1. Introduction
Mucins are a family of high-molecular weight
glycoproteins. In recent years, accumulating evidence has
demonstrated that mucins play an important role in the initiation
and progression of tumours (1).
Therefore, research on the members of the mucin family has become a
hot spot in the field of tumour immunotherapy. Among them, Mucin 1
(MUC1) is widely studied for its role in the pathogenesis of
various cancer types, and it is the most intensively studied
transmembrane protein of the mucin family. In general, abnormal
expression of the MUC1 oncogene is associated with the progression
of malignant tumours. For example, studies have found that the high
expression of MUC1 is associated with the survival and prognosis of
patients with lung, gastric, colorectal and pancreatic cancer
(2-4).
Thus, MUC1 is potentially a valid marker for the clinical diagnosis
of tumours and an important antigen for targeted therapy (5).
2. Distribution, structure and biological
characteristics of MUC1
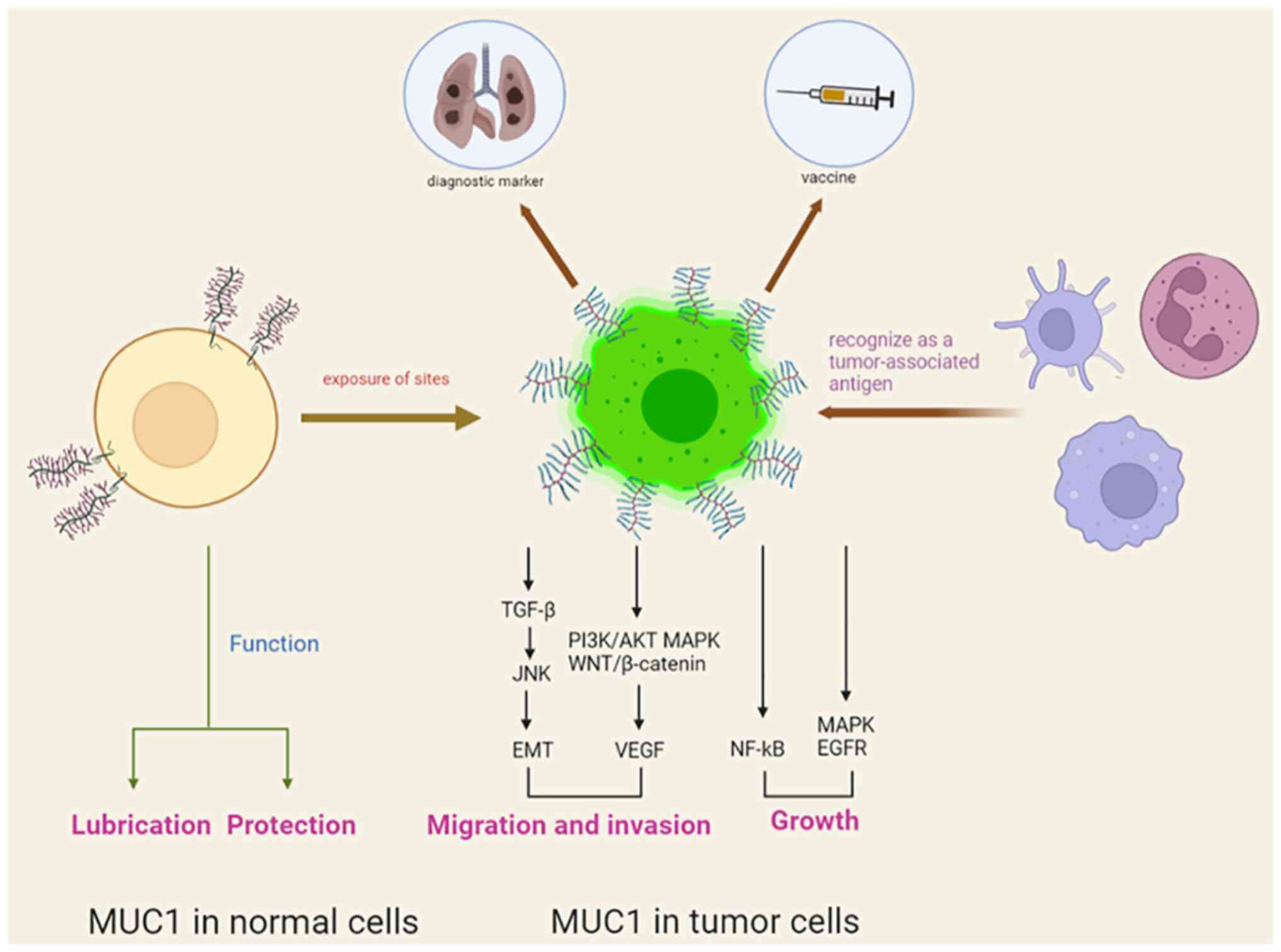
In healthy tissues, MUC1 is expressed on the
proximal luminal surface or proximal glandular surface of glandular
epithelial cells, and its expression is characterized by apical
expression, polar distribution and complete glycosylation. In
diseased tissues, the upregulation of MUC1 together with loss of
polarization and exposure of sites originally covered by glycan
chains leads to the recognition of MUC1 as a tumour-associated
antigen (TAA) by the immune system, indicating that it is a target
for immunotherapy (6,7).
MUC1 is a high-molecular weight transmembrane
glycoprotein, with a molecular weight of 300-600 kD, that is
composed of two subunits, including the extracellular
amino-terminal subunit (MUC1-N) and the transmembrane
carboxy-terminal subunit (MUC1-C) (8). These two subunits are linked by
non-covalent bonds to form a heterodimeric complex in the cell
membrane and can also be spontaneously hydrolysed into two
subunits. MUC1-N consists of 20-amino acid variable number tandem
repeats, which are rich in amino acid residues and can be highly
glycosylated. MUC1-C is a transmembrane subunit containing
extracellular, transmembrane and intracellular domains (9). The cytoplasmic tail of MUC1 (MUC1-CT)
consists of an extracellular domain of 58 amino acids, a
transmembrane domain of 28 amino acids and an intracellular domain
of 72 amino acids. MUC1-CT is highly conserved among different
species and plays an important role in numerous processes, such as
signal transduction and intercellular interactions (10).
MUC1 has a lubricating and protective function in
normal mucosal epithelial cells. However, upregulation of MUC1
promotes tumour progression by affecting multiple signalling
pathways, as well as by regulating the proliferation and epithelial
mesenchymal transition of tumourcells. Therefore, MUC1 is
considered a vital oncogene that regulates the developmental
processes of cancer. It has been shown that MUC1 promotes cell
growth and the proliferation of cancer by regulating PI3K/AKT,
MEK/ERK, p53, nuclear factor-κB, epidermal growth factor receptor,
WNT/β-catenin and JNK/TGF-β (3,11,12).
MUC1 also regulates tumour cell invasion and metastasis by
interacting with E-calmodulin and intercellular adhesion molecules
(13,14). In addition, MUC1 promotes tumour
angiogenesis and accelerates the invasion and metastasis of tumours
by stimulating the expression of proangiogenic factors, such as
vascular endothelial growth factor (4,15).
Taken together, these results show that the MUC1 oncogene plays an
important role in cancer development (Fig. 1).
3. MUC1 expression in different tumours and
its clinical significance
It has been reported that the MUC1 oncogene is
commonly overexpressed in various epithelial adenocarcinomas, such
as lung, liver, pancreatic, breast and ovarian cancer (10). The expression level of MUC1 in
different cancer types is a key factor for the application of MUC1
in clinical diagnosis and treatment. The present review assesses
the clinical significance of MUC1 by assembling cutting-edge data
about the expression of MUC1 in different tumours.
Expression of MUC1 in lung cancer
Lung cancer has become the most common cause of
cancer death worldwide. It has been reported that the mucin family,
especially MUC1, plays an important role in the progression of lung
cancer, and various vaccines for lung cancer targeting MUC1 are in
clinical trials (16,17).
Approximately 85% of patients with lung cancer have
the same histological subtype, namely, non-small cell lung cancer
(NSCLC) (18). MUC1 is apically
expressed and polar in normal tissues. However, in malignant
tumours, the distribution of MUC1 loses its polarity and shows
abnormal depolarization expression on the surface of the entire
tumour cell, which is often associated with a poor prognosis
(6,19). A clinical study reported that among
126 patients with non-small cell lung cancer, the 5-year survival
rates of patients in the MUC1 depolarized expression group
(percentage of tumour cells with depolarized MUC1 expression
>10%), the low-grade polarized expression group (polarized MUC1
expression <50% and depolarized MUC1 expression <10%) and the
high-grade polarized expression group (polarized MUC1 expression
>50% and depolarized MUC1 expression <10%) were 43.9, 61.5
and 79.4%, respectively (19).
These findings suggest that the depolarized expression of MUC1 in
tumour cells is significantly associated with poor outcome in
patients with lung cancer.
Lung adenocarcinoma and lung squamous cell carcinoma
are the most common types of NSCLC. In a previous study that
included 178 patients with stage IB NSCLC, the percentages of high
MUC1 expression in patients with lung adenocarcinoma and lung
squamous carcinoma were 86.3 and 39.1%, respectively (20). These findings suggest that MUC1
plays an important role in the progression of lung adenocarcinoma.
MUC1-Tn antigen is an oversimplified mucin-1 O-glycan that is
overexpressed in different cancer types. For example, the study
found that MUC1-Tn was abnormally expressed in breast, lung and
gastric cancer, among others, and may therefore be a target for
cancer diagnosis (21). Therefore,
the expression of MUC1-Tn in cancer tissues should be screened. In
a previous study, the results of immunohistochemical analysis of
175 lung adenocarcinoma tissues showed that high MUC1-Tn (MUC1
glycoconjugate antigen) expression was observed in 44 (25.1%)
specimens and was associated with patient sex (male patients,
33.3%; female patients, 17.6%), smoking history (ex-smoker, 31.8%;
non-smoker, 12.5%), tumour stage (T1a-c stage, 16.2%; T2a-b+T3+T4
stage, 40.6%) and pleural invasion (positive, 40%; negative, 20%)
(22). Another study suggested
that the abnormal expression of MUC1 was correlated with the poor
prognosis of patients with lung adenocarcinoma (23). Results indicate the potential
utility of MUC1 as a clinical diagnostic marker and therapeutic
target for lung adenocarcinoma through the contributing role in
pathological features, such as development and invasive metastasis
(24).
As it is difficult to obtain tumour tissues for
clinical analysis from patients with lung cancer who have
contraindications to surgery, blood markers are needed to predict
the degree of cancer disease progression and chemotherapy efficacy
in patients with advanced disease. It has been suggested that MUC1
can be used as a marker of circulating tumour cells (CTCs) in the
peripheral blood of patients with NSCLC (25). A previous study on 66 patients with
advanced NSCLC showed that MUC1 mRNA expression in the peripheral
blood of patients treated for 4 weeks (relative expression, 4.46)
was significantly lower than that in the patients before treatment
(relative expression, 5.95) (26).
In this previous study, the researchers also set 4.2 as the
threshold of positivity for MUC1 mRNA in the peripheral blood of
patients with NSCLC on the basis of the association between the
level of MUC1 mRNA and pathological features. According to this,
the positive expression of MUC1 in patients before and after 4
weeks of gefitinib treatment was 75.8% (50/66) and 45.5% (30/66),
respectively, and the follow-up revealed that the survival time of
MUC1-positive patients was significantly shorter than that of
MUC1-negative patients. These findings suggest that peripheral
blood MUC1 mRNA can be used to assess the therapeutic efficacy of
gefitinib for patients with NSCLC. Another study also found that
MUC1 could be used as a marker of CTCs in patients with NSCLC
(27). Therefore, MUC1 mRNA in
peripheral blood is expected to provide significant guidance for
adjusting treatment regimens for patients with advanced
disease.
Expression of MUC1 in breast
cancer
Breast cancer is the most common cancer in women.
The early diagnosis and treatment of patients with breast cancer is
often poor, as the pathogenesis of the disease is still not
clear.
Triple-negative breast cancer (TNBC) is a subtype of
breast tumour lacking oestrogen receptor, progesterone receptor and
human epidermal growth factor receptor 2 expression. TNBC is
difficult to treat and has a high mortality rate due to a lack of
therapeutic target molecules (28). A previous clinical study showed
that 49 out of 52 (94.2%) cancer tissues of patients with TNBC were
positive for MUC1 expression (29). These findings suggest that MUC1 is
an ideal target of tumour immunotherapy for TNBC. MUC1 promotes the
expression of programmed death ligand 1 in TNBC cells, resulting in
increased immune escape function and invasiveness of tumour cells
(30). MUC1has been suggested to
be a potential target to inhibit the development and progression of
TNBC (31).
In addition, MUC1 has great potential for the rapid
diagnosis of breast cancer. A previous clinical study showed that
the expression levels of serum and salivary IgG anti-MUC1 in
patients with breast cancer were higher than those in healthy women
(P<0.001) (32), suggesting
that the levels of autoantibodies against MUC1 in the serum and
saliva of patients with breast cancer may provide references in
cancer screening. Researchers have used quantitative (q)PCR to
detect the mRNA level of MUC1 in the blood from healthy volunteers
mixed with breast cancer cells (MCF-7) to simulate the CTCs of
breast cancer, which indicated that this method had a sensitivity
of detecting 1 CTC among 1x106-107 white
blood cells and a high specificity of 96.8% (detected 1
MUC1-positive individual among 30 healthy volunteers) (33). The qPCR method also found that
after the first cycle of chemotherapy, the treatment efficiency in
patients lacking MUC1 expression (60%; 6/10) was higher than that
in MUC1-positive patients (12.5%; 3/24) (33). These results suggest that MUC1 can
provide clinical significance in the diagnosis of CTCs and the
prediction of chemotherapy efficacy for patients with breast
cancer. Other studies have indicated that upregulation of the MUC1
gene is associated with a poor prognosis in patients with breast
cancer (34,35). MUC1 may also be a valid target for
predicting and improving the prognosis of patients.
Expression of MUC1 in ovarian
cancer
Ovarian cancer is one of the most lethal
gynaecological malignancies, and the prognosis of affected patients
is often poor due to its inconspicuous early symptoms and its
tendency to invade surrounding organs (36). The MUC1 oncogene is involved in the
progression, metastasis and drug resistance of ovarian cancer cells
(37).
The immunohistochemical results of a clinical study
revealed that all tumour specimens were MUC1-positive (19/19;
100%), with 47.4% (9/19) of these cases expressing high MUC1 levels
(+++) in more than one-half of the cancer tissues (positive
staining of cancer tissue >50%), and another 52.6% (10/19) of
these cases expressing very high MUC1 levels (++++) (38). Another study on 60 primary ovarian
cancer paraffin-embedded and sectioned tissue specimens showed that
the positive expression rate of MUC1 was 95.0% (57/60), and the
high expression rate of MUC1 was associated with tumour stage and
postoperative residual tumour tissue (39). It has been suggested that MUC1 is
involved in the progression of ovarian tumours and the poor
prognosis of patients. Therefore, the MUC1 gene has great potential
in the clinical diagnosis and treatment of patients with ovarian
cancer (40). The intracellular
segment of MUC1 (MUC1-CT) has also been reported as a potential
site for ovarian cancer immunotherapy (41).
Expression of MUC1 in
cholangiocarcinoma
The clinical outcome of patients with
cholangiocarcinoma is generally poor, as cholangiocarcinoma cells
are highly invasive and prone to lymph node and vascular metastasis
(42).
In a previous study, an immunohistochemical staining
analysis was performed to assay cancer tissues from 85 patients
with cholangiocarcinoma. The study reported that the positive
staining rate of MUC1 was 65.9% (56/85), and the positive
expression rate of MUC1 was associated with tumour differentiation
(poorly differentiated, 91%; moderately differentiated, 84%; highly
differentiated, 43%), tumour stage (T1 stage, 50%; ≥T2 stage, 80%),
neurological invasion (positive, 83%; negative, 57%) and patient
survival time (median survival time of MUC1-positive patients,
29.21 months; median survival time of MUC1-negative patients, 56.48
months) (43). The results of
another study showed that the positive immunohistochemical staining
rate of MUC1 in the cholangiocarcinoma tissues of 25 patients was
44% (11/25) (44). Thus, these
findings suggested that the upregulation of MUC1 plays an important
role in the progression of cholangiocarcinoma and is expected to be
a valid marker for the diagnosis of affected patients.
Cholangiocarcinoma can be divided into intrahepatic
cholangiocarcinoma and extrahepatic cholangiocarcinoma depending on
the site. One study showed that the positive expression rate of
MUC1 was 25, 57 and 80 in patients with three staging types of
intrahepatic cholangiocarcinoma, namely, intraductal, peri-biliary
infiltrative and mass type, respectively (43). These results suggest that the
abnormal expression of MUC1 has clinical value in the diagnosis of
intrahepatic cholangiocarcinoma of different stages. Survival
analysis of 61 patients with intrahepatic cholangiocarcinoma
revealed that the median survival time of the MUC1 low expression
group (qPCR: MUC1/GAPDH <0.056) was significantly higher (55.06
months) than that of the MUC1 high expression group (17.25 months);
the overall survival rates at 1, 3 and 5 years were 73, 57 and 45%,
respectively, for patients in the MUC1 low expression group,
whereas the overall survival rates for the same periods in the MUC1
high expression group were 35, 26 and 20%, respectively, with a
significantly higher recurrence rate in the MUC1 high expression
group (54.8%) than in the low expression group (30.0%) (45). Another study found that, in 50
tissues of mass-type intrahepatic cholangiocarcinoma, the positive
expression rate of MUC1 was 76.0% (38/50), and the abnormal
expression of MUC1 was a prognosis-related risk factor for the
disease (P=0.0011) (46). These
findings suggest that MUC1 is associated with a low survival time
and high recurrence rate in patients with intrahepatic
cholangiocarcinoma, which may be a valid predictor of prognostic
status for these patients.
Another study demonstrated that the positive
expression rate of MUC1 in the intraductal and peribiliary
infiltrative types of extrahepatic cholangiocarcinoma was 47 and
85% (P=0.006), respectively (43),
suggesting that MUC1 is also differentially expressed in different
stages of extrahepatic cholangiocarcinoma, which is expected to
assist in the diagnosis, prognosis prediction and treatment of
cholangiocarcinoma in clinical practice (47).
Expression of MUC1 in gallbladder
cancer
Gallbladder cancer has insidious symptoms in the
early stage and is prone to invade other surrounding organs;
therefore, patients are often in the middle and late stages when
they are diagnosed, resulting in poor treatment outcomes (48).
MUC1 has been found to be strongly positively
expressed in primary cancer cells derived from the ascites of
patients with gallbladder cancer (49). A study collected 629 specimens from
patients with gallbladder cancer for analysis, and the results
showed that the positive expression rate of MUC1 in gallbladder
cancer tissue specimens was 85.71% (18/21), which was significantly
higher than its expression level in 605 patients with
non-neoplastic gallbladder disease (5.29%; 32/605) (50).
Gallbladder adenocarcinoma is the most common type
of gallbladder cancer in clinical practice, accounting for 85% of
all gallbladder cancer cases. One study showed that the positive
expression of MUC1 in the cancerous tissues of 108 patients with
gallbladder adenocarcinoma (57.4%; 62/108) was significantly higher
than its expression in paraneoplastic tissues (21.7%; 10/46),
chronic cholecystitis (5.7%, 2/35) and adenomatous polyps (20.0%;
3/15) (51). These results suggest
that MUC1 has a high specificity and accuracy in the diagnosis of
gallbladder cancer, especially gallbladder adenocarcinoma, and that
it can be used as a marker for clinical diagnosis. Another study
also indicated that the positive expression rate of MUC1 was
correlated with tumour size (tumour maximum diameter <2 cm,
38.7%; maximum diameter ≥2 cm, 64.9%; P<0.05), tumour stage (T1
stage, 28.6%; T2 stage, 42.9%; T3 stage, 59.5%; T4 stage, 77.3%;
P<0.01) and lymph node metastasis (with lymph node metastasis,
69.5%; without metastasis, 42.9%; P<0.01) (51). These results further suggest that
the abnormal expression of MUC1 is involved in promoting the
progression and metastasis of gallbladder cancer, and that it may
be of clinical significance in the diagnosis and prediction of
clinical stage and metastasis for patients with gallbladder
cancer.
Expression of MUC1 in bladder
cancer
MUC1 plays a role in maintaining mucosal integrity
and inhibiting urinary bacterial invasion in the normal urinary
epithelium, and its abnormal expression is involved in promoting
the progression and metastasis of bladder cancer in cancerous
tissues (52).
A previous study showed that the positive expression
rate of MUC1 was 61.8% (333/539) in tissue specimens from patients
with bladder cancer, and its positive expression rate was
associated with patient sex (female, 24.3%; male, 75.7%; P=0.044)
and tumour pathological grade (high grade, 50.8%; low grade, 49.2%;
P=0.013) (53). A study on 97
bladder cancer tissue specimens found that the positive expression
rate of MUC1 was 89.7% (87/97); of these specimens, 57 had >50%
tumour cells positive for MUC1, indicating strong positive
expression of MUC1(54).
Similarly, another study found an increasing trend of MUC1
expression in normal bladder mucosa, benign bladder disease and
bladder tumours (55). It is
suggested that MUC1 is involved in the development and drug
resistance of bladder cancer (56). Thus, MUC1 may be an important
clinical marker and targeted therapeutic molecule due to its high
accuracy in the diagnosis of bladder cancer.
Expression of MUC1 in hepatocellular
carcinoma
Hepatocellular carcinoma is one of the most common
malignancies in clinical practice. The high aggressiveness and
recurrence rate of this disease are important reasons for the low
survival rate of patients (57).
One study showed that the positive expression rate
of MUC1 in 96 patients with primary hepatocellular carcinoma was
77.1% (74/96), 68 specimens of which had strong positive
immunohistochemical staining (++; positive cells >25%); MUC1 was
only weakly positively expressed (+; positive cells <25%) in
20.0% (4/20) of patients with cirrhosis and there was no MUC1
expression in 10 normal liver tissue samples (58). In the aforementioned specimens of
liver cancer, the positive expression rate of MUC1 was correlated
with the degree of tumour differentiation (positive expression rate
of MUC1: 53% highly differentiated, 85% moderately differentiated
and 92% hypofractionated; strong positive expression rate: 47%
highly differentiated, 80% moderately differentiated and 85%
hypofractionated) and lymph node metastasis (positive, 90%;
negative, 61%), suggesting that MUC1 is involved in the development
and metastasis of hepatocellular carcinoma.
Another study found that the positive expression
rate of MUC1 in 186 hepatocellular carcinoma specimens was 45.7%
(85/186), and its positive expression rate was correlated with
tumour differentiation (P=0.0001) and lymph node metastasis
(P=0.0419) (59). A similar study
showed that MUC1 was differentially expressed in hepatocellular
carcinoma and paraneoplastic tissues, and that its expression rate
was correlated with low patient survival rates (60). These findings suggest that MUC1 may
be a diagnostic marker and a potential therapeutic target for
hepatocellular carcinoma.
Expression of MUC1 in thyroid
cancer
A previous report showed that MUC1 was positively
expressed in 75.8% (219/289) of 289 patients with thyroid cancer,
which was significantly higher than its expression level in
non-malignant thyroid tissue (28/121; 23.1%) (61). Another study showed that the
positive expression of MUC1 was significantly higher in thyroid
cancer tissues (78.3%) than in paraneoplastic (24%) and normal
(10%) tissues, and that its expression was associated with tumour
stage (stage III+IV, 92.9%; stage I+II, 65.6%) and lymph node
metastasis (positive, 90.5%; negative, 50%) (62). A previous study also showed that
the positive expression rate of MUC1 in thyroid cancer was 77.6%,
and its expression was associated with peripheral tumour invasion
(P=0.035) and lymph node metastasis (P=0.013) (63). These results suggest that MUC1 is
involved in the development and metastatic invasion of thyroid
cancer, indicating that it is a potential specific marker for
clinical diagnosis.
Thyroid cancer is classified into papillary,
follicular, undifferentiated and medullary carcinoma (64). RT-PCR analysis revealed that the
expression of MUC1 in papillary thyroid cancer tissues was
significantly higher than that in follicular carcinoma (P<0.05)
(65), suggesting that there may
be variability in the expression of MUC1 in different types of
thyroid carcinoma. Additional clinical data are required to support
these findings.
Expression of MUC1 in colorectal
cancer
Colorectal cancer is one of the most common
malignancies in China, and is prone to occur in the sigmoid colon
and rectum. In recent years, a number of reports have confirmed
that MUC1 may be a dominant antigen for the diagnosis and targeted
therapy for colorectal cancer (66,67).
A previous study showed that the positive expression
rate of MUC1 was 55.6% (25/45) in the cancer tissues of 45 patients
with colorectal cancer, but that this rate was 0.0% in
paracancerous tissues (0/20); the expression rate in cancer tissues
was significantly correlated with lymph node metastasis (with
metastasis, 84.2%; without metastasis, 34.6%) (68). Another study reported that the
levels of MUC1 mRNA in colorectal cancer tissues were significantly
higher than those in normal tissues (P=0.004) (69). These results suggest that MUC1 is
involved in colorectal carcinogenesis and metastasis, indicating
that MUC1 has a high specificity and accuracy in the diagnosis and
prediction of colorectal cancer.
Another study showed that the positive expression
rate of MUC1 in 202 colorectal cancer specimens (43.6%; 88/202) was
significantly higher than its positive expression rate in 202
normal colorectal mucosa specimens (8.9%; 18/202), and the positive
expression rate of MUC1 showed a significant increasing trend in
tumour stages I (20%), II (35%), III (54%) and IV (60%) (P=0.006)
(70). In addition, the expression
rate of MUC1 was also associated with lymph node metastasis in
patients (N0, 31%; N1, 61%; N2, 47%; N3, 100%) (70). These studies suggest that the
abnormal expression of MUC1 is involved in the occurrence,
development and invasive metastasis of colorectal cancer (71), indicating that MUC1 may aid in the
clinical diagnosis of progression and postoperative metastasis. In
addition, MUC1 may also serve as a specific target for colorectal
cancer drugs or vaccines (72).
Expression of MUC1 in cervical
cancer
Cervical cancer is a malignant disease caused by
human papillomavirus infection, and it is divided into two main
histological types, namely, cervical adenocarcinoma and cervical
squamous carcinoma. The incidence of cervical adenocarcinoma is
higher than that of cervical squamous carcinoma and the prognosis
of patients with cervical adenocarcinoma is even worse than that of
patients with cervical squamous carcinoma (73).
Among 52 patients with cervical adenocarcinoma, a
study showed that the positive expression rate of MUC1 was 59.6%
(31/52), which was associated with cervical cancer stage (FIGO
stage 1a, 33%; FIGO stage 1b1, 50%; FIGO stage 1b2, 67%; FIGO stage
2a, 63%; FIGO stage 2b, 100%), lymph node metastasis (positive,
91%; negative, 51%) and ovarian metastasis (positive, 100%;
negative, 55%) (74). Thus, MUC1
is involved in the malignant process of cervical adenocarcinoma and
may be a target molecule for diagnosis and treatment.
As cervical cancer cells are prone to metastasis to
other organs (75), it is
important to detect early metastases of cervical cancer for
clinical treatment. qPCR analysis of 179 lymph nodes from 21
patients with primary cervical cancer revealed that the MUC1 mRNA
levels in lymph nodes with a positive histological diagnosis of
metastasis were significantly higher than those in lymph nodes with
negative histology (P<0.001); the specificity and sensitivity of
MUC1 for the diagnosis of cervical cancer lymph node metastasis was
78% (percentage of negative qPCR tests in 162 negative lymph nodes)
and 76% (percentage of positive qPCR tests in 17 positive lymph
nodes), respectively (76). These
results suggest that MUC1 level indicates lymph node metastasis in
cervical cancer and provides a reference for the extent of surgical
lymph node dissection.
Expression of MUC1 in pancreatic
cancer
Pancreatic cancer is one of the most rapidly
progressing malignancies with the worst prognosis. Most pancreatic
cancer patients have poor treatment outcomes due to missing the
optimal time for surgery (77).
A previous study showed that abnormal upregulation
of MUC1 can be detected in >60% of pancreatic cancer cases,
which correlates with the poor prognosis of the patients. It has
been suggested that MUC1 is involved in the development and
progression of pancreatic cancer, and that it may be an important
marker in the clinical diagnosis of the disease (78). In addition, the pro-cancer
mechanism of MUC1 may be associated with its promotion of glucose
metabolism in pancreatic cancer cells (79).
A previous study showed that among 101 patients with
pancreatic cancer, the median survival time of the patients in the
low MUC1 expression group (39.7 months) was significantly higher
than that of patients in the high MUC1 expression group (13.4
months) (80). These findings
indicated that MUC1 is associated with a poor prognosis and low
survival time in patients with pancreatic cancer, suggesting that
it may be an important target molecule to determine and improve the
prognosis of patients.
4. Progress and perspectives
In summary, the MUC1 oncogene is aberrantly
expressed in a variety of tumours, and its expression is mostly
associated with tumour progression (Table I). Therefore, MUC1 may play an
important role in the clinical diagnosis of tumours. Some
researchers have attempted to use radiolabelled MUC1 antibodies or
aptamers for targeted tumour imaging, which is expected to achieve
a rapid diagnosis with high specificity when used in combination
with traditional pathological biopsy methods (81). Studies have found that targeting
the MUC1 antigen can be used for the radiographic diagnosis of
breast cancer, which can be used to diagnose 90% of breast cancer
cases, including TNBC (82,83).
As CTCs also carry the MUC1 oncogene, the detection of MUC1 levels
in the peripheral blood can also be applied in the clinical
diagnosis of patients with cancer. The present review illustrates
that the level of MUC1 in the peripheral blood of patients with
NSCLC and breast cancer is associated with the treatment outcome
and prognosis of patients, and that it is expected to be widely
used in clinical practice in the future for the in vitro
diagnosis of cancer, for chemotherapy efficacy assessment, and for
postoperative recurrence and metastasis monitoring, due to its
advantages of being an easy and non-invasive sampling method
(26). Although, to the best of
our knowledge, there are few related reports to date, the level of
MUC1 mRNA in the patient serum is a significant reference for the
initial diagnosis of tumours (84).
 | Table IExpression of MUC1 in different
tumours. |
Table I
Expression of MUC1 in different
tumours.
| Cancer type | Positive expression
rate of MUC1, % (n/total n) (Ref.) | Positive expression
rate of MUC1 in patients with different stages, (%) (Ref.) | Overall survival
time, months |
|---|
| Lung
adenocarcinoma | 86.3 (44/51)
(20) | T1a-c, 16.2;
T2a-b+T3+T4, 40.6(22) | |
| Breast cancer | 94.2 (49/52)
(29) | | |
| Ovarian cancer | 100.0 (19/19)
(38); 95.0 (57/60) (39) | | |
|
Cholangiocarcinoma | 65.9 (56/85)
(43) | Poorly
differentiated, 91; moderately differentiated, 84; highly
differentiated, 43; T1, 50; ≥T2, 80(43) | MUC1 positive,
29.21; MUC1 negative, 56.48(43) |
| Gallbladder
carcinoma | 57.4 (62/108)
(51) | T1, 28.6; T2, 42.9;
T3, 59.5; T4, 77.3(51) | |
| Liver cancer | 77.1 (74/96)
(58) | Poorly
differentiated, 92; moderately differentiated, 85; highly
differentiated, 53(58) | |
| Thyroid
carcinoma | 78.3 (47/60)
(62) | I+II, 65.6; III+IV,
92.9(62) | |
| Colorectal
cancer | 43.6 (88/202)
(70) | I, 20; II, 35; III,
54; IV, 60(70) | |
| Cervical
carcinoma | 59.6 (31/52)
(74) | FIGO 1a, 33; FIGO
1b1, 50; FIGO 1b2, 67; FIGO 2a, 63; FIGO 2b, 100(74) | |
In tumour immunotherapy, the exposed glycosylation
sites can be recognized by the immune system as TAAs. Therefore,
MUC1 has been an important target for tumour vaccine design and
development in recent years. Tumour vaccines based on MUC1
effectively prevent cancer progression and metastasis. At present,
MUC1-based tumour vaccines mainly include DNA vaccines, dendritic
cell (DC) vaccines, virus vaccines and subunit vaccines. A variety
of MUC1 DNA vaccines have been developed to date. Studies have
confirmed that the MUC1 DNA vaccine induces a specific immune
response against MUC1, produces an obvious tumour suppression
effect and prolongs patient survival time (85-87).
In phase I/II clinical trials, MUC1-loaded DC vaccines in the
combination therapy of patients with advanced pancreatic cancer
enhanced the disease suppression rate and effectively extended the
survival period (88,89). TG4010, which is a viral vaccine
expressing MUC1 has attracted much attention in recent years. In a
phase II clinical trial, the vaccine extended the survival period
of patients with NSCLC and no serious adverse reactions were found.
At present, TG4010 has entered phase III clinical trials and is
expected to enhance the efficacy of radiotherapy and chemotherapy
for patients with cancer (16,90).
Studies have confirmed that MUC1 subunit vaccines enhance specific
immune responses, and these vaccines are expected to enter clinical
trials in the future (91,92). In addition, studies have confirmed
that chimeric antigen receptor-T cells targeting MUC1 have good
antitumour function in tumour models in vivo and in
vitro, which may provide new strategies for tumour treatment
(93-95).
Although MUC1-based tumour vaccines have not been successfully
applied to clinical treatment at present, MUC1 has great potential
in tumour treatment. In the process of vaccine development, it is
very important to design vaccines according to the expression
characteristics of MUC1 in different tumor tissues. In addition,
the safety and effectiveness of tumour vaccines still need to be
further verified, especially for patients with advanced cancer
whose T-cell functions are severely damaged. MUC1 is expected to
generate new hope for the clinical diagnosis and treatment of a
number of tumors in the near future.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
Not applicable.
Authors' contributions
YL drafted the initial manuscript, and edited and
critically revised the manuscript. WN contributed substantially in
drafting the manuscript, and in editing and critically revising the
manuscript for intellectual content. GT put forward the concept,
critically revised the article for intellectual content, and was
responsible for the organization, revision and submission of the
manuscript. All authors have read and approved the final
manuscript. Data authentication is not applicable.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Wi DH, Cha JH and Jung YS: Mucin in
cancer: A stealth cloak for cancer cells. BMB Rep. 54:344–355.
2021.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Xu F, Liu F, Zhao H, An G and Feng G:
Prognostic significance of mucin antigen MUC1 in various human
epithelial cancers: A meta-analysis. Medicine (Baltimore).
94(e2286)2015.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Bose M, Grover P, Sanders AJ, Zhou R,
Ahmad M, Shwartz S, Lala P, Nath S, Yazdanifar M, Brouwer C and
Mukherjee P: Overexpression of MUC1 induces non-canonical TGF-β
signaling in pancreatic ductal adenocarcinoma. Front Cell Dev Biol.
10(821875)2022.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Khodabakhsh F, Merikhian P, Eisavand MR
and Farahmand L: Crosstalk between MUC1 and VEGF in angiogenesis
and metastasis: A review highlighting roles of the MUC1 with an
emphasis on metastatic and angiogenic signaling. Cancer Cell Int.
21(200)2021.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Supruniuk K and Radziejewska I: MUC1 is an
oncoprotein with a significant role in apoptosis (Review). Int J
Oncol. 59(68)2021.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Chen W, Zhang Z, Zhang S, Zhu P, Ko JK and
Yung KK: MUC1: Structure, function, and clinic application in
epithelial cancers. Int J Mol Sci. 22(6567)2021.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Beatty PL and Finn OJ: Preventing cancer
by targeting abnormally expressed self-antigens: MUC1 vaccines for
prevention of epithelial adenocarcinomas. Ann N Y Acad Sci.
1284:52–56. 2013.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Guo M, You C and Dou J: Role of
transmembrane glycoprotein mucin 1 (MUC1) in various types of
colorectal cancer and therapies: Current research status and
updates. Biomed Pharmacother. 107:1318–1325. 2018.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Cascio S and Finn OJ: Intra- and
extra-cellular events related to altered glycosylation of MUC1
promote chronic inflammation, tumor progression, invasion, and
metastasis. Biomolecules. 6(39)2016.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Gao T, Cen Q and Lei H: A review on
development of MUC1-based cancer vaccine. Biomed Pharmacother.
132(110888)2020.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Li W, Han Y, Sun C, Li X, Zheng J, Che J,
Yao X and Kufe D: Novel insights into the roles and therapeutic
implications of MUC1 oncoprotein via regulating proteins and
non-coding RNAs in cancer. Theranostics. 12:999–1011.
2022.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Hagiwara M, Fushimi A, Bhattacharya A,
Yamashita N, Morimoto Y, Oya M, Withers HG, Hu Q, Liu T, Liu S, et
al: MUC1-C integrates type II interferon and chromatin remodeling
pathways in immunosuppression of prostate cancer. Oncoimmunology.
11(2029298)2022.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Yasumizu Y, Rajabi H, Jin C, Hata T,
Pitroda S, Long MD, Hagiwara M, Li W, Hu Q, Liu S, et al: MUC1-C
regulates lineage plasticity driving progression to neuroendocrine
prostate cancer. Nat Commun. 11(338)2020.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Hosseinzadeh A, Merikhian P, Naseri N,
Eisavand MR and Farahmand L: MUC1 is a potential target to overcome
trastuzumab resistance in breast cancer therapy. Cancer Cell Int.
22(110)2022.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Utispan K and Koontongkaew S: Mucin 1
regulates the hypoxia response in head and neck cancer cells. J
Pharmacol Sci. 147:331–339. 2021.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Quoix E, Lena H, Losonczy G, Forget F,
Chouaid C, Papai Z, Gervais R, Ottensmeier C, Szczesna A,
Kazarnowicz A, et al: TG4010 immunotherapy and first-line
chemotherapy for advanced non-small-cell lung cancer (TIME):
Results from the phase 2b part of a randomised, double-blind,
placebo-controlled, phase 2b/3 trial. Lancet Oncol. 17:212–223.
2016.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Ning Y, Zheng H, Zhan Y, Liu S, Yang Y,
Zang H, Luo J, Wen Q and Fan S: Comprehensive analysis of the
mechanism and treatment significance of Mucins in lung cancer. J
Exp Clin Cancer Res. 39(162)2020.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Kwan TY and Chowdhury EH: Clinical
outcomes of chemotherapeutic molecules as single and multiple
agents in advanced non-small-cell lung carcinoma (NSCLC) patients.
Medicina (Kaunas). 57(1252)2021.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Kaira K, Nakagawa K, Ohde Y, Okumura T,
Takahashi T, Murakami H, Endo M, Kondo H, Nakajima T and Yamamoto
N: Depolarized MUC1 expression is closely associated with hypoxic
markers and poor outcome in resected non-small cell lung cancer.
Int J Surg Pathol. 20:223–232. 2012.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Situ D, Wang J, Ma Y, Zhu Z, Hu Y, Long H
and Rong T: Expression and prognostic relevance of MUC1 in stage IB
non-small cell lung cancer. Med Oncol. 28 (Suppl 1):S596–S604.
2011.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Palladino P, Papi F, Minunni M, Nativi C
and Scarano S: Structurally constrained MUC1-tn mimetic antigen as
template for molecularly imprinted polymers (MIPs): A promising
tool for cancer diagnostics. Chempluschem.
87(e202200068)2022.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Kato T, Ujiie H, Hatanaka KC, Nange A,
Okumura A, Tsubame K, Naruchi K, Sato M, Kaga K, Matsuno Y, et al:
A novel Tn antigen epitope-recognizing antibody for MUC1 predicts
clinical outcome in patients with primary lung adenocarcinoma.
Oncol Lett. 21(202)2021.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Xie Q, Zhao S, Liu W, Cui Y, Li F, Li Z,
Guo T, Yu W, Guo W, Deng W and Gu C: YBX1 enhances metastasis and
stemness by transcriptionally regulating MUC1 in lung
adenocarcinoma. Front Oncol. 11(702491)2021.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Liu S, Zhang X, Jiang Q and Liang T:
Detection of circulating natural antibodies against CD25, MUC1, and
VEGFR1 for early diagnosis of non-small cell lung cancer. FEBS Open
Bio. 10:1288–1294. 2020.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Warawdekar UM, Sirajuddin MM, Pramesh CS
and Mistry RC: An approach of selecting appropriate markers from
the primary tumor to enable detection of circulating tumor cells in
patients with non-small cell lung cancer. J BUON. 20:782–790.
2015.PubMed/NCBI
|
|
26
|
Li J, Hu YM, Du YJ, Zhu LR, Qian H, Wu Y
and Shi WL: Expressions of MUC1 and vascular endothelial growth
factor mRNA in blood are biomarkers for predicting efficacy of
gefitinib treatment in non-small cell lung cancer. BMC Cancer.
14(848)2014.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Savarese-Brenner B, Heugl M, Rath B,
Schweizer C, Obermayr E, Stickler S and Hamilton G: MUC1 and CD147
are promising markers for the detection of circulating tumor cells
in small cell lung cancer. Anticancer Res. 42:429–439.
2022.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Borri F and Granaglia A: Pathology of
triple negative breast cancer. Semin Cancer Biol. 72:136–145.
2021.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Siroy A, Abdul-Karim FW, Miedler J, Fong
N, Fu P, Gilmore H and Baar J: MUC1 is expressed at high frequency
in early-stage basal-like triple-negative breast cancer. Hum
Pathol. 44:2159–2166. 2013.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Maeda T, Hiraki M, Jin C, Rajabi H, Tagde
A, Alam M, Bouillez A, Hu X, Suzuki Y, Miyo M, et al: MUC1-C
induces PD-L1 and immune evasion in triple-negative breast cancer.
Cancer Res. 78:205–215. 2018.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Yamashita N, Long M, Fushimi A, Yamamoto
M, Hata T, Hagiwara M, Bhattacharya A, Hu Q, Wong KK, Liu S and
Kufe D: MUC1-C integrates activation of the IFN-gamma pathway with
suppression of the tumor immune microenvironment in triple-negative
breast cancer. J Immunother Cancer. 9(e002115)2021.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Laidi F, Bouziane A, Errachid A and Zaoui
F: Usefulness of salivary and serum auto-antibodies against tumor
biomarkers HER2 and MUC1 in breast cancer screening. Asian Pac J
Cancer Prev. 17:335–339. 2016.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Cheng JP, Yan Y, Wang XY, Lu YL, Yuan YH,
Jia J and Ren J: MUC1-positive circulating tumor cells and MUC1
protein predict chemotherapeutic efficacy in the treatment of
metastatic breast cancer. Chin J Cancer. 30:54–61. 2011.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Jing X, Liang H, Hao C, Yang X and Cui X:
Overexpression of MUC1 predicts poor prognosis in patients with
breast cancer. Oncol Rep. 41:801–810. 2019.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Li J, Liu L, Feng Z, Wang X, Huang Y, Dai
H, Zhang L, Song F, Wang D, Zhang P, et al: Tumor markers CA15-3,
CA125, CEA and breast cancer survival by molecular subtype: A
cohort study. Breast Cancer. 27:621–630. 2020.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Gaitskell K, Hermon C, Barnes I, Pirie K,
Floud S, Green J, Beral V and Reeves GK: Million Women Study
Collaborators. Ovarian cancer survival by stage, histotype, and
pre-diagnostic lifestyle factors, in the prospective UK million
women study. Cancer Epidemiol. 76(102074)2022.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Ma Q, Song J, Wang S and He N: MUC1
regulates AKT signaling pathway by upregulating EGFR expression in
ovarian cancer cells. Pathol Res Pract. 224(153509)2021.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Budiu RA, Mantia-Smaldone G, Elishaev E,
Chu T, Thaller J, McCabe K, Lenzner D, Edwards RP and Vlad AM:
Soluble MUC1 and serum MUC1-specific antibodies are potential
prognostic biomarkers for platinum-resistant ovarian cancer. Cancer
Immunol Immunother. 60:975–984. 2011.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Wang L, Ma J, Liu F, Yu Q, Chu G, Perkins
AC and Li Y: Expression of MUC1 in primary and metastatic human
epithelial ovarian cancer and its therapeutic significance. Gynecol
Oncol. 105:695–702. 2007.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Barani M, Bilal M, Sabir F, Rahdar A and
Kyzas GZ: Nanotechnology in ovarian cancer: Diagnosis and
treatment. Life Sci. 266(118914)2021.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Hu XF, Yang E, Li J and Xing PX: MUC1
cytoplasmic tail: A potential therapeutic target for ovarian
carcinoma. Expert Rev Anticancer Ther. 6:1261–1271. 2006.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Elvevi A, Laffusa A, Scaravaglio M, Rossi
RE, Longarini R, Stagno AM, Cristoferi L, Ciaccio A, Cortinovis DL,
Invernizzi P and Massironi S: Clinical treatment of
cholangiocarcinoma: An updated comprehensive review. Ann Hepatol.
27(100737)2022.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Park SY, Roh SJ, Kim YN, Kim SZ, Park HS,
Jang KY, Chung MJ, Kang MJ, Lee DG and Moon WS: Expression of MUC1,
MUC2, MUC5AC and MUC6 in cholangiocarcinoma: Prognostic impact.
Oncol Rep. 22:649–657. 2009.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Mall AS, Tyler MG, Ho SB, Krige JEJ, Kahn
D, Spearman W, Myer L and Govender D: The expression of MUC mucin
in cholangiocarcinoma. Pathol Res Pract. 206:805–809.
2010.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Chen FY, Zhou C, Zhang XY, Zhou KQ, Peng
YF, Yu L, Fan J, Zhou J, Hu J and Wang Z: Integrated Bioinformatics
analysis and clinical validation reveals that high expression of
mucin 1 in intrahepatic cholangiocarcinoma predicts recurrence
after curative resection. Exp Ther Med. 20(50)2020.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Matsumura N, Yamamoto M, Aruga A, Takasaki
K and Nakano M: Correlation between expression of MUC1 core protein
and outcome after surgery in mass-forming intrahepatic
cholangiocarcinoma. Cancer. 94:1770–1776. 2002.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Supimon K, Sangsuwannukul T, Sujjitjoon J,
Phanthaphol N, Chieochansin T, Poungvarin N, Wongkham S, Junking M
and Yenchitsomanus PT: Anti-mucin 1 chimeric antigen receptor T
cells for adoptive T cell therapy of cholangiocarcinoma. Sci Rep.
11(6276)2021.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Bosch DE, Salipante SJ, Schmidt RA,
Swanson PE, Bryan A, SenGupta DJ, Truong CD and Yeh MM:
Neutrophilic inflammation in gallbladder carcinoma correlates with
patient survival: A case-control study. Ann Diagn Pathol.
56(151845)2022.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Garcia P, Bizama C, Rosa L, Espinoza JA,
Weber H, Cerda-Infante J, Sánchez M, Montecinos VP, Lorenzo-Bermejo
J, Boekstegers F, et al: Functional and genomic characterization of
three novel cell lines derived from a metastatic gallbladder cancer
tumor. Biol Res. 53(13)2020.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Bhoge A, Khandeparkar SGS, Joshi AR,
Gogate B, Kulkarni MM and Bhayekar P: Immunohistochemical study of
MUC1 and MUC5AC expression in gall bladder lesions. J Clin Diagn
Res. 11:EC12–EC16. 2017.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Xiong L, Yang Z, Yang L, Liu J and Miao X:
Expressive levels of MUC1 and MUC5AC and their clinicopathologic
significances in the benign and malignant lesions of gallbladder. J
Surg Oncol. 105:97–103. 2012.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Kaur S, Momi N, Chakraborty S, Wagner DG,
Horn AJ, Lele SM, Theodorescu D and Batra SK: Altered expression of
transmembrane mucins, MUC1 and MUC4, in bladder cancer:
Pathological implications in diagnosis. PLoS One.
9(e92742)2014.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Stojnev S, Ristic-Petrovic A, Velickovic
LJ, Krstic M, Bogdanovic D, Khanh DT, Ristic A, Conic I and
Stefanovic V: Prognostic significance of mucin expression in
urothelial bladder cancer. Int J Clin Exp Pathol. 7:4945–4958.
2014.PubMed/NCBI
|
|
54
|
Gonul II, Cakir A and Sozen S:
Immunohistochemical expression profiles of MUC1 and MUC2 mucins in
urothelial tumors of bladder. Indian J Pathol Microbiol.
61:350–355. 2018.PubMed/NCBI View Article : Google Scholar
|
|
55
|
Tao TT, Chen J, Hu Q, Huang XZ, Fu J, Lv
BD and Duan Y: Urothelial carcinoma of the bladder with abundant
myxoid stroma: A case report and literature review. Medicine
(Baltimore). 99(e21204)2020.PubMed/NCBI View Article : Google Scholar
|
|
56
|
Shigeta K, Hasegawa M, Kikuchi E, Yasumizu
Y, Kosaka T, Mizuno R, Mikami S, Miyajima A, Kufe D and Oya M: Role
of the MUC1-C oncoprotein in the acquisition of cisplatin
resistance by urothelial carcinoma. Cancer Sci. 111:3639–3652.
2020.PubMed/NCBI View Article : Google Scholar
|
|
57
|
Anwanwan D, Singh SK, Singh S, Saikam V
and Singh R: Challenges in liver cancer and possible treatment
approaches. Biochim Biophys Acta Rev Cancer.
1873(188314)2020.PubMed/NCBI View Article : Google Scholar
|
|
58
|
Yuan SF, Li KZ, Wang L, Dou KF, Yan Z, Han
W and Zhang YQ: Expression of MUC1 and its significance in
hepatocellular and cholangiocarcinoma tissue. World J
Gastroenterol. 11:4661–4666. 2005.PubMed/NCBI View Article : Google Scholar
|
|
59
|
Ichikawa T, Yamamoto T, Uenishi T, Tanaka
H, Takemura S, Ogawa M, Tanaka S, Suehiro S, Hirohashi K and Kubo
S: Clinicopathological implications of immunohistochemically
demonstrated mucin core protein expression in hepatocellular
carcinoma. J Hepatobiliary Pancreat Surg. 13:245–251.
2006.PubMed/NCBI View Article : Google Scholar
|
|
60
|
Jiang QL, Feng SJ, Yang ZY, Xu Q and Wang
SZ: CircHECTD1 up-regulates mucin 1 expression to accelerate
hepatocellular carcinoma development by targeting microRNA-485-5p
via a competing endogenous RNA mechanism. Chin Med J (Engl).
133:1774–1785. 2020.PubMed/NCBI View Article : Google Scholar
|
|
61
|
Morari EC, Silva JR, Guilhen AC, Cunha LL,
Marcello MA, Soares FA, Vassallo J and Ward LS: Muc-1 expression
may help characterize thyroid nodules but does not predict
patients' outcome. Endocr Pathol. 21:242–249. 2010.PubMed/NCBI View Article : Google Scholar
|
|
62
|
Zhan XX, Zhao B, Diao C, Cao Y and Cheng
RC: Expression of MUC1 and CD176 (Thomsen-Friedenreich antigen) in
papillary thyroid carcinomas. Endocr Pathol. 26:21–26.
2015.PubMed/NCBI View Article : Google Scholar
|
|
63
|
Hu YJ, Luo XY, Yang Y, Chen CY, Zhang ZY
and Guo X: Characterization and significance of MUC1 and c-myc
expression in elderly patients with papillary thyroid carcinoma.
Genet Mol Res. 14:15325–15330. 2015.PubMed/NCBI View Article : Google Scholar
|
|
64
|
Baloch ZW, Asa SL, Barletta JA, Ghossein
RA, Juhlin CC, Jung CK, LiVolsi VA, Papotti MG, Sobrinho-Simões M,
Tallini G and Mete O: Overview of the 2022 WHO classification of
thyroid neoplasms. Endocr Pathol. 33:27–63. 2022.PubMed/NCBI View Article : Google Scholar
|
|
65
|
Baek SK, Woo JS, Kwon SY, Lee SH, Chae YS
and Jung KY: Prognostic significance of the MUC1 and MUC4
expressions in thyroid papillary carcinoma. Laryngoscope.
117:911–916. 2007.PubMed/NCBI View Article : Google Scholar
|
|
66
|
Guo M, Luo B, Pan M, Li M, Xu H, Zhao F
and Dou J: Colorectal cancer stem cell vaccine with high expression
of MUC1 serves as a novel prophylactic vaccine for colorectal
cancer. Int Immunopharmacol. 88(106850)2020.PubMed/NCBI View Article : Google Scholar
|
|
67
|
Guo M, You C, Dong W, Luo B, Wu Y, Chen Y,
Li J, Pan M, Li M, Zhao F and Dou J: The surface dominant antigen
MUC1 is required for colorectal cancer stem cell vaccine to exert
anti-tumor efficacy. Biomed Pharmacother.
132(110804)2020.PubMed/NCBI View Article : Google Scholar
|
|
68
|
Wang HS and Wang LH: The expression and
significance of Gal-3 and MUC1 in colorectal cancer and colon
cancer. Onco Targets Ther. 8:1893–1898. 2015.PubMed/NCBI View Article : Google Scholar
|
|
69
|
Kasprzak A, Siodla E, Andrzejewska M,
Szmeja J, Seraszek-Jaros A, Cofta S and Szaflarski W: Differential
expression of mucin 1 and mucin 2 in colorectal cancer. World J
Gastroenterol. 24:4164–4177. 2018.PubMed/NCBI View Article : Google Scholar
|
|
70
|
Hazgui M, Weslati M, Boughriba R, Ounissi
D, Bacha D and Bouraoui S: MUC1 and MUC5AC implication in Tunisian
colorectal cancer patients. Turk J Med Sci. 51:309–318.
2021.PubMed/NCBI View Article : Google Scholar
|
|
71
|
Niv Y and Rokkas T: Mucin expression in
colorectal cancer (CRC): Systematic review and meta-analysis. J
Clin Gastroenterol. 53:434–440. 2019.PubMed/NCBI View Article : Google Scholar
|
|
72
|
Schimanski CC, Kasper S, Hegewisch-Becker
S, Schröder J, Overkamp F, Kullmann F, Bechstein WO, Vöhringer M,
Öllinger R, Lordick F, et al: Adjuvant MUC vaccination with
tecemotide after resection of colorectal liver metastases: A
randomized, double-blind, placebo-controlled, multicenter AIO phase
II trial (LICC). Oncoimmunology. 9(1806680)2020.PubMed/NCBI View Article : Google Scholar
|
|
73
|
Shimada M, Tsuji K, Shigeta S, Nagai T,
Watanabe Z, Tokunaga H, Kigawa J and Yaegashi N: Rethinking the
significance of surgery for uterine cervical cancer. J Obstet
Gynaecol Res. 48:576–586. 2022.PubMed/NCBI View Article : Google Scholar
|
|
74
|
Togami S, Nomoto M, Higashi M, Goto M,
Yonezawa S, Tsuji T, Batra SK and Douchi T: Expression of mucin
antigens (MUC1 and MUC16) as a prognostic factor for mucinous
adenocarcinoma of the uterine cervix. J Obstet Gynaecol Res.
36:588–597. 2010.PubMed/NCBI View Article : Google Scholar
|
|
75
|
Gardner AB, Charo LM, Mann AK, Kapp DS,
Eskander RN and Chan JK: Ovarian, uterine, and cervical cancer
patients with distant metastases at diagnosis: Most common
locations and outcomes. Clin Exp Metastasis. 37:107–113.
2020.PubMed/NCBI View Article : Google Scholar
|
|
76
|
Samouëlian V, Mechtouf N, Leblanc E,
Cardin GB, Lhotellier V, Querleu D, Révillion F and Rodier F:
Sensitive molecular detection of small nodal metastasis in uterine
cervical cancer using HPV16-E6/CK19/MUC1 cancer biomarkers.
Oncotarget. 9:21641–21654. 2018.PubMed/NCBI View Article : Google Scholar
|
|
77
|
Cai J, Chen H, Lu M, Zhang Y, Lu B, You L,
Zhang T, Dai M and Zhao Y: Advances in the epidemiology of
pancreatic cancer: Trends, risk factors, screening, and prognosis.
Cancer Lett. 520:1–11. 2021.PubMed/NCBI View Article : Google Scholar
|
|
78
|
Wang S, You L, Dai M and Zhao Y: Mucins in
pancreatic cancer: A well-established but promising family for
diagnosis, prognosis and therapy. J Cell Mol Med. 24:10279–10289.
2020.PubMed/NCBI View Article : Google Scholar
|
|
79
|
Fu X, Tang N, Xie WQ, Mao L and Qiu YD:
MUC1 promotes glycolysis through inhibiting BRCA1 expression in
pancreatic cancer. Chin J Nat Med. 18:178–185. 2020.PubMed/NCBI View Article : Google Scholar
|
|
80
|
Sierzega M, Mlynarski D, Tomaszewska R and
Kulig J: Semiquantitative immunohistochemistry for mucin (MUC1,
MUC2, MUC3, MUC4, MUC5AC, and MUC6) profiling of pancreatic ductal
cell adenocarcinoma improves diagnostic and prognostic performance.
Histopathology. 69:582–591. 2016.PubMed/NCBI View Article : Google Scholar
|
|
81
|
Maleki F, Rezazadeh F and Varmira K:
MUC1-targeted radiopharmaceuticals in cancer imaging and therapy.
Mol Pharm. 18:1842–1861. 2021.PubMed/NCBI View Article : Google Scholar
|
|
82
|
Alirezapour B, Ashkezari MD, Fini MM,
Rasaee MJ, Mohammadnejad J, Paknejad M, Maadi E, Yousefnia H and
Zolghadri S: Preparation and preclinical characterization of
(111)In-DTPA-Anti-MUC1 as a radioimmunoconjugate for diagnosis of
breast cancer by single-photon emission computed tomography. J
Cancer Res Ther. 18:158–167. 2022.PubMed/NCBI View Article : Google Scholar
|
|
83
|
Stergiou N, Nagel J, Pektor S, Heimes AS,
Jäkel J, Brenner W, Schmidt M, Miederer M, Kunz H, Roesch F and
Schmitt E: Evaluation of a novel monoclonal antibody against
tumor-sassociated MUC1 for diagnosis and prognosis of breast
cancer. Int J Med Sci. 16:1188–1198. 2019.PubMed/NCBI View Article : Google Scholar
|
|
84
|
Pierga JY, Bidard FC, Denis MG and de
Cremoux P: Prognostic value of peripheral blood double detection of
CK19 and MUC1 mRNA positive cells detected by RT-quantitative PCR
in 94 breast cancer patients with a follow up of 9 years. Mol
Oncol. 1:267–268. 2007.PubMed/NCBI View Article : Google Scholar
|
|
85
|
Liu C, Xie Y, Sun B, Geng F, Zhang F, Guo
Q, Wu H, Yu B, Wu J, Yu X, et al: MUC1- and survivin-based DNA
vaccine combining immunoadjuvants CpG and interleukin-2 in a
bicistronic expression plasmid generates specific immune responses
and antitumour effects in a murine colorectal carcinoma model.
Scand J Immunol. 87:63–72. 2018.PubMed/NCBI View Article : Google Scholar
|
|
86
|
Ruan J, Duan Y, Li F and Wang Z: Enhanced
synergistic anti-Lewis lung carcinoma effect of a DNA vaccine
harboring a MUC1-VEGFR2 fusion gene used with GM-CSF as an
adjuvant. Clin Exp Pharmacol Physiol. 44:71–78. 2017.PubMed/NCBI View Article : Google Scholar
|
|
87
|
Gong YF, Zhou QB, Liao YD, Mai C, Chen TJ,
Tang YQ and Chen RF: Optimized construction of MUC1-VNTRn DNA
vaccine and its anti-pancreatic cancer efficacy. Oncol Lett.
13:2198–2206. 2017.PubMed/NCBI View Article : Google Scholar
|
|
88
|
Ogasawara M, Miyashita M, Yamagishi Y and
Ota S: Dendritic cell vaccination combined with a conventional
chemotherapy for patients with relapsed or advanced pancreatic
ductal adenocarcinoma: A single-center phase I/II trial. Ther Apher
Dial. 25:415–424. 2021.PubMed/NCBI View Article : Google Scholar
|
|
89
|
Ota S, Miyashita M, Yamagishi Y and
Ogasawara M: Baseline immunity predicts prognosis of pancreatic
cancer patients treated with WT1 and/or MUC1 peptide-loaded
dendritic cell vaccination and a standard chemotherapy. Hum Vaccin
Immunother. 17:5563–5572. 2021.PubMed/NCBI View Article : Google Scholar
|
|
90
|
Tosch C, Bastien B, Barraud L, Grellier B,
Nourtier V, Gantzer M, Limacher JM, Quemeneur E, Bendjama K and
Préville X: Viral based vaccine TG4010 induces broadening of
specific immune response and improves outcome in advanced NSCLC. J
Immunother Cancer. 5(70)2017.PubMed/NCBI View Article : Google Scholar
|
|
91
|
Glaffig M, Stergiou N, Hartmann S, Schmitt
E and Kunz H: A synthetic MUC1 anticancer vaccine containing
mannose ligands for targeting macrophages and dendritic cells.
ChemMedChem. 13:25–29. 2018.PubMed/NCBI View Article : Google Scholar
|
|
92
|
Hu B, Wang J, Guo Y, Chen T, Ni W, Yuan H,
Zhang N, Xie F and Tai G: Pre-clinical toxicity and immunogenicity
evaluation of a MUC1-MBP/BCG anti-tumor vaccine. Int
Immunopharmacol. 33:108–118. 2016.PubMed/NCBI View Article : Google Scholar
|
|
93
|
Zhang H, Zhao H, He X, Xi F and Liu J:
JAK-STAT domain enhanced MUC1-CAR-T cells induced esophageal cancer
elimination. Cancer Manag Res. 12:9813–9824. 2020.PubMed/NCBI View Article : Google Scholar
|
|
94
|
Mei Z, Zhang K, Lam AK, Huang J, Qiu F,
Qiao B and Zhang Y: MUC1 as a target for CAR-T therapy in head and
neck squamous cell carinoma. Cancer Med. 9:640–652. 2020.PubMed/NCBI View Article : Google Scholar
|
|
95
|
Zhou R, Yazdanifar M, Roy LD, Whilding LM,
Gavrill A, Maher J and Mukherjee P: CAR T cells targeting the tumor
MUC1 glycoprotein reduce triple-negative breast cancer growth.
Front Immunol. 10(1149)2019.PubMed/NCBI View Article : Google Scholar
|
|
96
|
Pang L, Wang J, Fan Y, Xu R, Bai Y and Bai
L: Correlations of TNM staging and lymph node metastasis of gastric
cancer with MRI features and VEGF expression. Cancer Biomark.
23:53–59. 2018.PubMed/NCBI View Article : Google Scholar
|
|
97
|
Jeong O, Jung MR and Kang JH: Prognostic
value of the anatomic region of metastatic lymph nodes in the
current TNM staging of gastric cancer. J Gastric Cancer.
21:236–245. 2021.PubMed/NCBI View Article : Google Scholar
|