1. Introduction
Gastric cancer is the fifth most common cancer
worldwide in terms of incidence, with >1 million new cases in
2020, and the fourth most frequently implicated in cancer-related
deaths, with 768,793 deaths occurring per year (1). Incidence varies according to sex
(15.7 cases/100,000 for men and 7.0 cases/100,000 for women) and
age, with the highest incidence amongst people aged 55-80 years old
(2). In addition, 50% of cases
occur in Eastern Asia (3). Gastric
adenocarcinoma (GC) represents 90% of all gastric cancer cases
(4), whereas gastric squamous cell
carcinoma (GSCC) accounts for 0.04-0.5% of cases (5,6).
Other rare histological variants include adenosquamous carcinoma,
carcinosarcoma, and oncocytic and malignant rhabdoid tumours
(7). Rolleston and Trevor
(8) described the first primary
GSCC case in 1905 in a 39-year-old female patient. Akce et
al (6) collected retrospective
data on 61,215 gastric cancer cases diagnosed between 2004 and 2013
using the National Cancer Database. In this cohort, GSCC
represented 1.4% of cases (n=836) with a mean age at diagnosis of
65.9 years (range, 23-90 years); in addition, a large proportion of
the patients were male, 72.5% of all cases. Furthermore, in this
cohort, 14.4% of patients with GC and 24.3% of patients with GSCC
were African American (6). Using
the Surveillance, Epidemiology, and End Results (SEER) database,
Dong et al (9) revealed
that 50% of patients with GSCC are diagnosed with stage IV disease.
Mixed histology is also found in GSCC (10).
2. Pathogenesis and aetiology
The aetiology of GSCC is currently unknown.
Pathophysiological hypotheses include differentiation of totipotent
stem cells, the transformation of existing ectopic squamous tissue,
squamous metaplasia resulting from chronic inflammation, a squamous
transformation of a pre-existing adenocarcinoma, and infection with
Epstein-Barr virus (EBV) or human papillomavirus (HPV) (5,11).
First mentioned by Boswell and Helwig in 1965(12), squamous metaplasia is thought to be
associated with certain factors, such as peptic ulcers, corrosive
burns, congenital syphilis, chemoradiotherapy and long-term
treatment with cyclophosphamide. These stressors create an
inflammatory setting within the gastric mucosa, leading to
structural changes and squamous metaplasia (13). In GC, the pathophysiological
sequence is widely accepted to be a progression from chronic
gastritis to atrophic gastritis and metaplasia, dysplasia, and,
eventually, carcinoma (14).
GSCC and GC may share certain risk factors.
Helicobacter pylori infection is a well-known risk factor
for GC and gastritis, accounting for 90% of non-cardia cases;
however, its association with GSCC has yet to be proven (15,16).
Out of four case reports, only one has reported on the synchronous
occurrence of H. pylori and GSCC (17-20).
Smoking is also a known risk factor for GC (15), and three studies have highlighted
smoking as a potential risk factor for GSCC (21-23).
The hypothesis that EBV could be a risk factor comes from the fact
that EBV is detected in 10% of gastric cancer cases (24) and that it was detected in two case
reports of GSCC (17,25,26).
Furthermore, HPV is known to cause dysplasia in squamous epithelia,
and it is strongly associated with head/neck, cervix and anus
squamous cell carcinoma (27);
however, its association with GSCC is still unproven. Of the three
case reports of GSCC using immunohistochemistry and/or in
situ hybridisation for HPV detection, none were positive
(17,19,25).
Other established risk factors for GC, such as heavy alcohol
consumption, foods preserved by salting, gastroesophageal reflux
and obesity, may also be implicated in the pathogenesis of GSCC,
but data are still insufficient (15). Ma et al (28) performed molecular analyses on six
cases of GSCC and demonstrated an increase in the Sonic hedgehog
signalling pathway-related molecules compared with in GC.
3. Prognosis
GC has a 5-year overall survival rate of 20%,
whereas the 5-year overall survival rate for GSCC ranges between 13
and 51.9% (6,9,29,30).
Notably, ~50% of GSCC cases are diagnosed as locally advanced or
metastatic disease, which may explain the lower survival rate
compared with GC (9). The median
overall survival range is between 7 and 8.9 months (6,9,31).
In a retrospective study, Akce et al (6) showed that, stage by stage, median
overall survival for GSCC was lower compared with GC survival at
any stage: Stage I, 16.1 vs. 32.2 months; stage II, 19.3 vs. 23.7
months; stage III, 14.2 vs. 16.4 months (6). As for GC, staging is the most
important prognostic factor for GSCC (6,30).
Furthermore, not receiving chemotherapy or surgery is associated
with worse survival rates (6).
4. Clinical presentation
The clinical presentation of GSCC is similar to GC
since symptoms are often non-specific. Common complaints include
abdominal pain, weight loss, melena, as well as nausea and vomiting
(9,30).
5. Diagnosis
As for GC, GSSC diagnosis requires histological
proof obtained during a gastroscopy. The European Society of
Gastrointestinal Endoscopy recommends that the gastroscopy last ≥7
min for an accurate diagnosis (32). Notably, GSCC cannot be
differentiated from GC based on visual appearance during endoscopic
procedures and thus histopathological analysis is required
(9). Both GC and GSCC lesions
usually present as a mass or a non-healing ulcer (33).
GSCC is referenced by the World Health Organization
classification under the number: ICD 8070/3(7). The Japanese Gastric Cancer
Association has set specific histological criteria for GSCC
including: i) Tumour cells are exclusively SCC cells, with no
adenocarcinomatous cell contingent, and ii) evidence that the GSCC
arose from the gastric mucosa directly (34). Boswell and Helwig (12) were the first to set histological
morphological criteria for GSCC. The lesion should include at least
one of the following criteria: i) Keratinized cell masses forming
keratin pearls, ii) mosaic cell arrangement, iii) presence of
intercellular bridges, and iv) high concentration of sulfhydryl
and/or disulfide groups, indicating the presence of keratin or
prekeratin (12). Large biopsies
are mandatory to exclude another associated component
(adenocarcinoma in particular).
The morphological aspect is the cornerstone of the
differential diagnosis between GSCC and GC. However, on biopsies,
in case of diagnostic doubt between a poorly differentiated
adenocarcinoma and a poorly differentiated SCC, complementary
techniques such as staining with Alcian blue-PAS (in search of
mucus in GC) or immunohistochemical markers (such as p40, which is
positive in GSCC) can be used. Parks (35) first proposed diagnostic criteria to
differentiate GSCC from SCC of the oesophagus or metastasis from
another primary site: i) Tumour not located in the cardia, ii) no
oesophageal extension of the tumour, and iii) no evidence of SCC in
any other part of the body (35).
To the best of our knowledge, molecular analyses have been
performed in only two case reports (36,37),
with one reporting a mismatch repair deficient lesion (36).
6. Staging
There is no specific recommendation for GSCC
regarding staging. We recommend following the European Society for
Medical Oncology (ESMO) GC staging recommendations for GSCC,
including endoscopic ultrasound, with or without fine needle
aspiration for the assessment of tumour depth and regional lymph
node involvement, computed tomography (CT) of the thorax and
abdomen and/or pelvis for detecting distant metastasis, and
laparoscopy for peritoneum assessment (33). Schizas et al (30) reported the use of positron emission
tomography (PET)-CT in preoperative staging in 18.3% of cases. This
could prove to be a useful additional tool in the detection of
distant metastasis, although it is not recommended routinely by the
ESMO (4). To the best of our
knowledge, there are currently no data on magnification endoscopy
for GSCC; this tool has however proven to be useful in oesophageal
SCC, enabling better identification of the margins, as well as
predicting the depth of infiltration to optimize endoscopic
treatment (38).
GSCC staging is also performed using the American
Joint Committee on Cancer TNM classification for GC, which depends
on the depth of invasion, lymph node invasion, and the presence or
absence of distant metastases (39). The most common metastasis sites for
GSCC are the liver, peritoneum, lung and bones (40). Another classification system by the
Japanese Gastric Cancer Association is based on refined anatomic
location, particularly on the lymph node stations (41). To the best of our knowledge, these
staging systems have not been formally compared.
7. Treatment options
Neither the ESMO nor the National Comprehensive
Cancer Network (NCCN) has recommendations for how to treat GSSC.
Treatment trends were reported by Akce et al (6) in their study of 836 cases of GSCC.
Surgical treatment was used in 26% of cases, compared with 32 and
95% reported in other studies (6,9,18)
(Table I). They also reported that
patients not receiving surgery were associated with worse survival
rates (hazard ratio, 2.79) (6). In
another study, Dong et al (9) reported that the 5-year overall
survival rates were 17.4 and 59.2% in the surgery and non-surgery
subgroups of patients with GSCC. Furthermore, Dong et al
(9) reported radiation therapy in
23.3% of patients, compared with in 48.1% of patients reported by
Akce et al (6). Akce et
al (6) also observed that
patients not treated with chemotherapy were associated with worse
survival (hazard ratio, 1.71). A previous literature review
conducted by Schizas et al (30) showed a 5-year overall survival rate
of 51.9% and 3-year disease-free survival rate of 30.8% for
patients undergoing surgical treatment for GSCC. In this review,
only one patient received neoadjuvant chemotherapy with
carboplatin/paclitaxel, 20 patients (60%) received adjuvant
chemotherapy (mostly cisplatin or 5-fluorouracil based), and three
patients (10%) benefited from radiation therapy (45 Gy in 25
fractions or 50.4 Gy in 28 fractions) (30). These survival results are inferior
to the reported 70% 5-year survival rate for localized GC (42). To the best of our knowledge, no
difference in resection margins has been reported for GSCC compared
with GC. We propose the use of a management algorithm, as shown in
Fig. 1.
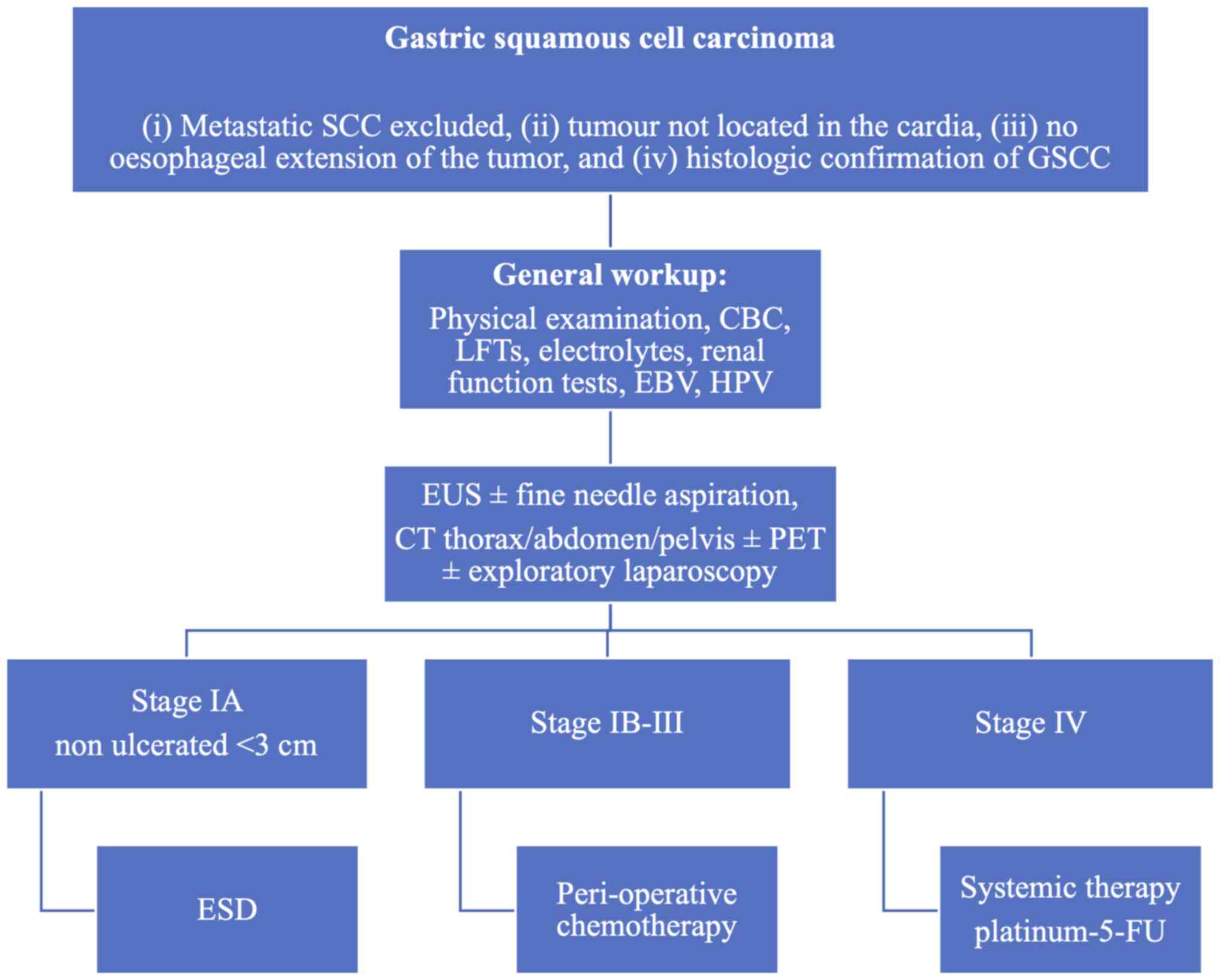 | Figure 1Proposed treatment algorithm for
GSCC. GSCC, gastric squamous cell carcinoma; CBC, complete blood
count; LFTs, liver function tests; EBV, Epstein-Barr virus; HPV,
human papillomavirus; EUS, endoscopic ultrasound; CT, computed
tomography; PET, positron emission tomography; ESD, endoscopic
submucosal dissection; 5-FU, 5-fluorouracil. |
 | Table IGastric squamous cell carcinoma case
series. |
Table I
Gastric squamous cell carcinoma case
series.
| First author,
year | Number of included
cases | Use of surgery,
% | Use of radiation
therapy, % | Use of systemic
therapy, % | 5-year overall
survival rate, % | (Refs.) |
|---|
| Akce, 2019 | 836 | 26.0 | 48.1 | 59.8 | 17.4 | (6) |
| Dong, 2016 | 163 | 31.9 | 23.3 | Not reported | 32.7 | (9) |
| Wakabayashi,
2014 | 56 | 94.6 | Not reported | 20 | Not reported | (18) |
Non-metastatic disease
A literature review performed by Schizas et
al (30) suggested that
radical resection is an important factor in improving patient
survival. Although no data on the topic exists, we hypothesize that
for early GSCC lesions (≤cT1 cN0) endoscopic submucosal dissection
could be proposed for non-ulcerated lesions with a maximum diameter
of 3 cm. This procedure could also serve as a ‘staging macro
biopsy’ in case of histological features conferring a higher risk
for nodal or systemic spread. For localised but more advanced
disease (>cT1), Schizas et al (30) showed that most patients benefited
from adjuvant therapy following resection, and despite the lack of
strong evidence, we recommend a peri-operative chemotherapy
approach with primary tumour resection and D2 lymphadenectomy, due
to the poor prognosis of GSCC. Although without formal evidence we
recommend the use of FLOT (5-fluorouracil, oxaliplatin and
docetaxel) as a peri-operative regimen based on the fact that these
drugs seem to have some level of efficacy in metastatic GSCC
(4).
Metastatic disease
Very little is known about the treatment for
metastatic GSCC. To the best of our knowledge, only nine cases have
been published (Table II), with
clinicians using platinum-fluoropyrimidine or platinum-taxane
doublet (18,23,34,43-48).
Chemoradiotherapy was used in one case with capecitabine and
oxaliplatin and reported survival of 27 months (18). Due to the lack of reporting, it is
not possible to generate strong evidence. In line with the
published cases, we recommend using platinum-fluoropyrimidine or
platinum-taxane doublet as the first line of treatment. Although
molecular knowledge in GSCC is poor and response to targeted
therapies has not been described in this pathology we are
recommending testing metastatic GSCC, similar to GC, at least for
HER-2 amplification and microsatellite instability. Notably, those
molecular alterations and their associated therapies (namely,
trastuzumab or anti-PD-1 immunotherapy) have shown efficacy in all
but a few tumour types, independently of the tumour histology and
localisation (4). Psychological
and dietary support is also recommended with attention to vitamin
and mineral deficiencies (4).
| Table IIMetastatic gastric squamous cell
carcinoma case reports. |
Table II
Metastatic gastric squamous cell
carcinoma case reports.
| First author,
year | Sex | Age, years | Metastasis
site | Treatment | Survival after
diagnosis | (Refs.) |
|---|
| Amado Villanueva,
2022 | Female | 32 | Liver | Folinic acid, 5-FU,
oxaliplatin | 8 months | (43) |
| Beattie, 2019 | Male | 53 | Liver | Carboplatin,
paclitaxel | Not reported (>6
months) | (44) |
| Sabbah, 2021 | Female | 66 | Ovary | Symptomatic | Few months | (34) |
| Vailas, 2019 | Male | 66 | Lungs | Surgery,
paclitaxel, carboplatin | Not reported
(>12 months) | (45) |
| Von Waagner,
2015 | Male | 70 | Peritoneum,
liver | Surgery, radiation,
capecitabine, oxaliplatin | 27 months | (23) |
| Wakabayashi,
2014 | Male | 69 | Liver | Surgery, 5-FU,
cisplatin, docetaxel | 36 months | (18) |
| Wu, 2016 | Male | 59 | Liver, spleen | Surgery, docetaxel,
cisplatin | 16 months | (46) |
| Yamagata, 2019 | Male | 60 | Liver | Surgery, S-1 (novel
5-FU derivative) | 17 months | (48) |
| Yang, 2020 | Female | 51 | Peritoneum | Docetaxel,
cisplatin | Not reported | (47) |
8. Treatment evaluation and follow-up
Due to the aggressiveness of the disease, we
recommend a close follow-up of patients with GSSC. Due to the
current lack of data, we recommend referring to the ESMO or NCCN
guidelines described for GC for treatment assessment and follow-up
of GSSC (4).
9. Conclusion
GSSC is a rare entity regarding which little is
currently known. Similarly to other rare histological subtypes, a
precise definition is needed to ensure an adequate diagnosis
(35,49). The present review summarized the
few reports regarding GSSC showing that patients diagnosed with
GSSC seem to respond to molecules used to treat GC; therefore, our
recommendation is currently to treat GSSC accordingly.
The present literature review has several
limitations: First, a reporting bias could exist due to the rarity
of the pathology of which only a handful of cases have been
reported. Second, a selection bias may exist, in that not all cases
used the diagnostic criteria set by Parks (35), Boswell and Helwig (12), or the Japanese Gastric Cancer
Association (34). It is likely
that database analyses, such as the SEER database analysed by Dong
et al (9) or the National
Cancer Database analysed by Akce et al (6), are unable to assess the correctness
of the diagnosis based on the three criteria listed by Parks
(35) and will have most likely
misclassified some cases. Third, data to support endoscopic
submucosal dissection in GSCC are lacking and would benefit from
future research; the prognosis of GSCC is inferior to GC, and for
this reason, endoscopic submucosal dissection should only be
considered for stage IA non-ulcerated lesions <3 cm with no
additional risk factors. Finally, the retrospective nature of the
present review is prone to bias that can only be addressed by
prospectively collecting and analysing GSSC data.
To improve our knowledge, we recommend
systematically testing for H. pylori, EBV or HPV to
determine their potential role in the pathogenesis of GSCC.
Extensive molecular profiling could help to determine if GSSC is
molecularly related to oesophageal SCC. This element is of utmost
importance as GSSC has been classically treated as GC with
chemotherapy; however, the chemoradiotherapy regimens used for
oesophageal SCC could prove to be a valid option. Finally, we are
pledging the creation of an international database of rare gastric
cancer cases to improve the care of these patients.
Acknowledgements
The authors would like to thank Professor Mary
Flannery (Department of English, University of Bern) for her help
in the writing of this article.
Funding
Funding: No funding was received.
Availability of data and materials
Not applicable.
Authors' contributions
TK designed the study. GDL collected the data and
conducted the literature review. GDL, TK, EC and AB interpreted the
data and contributed to the writing of the draft manuscript. Data
authentication is not applicable. All authors read and approved the
final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
TK discloses consulting or advisory roles for Merck
Sharp & Dohme (MSD), Bristol-Myers Squibb (BMS), Lilly, Roche,
Boehringer Ingelheim and Servier. All other authors declare that
they have no competing interests.
References
|
1
|
Sung H, Ferlay J, Siegel RL, Laversanne M,
Soerjomataram I, Jemal A and Bray F: Global cancer statistics 2020:
GLOBOCAN estimates of incidence and mortality worldwide for 36
cancers in 185 countries. CA Cancer J Clin. 71:209–249.
2021.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Thrift AP and El-Serag HB: Burden of
gastric cancer. Clin Gastroenterol Hepatol. 18:534–542.
2020.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Rahman R, Asombang AW and Ibdah JA:
Characteristics of gastric cancer in Asia. World J Gastroenterol.
20:4483–4490. 2014.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Lordick F, Carneiro F, Cascinu S, Fleitas
T, Haustermans K, Piessen G, Vogel A and Smyth EC: ESMO Guidelines
Committee. Electronic address: simpleClinicalguidelines@esmo.org.
Gastric cancer: ESMO Clinical Practice Guideline for diagnosis,
treatment and follow-up. Ann Oncol. 33:1005–1020. 2022.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Guzman Rojas P, Parikh J, Vishnubhotla P
and Oharriz JJ: Primary gastric squamous cell carcinoma. Cureus.
10(e2389)2018.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Akce M, Jiang R, Alese OB, Shaib WL, Wu C,
Behera M and El-Rayes BF: Gastric squamous cell carcinoma and
gastric adenosquamous carcinoma, clinical features and outcomes of
rare clinical entities: A National Cancer Database (NCDB) analysis.
J Gastrointest Oncol. 10:85–94. 2019.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Nagtegaal ID, Odze RD, Klimstra D, Paradis
V, Rugge M, Schirmacher P, Washington KM, Carneiro F and Cree IA:
WHO Classification of Tumours Editorial Board. The 2019 WHO
classification of tumours of the digestive system. Histopathology.
76:182–188. 2020.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Rolleston HD and Trevor RS: A case of
columnar-celled carcinoma of the stomach showing squamous-celled
metaplasia. J Pathol Bacteriol. 10:418–422. 1905.
|
|
9
|
Dong C, Jiang M, Tan Y, Kong Y, Yang Z,
Zhong C, Li D and Yuan Y: The clinicopathological features and
prognostic factors of gastric squamous cell carcinoma. Medicine
(Baltimore). 95(e4720)2016.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Faria GR, Eloy C, Preto JR, Costa EL,
Almeida T, Barbosa J, Paiva ME, Sousa-Rodrigues J and Pimenta A:
Primary gastric adenosquamous carcinoma in a Caucasian woman: A
case report. J Med Case Reports. 4(351)2010.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Straus R, Heschel S and Fortmann DJ:
Primary adenosquamous carcinoma of the stomach. A case report and
review. Cancer. 24:985–995. 1969.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Boswell JT and Helwig EB: Squamous cell
carcinoma and adenoacanthoma of the stomach. A clinicopathologic
study. Cancer. 18:181–192. 1965.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Chang YS, Kim MS, Kim DH, Park S, You JY,
Han JK, Kim SH and Lee HJ: Primary squamous cell carcinoma of the
remnant stomach after subtotal gastrectomy. J Gastric Cancer.
16:120–124. 2016.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Mukkamalla SKR, Recio-Boiles A and Babiker
HM: Gastric Cancer. In: StatPearls. StatPearls Publishing, Treasure
Island (FL), 2023.
|
|
15
|
Morgan E, Arnold M, Camargo MC, Gini A,
Kunzmann AT, Matsuda T, Meheus F, Verhoeven RHA, Vignat J,
Laversanne M, et al: The current and future incidence and mortality
of gastric cancer in 185 countries, 2020-40: A population-based
modelling study. EClinicalMedicine. 47(101404)2022.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Lee YC, Chiang T-H, Chou CK, Tu YK, Liao
WC, Wu MS and Graham DY: Association between helicobacter pylori
eradication and gastric cancer incidence: A systematic review and
Meta-Analysis. Gastroenterology. 150:1113–1124.e5. 2016.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Callacondo D, Ganoza-Salas A, Anicama-Lima
W, Quispe-Mauricio A and Longacre TA: Primary squamous cell
carcinoma of the stomach with paraneoplastic leukocytosis: A case
report and review of literature. Hum Pathol. 40:1494–1498.
2009.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Wakabayashi H, Matsutani T, Fujita I,
Kanazawa Y, Nomura T, Hagiwara N, Hosone M, Katayama H and Uchida
E: A rare case of primary squamous cell carcinoma of the stomach
and a review of the 56 cases reported in Japan. J Gastric Cancer.
14:58–62. 2014.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Yamada R, Horiguchi SI, Shimizuguchi R,
Nakano N, Motoi T, Monma K and Hishima T: A first case of primary
gastric verrucous carcinoma with isolated squamous epithelium in
the stomach. Virchows Arch. 475:115–119. 2019.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Zhou K, Faraz A, Magotra M and Tahir M:
Exophytic primary gastric squamous cell carcinoma and H. pylori
gastritis. BMJ Case Rep. 12(e230310)2019.PubMed/NCBI View Article : Google Scholar
|
|
21
|
González-Sánchez JA, Vitón R, Collantes E
and Rodríguez-Montes JA: Primary squamous cell carcinoma of the
stomach. Clin Med Insights Oncol.
11(1179554916686076)2017.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Chen Y, Zhu H, Xu F, Cao Y, Gu X, Wan Y
and Gou H: Clinicopathological characteristics, treatment, and
prognosis of 21 patients with primary gastric squamous cell
carcinoma. Gastroenterol Res Pract. 2016(e3062547)2016.PubMed/NCBI View Article : Google Scholar
|
|
23
|
von Waagner W, Wang Z and Picon AI: A Rare
Case of a primary squamous cell carcinoma of the stomach presenting
as a submucosal mass. Case Rep Surg. 2015(482342)2015.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Takada K: Epstein-Barr virus and gastric
carcinoma. Mol Pathol. 53:255–261. 2000.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Katsura Y, Okabayashi T, Ozaki K, Shibuya
Y and Iwata J: A case of Epstein Barr virus-associated primary
squamous cell carcinoma of stomach. Surg Case Rep.
7(240)2021.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Takita J, Kato H, Miyazaki T, Nakajima M,
Fukai Y, Masuda N, Manda R, Fukuchi M and Kuwano H: Primary
squamous cell carcinoma of the stomach: A case report with
immunohistochemical and molecular biologic studies.
Hepatogastroenterology. 52:969–974. 2005.PubMed/NCBI
|
|
27
|
Szymonowicz KA and Chen J: Biological and
clinical aspects of HPV-related cancers. Cancer Biol Med.
17:864–878. 2020.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Ma XL, Sun HJ, Wang YS, Huang SH, Xie JW
and Zhang HW: Study of Sonic hedgehog signaling pathway related
molecules in gastric carcinoma. World J Gastroenterol.
12:3965–3969. 2006.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Thomas RM and Sobin LH: Gastrointestinal
cancer. Cancer. 75:154–170. 1995.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Schizas D, Papaconstantinou D, Syllaios A,
Ntomi V, Kykalos S, Tsourouflis G, Nastos C, Misiakos E and
Pikoulis E: Oncologic outcomes of patients with resectable primary
gastric squamous cell carcinoma: A systematic review. Ann
Gastroenterol. 35:376–382. 2022.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Meng Y, Zhang J, Wang H, Zhang Y, Sun R,
Zhang Z, Gao F, Huang C and Zhang S: Poorer prognosis in patients
with advanced gastric squamous cell carcinoma compared with
adenocarcinoma of the stomach: Case report. Medicine (Baltimore).
96(e9224)2017.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Bisschops R, Areia M, Coron E, Dobru D,
Kaskas B, Kuvaev R, Pech O, Ragunath K, Weusten B, Familiari P, et
al: Performance measures for upper gastrointestinal endoscopy: A
European Society of Gastrointestinal Endoscopy (ESGE) Quality
Improvement Initiative. Endoscopy. 48:843–864. 2016.PubMed/NCBI View Article : Google Scholar
|
|
33
|
ASGE Standards of Practice Committee.
Evans JA, Chandrasekhara V, Chathadi KV, Decker GA, Early DS,
Fisher DA, Foley K, Hwang JH, Jue TL, et al: The role of endoscopy
in the management of premalignant and malignant conditions of the
stomach. Gastrointest Endosc. 82:1–8. 2015.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Sabbah M, Gharbi G, Bellil N, Helal I,
Chamakhi C and Gargouri D: Primary gastric squamous cell carcinoma
with a bilio-gastric fistula and Krukenberg syndrome. Clin Case
Rep. 9(e04325)2021.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Parks RE: Squamous neoplasms of the
stomach. Am J Roentgenol. 101:447–449. 1967.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Jakubik J, Majos A, Jesionek-Kupnicka D,
Wrona E, Kaufman-Szymczyk A, Lubecka-Gajewska K and Jakubik J: An
unusual non-metastatic, mismatch repair-deficient primary gastric
squamous cell carcinoma presenting as a large, exophytic, bleeding
tumor: A case report. Oncol Lett. 25(82)2023.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Schonhart L, Kaiser R, Schmidt R, Sailer
A, Steinestel K, Schneider-Kappus W and Beltzer C: Primary gastric
squamous cell carcinoma-a case report of diagnosis, treatment,
histological findings and follow-up. Z Gastroenterol. 61:178–182.
2022.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Dekker E, Houwen BBSL, Puig I,
Bustamante-Balén M, Coron E, Dobru DE, Kuvaev R, Neumann H, Johnson
G, Pimentel-Nunes P, et al: Curriculum for optical diagnosis
training in Europe: European Society of Gastrointestinal Endoscopy
(ESGE) Position Statement. Endoscopy. 52:899–923. 2020.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Amin MB, Edge SB, Greene FL, et al: AJCC
Cancer Staging Manual. Springer International Publishing, 2018.
|
|
40
|
Riihimäki M, Hemminki A, Sundquist K,
Sundquist J and Hemminki K: Metastatic spread in patients with
gastric cancer. Oncotarget. 7:52307–52316. 2016.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Rosa F, Costamagna G, Doglietto GB and
Alfieri S: Classification of nodal stations in gastric cancer.
Transl Gastroenterol Hepatol. 2(2)2017.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Siegel RL, Miller KD, Fuchs HE and Jemal
A: Cancer statistics, 2022. CA Cancer J Clin. 72:7–33.
2022.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Amado Villanueva PP, López González J,
Lázaro Sáez M, Cuello Entrena E and Delgado Maroto A: An unusual
presentation of advanced primary gastric squamous cell carcinoma in
a young woman. Gastroenterol Hepatol. 45 (Suppl 1):S39–S40.
2022.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Beattie M, Mansour R, Thigpin D and Haus
C: Metastatic primary gastric squamous cell carcinoma: An uncommon
presentation of a rare malignancy. Case Rep Gastrointest Med.
2019(5305023)2019.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Vailas MG, Syllaios A, Hasemaki N,
Sotiropoulou M, Mpaili E, Sarlanis H, Felekouras E and Papalampros
A: A type of neoplasia deadlier than gastric adenocarcinoma? Report
of a case of primary gastric squamous cell carcinoma. World J Surg
Oncol. 17(113)2019.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Wu XD, Zhou Y, Fan RG, Zhou B, Shi Q and
Jia J: Primary squamous cell carcinoma of the stomach presenting as
a huge retroperitoneal tumor: A case report. Rev Esp Enferm Dig.
108:283–284. 2016.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Yang F, Lan Z and He Y: Gastric squamous
cell carcinoma presenting in ascites: Negative to P63 and P40 after
one course of chemotherapy. Diagn Cytopathol. 48:787–789.
2020.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Yamagata Y, Saito K, Ban S, Fujii A and
Oya M: The origin of p40-negative and CDX2-positive primary
squamous cell carcinoma of the stomach: Case report. World J Surg
Oncol. 17(53)2019.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Astaras C, Bornand A and Koessler T:
Squamous rectal carcinoma: A rare malignancy, literature review and
management recommendations. ESMO Open. 6(100180)2021.PubMed/NCBI View Article : Google Scholar
|














