Introduction
At present, it is estimated that 240 million people
globally are chronically infected with hepatitis B virus (HBV)
(1,2). In addition, patients with chronic HBV
infection are at increased risk of developing a progressive liver
disease, including fibrosis, cirrhosis or hepatocellular carcinoma
(HCC) (3).
Antiviral therapies are used for prevention of
clinical and histological progression of the disease, which is
achieved through long-term suppression of HBV replication. Among
these therapies, the nucleos(t)ide analogues (NAs) are the
treatment of choice (3). However,
the efficacy of antiviral therapy for chronic hepatitis B virus
(HBV) is impaired by emerging viral resistance (4,5). The
selection of antiviral-resistant mutations depends on viral
factors, such as the lack of a proofreading mechanisms during
reverse transcription, which creates a large pool of HBV
quasispecies that are better able to replicate due to their
increased resistance levels (6,7). In
addition, the available replication space in either the cytoplasm
or nucleus, and the structural flexibility of viral enzymes,
alongside host and drug factors including pretreatment serum
HBV-DNA level, quickness of viral suppression, duration of
treatment, compliance and prior exposure to NA therapies, are other
major factors involved in the development of resistance (6,7).
Among the approved NA therapies for HBV, lamivudine
(LVD), adefovir-dipivoxil and telbivudine (LdT) are associated with
the highest rate of drug resistance in NA-naïve patients, as these
offer a lower barrier to resistance exerting modest antiviral
activity that incompletely suppresses viral replication providing
the greatest opportunity for selecting drug-resistant virus,
whereas entecavir (ETV) and tenofovir (either TAF or TDF) are
associated with the lowest rate of drug resistance (5,6).
Resistance to nucleoside/nucleotide antivirals arises through
specific mutations in the HBV polymerase (pol) reverse
transcriptase (RT) domain (5). The
first cases of ETV resistance (ETVr) were observed in patients
receiving ETV after failure of LVD. In fact, resistance to ETV
appears to occur through a two-hit mechanism with primary LVD
resistance (LVDr) substitutions (M204V/I with/without rtL180M)
followed by amino acid substitutions at the rtI169, rtT184, rtS202
or rtM250 sites (5,6).
The requirement for three substitutions for ETVr,
combined with the potent suppression of HBV replication, results in
a high genetic barrier (due to a complete suppression of viral
replication) to ETV virological breakthrough in patients infected
with wild-type virus (8,9). Hence, ETV is a potent NA against HBV,
and emergence of drug resistance is rare in NA-naïve patients
(10-12).
However, cases of ETVr, which developed in nucleoside-naïve
patients, have been described in the literature (5,8,11-13).
The present report describes a NA-naïve patient with chronic HBV,
who experienced ETVr and viral rebound during ETV treatment, when
there was only one mutation present in the RT domain.
Case report
A 58-year-old Italian female patient underwent a
check-up in January 2014 and was found to be seropositive for
hepatitis B virus surface antigen (HBsAg) with elevated liver
enzymes (glutamic oxaloacetic transaminase, 100 IU/ml (Normal level
15-45 IU/ml); glutamic pyruvic transaminase, 180 IU/ml (normal
level 15-45 IU/ml)). HBeAb was positive and serum HBV-DNA was
2.7x107 IU/ml (measured by reverse transcription-PCR;
normal level, 0 IT/ml). Additional baseline characteristics of the
patient are presented in Table
I.
 | Table IBaseline characteristics of the female
patient diagnosed with hepatitis B virus in the present case
report. |
Table I
Baseline characteristics of the female
patient diagnosed with hepatitis B virus in the present case
report.
| Baseline
characteristic | Normal range | Patient value |
|---|
| Fasting blood
glucose, mg/dl | 70-99 | 105 |
| Creatinine,
mg/dl | 0.8-1.3 | 0.8 |
| AST, IU/ml | <40 | 100 |
| ALT, IU/ml | <40 | 180 |
| GGT, UI/l | 6-29 | 78 |
| Bilirubin total,
mg/dl | 0.3-1 | 0.4 |
| Bilirubin direct,
mg/dl | 0.1-0.3 | 0.2 |
| Albumin, g/dl | 3.5-5 | 4.37 |
| Hb, g/dl | 12-16 | 14.5 |
| RBC, x106
cells/mm3 | 4.10-5.10 | 4.56 |
| WBC, x103
cells/mm3 | 4.5-11 | 5.2 |
| PLT, x103
cells/mm3 | 150-450 | 150 |
| INR | 0.8-1.2 | 1 |
| Prothrombin time,
% | 80-100 | 96 |
| AFP, IU/ml | <7 | 4.2 |
| HBsAg | Negative | Positive |
| HBsAb | Negative | Negative |
| HBeAg | Negative | Negative |
| HBeAb | Negative | Positive |
| HBcAb | Negative | Positive |
| HCVAb | Negative | Negative |
| HIVAb | Negative | Negative |
| Anti-Δ | Negative | Negative |
Liver ultrasound revealed hepatomegaly with
steatosis pattern, and liver elastography showed a stiffness of
23.4 kPa (14) (normal value <5
kPa). However, there were no focal lesions. The patient refused to
undergo liver biopsy; therefore, only clinical diagnosis of
compensated cirrhosis was performed. The patient had a history of
diabetes, hypertension, hypercholesterolemia and depressive
disorder, and he was treated with amlodipine, bisoprolol,
simvastatin, reboxetine, quinapril, metformin and insulin. During
this period of treatments, the patient had not been diagnosed with
HBV and was naïve to antiHBV drugs. The patient had undergone
cholecystectomy 10 years prior to treat lithiasis. In addition, the
patient had no history of alcohol consumption, smoking, drug abuse
or blood transfusions, nor did they have unprotected sex or sex
with multiple partners. Family history was unremarkable and no
relatives had been found to be positive for HBV.
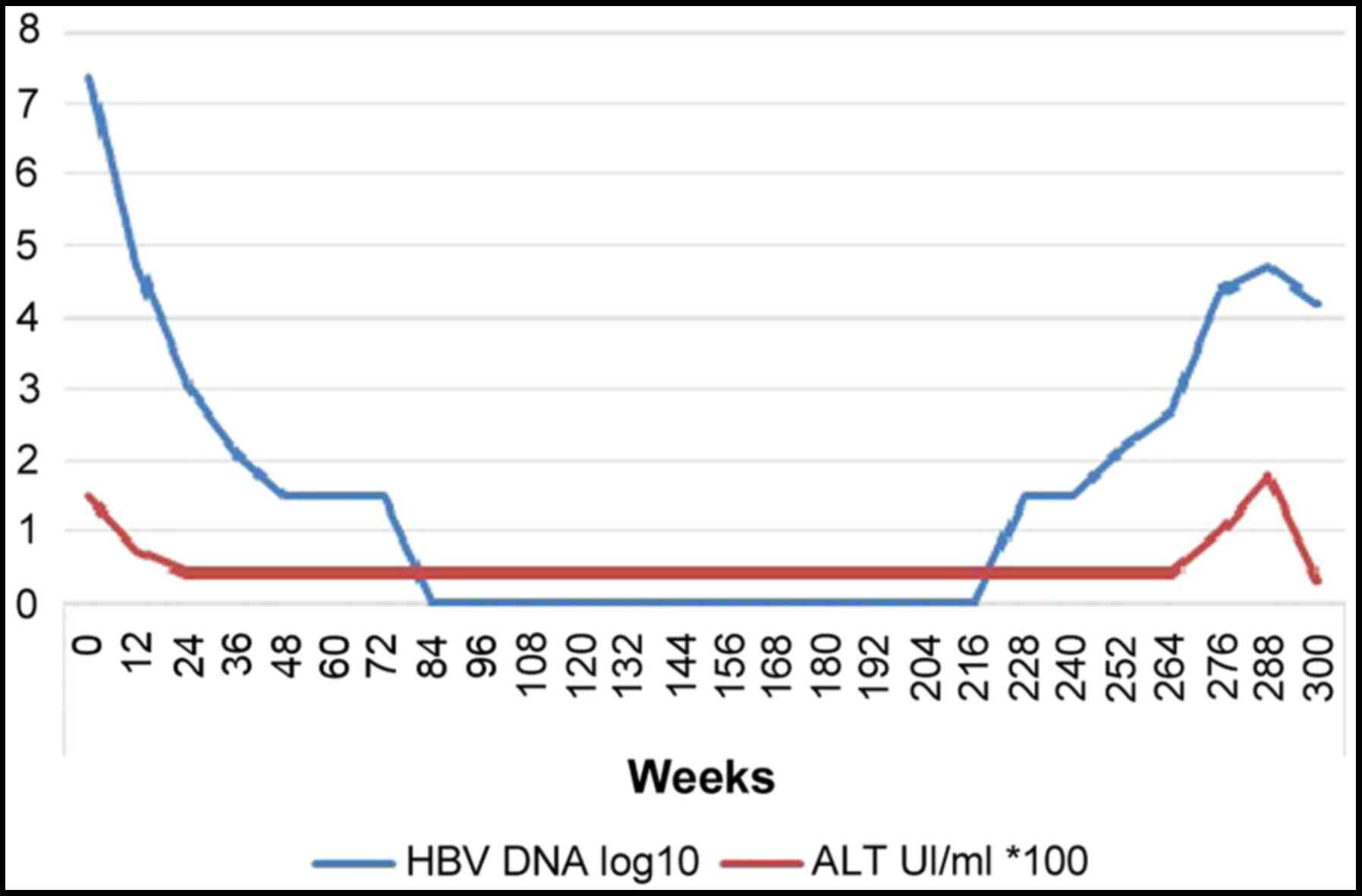
At that time of HBV diagnosis, treatment with ETV
started at 0.5 mg/day; drug-drug interactions were negative
(confirmed by Hepatic Drug Interactions Checker; University of
Liverpool, Liverpool, UK; https://www.hep-druginteractions.org). After the start
of ETV, serum HBV-DNA levels declined to a nadir point of 0 IU/ml
at week 85 of ETV treatment. HBV-DNA remained undetectable for 3
years. However, from September 2018 (week 228), serum HBV-DNA
started to rebound up to 52,500 IU/ml in September 2019 (week 288)
(Fig. 1). At the first stages (week
228) of this rebound, liver enzymes were normal, but gradually
started to increase along with HBV-DNA (Fig. 1). Other blood values (full blood
count, renal function and coagulation) were normal and the patient
denied any relevant symptoms, except for asthenia. Furthermore, the
patient guaranteed complete therapeutic adherence and strongly
denied the use of other non-prescribed medications. Ultrasonography
analysis did not reveal focal lesions.
Amplification of the HBV pol region was performed
for the analysis of HBV drug resistance (Sanger sequencing).
ETVr-related substitution M204I was detected, but no other
mutations were identified (Table
II). The patient discontinued ETV therapy at week 296, and then
received 245 mg/day of tenofovir disoproxil fumarate (TDF).
Afterwards, HBV-DNA levels dropped to 15,000 IU/ml in December 2019
and liver enzymes were normalized. The patient is currently
continuing a 3-month follow-up.
| Table IIMutations assessed in the hepatitis B
virus polymerase region of reverse transcriptase by Sanger
sequencing (performed by Abbott Hepatitis B virus Sequencing
assay). |
Table II
Mutations assessed in the hepatitis B
virus polymerase region of reverse transcriptase by Sanger
sequencing (performed by Abbott Hepatitis B virus Sequencing
assay).
| Mutation site | Mutation status |
|---|
| 80 | Absent |
| 84 | Absent |
| 85 | Absent |
| 169 | Absent |
| 173 | Absent |
| 180 | Absent |
| 181 | Absent |
| 184 | Absent |
| 194 | Absent |
| 202 | Absent |
| 204 | Present
(substitution M204I) |
| 214 | Absent |
| 215 | Absent |
| 217 | Absent |
| 219 | Absent |
| 221 | Absent |
| 233 | Absent |
| 236 | Absent |
| 250 | Absent |
Methods
All data were collected from patient's clinical
records, after informed consent. Biochemical and virological data
were collected from blood venipuncture in the contest of routine
blood sampling for clinical monitoring of patients treated with
anti-HBV antivirals, as suggested by guidelines (3). Sanger sequencing (performed by Abbott
HBV Sequencing assay) targets the polymerase (pol) region of the
HBV viral genome and detects both HBV genotype and drug
resistance.
Discussion
The treatment of chronic HBV infection has been
markedly improved in the last decade, primarily due to the
availability of oral NA antiviral agents, such as LdT, adefovir,
LVD, ETV and tenofovir (15). The
latest European Association for the Study of the Liver guidelines
(2017) recommend the use of TDF (or the new formulation tenofovir
alafenamide) or ETV in monotherapy as first line therapy, due to
their current lack of HBV resistance (3). These agents are very efficient at
inhibiting viral replication and are well tolerated by patients,
appearing to be safe with no relevant or acute side effects, to the
best of our knowledge and experience (3).
The major limitation of long-term antiviral therapy
for chronic HBV is the development of drug resistance, shown
initially as an increase in HBV-DNA level (virological
breakthrough) and then as an increase of liver enzymes (biochemical
breakthrough) (16). The mutations
conferring resistance to NA can be classified as either single-base
or multi-base mutations (17). To
date, TDF is the only oral antiviral with no evidence of
genotypical resistance development during monotherapy treatment in
chronic HBV-naïve patients for up to 8 years (17), and with no detectable resistance
mutations in treatment-experienced patients (15).
The substitution rtM204V/I in the
tyrosine/methionine/aspartate/aspartate (YMDD) motif of the pol
gene domain in HBV-DNA is the most common mutation linked to LVD
resistance (18), which was
observed at a rate of 14-32% after 1 year, and 60-70% after 5 years
of LVD treatment (6). In patients
infected with LVDr virus, the barrier to ETV is decreased as the
virus already contains two of the three substitutions conferring
resistance to ETV. These LVDr substitutions result in an 8-fold
reduction in HBV susceptibility to ETV (6). Furthermore, data in the literature
(18-22)
show that, among primary drug resistance mutations, M204I/V is the
most frequently encountered in treatment-naïve patients (23). In fact, a systematic review by Zhang
et al (24) revealed that
the global incidence of rtM204I/V/S is 4.85%.
Although the association between pre-existing RT
mutations and advanced liver diseases has not been fully
investigated, several types of HBV mutations in RT have previously
been reported to be associated with the progression of liver
diseases, such as cirrhosis and HCC (23). For example, Kim et al
(25), by comparing frequencies and
types of pre-existing RT mutations in treatment-naïve patients,
found a significantly higher rate of RT mutations in patients with
HCC compared with patients with chronic hepatitis, and also
identified three mutations that induced NA resistance (rtL80I,
rtN139K/T/H and rtM204I/V) and were significantly associated with
the progression of HCC.
Genotype C infection, HBeAg-negative status, and low
viral loads are significantly associated with higher frequencies
and prevalence rates of pre-existing HBV RT mutations (23). Higher frequencies of pre-existing RT
mutations were also generally associated, in addition to worse drug
treatment outcomes, with liver disease progression, including HCC
and cirrhosis. There were 8 mutations in the RT region, rtL80I,
rtD134N, rtN139K/T/H, rtY141F, rtM204I/V, rtF221Y, rtI224V and
rtM309K that were significantly associated with the progression of
HCC in treatment-naïve patients (23).
In the present case report, despite the presence of
only one RT substitution (rtM204I), the case showed both
genotypical and clinical resistance to ETV, requiring a therapeutic
switch to a higher barrier treatment, such as TDF. Analysis of HBV
resistance was not performed prior to treatment in the present
case, and thus, whether the baseline rtM204I substitution was
present before the treatment is not known.
To the best of our knowledge, the present report is
one of very few that describe emerging resistance to ETV in a
NA-naïve patient after complete viral suppression. Furthermore, the
presence of only the M204I substitution makes this case uncommon
and unique. Despite the low rate of viral mutations during ETV
treatment, NA-naïve patients should be cautiously monitored, even
more so than biochemically (GOT and GPT) and virologically
(HBV-DNA), for resistance even when complete HBV suppression is
achieved.
Acknowledgements
The authors would like to thank Dr Pietro Leanza,
Catania, Sicily, Italy for his help with English revisions.
Funding
Not applicable.
Availability of data and materials
Data sharing is not applicable to this article, as
no datasets were generated or analyzed during the current
study.
Authors' contributions
AM and FC contributed to study conception and
design. MC, VM, AP, DS acquired the data. FB, FDA and EVR were
involved in analysis and interpretation of data. GN, BMC and BC
critically revised the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patient for publication of this case report.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Schweitzer A, Horn J, Mikolajczyk RT,
Krause G and Ott JJ: Estimations of worldwide prevalence of chronic
hepatitis B virus infection: A systematic review of data published
between 1965 and 2013. Lancet. 386:1546–1555. 2015.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Ott JJ, Stevens GA, Groeger J and Wiersma
ST: Global epidemiology of hepatitis B virus infection: New
estimates of age-specific HBsAg seroprevalence and endemicity.
Vaccine. 30:2212–2219. 2012.PubMed/NCBI View Article : Google Scholar
|
|
3
|
European Association for the Study of the
Liver. Electronic address: simpleeasloffice@easloffice.eu;
European Association for the Study of the Live. EASL 2017 Clinical
Practice Guidelines on the management of hepatitis B virus
infection. J Hepatol. 67:370–398. 2017.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Baldick CJ, Eggers BJ, Fang J, Levine SM,
Pokornowski KA, Rose RE, Yu CF, Tenney DJ and Colonno RJ: Hepatitis
B virus quasispecies susceptibility to entecavir confirms the
relationship between genotypic resistance and patient virologic
response. J Hepatol. 48:895–902. 2008.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Doğan ÜB, Öztürk AB, Akın MS, Yalaki S and
Sayan M: A case of entecavir resistance which is developed after
complete viral suppression during entecavir treatment for
nucleoside-naïve chronic hepatitis B. Turk J Gastroenterol. 25
(Suppl 1):S206–S209. 2014.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Lok ASF and McMahon BJ: Chronic hepatitis
B: Update 2009. Hepatology. 50:661–662. 2009.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Bartholomeusz A and Locarnini SA:
Antiviral drug resistance: Clinical consequences and molecular
aspects. Semin Liver Dis. 26:162–170. 2006.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Zoulim F: Hepatitis B virus resistance to
entecavir in nucleotide naïve patients: Does it exist? Hepatology.
44:1404–1407. 2006.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Colonno RJ, Rose R, Baldick CJ, Levine S,
Pokornowski K, Yu CF, Walsh A, Fang J, Hsu M, Mazzucco C, et al:
Entecavir resistance is rare in nucleoside naïve patients with
hepatitis B. Hepatology. 44:1656–1665. 2006.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Tenney DJ, Rose RE, Baldick CJ,
Pokornowski KA, Eggers BJ, Fang J, Wichroski MJ, Xu D, Yang J,
Wilber RB and Colonno RJ: Long-term monitoring shows hepatitis B
virus resistance to entecavir in nucleoside-naïve patients is rare
through 5 years-of therapy. Hepatology. 49:1503–1514.
2009.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Suzuki F, Akuta N, Suzuki Y, Yatsuji H,
Sezaki H, Arase Y, Kawamura Y, Hosaka T, Kobayashi M, Ikeda K, et
al: Selection of a virus strain resistant to entecavir in a
nucleoside-naïve patient with hepatitis B of genotype H. J Clin
Virol. 39:149–152. 2007.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Lee HW, Kim HJ, Hong SP, Cha BK, Chang HY,
Choi CH, Do JH, Kim JG and Chang SK: Simultaneous emergence of
entecavir resistance mutations in a nucleoside-naïve chronic
hepatitis B patient. Intervirology. 55:380–384. 2012.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Kobashi H, Fujioka S, Kawaguchi M, Kumada
H, Yokosuka O, Hayashi N, Suzuki K, Okanoue T, Sata M, Tsubouchi H,
et al: Two cases of development of entecavir resistance during
entecavir treatment for nucleoside-naïve chronic hepatitis B.
Hepatol Int. 3:403–410. 2009.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Gherlan GS: Liver ultrasound elastography:
More than staging the disease. World J Hepatol. 7:1595–1600.
2015.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Cho WH, Lee HJ, Bang KB, Kim SB and Song
IH: Development of tenofovir disoproxil fumarate resistance after
complete viral suppression in a patient with treatment-naïve
chronic hepatitis B: A case report and review of the literature.
World J Gastroenterol. 24:1919–1924. 2018.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Hulgan T and Haas DW: Toward a
pharmacogenetic understanding of nucleotide and nucleoside analogue
toxicity. J Infect Dis. 194:1471–1474. 2006.PubMed/NCBI View
Article : Google Scholar
|
|
17
|
Liu Y, Corsa AC, Buti M, Cathcart AL,
Flaherty JF, Miller MD, Kitrinos KM, Marcellin P and Gane EJ: No
detectable resistance to tenofovir disoproxil fumarate in HBeAg+
and HBeAg-patients with chronic hepatitis B after 8 years of
treatment. J Viral Hepat. 24:68–74. 2017.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Lai CL, Chien RN, Leung NWY, Chang TT,
Guan R, Tai DI, Ng KY, Wu PC, Dent JC, Barber J, et al: A one-year
trial of lamivudine for chronic hepatitis B. Asia Hepatitis
Lamivudine Study Group. N Engl J Med. 339:61–68. 1998.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Kobayashi S, Ide T and Sata M: Detection
of YMDD motif mutations in some lamivudine-untreated asymptomatic
hepatitis B virus carriers. J Hepatol. 34:584–586. 2001.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Lee CZ, Lee HS, Huang GT, Yang PM and Sheu
JC: Detection of YMDD mutation using mutant-specific primers in
chronic hepatitis B patients before and after lamivudine treatment.
World J Gastroenterol. 12:5301–5355. 2006.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Tunçbilek S, Köse Ş, Elaldi A and Akman S:
Lamivudine resistance in untreated chronic hepatitis B patients in
Turkey. Turkish J Gastroenterol. 19:99–103. 2008.PubMed/NCBI
|
|
22
|
Huang CJ, Wu CF, Lan CY, Sung FY, Lin CL,
Liu CJ, Liu HF and Yu MW: Impact of Genetic Heterogeneity in
Polymerase of Hepatitis B virus on dynamics of viral load and
hepatitis B progression. PLoS One. 8(e70169)2013.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Choi YM, Lee SY and Kim BJ: Naturally
occurring hepatitis B virus reverse transcriptase mutations related
to potential antiviral drug resistance and liver disease
progression. World J Gastroenterol. 24:1708–1724. 2018.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Zhang Q, Liao Y, Cai B, Li Y, Li L, Zhang
J, An Y and Wang L: Incidence of natural resistance mutations in
naïve chronic hepatitis B patients: A systematic review and
meta-analysis. J Gastroenterol Hepatol. 30:252–261. 2015.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Kim JE, Lee SY, Kim H, Kim KJ, Choe WH and
Kim BJ: Naturally occurring mutations in the reverse transcriptase
region of hepatitis B virus polymerase from treatment-naïve Korean
patients infected with genotype C2. World J Gastroenterol.
23:4222–4232. 2017.PubMed/NCBI View Article : Google Scholar
|