Introduction
By undertaking local treatment, such as surgical
resection, radiation therapy or radiofrequency ablation, for a
small number of recurrent or metastatic cancers for metastatic
lesions, patient survival can be prolonged (1). Patients with oligometastasis (OM)
follow a unique course and, according to previous reviews (1,2), there
is increasing evidence of improved prognosis for this condition.
According to National Cancer Institute Dictionary (3), OM is a type of metastasis in which
cancer cells from the original primary tumor travel through the
body and form a small number of new metastatic tumors in one or
more other parts of the body.
According to a review by Ashworth et al
(1), local treatment, such as
surgical resection or stereotactic body radiation therapy (SBRT),
has emerged as an additional treatment for OM. Either surgical
resection, chemoradiotherapy (CRT) or a tri-modality of surgery
plus CRT is commonly selected as a curative treatment strategy
(4,5).
Depending on location, SBRT induces minimal side
effects and exhibits long-lasting local control (2,6-8).
However, there are limited data concerning the outcome and side
effects following SBRT for metastasis. A study to investigate the
safety, efficacy and toxicity of SBRT for OM is therefore required.
Certain clinical data exist regarding the application of SBRT, with
a protocol of 50 Gy delivered in 10 fractions for OM at various
sites except for the brain (9-12).
SBRT has also been used for OM in the abdominal lymph nodes (LNs)
(5,13-16).
Although concurrent CRT has become the first method
of choice for isolated LN metastasis after primary radical
treatment for solid cancers, certain clinical cases exist for which
the administration of chemotherapy is difficult, due to reasons
such as having an unsatisfactory general condition, renal failure
or being elderly, and in such cases, radiation therapy alone
becomes a treatment option; however, the local control rate is
inadequate when using conventional radiation therapy alone with 2
Gy for each fraction (5,8,10-15).
Therefore, it is highly likely that SBRT using an increased
radiation dose per fraction will be more useful due to the enhanced
antitumor effect.
At our institution, in cases where the
administration of chemotherapy was difficult on the basis of the
cancer being inoperable for various reasons, including patients who
refused surgery, or had decreased renal function or poor general
condition, SBRT was performed for OM after primary radical
treatment. The safety and effectiveness of SBRT in the treatment of
OM from various cancers were examined in the present study.
Materials and methods
Study participants
A total of 40 patients were recruited in this
retrospective cohort study (median age, 70 years; range, 51-91
years; 29 males and 11 females) at the University of Tokyo Hospital
between February 2012 and April 2017. Ethical approval was granted
by the Clinical Research Review Board of the University of Tokyo
Hospital. Informed consent was obtained from all patients prior to
the initiation of procedures.
The following inclusion criteria were set for the
study: i) The maximum diameter of the OM was not more than 5 cm;
ii) up to three lesions per patient were present; iii) an
increasing trend for computed tomography (CT) scanning was noted;
iv) by positron emission tomography (PET) scanning, an accumulation
of 2-(18F)fluoro-2-deoxy-D-glucose (FDG) with a maximum
standardized uptake value (SUV-max) ≥2.0 was present (15); v) the OM lesion was judged as
inoperable by the respiratory cancer board; vi) there was no
history of radiation therapy for the target lesion; vii) the
Karnofsky performance status (KPS) (17) was ≥60%; viii) the primary tumor was
confirmed via pathology; and ix) the prognosis was expected to be
>3 months.
Treatment
SBRT of a total of 50 Gy in 10 fractions was
performed 5 times a week using a linear accelerator (linac).
Adjuvant therapy was not acceptable soon after SBRT. However,
additional treatment for relapse cases after SBRT was allowed. This
treatment had been performed since February 2012, and those
patients who received SBRT up to April 2017 were analyzed.
Irradiation method
Image-guided radiation therapy was performed each
time. Each OM was contoured as separate irradiation sites.
Four-dimensional (4D)-CT was used when possible.
The gross tumor volume (GTV) was for a tumor
detectable via CT. The internal target volume (ITV) was calculated
from the sum of all GTVs from 4D-CT. The margin between the ITV and
clinical target volume (CTV) was 0 mm. In other words, the
microinvasive margin was not added. The margin between the CTV and
the planning target volume (PTV) was 5 mm in all six directions.
The stomach, duodenum, small intestine, liver, spinal cord and
kidney were contoured as the organs at risk. The prescribed dose
was calculated to cover 95% of PTV or the point of the isocenter
using volumetric modulated arc therapy (VMAT). The total radiation
dose was 50 Gy in 10 fractions over 2 weeks. The biologically
effective dose (BED) in the α/β=10 was 75 Gy.
Adverse events related to SBRT were evaluated using
the National Cancer Institute Common Terminology Criteria for
Adverse Events version 3.0(18). The
primary tumor at initial diagnosis was staged according to the
sixth edition of the American Joint Committee on Cancer (19).
Follow-up schedule
Regarding the post-treatment follow-up schedule,
neck, chest, abdominal and pelvic CT scans with contrast if
possible were performed at intervals of 3-4 months for the first 3
years, and 4-6 months after this time point. Complete response was
evaluated according to the Response Evaluation Criteria In Solid
Tumors criteria (version 1.1) (20).
Statistical analysis
Survival curves were drawn according to the
Kaplan-Meier method. P-values in the univariate analysis for
overall survival (OS) were calculated by the log-rank test. The 95%
confidence interval (CI) was calculated using Greenwood's formula
(21). The significance level was
set at 5%. An event was defined as any death in OS calculations,
and as any death or progression in progression-free survival
calculations, respectively.
Results
A total of 40 patients and 49 lesions fulfilled the
aforementioned criteria for the present study. Patient and disease
characteristics are presented in Table
I. The highest KPS score was 90%. Primary tumors in patients
recruited in this study were most frequently located in the
esophagus (45%), with the lungs the second most common site (20%).
Surgical resection was the most common primary therapy (83%).
 | Table IPatient and disease
characteristics. |
Table I
Patient and disease
characteristics.
| Parameter | Number of cases | Frequency (%) |
|---|
| Number of
patients | 40 | |
| Number of
lesions | 49 | |
| Age at the start of
SBRT, years (n=40) | | |
|
Median
(range) | 70 (51-91) | |
| KPS at SBRT
(n=49) | | |
|
70% | 6 | 12.8 |
|
80% | 9 | 19.1 |
|
90% | 32 | 68.1 |
|
100% | 0 | |
| Gender (n=40) | | |
|
Male | 29 | 75.0 |
|
Female | 11 | 25.0 |
| Primary tumor
(n=40) | | |
|
Esophagus | 18 | 45.0 |
|
Lung | 8 | 20.0 |
|
Colorectum | 4 | 10.0 |
|
Uterus | 3 | 7.5 |
|
Thymus | 2 | 5.0 |
|
Head and
neck | 2 | 5.0 |
|
Liver | 2 | 5.0 |
|
Liposarcoma | 1 | 2.5 |
| Primary treatment
(n=40) | | |
| Radical surgery | 33 | 82.5 |
| Definitive
chemoradiation | 6 | 15.0 |
| Chemotherapy | 1 | 2.5 |
Target lesion characteristics are presented in
Table II. The median interval
between primary therapy and OM was 25 months. OM occurred most
frequently in the mediastinal LN (61%). A solitary metastasis
comprised the largest proportion of cases (92%). The median value
of the SUV-max was 5.0. Loco-regional metastases of the primary
tumor comprised 55% of OM sites. The median GTV was 18
cm3, and the median PTV was 32.9 cm3 (range,
15.6-166.4 cm3).
| Table IITarget lesion characteristics
(n=49). |
Table II
Target lesion characteristics
(n=49).
| Characteristics | Number of cases | Frequency (%) |
|---|
| Interval between
diagnosis of primary tumor and SBRT/per lesion (months) |
|
Mean | 41 | |
|
Median
(range) | 25 (2-169) | |
| SBRT site |
|
Mediastinum
LN | 30 | 61.2 |
|
Supraclavicular
LN | 7 | 14.3 |
|
Chest
wall/pleural/rib | 4 | 8.2 |
|
Pelvic/Para-aortic
LN | 4 | 8.2 |
|
Hilar
LN | 3 | 6.1 |
|
Axilla
LN | 1 | 2.0 |
| Number of treated
lesions |
|
1 | 45 | 91.8 |
|
2 | 3 | 6.1 |
|
3 | 1 | 2.0 |
| SUV-max by
FDG-PET |
|
Median
(range) | 5.0 (2.3-17.1) | |
| SBRT treatment
group |
|
Locoregional | 27 | 55.1 |
|
Metastatic | 22 | 44.9 |
| GTV volume
(cm3) |
|
Mean | 25.0 | |
|
Median
(range) | 18.0
(8.0-120.0) | |
| GTV >60 cc | 3 lesions | |
The outcomes of SBRT are summarized in Table III. The progression of lesions
within a radiation field was not observed during the follow-up
period. At the last observation, half of all patients had succumbed
to cancer. The rate of disease-free patients was 45%; 60% of cases
ended with distant progression (some of these cases were cured by
salvage therapy), occurring in the lung, LN, primary tumor site,
liver, bone and brain in eight, seven, three, three, two and one
cases, respectively.
| Table IIISBRT outcomes. |
Table III
SBRT outcomes.
| Outcome | Number of
cases | Frequency (%) |
|---|
| Response to SBRT
(n=49) |
|
Complete
response | 24 | 49.0 |
|
Partial
response | 8 | 16.3 |
|
Stable
disease | 8 | 16.3 |
|
Progressive
disease (local) | 0 | 0 |
|
Distant
progression (n=40) | 24 | 60.0 |
| Status at the last
observation (n=40) |
|
No evidence
of disease | 18 | 45.0 |
|
Alive with
disease | 0 | 0 |
|
Cancer-related
mortality | 20 | 50.0 |
|
Unrelated
mortality | 2 | 5.0 |
All SBRT treatments were intended to be curative. As
for the disease extent at the onset of SBRT, all 49 lesions were
not associated with other lesions. A total of 9 patients underwent
prior radiotherapy for the primary tumor. No concomitant systemic
therapy was undertaken for all 49 lesions. Two patients received
chemotherapy prior to SBRT.
The median follow-up time was 14.0 months (range,
6.8-57.1 months). The median time to distant progression after SBRT
was 4.9 months (range, 0.7-34.2 months); the time was computed from
a diagnosis of the treated OM. The date of initiating SBRT for OM
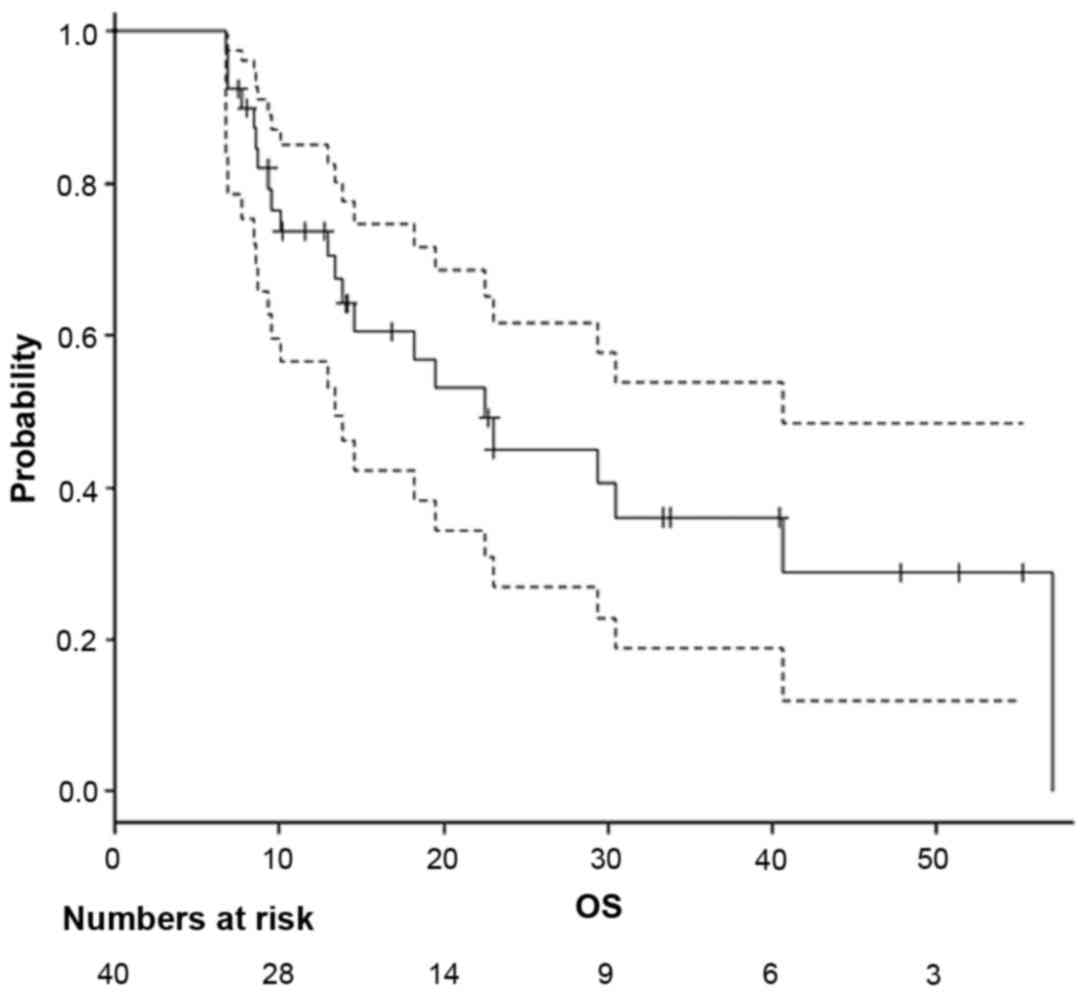
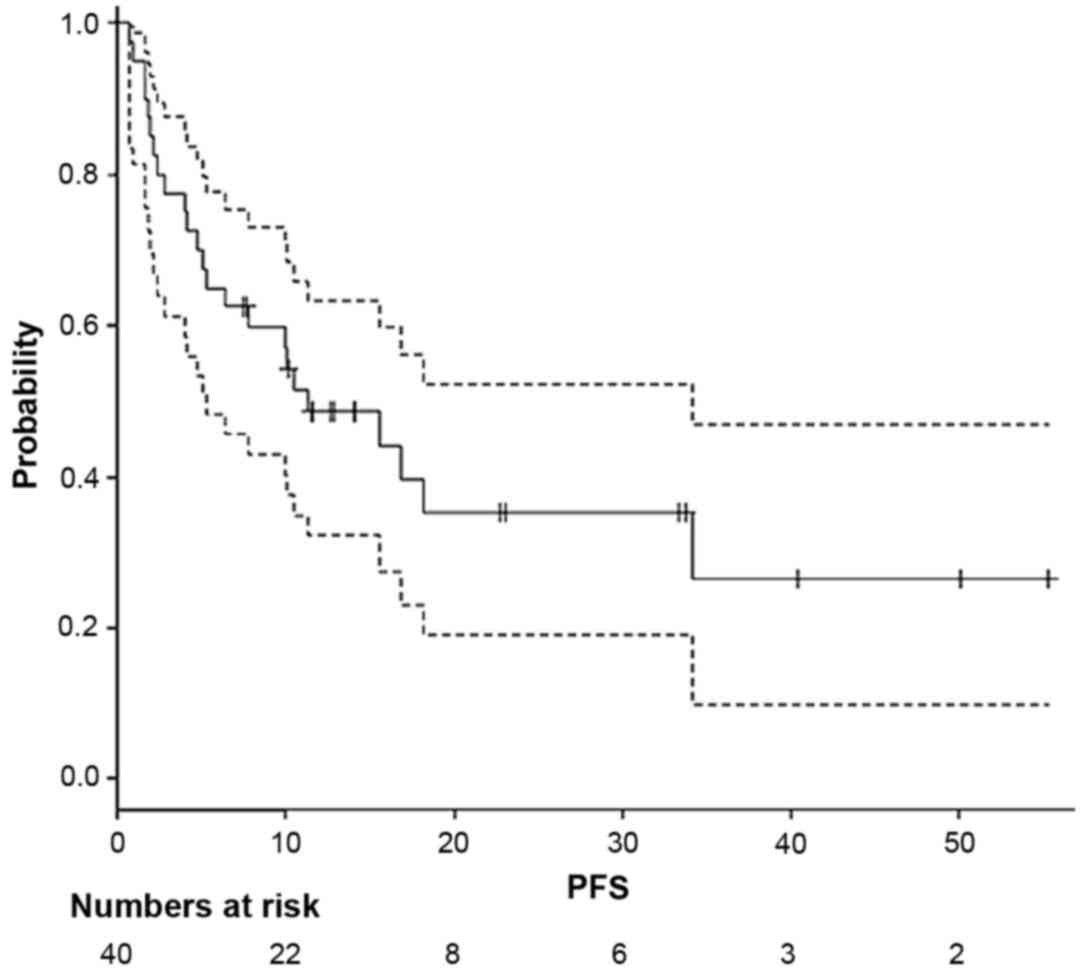
was calculated as day 0 in survival. OS (Fig. 1) and progression-free survival (PFS;
Fig. 2) curves were generated using
the Kaplan-Meier method. The median survival time was 22.5 months
(95% CI, 13.3-40.7 months). The 2- and 3-year OS rates were 45.1%
(range, 26.9-61.7%) and 36.1% (range, 18.8-53.7%), respectively.
The median PFS time was 11.3 months (range, 5.3-34.2 months). The
2- and 3-year PFS rates were 35.4% (range, 19.0-52.2%) and 26.5%
(range, 9.7-47.0%), respectively. The median survival time of the 2
patients who received pre-chemotherapy before SBRT was 14.5 and
12.7 months, respectively. Additionally, the median survival time
of 1 patient with three OM lesions was 23.0 months.
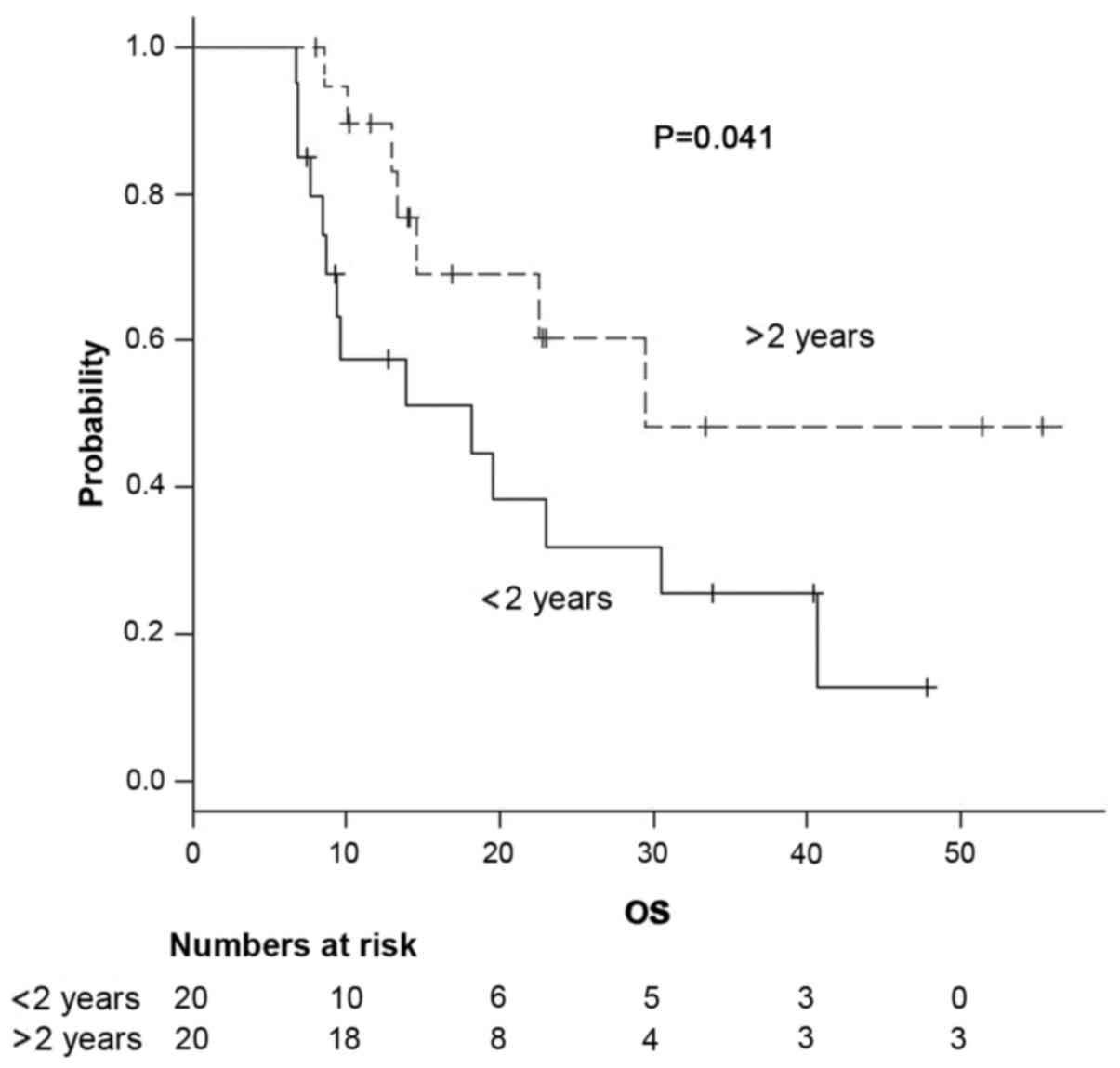
The results of the univariate analysis of factors
that affected OS and PFS are presented in Table IV. A significant difference in both
OS and PFS was seen based on the interval between diagnosis and
detection of OM (<2 years vs. >2 years (P=0.041 and P=0.028,
respectively, via log-rank test; Fig.
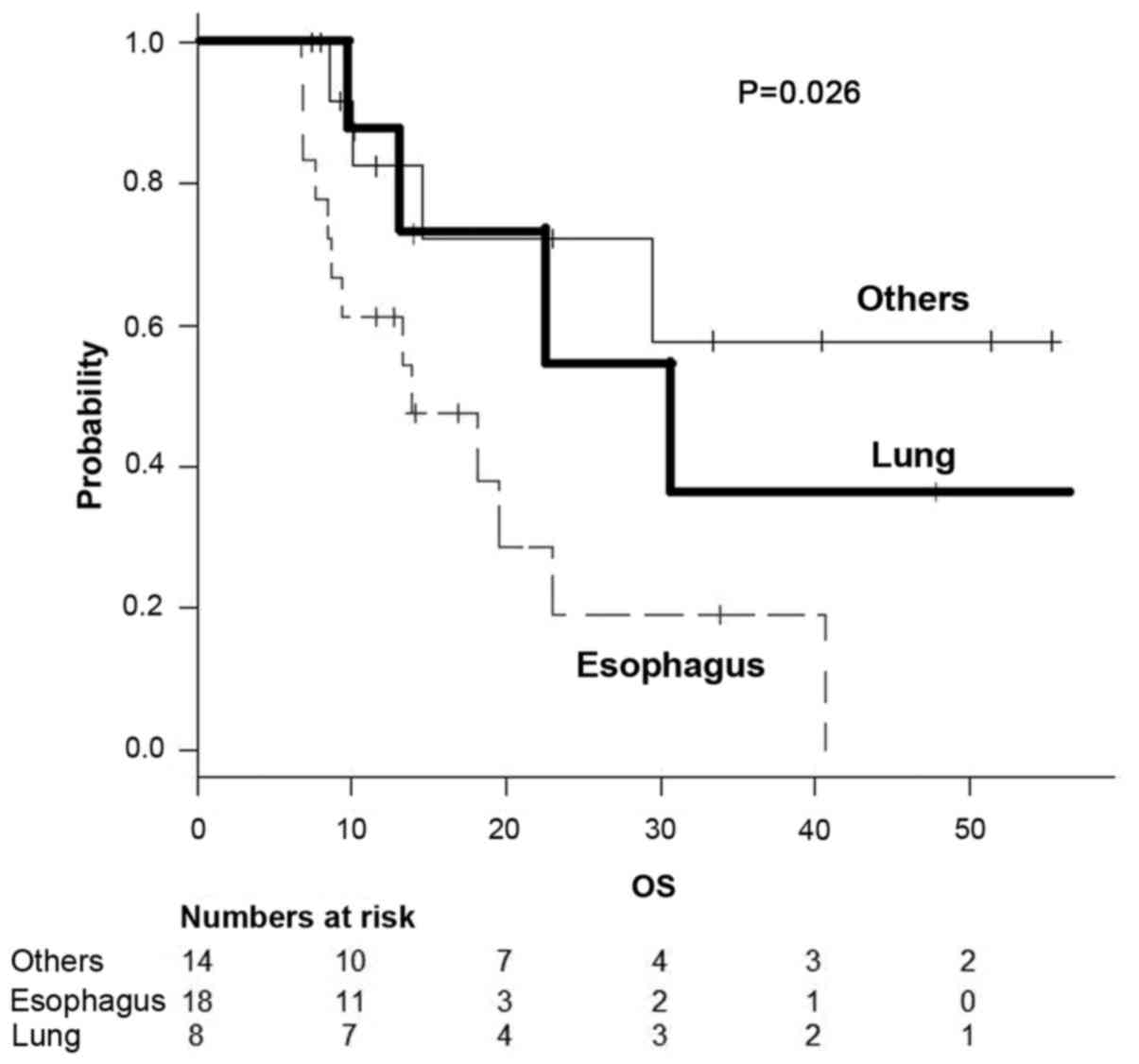
3). A primary tumor located in the esophagus was significantly
associated with worse OS compared with lung or other locations
(P=0.026; Fig. 4). Patients with OM
from esophageal cancer succumbed to further distant metastases
(n=9) or local recurrence (n=3) with the exception of 1 patient;
patients with OM from lung cancer died of further distant
metastases (n=5) and no local recurrence.
| Table IVUnivariate analysis of factors that
affected OS and PFS. |
Table IV
Univariate analysis of factors that
affected OS and PFS.
| | | OS | | PFS | |
|---|
| Factors | N | Median
(months) | 95% CI
(months) | P-value | Median
(months) | 95% CI
(months) | P-value |
|---|
| GTV |
|
>20
cm3 | 18 | 14.5 | 9.6-30.5 | 0.12 | 7.5 | 2.8-16.8 | 0.052 |
|
≤20
cm3 | 22 | 40.1 | 12.9-NA | | 34.2 | 6.4-NA | |
| Interval between
the primary therapy and OM (years) |
|
≤1 | 7 | 19.5 | 6.8-NA | 0.32 | 10.0 | 2.8-NA | 0.29 |
|
>1 | 33 | 23.0 | 13.3-NA | | 11.3 | 5.3-NA | |
|
≤2 | 20 | 18.2 | 8.4-30.5 | 0.041 | 7.7 | 1.9-16.8 | 0.028 |
|
>2 | 20 | 29.4 | 13.3-NA | | 34.2 | 6.4-NA | |
| Primary tumor |
|
Esophagus | 18 | 13.8 | 8.4-23.0 | 0.026 | 7.7 | 2.8-15.6 | 0.10 |
|
Lung | 8 | 30.5 | 9.6-NA | | 16.8 | 2.2-NA | |
|
Others | 14 | NA | 10.1-NA | | NA | 2.4-NA | |
| SBRT target |
|
Mediastinum | 25 | 23.0 | 12.9-NA | 0.65 | 15.6 | 7.7-34.2 | 0.55 |
|
Others | 15 | 14.5 | 8.5-NA | | 6.4 | 1.7-NA | |
| Primary
treatment |
|
Surgical
resection | 30 | 29.4 | 13.3-NA | 0.088 | 10.5 | 5.3-NA | 0.57 |
|
Others | 10 | 22.5 | 6.8-NA | | 11.3 | 0.7-NA | |
For acute radiation toxicities, five events were
grade 1 and two events were grade 2. For subacute and late
toxicities, grade 3 radiation enteritis was seen in one case at 0.7
months, grade 4 radiation proctitis in one case at 2.7 months and
grade 4 radiation mediastinitis in one case at 9.0 months after
SBRT.
Discussion
In the present study, the median survival time after
SBRT for OM was ~2 years, a period comparable to that observed in
previous reports (5), although study
participants were not approved for concurrent chemoradiation. As
92% of patients had a single isolated OM in this study, treatment
results may have been relatively positive even without combined
chemotherapy. In 2012, Jereczek-Fossa et al (22) reported the outcome of SBRT using 33
Gy in three fractions for 16 LN cancers from prostate cancer. No
regrowth occurred within the irradiated field, while PFS was >30
months. In 2014, the same group (18) performed linac-based SBRT for the
recurrence of isolated abdominal LN cancers. Various dose fractions
such as 6-45 Gy in 1-5 fractions (mean, 24 Gy) were included. The
median BED was 120 Gy. For 81 evaluable lesions, a complete
response was achieved in 44% of lesions, a partial response in 26%
and stable disease in 25%. Milano et al (23) reported that the 2-year local control
rate was 74% in non-breast cancer cases. Surgical resection is less
likely to be indicated for abdominal LN cancers, while a high local
control rate of 70-80% after SBRT has been reported (20,21). The
49 lesions within the irradiation field had not progressed in any
of the cases examined. This indicated that the irradiation dose of
50 Gy in 10 fractions was sufficient. However, new distant
metastases developed outside the irradiation field, which were the
cause of death in a number of cases.
For patients who showed an interval prior to OM
occurrence of >2 years, the prognosis was improved compared with
those with an interval <2 years, as previously reported
(4). OM from esophageal cancer had a
worse prognosis than that from other primary tumors. This is
consistent with the fact that esophageal cancer itself has a poor
prognosis (23). The site of OM was
not a prognostic factor. As most patients had an isolated OM, the
difference in prognosis according to the number of OM could not be
compared in this study.
Further distant metastases were more likely to occur
in patients with OM from esophageal cancer (50%) and lung cancer
(62.5%). The difference in survival for each type of cancer could
be justified by their differing characteristics.
A grade 4 side effect of radiation therapy was
observed in two cases. In both cases, a recurrence outside of the
field occurred at the same time as the side effect. A case showing
a grade 4 intestinal perforation had uncontrolled diabetes. In a
case with an esophageal perforation, a higher radiation-dose region
had spread around the trachea, perhaps as it was difficult to
increase the dose to the surrounding lungs. Additionally, in this
case, the dose was prescribed to cover 95% of the PTV using VMAT.
After this case, the prescription point was positioned on the
isocenter at our institution. In 2006, Hoyer et al (24) were the first to report SBRT for a
total of 64 metastases for up to three lesions per patient from
colorectal cancer, with a 2-year local control rate of 79%,
although serious side effects were reported in several cases. In
2008, Kim et al (25) carried
out SBRT of 36-51 Gy in three fractions using a cyberknife on 23
patients with pelvic LN metastases from rectal cancer, and reported
that the 4-year local PFS was 74.3%. A grade 4 rectal perforation
occurred in one case with 51 Gy. Casamassima et al (26) reported that only a Radiation Therapy
Oncology Group grade 1 side effect occurred after SBRT of 45 Gy in
six fractions for abdominal or pelvic LN metastases from prostate
cancer. Corvò et al (27)
treated 36 patients with SBRT of 35 Gy in five fractions per week.
Lesions were confined to the pelvis, hepatic portal section and
retroperitoneal space. Moderate to severe acute side effects did
not occur. In this study, brachial plexus palsy did not occur in
seven lesions for 7, 7, 8, 8, 14, 18 and 34 months, even if 50 Gy
of radiation was used in the supraclavicular region. The risk of
the occurrence of the palsy may be high, as only 1 patient could be
followed for >2 years.
Regarding the limitations of this study, first of
all, the number of cases investigated was small. In addition, this
was a retrospective study in which irradiation sites varied
spanning supraclavicular to pelvic regions. OM was proven
pathologically in only certain patients. Although a tendency to
increase the size and uptake of FDG in PET imaging was confirmed,
there may be the possibility of infection or other factors
affecting this. Furthermore, the primary tumors studied also
varied. Finally, 2 patients that received pre-chemotherapy prior to
SBRT and 1 patient with 3 OM lesions were also included.
SBRT of 50 Gy in 10 fractions for OM by various
primary tumors was demonstrated to be practical, with good clinical
outcomes from the standpoints of local control and frequency of
toxic side effects. However, additional studies are required in
order to identify patient groups that would receive maximum
benefits from this treatment.
Acknowledgements
The authors thank Miss Alisha Huang (Taipei European
School) for the English proofreading.
Funding
No funding was received.
Availability of data and materials
The datasets during and/or analyzed during the
current study available from the corresponding author on reasonable
request.
Authors' contributions
HY designed the study, and wrote the initial draft
of the manuscript. MO contributed to analysis and interpretation of
data, and assisted in the preparation of the manuscript. SA, OA,
and KN contributed to data collection and interpretation, and
critically reviewed the manuscript. All authors approved the final
version of the manuscript, and agree to be accountable for all
aspects of the work in ensuring that questions related to the
accuracy or integrity of any part of the work are appropriately
investigated and resolved.
Ethics approval and consent to
participate
Informed consent was obtained from all patients
prior to the procedures. Ethical approval was granted by the
Clinical Research Review Board of the University of Tokyo
Hospital.
Patient consent for publication
Not applicable.
Competing interests
All authors declare they have no competing
interests.
References
|
1
|
Ashworth A, Rodrigues G, Boldt G and Palma
D: Is there an oligometastatic state in non-small cell lung cancer?
A systematic review of the literature. Lung Cancer. 82:197–203.
2013.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Salah S, Tanvetyanon T and Abbasi S:
Metastatectomy for extra-cranial extra-adrenal non-small cell lung
cancer solitary metastases: Systematic review and analysis of
reported cases. Lung Cancer. 75:9–14. 2012.PubMed/NCBI View Article : Google Scholar
|
|
3
|
https://www.cancer.gov/publications/dictionaries/cancer-terms/def/oligometastasis.
|
|
4
|
Yano T, Haro A, Yoshida T, Morodomi Y, Ito
K, Shikada Y, Shoji F, Maruyama R and Maehara Y: Prognostic impact
of local treatment against postoperative oligometastases in
non-small cell lung cancer. J Surg Oncol. 102:852–855.
2010.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Alongi F, Arcangeli S, Filippi AR, Ricardi
U and Scorsetti M: Review and uses of stereotactic body radiation
therapy for oligometastases. Oncologist. 17:1100–1107.
2012.PubMed/NCBI View Article : Google Scholar
|
|
6
|
De Ruysscher D, Wanders R, van Baardwijk
A, Dingemans AM, Reymen B, Houben R, Bootsma G, Pitz C, van Eijsden
L, Geraedts W, et al: Radical treatment of non-small-cell lung
cancer patients with synchronous oligometastases: Long-term results
of a prospective phase II trial (Nct01282450). J Thorac Oncol.
7:1547–1555. 2012.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Griffioen GH, Toguri D, Dahele M, Warner
A, de Haan PF, Rodrigues GB, Slotman BJ, Yaremko BP, Senan S and
Palma DA: Radical treatment of synchronous oligometastatic
non-small cell lung carcinoma (NSCLC): Patient outcomes and
prognostic factors. Lung Cancer. 82:95–102. 2013.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Tree AC, Khoo VS, Eeles RA, Ahmed M,
Dearnaley DP, Hawkins MA, Huddart RA, Nutting CM, Ostler PJ and van
As NJ: Stereotactic body radiotherapy for oligometastases. Lancet
Oncol. 14:e28–e37. 2013.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Engels B, Gevaert T, Everaert H, De
Coninck P, Sermeus A, Christian N, Storme G, Verellen D and De
Ridder M: Phase II study of helical tomotherapy in the
multidisciplinary treatment of oligometastatic colorectal cancer.
Radiat Oncol. 7(34)2012.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Milano MT, Katz AW, Zhang H and Okunieff
P: Oligometastases treated with stereotactic body radiotherapy:
Long-term follow-up of prospective study. Int J Radiat Oncol Biol
Phys. 83:878–886. 2012.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Hasselle MD, Haraf DJ, Rusthoven KE,
Golden DW, Salgia R, Villaflor VM, Shah N, Hoffman PC, Chmura SJ,
Connell PP, et al: Hypofractionated image-guided radiation therapy
for patients with limited volume metastatic non-small cell lung
cancer. J Thorac Oncol. 7:379–381. 2012.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Choi CW, Cho CK, Yoo SY, Kim MS, Yang KM,
Yoo HJ, Seo YS, Kang JK, Lee DH, Lee KH, et al: Image-guided
stereotactic body radiation therapy in patients with isolated
para-aortic lymph node metastases from uterine cervical and corpus
cancer. Int J Radiat Oncol Biol Phys. 74:147–153. 2009.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Kim MS, Yoo SY, Cho CK, Yoo HJ, Yang KM,
Kang JK, Lee DH, Lee JI, Bang HY, Kim MS and Kang HJ: Stereotactic
body radiotherapy for isolated para-aortic lymph node recurrence
after curative resection in gastric cancer. J Korean Med Sci.
24:488–492. 2009.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Kim MS, Cho CK, Yang KM, Lee DH, Moon SM
and Shin YJ: Stereotactic body radiotherapy for isolated paraaortic
lymph node recurrence from colorectal cancer. World J
Gastroenterol. 15:6091–6095. 2009.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Hanna GG and Landau D: Stereotactic body
radiotherapy for oligometastatic disease. Clin Oncol (R Coll
Radiol). 27:290–297. 2015.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Duan Y, Li J, Zhang Y, Wang W, Sun X, Fan
T, Shao Q, Xu M, Guo Y and Shang D: Comparison of primary tumour
volumes delineated on four-dimensional computed tomography maximum
intensity projection and (18) F-fluorodeoxyglucose positron
emission tomography computed tomography images of non-small cell
lung cancer. J Med Imaging Radiat Oncol. 59:623–630.
2015.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Schag CC, Heinrich RL and Ganz PA:
Karnofsky performance status revisited: Reliability, validity, and
guidelines. J Clin Oncol. 2:187–193. 1984.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Trotti A, Colevas AD, Setser A, Rusch V,
Jaques D, Budach V, Langer C, Murphy B, Cumberlin R, Coleman CN and
Rubin P: CTCAE v3.0: Development of a comprehensive grading system
for the adverse effects of cancer treatment. Semin Radiat Oncol.
13:176–181. 2003.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Greene FL, Page DL, Fleming ID, Fritz AG,
Balch CM, Haller DG and Morrow M (eds): Esophagus. In: American
Joint Committee on Cancer (AJCC) cancer staging manual. 6th
edition. Springer, New York, NY, pp167-178, 2002.
|
|
20
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Pokhrel A, Dyba T and Hakulinen T: A
greenwood formula for standard error of the age-standardised
relative survival ratio. Eur J Cancer. 44:441–447. 2008.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Jereczek-Fossa BA, Beltramo G, Fariselli
L, Fodor C, Santoro L, Vavassori A, Zerini D, Gherardi F, Ascione
C, Bossi-Zanetti I, Mauro R, Bregantin A, Bianchi LC, De Cobelli O
and Orecchia R: Robotic image-guided stereotactic radiotherapy, for
isolated recurrent primary, lymph node or metastatic prostate
cancer. Int J Radiat Oncol Biol Phys. 82:889–897. 2012.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Milano MT, Katz AW, Schell MC, Philip A
and Okunieff P: Descriptive analysis of oligometastatic lesions
treated with curative-intent stereotactic body radiotherapy. Int J
Radiat Oncol Biol Phys. 72:1516–1522. 2008.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Hoyer M, Roed H, Traberg Hansen A, Ohluis
L, Petersen J, Nellemann H, Kiil Berthelsen A, Grau C, Aage
Engelholm S and Von der Maase H: Phase II study on stereotactic
body radiotherapy of colorectal metastases. Acta Oncol. 45:823–830.
2006.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Kim MS, Choi C, Yoo S, Cho C, Seo Y, Ji Y,
Lee D, Hwang D, Moon S, Kim MS and Kang H: Stereotactic body
radiation therapy in patients with pelvic recurrence from rectal
carcinoma. Jpn J Clin Oncol. 38:695–700. 2008.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Casamassima F, Masi L, Menichelli C,
Bonucci I, Casamassima E, Lazzeri M, Gulisano M and Aterini S:
Efficacy of eradicative radiotherapy for limited nodal metastases
detected with choline PET scan in prostate cancer patients. Tumori.
97:49–55. 2011.PubMed/NCBI
|
|
27
|
Corvò R, Lamanna G, Vagge S, Belgioia L,
Bosetti D, Aloi D, Timon G and Bacigalupo A: Once-weekly
stereotactic radiotherapy for patients with oligometastases:
Compliance and preliminary efficacy. Tumori. 99:159–163.
2013.PubMed/NCBI View Article : Google Scholar
|