxicity events of grade 2 or more (according to
the Common Terminology Criteria for Adverse Events, version 4.03)
were observed until the last follow-up 16 months after the fourth
PBT (60 months from the first PBT). A multiple intrahepatic
recurrence developed 22 months after the fourth PBT (66 months from
the first PBT). Alpha-fetoprotein (AFP) and Des-gamma
carboxyprothrombin (DCP) remained mainly below 100 mg/ml and 100
mAU/ml, respectively, during follow up (Fig. 1D). This patient died a total of 96
months after the first PBT.
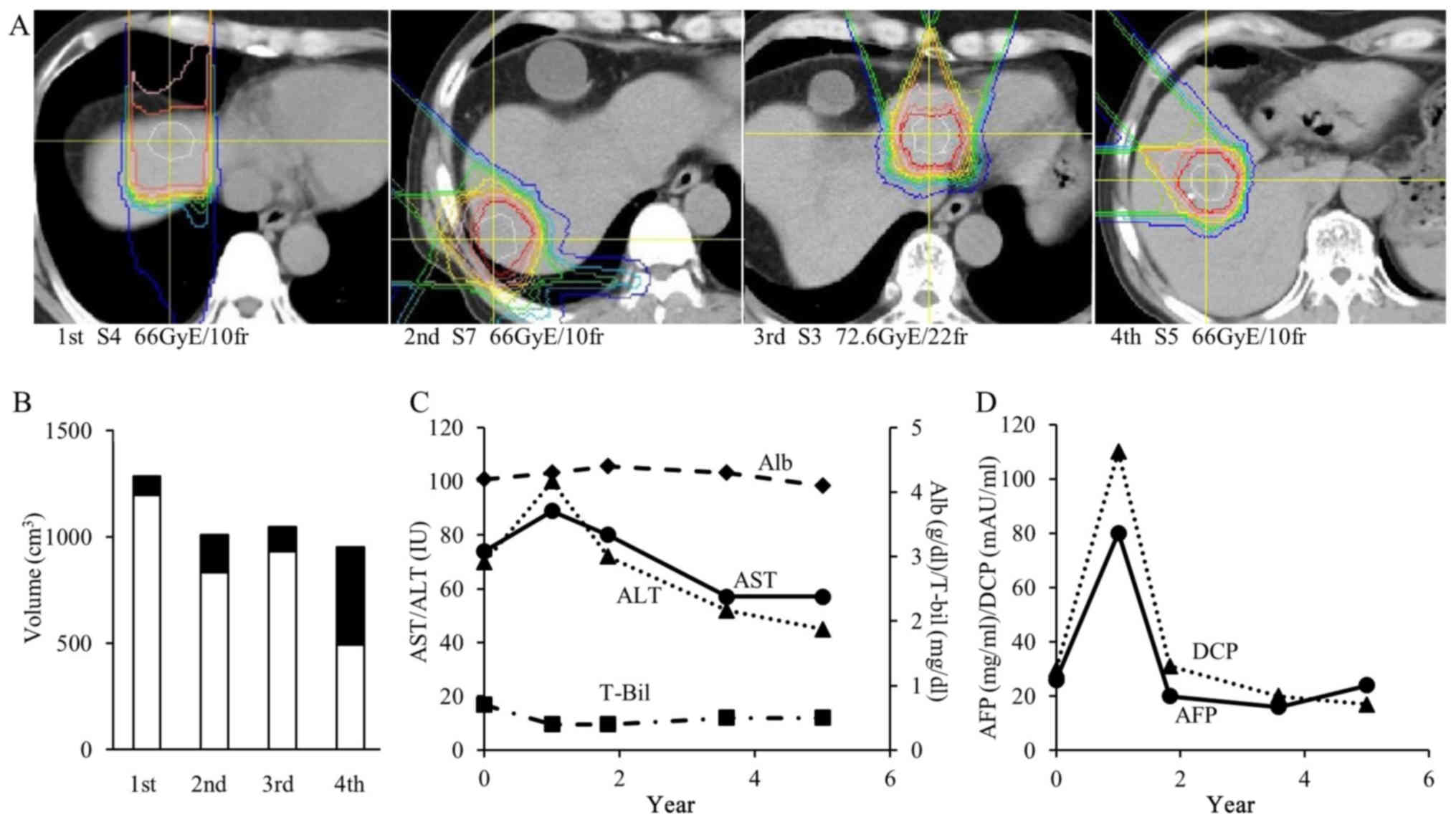 | Figure 1.A 60-year-old male patient with
hepatocellular carcinoma. (A) Dose distribution image of each
treatment. Dose lines represent 95–10% of the isocenter dose from
inside to outside. (B) Liver volume at each proton beam therapy.
Irradiated volume represents an absolute volume of >1.0 Gy (RBE)
delivery in the liver [V1.0 Gy (RBE)]. Unirradiated
volume represents an absolute volume <1.0 Gy (RBE) delivery in
the liver. (C) Change of liver function. AST, ALT, Alb and T. Bil
values following each treatment session and the last follow-up are
presented. (D) Change of tumor markers. AFP and DCP values at each
treatment session and last follow-up are presented. GY, gray; RBE,
relative biological effectiveness; AST, aminotransferase; ALT,
alanine aminotransferase, Alb, albumin; T. Bil, total bilirubin;
AFP, alpha-fetoprotein; DCP, Des-gamma carboxyprothrombin; S,
couinaud liver segment. |
Case 2
A 69-year-old man with HBV infection had an HCC of 3
cm in diameter in S8 and 4.5 cm in S6 and had already received
transarterial chemoembolization (TACE) 5 times before consulting
our hospital. PBT was performed simultaneously for the tumors in S8
[66 Gy (RBE) in 10 fractions over 15 days] and S6 [77 Gy (RBE) in
35 fractions over 57 days] and we confirmed that the two
irradiation fields did not overlap. A second PBT course for a new
2.7 cm diameter tumor in S8 was performed 25 months later [77 Gy
(RBE) in 35 fractions over 57 days]. A third PBT round for a new
1.8 cm diameter tumor in S8 was performed 14 months after the
second PBT [72.6 Gy (RBE) in 22 fractions over 34 days]. In this
treatment, beams were delivered from the back to avoid overlapping
the first irradiation field, although a right lateral beam could
have greatly reduced the irradiation dose of the right lung field.
The fourth and final PBT for a recurrent tumor of 7 cm in diameter
in S7/8 with inferior vena cava tumor thrombosis was performed 8
months after the third PBT course [66 Gy (RBE) in 10 fractions over
56 days] (Fig. 2A). The total liver
volume was 1073 cm3 at the first PBT while the
irradiated liver volumes over the four treatments were 260, 221,
114 and 330 cm3, respectively (Fig. 2B). Unirradiated volume in the liver
throughout all treatment was 320 cm3. Serum
concentrations of ALT showed no significant changes but AST and T.
Bil increased and Alb showed a reduced, albeit mild trend which was
noticeable after the fourth treatment (Fig. 2C). The Child-Pugh classification
remained class A and no acute or late treatment-related toxicity
events of grade 2 or more were observed. A multiple intrahepatic
recurrence appeared at 4 months after the fourth PBT (50 months
from the first PBT). AFP was largely decreased after first PBT and
rapidly increased after the second PBT. AFP once decreased from
2005 to 999 mg/ml during the fourth PBT but rebounded after that
then reached 1789 mg/ml 5 months after the fourth PBT. DCP showed a
similar pattern (Fig. 2D). This
patient died 51 total months after the first PBT.
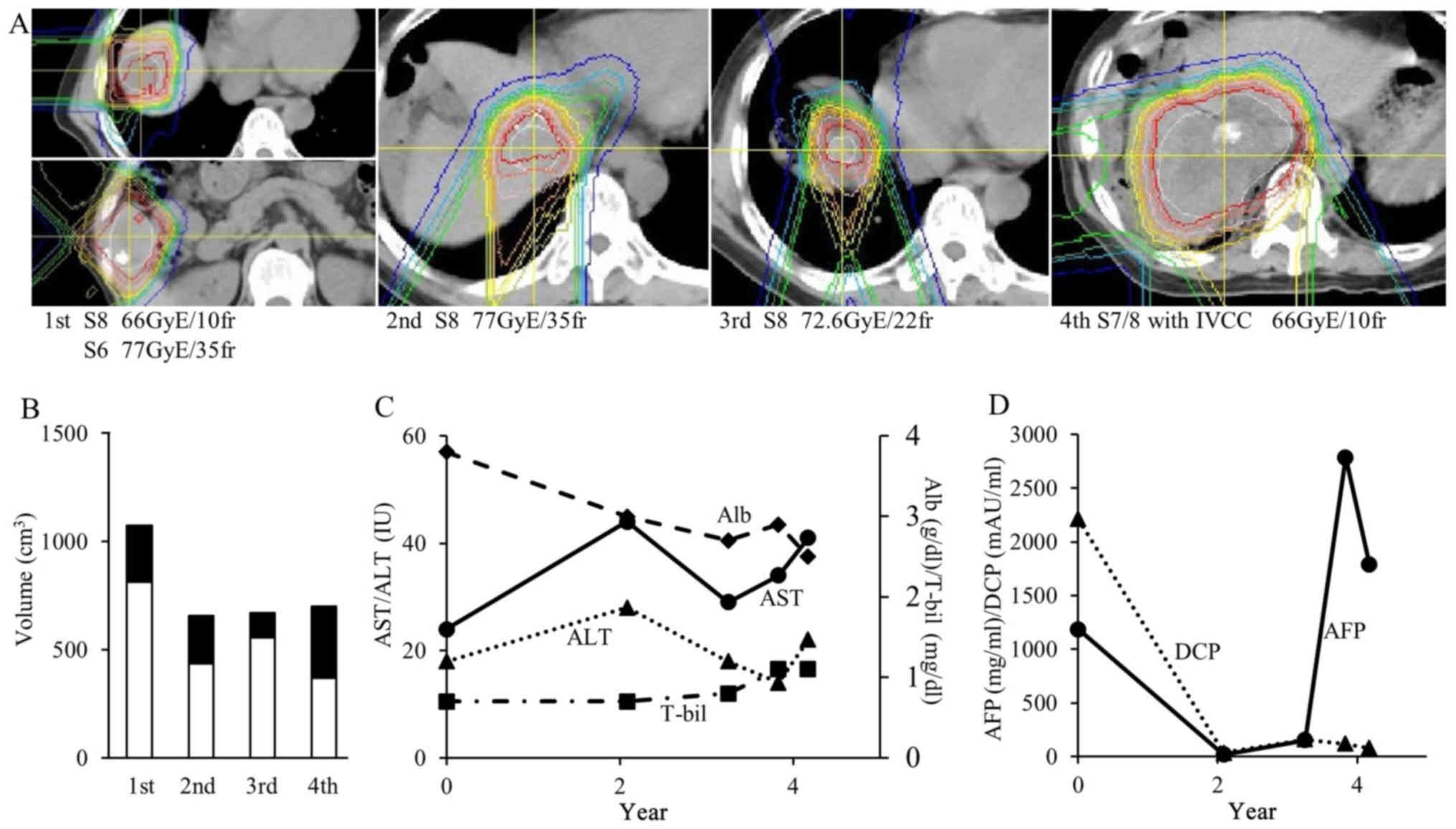 | Figure 2.A 69-year-old male patient with
hepatocellular carcinoma. (A) Dose distribution image of each
treatment. Dose lines represent 95–10% of the isocenter dose from
inside to outside. (B) Liver volume at each proton beam therapy.
(C) AST, ALT, Alb and T. Bil values following each treatment
session and the last follow-up are presented. (D) Change of tumor
markers. AFP and DCP values at each treatment session and last
follow-up are presented. AST, aminotransferase; ALT, alanine
aminotransferase, Alb, albumin; T. Bil, total bilirubin; AFP,
Alpha-fetoprotein; DCP, Des-gamma carboxyprothrombin; GY, gray;
RBE, relative biological effectiveness; S, couinaud liver
segment. |
Case 3
A 51-year-old man with HCV infection had multiple
HCC (1 cm in diameter in S5 and 1 cm in diameter in S6). PBT for
both tumors were performed simultaneously [66 Gy (RBE) in 10
fractions over 15 days] and we confirmed that the two irradiation
fields did not overlap. A second PBT round was then performed for a
new 2 cm diameter tumor in S8 10 months later [66 Gy (RBE) in 10
fractions over 16 days]. In this treatment, beams were delivered
from the front and right back to avoid overlapping the first
irradiation field, although a right lateral beam could have greatly
reduced the irradiation dose of the liver. A third PBT course for a
new 3 cm diameter tumor in S4 was performed 4 months after the
second PBT [66 Gy (RBE) in 10 fractions over 16 days]. The fourth
and final PBT course for a new 4 cm diameter tumor in S8 was
performed 27 months after the third PBT [72.6 Gy (RBE) in 22
fractions over 36 days] (Fig. 3A).
The total liver volume was 1624 cm3 at the first PBT
while the irradiated liver volumes over the four treatments
[V1.0 Gy (RBE)] were 225, 388, 177 and 295
cm3, respectively (Fig.
3B). Total liver volume was dramatically altered by the
repeated atrophy of the irradiation site and compensatory
hypertrophy of the normal liver. AST and ALT showed a downward
trend while Alb and T. Bil showed no significant changes (Fig. 3C). The Child-Pugh classification
remained class A and no acute or late treatment-related toxicity
events of grade 2 or more were observed until the last follow-up 60
months after the fourth PBT (101 months from the first PBT). A
multiple intrahepatic recurrence appeared at 61 months after the
fourth PBT (102 months from the first PBT). AFP and DCP showed no
relatively big changes mainly at levels below 100 mg/ml and 100
mAU/ml, respectively, until the fourth PBT, but there was a rapid
and large increase after that (Fig.
3D). This patient died 107 months after the first PBT.
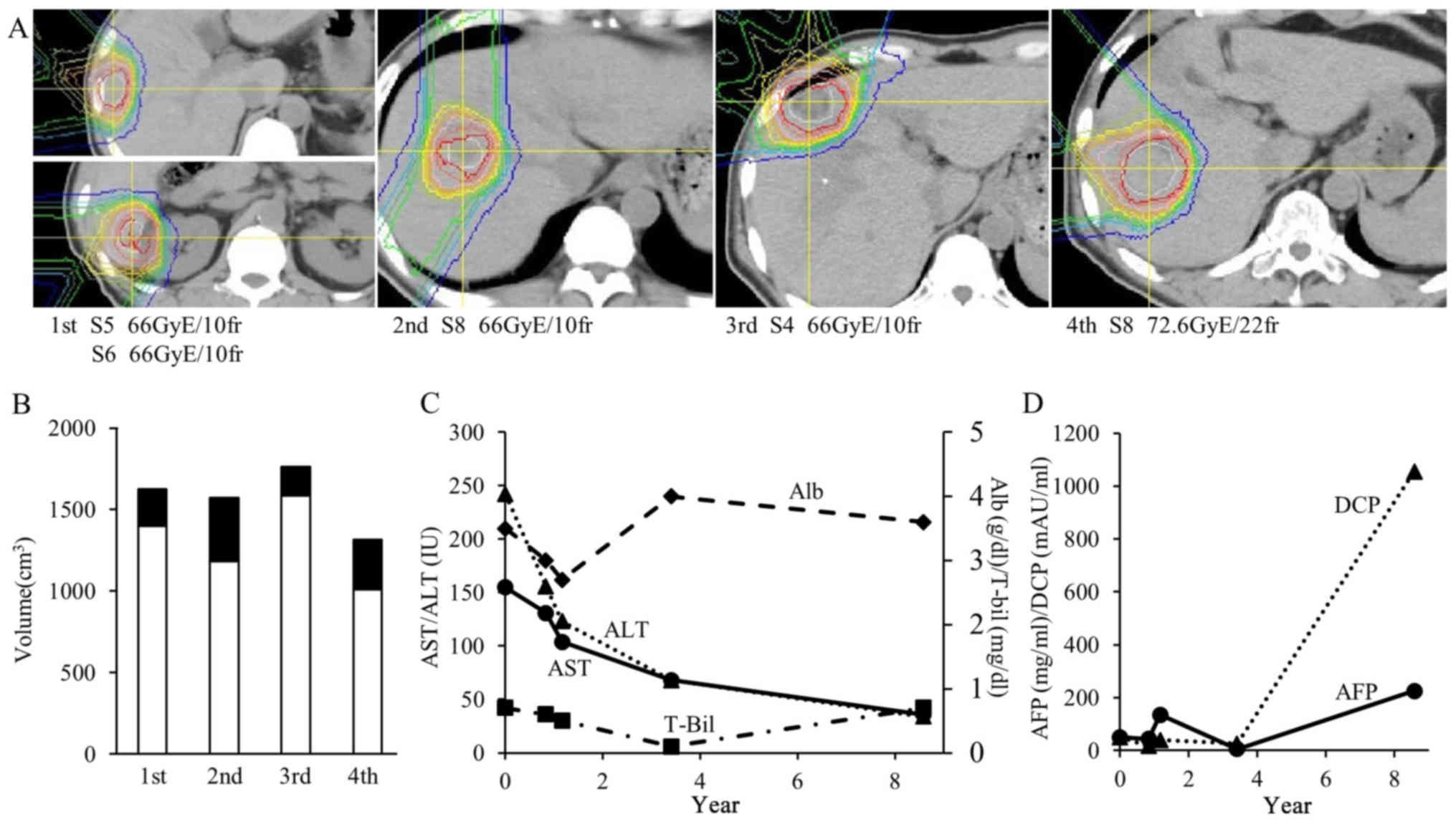 | Figure 3.A 51-year-old male patient with
hepatocellular carcinoma. (A) Dose distribution image of each
treatment. Dose lines represent 95–10% of the isocenter dose from
inside to outside. (B) Liver volume at each proton beam therapy.
(C) AST, ALT, Alb and T. Bil values following each treatment
session and the last follow-up are presented. (D) Change of tumor
markers. AFP and DCP values at each treatment session and last
follow-up are presented. AST, aminotransferase; ALT, alanine
aminotransferase, Alb, albumin; T. Bil, total bilirubin; AFP,
Alpha-fetoprotein; DCP, Des-gamma carboxyprothrombin; GY, gray;
RBE, relative biological effectiveness; S, couinaud liver
segment. |
Discussion
There are some reports which refer to outcomes
multiple treatment courses for HCC patients. Nishikawa et al
(9) reported that overall survival
rates of 130 relapsed patients treated with repeated-RFA were not
significantly different to those of 150 non-relapsed patients after
RFA. Joliat et al (10)
analyzed 67 patients with recurrent HCC after hepatectomy and found
that the median survival time for patients receiving surgery, RFA
or TACE was 77 months but it was 20 months for patients receiving
chemotherapy or palliative care. Additionally, the survival period
of those patients who received surgery/RFA/TACE was not
significantly different from non-relapsed patients (10). These reports demonstrate that
long-term survival can be obtained if sufficient local control is
achieved in spite of HCC recurrence. However, patients were treated
no more than twice in most of the published reports and there are
very few reports on the survival period after multiple treatment
courses for HCC.
While our facility commonly encounters HCC patients
with multiple treatment histories, a lack of literature on this
topic adds to the difficulty of accurately predicting patient
outcomes. Although (to the best of our knowledge) there are no
reports of repeated conventional photon radiotherapy treatments in
HCC patients, Lo et al (11)
reported the outcome of repeated stereotactic body radiotherapy
(SBRT) in 14 HCC patients. The median first treatment dose was 41
Gy and second treatment dose was 40 Gy, leading to 1 and 2-year
progression free survival rates of 68.6 and 42.9%, respectively,
and 1 and 2-year overall survival rates of 76 and 59.1%,
respectively. As for treatment effect, in-field recurrence happened
in only 1 of the 18 tumors (5.6%) but one patient developed
radiation-induced liver disease and three showed progression in
Child-Pugh classification after their second treatment. Sanuki
et al (12) reported that 4%
of patients who received SBRT suffered from fatal hepatic failure
within 12 months after SBRT and liver function and platelet count
can predict liver failure. Data such as these therefore indicate
that, although local control may be established, preservation of
liver function is not always guaranteed (12).
The criteria of repeated PBT in our facility is
exactly the same as the first PBT, namely that PS is 0–2,
Child-Pugh classification is A-B and tumor number must be single or
a few with an upper size limit of 15 cm. However, tumor location
and vessel invasion only have a small influence on treatment
adaptation. The existence of ascites requires more careful
treatment planning, especially if the ascites amount is unstable.
Maintenance of liver function is clinically very important for
repeated PBT but all three patients in our study were positive for
HBV or HCV, potentially impacting liver dysfunction. The irradiated
volume for the 12 total irradiation events was 7–50% of the total
liver volume, the summation of which corresponded to 51–91% of the
total liver volume at the first treatment. Most published liver
dosage tolerances are based on whole liver irradiation data
(13,14) and available data relating liver
tolerance to PBT are scarce. It is thought that liver function or
irradiation volume affects radiation-induced liver dysfunction
(15,16); however, no definite consensus has
been reached because of sparse data and reports. We therefore
defined our own dose constraint as an unirradiated liver volume of
> 500 cm3 based on our previous studies and clinical
experience (15). However, the
unirradiated volume is occasionally forced to be <500
cm3 by repeat irradiation. In such cases, liver dosage
and treatment protocol are determined by multiple considerations,
including age, PS, liver function, treatment strategy, patient
wishes, etc. (example: Case 2). It is fortunate that no severe side
effects occurred in these 3 cases. Clarification of the ability of
these 3 patients to tolerate PBT for 4 courses is important. Our
precise dose calculation for each organ and careful treatment
strategy may be responsible. Alternately, these patients might have
had some pathological condition or constitution conducive to
enduring repeated treatment. One possible common point was the
maintenance of liver function over several years after the first
PBT in spite of the repetitive treatment. Next, as far as observing
the transition of the biomarkers in these 3 cases, viral hepatitis
and cumulative dosage to the liver did little to affect the
prognosis. In summation, although we cannot conclude how liver
dysfunction was avoided from such a small cohort, further studies
with higher patient numbers could shed light upon this issue.
We have previously reported the results of
repetitive PBT for HCC at our facility. At the initial treatment
center (1989–2000), we analyzed 27 cases and revealed that
re-irradiation is safe if liver function is Child-Pugh class A and
the target is located in a peripheral tumor (17). At the current center (2002–2010), 83
cases were analyzed and it was revealed that liver function tended
to gradually decline as the number of irradiation events increased
(18). As the number of treatment
courses piles on top of cumulative dose elevation, the treatment
effect becomes difficult to be predicted and risk to normal organs
becomes higher. In general, this analysis features long-term
follow-ups and descriptions of side effects for selected HCC
patients receiving many repetitions of PBT, which differs from past
studies of PBT for HCC. Moreover, this data lends credence to our
recommendation that repeated PBT can be safely selected for the
curative treatment of HCC.
There are some limitations in the current study.
Various reports for liver dose tolerance exist but they are mostly
based on the outdated concept of total liver irradiation, which may
not always apply to modern, locally high dose treatment. Another
subject is deformation of the liver, which dramatically and
non-uniformly deforms after PBT in patients with chronic liver
disease (18,19). This means that our method of summing
irradiated volumes by simply adding them together may be overly
simplistic. However, it is technically difficult to correctly
calculate cumulative dose distribution in deformed livers,
highlighting the necessity to improve dose distribution calculation
techniques which can overcome this limitation and establish the
safety of repeated PBT.
Here, we reported on three HCC patients who each
received 4 courses of PBT. Liver function was considerably
preserved until final follow-up and long-term survival (>48
months) was achieved. We consider that PBT has the potential to be
applied to recurrent HCC due to less liver damage and a superior
local treatment effect. Repeated PBT can therefore be an effective
treatment option for persistently recurring HCC.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All data and materials included in the present study
are included in this published article.
Authors' contributions
MMu, NF, HS and TO wrote this manuscript and
analyzed all of the data. NF, TO, HN, KM, KO, HI, KT and MMi
provided medical care for the patients and collected the data. TO
and HS revised the article. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
The present study was approved by institutional
research committee of University of Tsukuba (approval no.
H28-101).
Patient consent for publication
Patient consent was obtained for publication.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
El-Serag HB: Hepatocellular carcinoma. N
Engl J Med. 365:1118–1127. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Yamamoto T, Kajino K, Kudo M, Sasaki Y,
Arakawa Y and Hino O: Determination of the clonal origin of
multiple human hepatocellular carcinomas by cloning and polymerase
chain reaction of the integrated hepatitis B virus DNA. Hepatology.
29:1446–1452. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Komatsu S, Fukumoto T, Demizu Y, Miyawaki
D, Terashima K, Sasaki R, Hori Y, Hishikawa Y, Ku Y and Murakami M:
Clinical results and risk factors of proton and carbon ion therapy
for hepatocellular carcinoma. Cancer. 117:4890–4904. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kawashima M, Kohno R, Nakachi K, Nishio T,
Mitsunaga S, Ikeda M, Konishi M, Takahashi S, Gotohda N, Arahira S,
et al: Dose-volume histogram analysis of the safety of proton beam
therapy for unresectable hepatocellular carcinoma. Int J Radiat
Oncol Biol Phys. 79:1479–1486. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Chadha AS, Gunther JR, Hsieh CE, Aliru M,
Mahadevan LS, Venkatesulu BP, Crane CH, Das P, Herman JM, Koay EJ,
et al: Proton beam therapy outcomes for localized unresectable
hepatocellular carcinoma. Radiother Oncol. 133:54–61. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Mizumoto M, Okumura T, Hashimoto T, Fukuda
K, Oshiro Y, Fukumitsu N, Abei M, Kawaguchi A, Hayashi Y, Ookawa A,
et al: Proton beam therapy for hepatocellular carcinoma: A
comparison of three treatment protocols. Int J Radiat Oncol Biol
Phys. 81:1039–1045. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Chiba T, Tokuuye K, Matsuzaki Y, Sugahara
S, Chuganji Y, Kagei K, Shoda J, Hata M, Abei M, Igaki H, et al:
Proton beam therapy for hepatocellular carcinoma: A retrospective
review of 162 patients. Clin Cancer Res. 11:3799–3805. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Fukumitsu N, Sugahara S, Nakayama H,
Fukuda K, Mizumoto M, Abei M, Shoda J, Thono E, Tsuboi K and
Tokuuye K: A prospective study of hypofractionated proton beam
therapy for patients with hepatocellular carcinoma. Int J Radiat
Oncol Biol Phys. 74:831–836. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Nishikawa H, Osaki Y, Iguchi E, Takeda H,
Ohara Y, Sakamoto A, Hatamaru K, Saito S, Nasu A, Kita R and Kimura
T: Percutaneous radiofrequency ablation therapy for recurrent
hepatocellular carcinoma. Anticancer Res. 32:5059–5065.
2012.PubMed/NCBI
|
|
10
|
Joliat GR, Allemann P, Labgaa I,
Demartines N and Halkic N: Treatment and outcomes of recurrent
hepatocellular carcinomas. Langenbecks Arch Surg. 402:737–744.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Lo CH, Huang WY, Lin KT, Lin MJ, Lin TP
and Jen YM: Repeated stereotactic ablative radiotherapy using
CyberKnife for patients with hepatocellular carcinoma. J
Gastroenterol Hepatol. 29:1919–1925. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Sanuki N, Takeda A, Oku Y, Eriguchi T,
Nishimura S, Aoki Y and Kunieda E: Influence of liver toxicities on
prognosis after stereotactic body radiation therapy for
hepatocellular carcinoma. Hepatol Res. 45:540–547. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ingold JA, Reed GB, Kaplan HS and Bagshaw
MA: Radiation hepatitis. Am J Roentgenol Radium Ther Nucl Med.
93:200–208. 1965.PubMed/NCBI
|
|
14
|
Emami B, Lyman J, Brown A, Coia L, Goitein
M, Munzenrider JE, Shank B, Solin LJ and Wesson M: Tolerance of
normal tissue to therapeutic irradiation. Int J Radiat Oncol Biol
Phys. 21:109–122. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Mizumoto M, Okumura T, Hashimoto T, Fukuda
K, Oshiro Y, Fukumitsu N, Abei M, Kawaguchi A, Hayashi Y, Ohkawa A,
et al: Evaluation of liver function after proton beam therapy for
hepatocellular carcinoma. Int J Radiat Oncol Biol Phys.
82:e529–e535. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Hsieh CE, Venkatesulu BP, Lee CH, Hung SP,
Wong PF, Aithala SP, Kim BK, Rao A, Tung-Chieh Chang J, Tsang NM,
et al: Predictors of radiation-induced liver disease in eastern and
western patients with hepatocellular carcinoma undergoing proton
beam therapy. Int J Radiat Oncol Biol Phys. S0360-3016(19)30264-0.
Feb 21–2019.(Epub ahead of print). View Article : Google Scholar
|
|
17
|
Hashimoto T, Tokuuye K, Fukumitsu N, Igaki
H, Hata M, Kagei K, Sugahara S, Ohara K, Matsuzaki Y and Akine Y:
Repeated proton beam therapy for hepatocellular carcinoma. Int J
Radiat Oncol Biol Phys. 65:196–202. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Oshiro Y, Mizumoto M, Okumura T, Fukuda K,
Fukumitsu N, Abei M, Ishikawa H, Takizawa D and Sakurai H: Analysis
of repeated proton beam therapy for patients with hepatocellular
carcinoma. Radiother Oncol. 123:240–245. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Fukumitsu N, Takahashi S, Okumura T,
Ishida T, Murofushi KN, Ohnishi K, Aihara T, Ishikawa H, Tsuboi K
and Sakurai H: Normal liver tissue change after proton beam
therapy. Jpn J Radiol. 36:559–565. 2018. View Article : Google Scholar : PubMed/NCBI
|














