Introduction
Bladder cancer is the most common malignant tumor of
the urinary tract, with an estimated 386,300 new cases and 150,200
mortalities from bladder cancer annually (1), ranking seventh in men and seventeenth
in women worldwide (2). The
etiology of bladder cancer involves the interaction between genetic
and environmental factors. Common risk factors include cigarette
smoking, occupational exposure to aromatic amines and polycyclic
aromatic hydrocarbons, inflammation of the urinary tract and
consumption of certain drugs (3).
Current evidence supports that molecular alterations and DNA
polymorphisms potentially alter individual susceptibility to
bladder cancer (4–5).
Of all the genetic susceptibility factors of bladder
cancer, folate metabolic pathway has received increasing attention
(5–7). Since it is the one-carbon groups donor
in DNA methylation and synthesis, folate deficiency may induce DNA
hypomethylation and potentially induce a proto-oncogene expression
leading to cancer.
Methylenetetrahydrofolate reductase (MTHFR) is the
key enzyme involved in folate metabolism, which acts as a critical
metabolic node in the regulation of methylation reactions. It
catalyzes the conversion of 5,10-methylenetetrahydrofolate to
5-methyltetrahydrofolate. The 5,10-methylenetetrahydrofolate is the
methyl donor for de novo thymidine synthesis and the
5-methyltetrahydrofolate is used as a cosubstrate to convert
homocysteine into methionine, which is the immediate precursor of
S-adenosylmethionine and the primary methyl donor of DNA
methylation. A less active form of MTHFR may result in
hypomethylation, which is a candidate mechanism for the development
of cancer (8).
The functional polymorphisms in the MTHFR gene,
Ala222Val (C677T) and Glu429Ala (A1298C), have received increasing
attention. Ala222Val homozygotes have been associated with reduced
enzyme activity of ~30% of the control value (9), while the Glu429Ala homozygotes exhibit
~60% of the control activity. Heterozygotes for the Ala222Val and
Glu429Ala mutations had ~50–60% of control activity (10). Since the two variants result in
reduced activity of MTHFR, their associations with the
susceptibility of a variety of cancers has been evaluated (11–14).
MTHFR Ala222Val and Glu429Ala polymorphisms have
also been evaluated in relation to bladder cancer risk. However,
the results of previous studies have yielded conflicting results.
Given the amount of accumulated data, this meta-analysis was
performed to derive a more precise estimation of the association of
MTHFR Ala222Val and Glu429Ala and bladder cancer risk.
Materials and methods
Publication search
An exhaustive search of the literature was performed
using the electronic databases: PubMed, EBSCO-Medline, Elsevier
ScienceDirect and BIOSIS Previews for relevant articles published
(up to September 2013). The articles were identified by using the
search terms ‘methylenetetrahydrofolate reductase’, ‘MTHFR’,
‘NADPH2’, ‘urinary bladder’ and ‘bladder’. The search was limited
to human studies with no language restrictions being applied.
Additional studies were obtained through the references cited in
retrieved articles on the association between the MTHFR Ala222Val
and Glu429Ala polymorphisms and bladder cancer. The searching of
the electronic databases and reviewing of the references in
retrieved articles were independently achieved by two
investigators.
Inclusion and exclusion criteria
Inclusion criteria for the studies were:
case-control studies on the association between MTHFR Ala222Val and
Glu429Ala polymorphisms and bladder cancer risk, and the data of
each study was required to be sufficient for statistical analysis
of odds ratio (OR) and 95% confidence interval (CI). Studies that
had duplicated data and in which genotypes could not be ascertained
were excluded.
Data abstraction
Information was extracted from all the eligible
publications independently by two investigators as per the
inclusion and exclusion criteria. For disagreements, consensus was
reached by discussion of the two investigators. The data abstracted
from each study were as follows: first author’s name, publication
date, country, ethnicity, source of controls, number of cases and
controls, and number of cases and controls for MTHFR Ala222Val and
Glu429Ala polymorphisms. Individuals of different descents were
classified as Chinese, European, American and Middle Eastern.
Statistical analysis
ORs with 95% CIs were applied to evaluate the
strength of association between MTHFR Ala222Val and Glu429Ala
polymorphisms and bladder cancer risk. The pooled ORs were
estimated for the co-dominant model (Val/Val vs. Ala/Ala and
Val/Ala vs. Ala/Ala for Ala222Val; Ala/Ala vs. Glu/Glu and Ala/Glu
vs. Glu/Glu for Glu429Ala), dominant model (Val/Val + Val/Ala vs.
Ala/Ala for Ala222Val; Ala/Ala + Ala/Glu vs. Glu/Glu for Glu429Ala)
and recessive model (Val/Val vs. Val/Ala + Ala/Ala for Ala222Val;
Ala/Ala vs. Ala/Glu + Glu/Glu for Glu429Ala), respectively. The
Chi-square test-based Q-statistic (Q test) was applied to assess
heterogeneity among the studies. The fixed-effects model was used
to calculate the pooled ORs if no heterogeneity was detected
(Ph≥0.05 by Q test) (15).
Otherwise, the random-effects model was applied (Ph<0.05 by Q
test) (16).
Subgroup analyses were performed by ethnicity and
source of controls. The sensitivity analyses were conducted by
excluding each study at a time to determine its effect on the
overall estimation, since all the studies indicated that they
conformed to the Hardy-Weinberg equilibrium (HWE). The publication
bias was estimated by the funnel plot, in which the standard error
of log (OR) was plotted against its log (OR) for each study.
Egger’s linear regression test was applied to assess the asymmetry
of the funnel plot, with P<0.05 indicating an asymmetric plot
and a possible publication bias (17). In this meta-analysis, the Stata
version 11.0 (StataCorp, College Station, TX, USA) was applied for
all the statistical tests.
Results
Flow of included studies
A total of 420 articles potentially relevant to the
searching terms were screened, including PubMed, 25; EBSCO-Medline,
24; Elsevier ScienceDirect, 338; and BIOSIS Previews, 33. Based on
the inclusion criteria, a total of 13 studies (5–7,18–27)
with full-text articles on polymorphisms of MTHFR Ala222Val and
Glu429Ala and bladder cancer risk were identified as eligible. Of
the 13 studies, two studies (22,24)
were excluded due to duplicated data with the study by Rouissi
et al (6).
Study characteristics
A total of 11 studies (5–7,18–21,23,25–27)
were included in this meta-analysis for Ala222Val (including 3,463
cases and 3,.927 controls) and 9 studies (5–7,19–21,23,25,27)
were included for Glu429Ala (including 3,177 cases and 3,502
controls) (Table I). Three of the
11 studies were population-based and eight were hospital-based
studies. The studies indicated that the distribution of genotypes
in controls was consistent with HWE. Detailed data from the
included studies were abstracted (Table II).
 | Table ICharacteristics of the case-control
studies considered in the meta-analysis. |
Table I
Characteristics of the case-control
studies considered in the meta-analysis.
| Authors (refs.) | Year | Ethnicity | Genotyping
method | HWE | Control source | Demographic
characteristics |
|---|
|
|---|
| Cases | Controls |
|---|
| Safarinejad et
al (27) | 2011 | Iranian (Asian) | PCR-RFLP | 0.56 | HB | 158 bladder cancer
patients, mean age: 62.7±10.6 years | 316 controls, mean
age: 61.6±9.4 years |
| Chung et al
(26) | 2010 | Chinese-Taiwan
(Asian) | PCR-RFLP | 0.26 | HB | 150 bladder cancer
patients, mean age: 65.3±1.1 years | 300 controls, mean
age: 66.2±0.7 years |
| Cai et al
(23) | 2009 | Chinese (Asian) | PCR-RFLP | 0.08 | HB | 312 bladder cancer
patients, mean age: 63.1±11.3 years | 325 controls, mean
age: 63.7±12.2 years |
| Rouissi et al
(6) | 2009 | Tunisian
(African) | PCR-RFLP | 0.49 | PB | 185 bladder cancer
patients, mean age 67.5±9.7 years | 191 controls, mean
age (match the case) |
| Wang et al
(25) | 2009 | Chinese
(Asian) | PCR-RFLP | 0.07 | HB | 239 bladder cancer
patients, pack years <55 (n=42); 55–65 (77); >65 (n=120) | 250 controls, pack
years <55 (n=45); 55–65 (n=81); >65 (n=124) |
| Moore et al
(7) | 2007 | Spanish
(European) | TaqMan and Golden
Gate | 0.48 | HB | 1,150 bladder
cancer patients, mean age: 66.0±10.0 years | 1,149 controls,
mean age: 65.0±10.0 years |
| Karagas et
al (21) | 2005 | USA (American) | PCR-RFLP | 0.70 | PB | 352 bladder cancer
patients, pack years ≤40 (9); 41–55 (n=60); 56–70 (n=203); >70
(n=80) | 551 controls, pack
years ≤40 (31); 41–55 (n=110); 56–70 (n=304); >70 (n=106) |
| Moore et al
(19) | 2004 | Argentina
(American) | PCR-RFLP | 0.29 | PB | 110 bladder cancer
patients, mean age: 68.1 (range, 20–80 years) | 110 controls, mean
age: 68.4 years (match the case) |
| Lin et al
(5) | 2004 | USA (American) | PCR-RFLP | 0.07 | HB | 457 bladder cancer
patients, mean age: 65.0 (range, 18–86 years) | 457 controls, mean
age: 64.0 (range, 21–89 years) |
| Sanyal et al
(20) | 2004 | Swedish
(European) | PCR-RFLP | 0.82 | HB | 327 bladder cancer
patients, mean age: 70.0 (range, 33–96 years) | 246 controls, mean
age (match the case) |
| Kimura et al
(18) | 2001 | Germany
(European) | PCR-RFLP | 0.17 | HB | 165 bladder cancer
patients, mean age: 67.4±11.5 years | 150 controls, mean
age: 62.0±11.4 years |
| Table IIDistribution of
methylenetetrahydrofolate reductase (MTHFR) gene Ala222Val and
Glu429Ala genotypes for bladder cancer patients and controls. |
Table II
Distribution of
methylenetetrahydrofolate reductase (MTHFR) gene Ala222Val and
Glu429Ala genotypes for bladder cancer patients and controls.
| Study (refs.) | Ethnicity | Ala222Val of
MTHFR | Glu429Ala of
MTHFR |
|---|
|
|
|---|
| Sample size
(case/control) | Case | Control | Sample size
(case/control) | Case | Control |
|---|
|
|
|---|
| AA | AV | VV | AA | AV | VV | GG | GA | AA | GG | GA | AA |
|---|
| Safarinejad et
al (27) | Iranian | 158/316 | 67 | 74 | 17 | 144 | 142 | 30 | 158/316 | 48 | 85 | 25 | 178 | 115 | 23 |
| Chung et al
(26) | Chinese | 150/300 | 80 | 57 | 13 | 141 | 123 | 36 | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| Cai et al
(23) | Chinese | 312/325 | 82 | 169 | 61 | 113 | 170 | 42 | 312/325 | 215 | 91 | 6 | 226 | 92 | 7 |
| Rouissi et
al (6) | Tunisian | 185/191 | 87 | 86 | 12 | 81 | 90 | 20 | 185/191 | 97 | 78 | 10 | 121 | 60 | 10 |
| Wang et al
(25) | Chinese | 239/250 | 66 | 128 | 45 | 88 | 132 | 30 | 239/250 | 169 | 67 | 3 | 171 | 75 | 4 |
| Moore et al
(7) | Spanish | 1,041/1,049 | 418 | 478 | 145 | 402 | 486 | 161 | 1,068/1,078 | 537 | 457 | 74 | 557 | 429 | 92 |
| Karagas et
al (21) | American | 350/543 | 140 | 171 | 39 | 227 | 245 | 71 | 350/542 | 173 | 146 | 31 | 267 | 220 | 55 |
| Moore et al
(19) | Argentina | 106/109 | 45 | 42 | 19 | 32 | 59 | 18 | 106/108 | 52 | 45 | 9 | 55 | 45 | 8 |
| Lin et al
(5) | American | 448/448 | 199 | 197 | 52 | 218 | 177 | 53 | 448/447 | 219 | 199 | 30 | 213 | 197 | 37 |
| Sanyal et al
(20) | Swedish | 309/246 | 173 | 113 | 23 | 121 | 102 | 23 | 311/245 | 145 | 133 | 33 | 110 | 111 | 24 |
| Kimura et al
(18) | Germany | 165/150 | 70 | 80 | 15 | 65 | 73 | 12 | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
Quantitative data synthesis
Overall, no significant associations of Ala222Val
and Glu429Ala polymorphisms with bladder cancer risk were
identified by this meta-analysis (Table III). For MTHFR Ala222Val: Val/Val
vs. Ala/Ala: OR, 1.02; 95% CI: 0.80–1.29; Val/Ala vs. Ala/Ala: OR,
1.02; 95% CI: 0.92–1.12; dominant model: OR, 1.01; 95% CI:
0.87–1.17; recessive model: OR, 1.00; 95% CI: 0.87–1.15; and for
MTHFR Glu429Ala: Ala/Ala vs. Glu/Glu: OR, 1.11; 95% CI: 0.78–1.58;
Ala/Glu vs. Glu/Glu: OR, 1.16; 95% CI: 0.95–1.40; dominant model:
OR, 1.15; 95% CI: 0.94–1.41; recessive model: OR, 0.96; 95% CI:
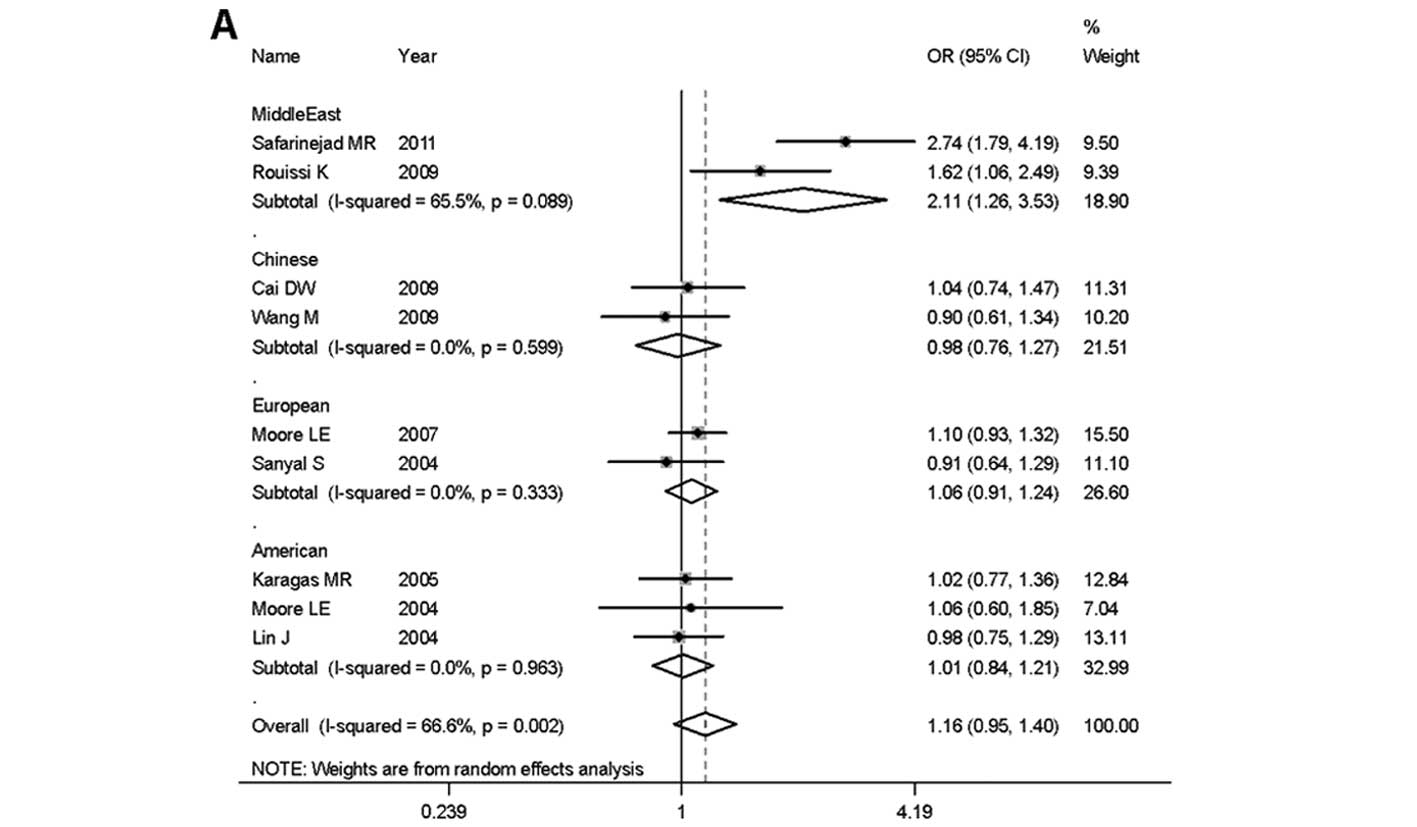
0.79–1.15. In the subgroup analyses by ethnicity, no significant
associations were found in any of the genetic models for the MTHFR
Ala222Val polymorphisms with bladder cancer risk. By contrast, the
Glu429Ala polymorphism was found to be significantly associated
with increased bladder cancer risk in individuals of Middle Eastern
descent (Ala/Glu vs. Glu/Glu: OR, 2.11; 95% CI: 1.26–3.53; dominant
model: OR, 2.16; 95% CI: 1.16–4.01; recessive model: OR, 1.82; 95%
CI: 1.11–3.01), whereas no significant associations were identified
in individuals of Chinese descent (Ala/Glu vs. Glu/Glu: OR, 0.98;
95% CI: 0.76–1.27; dominant model: OR, 0.97; 95% CI: 0.75–1.25;
recessive model: OR, 0.85; 95% CI: 0.35–2.07), European descent
(Ala/Glu vs. Glu/Glu: OR, 1.06; 95% CI: 0.91–1.24; dominant model:
OR, 1.03; 95% CI: 0.89–1.20; recessive model: OR, 0.86; 95% CI:
0.66–1.14), and American descent (Ala/Glu vs. Glu/Glu: OR, 1.01;
95% CI: 0.84–1.21; dominant model: OR, 0.98; 95% CI: 0.82–1.17;
recessive model: OR, 0.86; 95% CI: 0.62–1.18). The results of the
subgroup analysis by ethnicity were also shown by forest plots in
Fig. 1. In the subgroup analysis by
the source of controls, no significant associations were found in
any of the genetic models for the two polymorphisms (Table III).
| Table IIIResults of meta-analysis for
methylenetetrahydrofolate reductase (MTHFR) gene Ala222Val and
Glu429Ala polymorphism and bladder cancer risk. |
Table III
Results of meta-analysis for
methylenetetrahydrofolate reductase (MTHFR) gene Ala222Val and
Glu429Ala polymorphism and bladder cancer risk.
| Genetic model | Recessive
model | Dominant model | Homozygote | Heterozygote |
|---|
|
|
|
|
|
|---|
| Ala222Val | No. of study
(sample size case/control) | Val/Val vs. Val/Ala
+ Ala/Ala | Val/Val + Val/Ala
vs. Ala/Ala | Val/Val vs.
Ala/Ala | Val/Ala vs.
Ala/Ala |
|---|
|
|
|
|
|---|
| OR (95% CI) | Ph | OR (95% CI) | Ph | OR (95% CI) | Ph | OR (95% CI) | Ph |
|---|
| Overall | 11
(3,463/3,927) | 1.00
(0.87–1.15) | 0.130 | 1.01
(0.87–1.17) | 0.024 | 1.02
(0.80–1.29) | 0.019 | 1.02
(0.92–1.12) | 0.103 |
| Ethnicity | | | | | | | | | |
| Chinese | 3 (701/875) | 1.32
(0.80–2.15) | 0.070 | 1.19
(0.79–1.78) | 0.029 | 1.42
(0.72–2.78) | 0.016 | 1.16
(0.93–1.45) | 0.146 |
| European | 3
(1,515/1,445) | 0.89
(0.72–1.11) | 0.747 | 0.90
(0.78–1.05) | 0.485 | 0.86
(0.68–1.09) | 0.629 | 0.92
(0.79–1.07) | 0.558 |
| American | 3 (904/1,100) | 0.93
(0.71–1.22) | 0.759 | 0.98
(0.71–1.36) | 0.063 | 0.95
(0.71–1.26) | 0.690 | 0.97
(0.66–1.43) | 0.031 |
| Middle East | 2 (343/507) | 0.87
(0.54–1.40) | 0.184 | 0.98
(0.74–1.30) | 0.270 | 0.87
(0.53–1.44) | 0.134 | 1.00
(0.75–1.34) | 0.440 |
| Source of
control | | | | | | | | | |
| PB | 3 (641/843) | 0.83
(0.60–1.14) | 0.496 | 0.92
(0.74–1.13) | 0.109 | 0.78
(0.56–1.11) | 0.589 | 0.86
(0.57–1.29) | 0.057 |
| HB | 8
(2,822/3,084) | 1.08
(0.86–1.35) | 0.099 | 1.06
(0.89–1.25) | 0.033 | 1.12
(0.83–1.50) | 0.013 | 1.03
(0.92–1.15) | 0.203 |
|
| Glu429Ala | No. of study
(sample size case/control) | Ala/Ala vs. Ala/Glu
+ Glu/Glu | Ala/Ala + Ala/Glu
vs. Glu/Glu | Ala/Ala vs.
Glu/Glu | Ala/Glu vs.
Glu/Glu |
|
|
|
|
| OR (95% CI) | Ph | OR (95% CI) | Ph | OR (95% CI) | Ph | OR (95% CI) | Ph |
|
| Overall | 9
(3,177/3,257) | 0.96
(0.79–1.15) | 0.182 | 1.15
(0.94–1.41) | <0.001 | 1.11
(0.78–1.58) | 0.009 | 1.16
(0.95–1.40) | 0.002 |
| Ethnicity | | | | | | | | | |
| Chinese | 2 (551/575) | 0.85
(0.35–2.07) | 0.891 | 0.97
(0.75–1.25) | 0.595 | 0.85
(0.35–2.07) | 0.857 | 0.98
(0.76–1.27) | 0.599 |
| European | 2
(1,379/1,078) | 0.86
(0.66–1.14) | 0.335 | 1.03
(0.89–1.20) | 0.515 | 0.88
(0.66–1.17) | 0.512 | 1.06
(0.91–1.24) | 0.333 |
| American | 3 (904/1,097) | 0.86
(0.62–1.18) | 0.801 | 0.98
(0.82–1.17) | 0.915 | 0.86
(0.62–1.20) | 0.781 | 1.01
(0.84–1.21) | 0.963 |
| Middle East | 2 (343/507) | 1.82
(1.11–3.01) | 0.129 | 2.16
(1.16–4.01) | 0.032 | 2.35
(0.75–7.40) | 0.040 | 2.11
(1.26–3.53) | 0.089 |
| Source of
control | | | | | | | | | |
| PB | 3 (641/841) | 0.93
(0.64–1.36) | 0.839 | 1.13
(0.92–1.39) | 0.188 | 0.97
(0.66–1.44) | 0.726 | 1.16
(0.93–1.44) | 0.204 |
| HB | 6
(2,536/2,416) | 1.04
(0.72–1.51) | 0.052 | 1.15
(0.87–1.52) | <0.001 | 1.15
(0.68–1.93) | 0.001 | 1.14
(0.89–1.48) | 0.001 |
Heterogeneity and sensitivity
analysis
In the heterogeneity analysis, the Val/Val vs.
Ala/Ala model and dominant genetic model for the Ala222Val
polymorphism, as well as the Ala/Ala vs. Glu/Glu, Ala/Glu vs.
Glu/Glu and dominant genetic models for the Glu429Ala polymorphism
were found to be significant (Ph<0.05 by Q test, Table III). The Ph value of the subgroup
analysis showed that the heterogeneity was effectively decreased in
some of the comparisons and the major source of heterogeneity may
stem from the hospital-based controls and ethnicity, such as the
Chinese and American subgroups. In the sensitivity analyses, with
each study been excluded one at a time during the analysis, the
overall results were not altered and no different conclusions were
obtained, although the heterogeneity of the analysis was obviously
decreased during the exclusion.
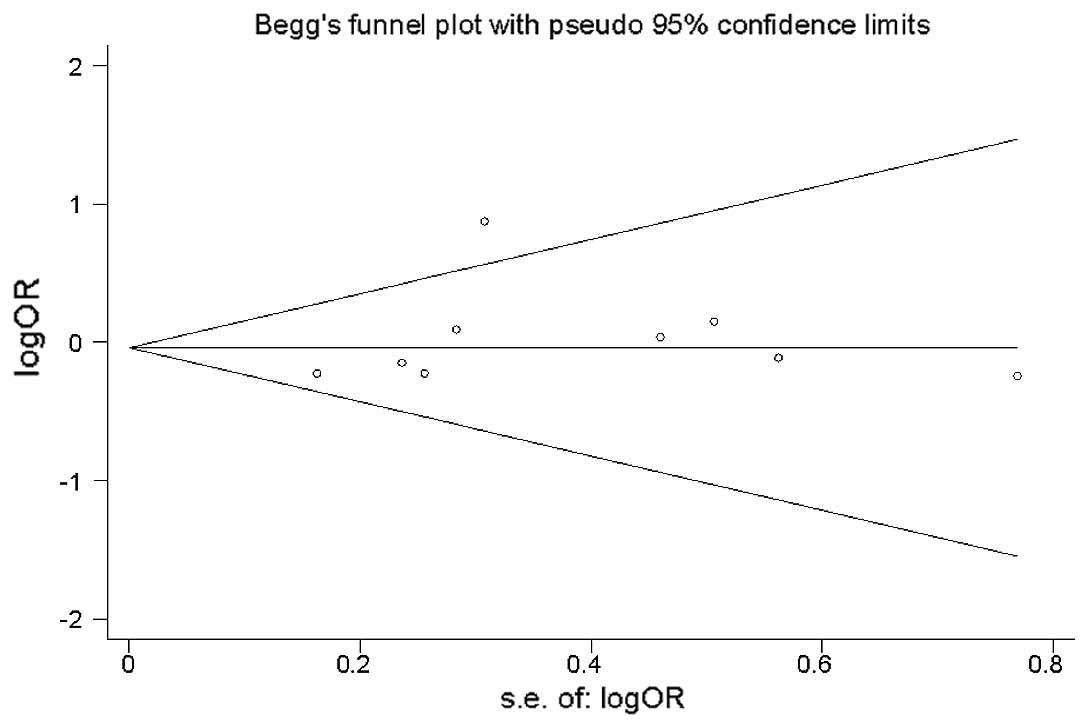
Publication bias test
Begg’s funnel plot and Egger’s test were applied to
assess the publication bias of the studies. No obvious asymmetry
was identified by the Begg’s plots. The funnel plot for ORs of the
recessive model for Glu429Ala (Ala/Ala vs. Ala/Glu + Glu/Glu) was
shown in Fig. 2 as an example.
Furthermore, the results of Egger’s test did not show any evidence
of publication bias (for the Ala222Val polymorphism: P=0.961 for
Val/Val vs. Ala/Ala, 0.558 for Val/Ala vs. Ala/Ala, 0.884 for the
recessive genetic model and 0.810 for the dominant genetic model;
for the Glu429Ala polymorphism: P=0.468 for Ala/Ala vs. Glu/Glu,
0.457 for Ala/Glu vs. Glu/Glu, 0.440 for the recessive genetic
model and 0.362 for the dominant genetic model, respectively).
Discussion
The MTHFR Ala222Val and Glu429Ala polymorphisms have
been found to be a risk factor for a variety of cancers including
colon cancer (11), acute
lymphoblastic leukemia (12),
gastric cancer (13) and head and
neck squamous cell carcinoma (14).
As for bladder cancer, several epidemiological studies (5–7,
18–27) have been investigated for their
association with cancer risk. However, the results are not
conclusive due to small sample-sized association studies that lack
statistical power. In the current meta-analysis, a more precise
estimation of MTHFR Ala222Val and Glu429Ala and bladder cancer was
derived by including a pooled total of 3,463 cases and 3,927
controls for Ala222Val in 11 studies and 3,177 cases and 3,502
controls for Glu429Ala in 9 studies.
The data showed that the Ala222Val and Glu429Ala
polymorphisms were not significantly associated with bladder cancer
susceptibility in the entire population. Furthermore, the role of
Ala222Val and Glu429Ala polymorphism was evaluated in different
subgroups (Chinese, European, American and individuals of Middle
Eastern descent), and the results indicated that the Ala222Val
polymorphism was not significantly associated with bladder cancer
risk in any of the genetic models. Notably, Glu429Ala polymorphism
was significantly associated with bladder cancer risk in
individuals of Middle Eastern descent. Individuals of Middle
Eastern descent who had the Ala/Ala allele were ~82% more likely to
have bladder cancer than those who had Ala/Glu or Glu/Glu genotype.
Our results suggest that the Glu429Ala polymorphism was not
significantly associated with bladder cancer risk in individuals of
Chinese, European or American descent. The reason may be attributed
to genetic and environmental factors. Since cancer is a complicated
multi-genetic disease, different genetic backgrounds may contribute
to the discrepancy that the same polymorphisms play different roles
among different ethnic populations (28).
As a potential problem when interpreting the results
of all meta-analyses (29),
heterogeneity was reduced in this study. Significant between-study
heterogeneity existed in the Val/Val vs. Ala/Ala and dominant
genetic models of the Ala222Val polymorphism, as well as Ala/Ala
vs. Glu/Glu, Ala/Glu vs. Glu/Glu and the dominant genetic model for
the Glu429Ala polymorphism when all studies were pooled. Following
the subgroup analyses by source of control, the heterogeneity among
the Val/Val vs. Ala/Ala and dominant genetic models of the
Ala222Val polymorphism arose from the hospital-based subgroup. By
contrast, heterogeneity of the Ala/Ala vs. Glu/Glu, Ala/Glu vs.
Glu/Glu and dominant genetic models of the Glu429Ala polymorphism
arose from hospital-based subgroups, as well as from ethnicity,
which was effectively decreased in the Chinese, European and
American subgroup analyses. There are two reasons for the
heterogeneity: i) hospital-based controls did not represent the
entire population and ii) differences of genetic backgrounds and
environmental factors potentially exist among different ethnical
subgroups.
The associations between the Ala222Val and Glu429Ala
polymorphisms and bladder cancer risk have been previously studies.
For the variant genotype of Ala222Val polymorphism, Lin et
al (5), Cai et al
(23) and Wang et al
(25) reported that it was
associated with a higher risk of bladder cancer. Safarinejad et
al (27) reported that the
polymorphism was not associated with bladder cancer but was
associated with increased risk of muscle-invasive bladder cancer.
By contrast, Moore et al (19) reported conflicting results,
suggesting a lower risk of bladder cancer was observed in
individuals carrying either the Ala/Val or Val/Val genotype
compared to those carrying the Ala/Ala genotype. The remaining 6
studies reported that there were no statistically significant
associations between the Ala222Val polymorphism and bladder cancer
risk (6–7,18,20–21,26).
For the variant genotypes of Glu429Ala polymorphism, Rouissi et
al (6) reported that it was
associated with a higher risk of bladder cancer. However,
Safarinejad et al (27)
reported that it was not associated with bladder cancer but
associated with increased risk of muscle-invasive bladder cancer.
The remaining 7 studies reported that there were no statistically
significant associations between the Glu429Ala polymorphism and
bladder cancer risk (5,7,19–21,23,25).
Although Wang et al (25) previously published a case-control
study with meta-analysis, in which the data included were up to
2007 and 7 case-control studies were analyzed with conclusions
suggesting no significant associations between Ala222Val and
Glu429Ala polymorphisms and bladder cancer risk, which was in
accordance with results of this meta-analysis. However, in the
demographic characteristics of that study (25), all the cases and controls of
different studies, including individuals from the USA, Argentina
and Tunis (mistaken for Turkey in that study) were considered
Caucasian, rendering the subgroup analyses by ethnicity impossible,
thereby discounting the statistical power of analysis for the
estimation of genetic effects. In the present study, the Glu429Ala
polymorphism was found to be significantly associated with
increased bladder cancer risk in individuals of Middle Eastern
descent.
Given the data was abstracted from these
publications, there are some limitations that should be addressed
with regard to this meta-analysis. Firstly, the ethnicity of the
cases and controls were not uniformly defined. The Glu429Ala
polymorphism for the Middle Eastern individuals, which was found to
be significant, had only 2 publications with 343 cases and 507
controls in total. Secondly, the controls may not truly represent
the populations, since most of the controls included in this study
were hospital-based controls and the Ala222Val and Glu429Ala
polymorphism is known to be potentially associated with other
diseases. Thirdly, some of the environmental risk factors of
bladder cancer, such as cigarette smoking habits and occupational
exposure were not uniformly provided by the original studies.
Furthermore, some inevitable publication bias might exist in the
publications. Therefore, the results of this study should be
interpreted with caution and additional studies with a large amount
of data are needed for evaluation.
In conclusion, the results of the present
meta-analysis suggest that heterozygous and homozygous variant
carriers of the MTHFR Glu429Ala polymorphism are significantly
associated with increased bladder cancer risk in individuals of
Middle Eastern descent, with no evidence of an association between
this polymorphism and bladder cancer risk in individuals of
Chinese, European and American descent. Since the Ala/Ala genotype
is relatively infrequent in the population, more well-designed
studies with larger sample sizes are required to confirm the
findings of the present study.
Acknowledgements
The study was supported by the National Natural
Science Foundation of China (grant nos. 81101536 and 81201565), the
Program of the Pearl River Young Talents of Science and Technology
in Guangzhou, China (no. 2011J2200070) and the Specialized Research
Fund for the Doctoral Program of Higher Education (nos.
20104433120001 and 20124433120001).
References
|
1
|
Jemal A, Bray F, Center MM, Ferlay J, Ward
E and Forman D: Global cancer statistics. CA Cancer J Clin.
61:69–90. 2011. View Article : Google Scholar
|
|
2
|
Ploeg M, Aben KK and Kiemeney LA: The
present and future burden of urinary bladder cancer in the world.
World J Urol. 27:289–293. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Chu H, Wang M and Zhang Z: Bladder cancer
epidemiology and genetic susceptibility. J Biomed Res. 27:170–178.
2013. View Article : Google Scholar
|
|
4
|
Cordon-Cardo C: Molecular alterations
associated with bladder cancer initiation and progression. Scand J
Urol Nephrol Suppl. 154–165. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lin J, Spitz MR, Wang Y, et al:
Polymorphisms of folate metabolic genes and susceptibility to
bladder cancer: a case-control study. Carcinogenesis. 25:1639–1647.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Rouissi K, Ouerhani S, Oliveira E, et al:
Polymorphisms in one-carbon metabolism pathway genes and risk for
bladder cancer in a Tunisian population. Cancer Genet Cytogenet.
195:43–53. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Moore LE, Malats N, Rothman N, et al:
Polymorphisms in one-carbon metabolism and trans-sulfuration
pathway genes and susceptibility to bladder cancer. Int J Cancer.
120:2452–2458. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Bailey LB: Folate, methyl-related
nutrients, alcohol, and the MTHFR 677C→T polymorphism affect cancer
risk: intake recommendations. J Nutr. 133(Suppl 1): S3748–S3753.
2003.PubMed/NCBI
|
|
9
|
Frosst P, Blom HJ, Milos R, et al: A
candidate genetic risk factor for vascular disease: a common
mutation in methylenetetrahydrofolate reductase. Nat Genet.
10:111–113. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Weisberg I, Tran P, Christensen B, Sibani
S and Rozen R: A second genetic polymorphism in
methylenetetrahydrofolate reductase (MTHFR) associated with
decreased enzyme activity. Mol Genet Metab. 64:169–172. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Yin G, Kono S, Toyomura K, et al:
Methylenetetrahydrofolate reductase C677T and A1298C polymorphisms
and colorectal cancer: the Fukuoka Colorectal Cancer Study. Cancer
Sci. 95:908–913. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Tong N, Fang Y, Li J, et al:
Methylenetetrahydrofolate reductase polymorphisms, serum
methylenetetrahydrofolate reductase levels, and risk of childhood
acute lymphoblastic leukemia in a Chinese population. Cancer Sci.
101:782–786. 2010. View Article : Google Scholar
|
|
13
|
Boccia S, Gianfagna F, Persiani R, et al:
Methylenetetrahydrofolate reductase C677T and A1298C polymorphisms
and susceptibility to gastric adenocarcinoma in an Italian
population. Biomarkers. 12:635–644. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Galbiatti AL, Ruiz MT, Rodrigues JO, et
al: Polymorphisms and haplotypes in methylenetetrahydrofolate
reductase gene and head and neck squamous cell carcinoma risk. Mol
Biol Rep. 39:635–643. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Mantel N and Haenszel W: Statistical
aspects of the analysis of data from retrospective studies of
disease. J Natl Cancer Inst. 22:719–748. 1959.PubMed/NCBI
|
|
16
|
DerSimonian R and Laird N: Meta-analysis
in clinical trials. Control Clin Trials. 7:177–188. 1986.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Egger M, Davey Smith G, Schneider M and
Minder C: Bias in meta-analysis detected by a simple, graphical
test. BMJ. 315:629–634. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kimura F, Florl AR, Steinhoff C, et al:
Polymorphic methyl group metabolism genes in patients with
transitional cell carcinoma of the urinary bladder. Mutat Res.
458:49–54. 2001.PubMed/NCBI
|
|
19
|
Moore LE, Wiencke JK, Bates MN, Zheng S,
Rey OA and Smith AH: Investigation of genetic polymorphisms and
smoking in a bladder cancer case-control study in Argentina. Cancer
Lett. 211:199–207. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Sanyal S, Festa F, Sakano S, et al:
Polymorphisms in DNA repair and metabolic genes in bladder cancer.
Carcinogenesis. 25:729–734. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Karagas MR, Park S, Nelson HH, et al:
Methylenetetrahydrofolate reductase (MTHFR) variants and bladder
cancer: a population-based case-control study. Int J Hyg Environ
Health. 208:321–327. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ouerhani S, Oliveira E, Marrakchi R, et
al: Methylenetetrahydrofolate reductase and methionine synthase
polymorphisms and risk of bladder cancer in a Tunisian population.
Cancer Genet Cytogenet. 176:48–53. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Cai DW, Liu XF, Bu RG, et al: Genetic
polymorphisms of MTHFR and aberrant promoter hypermethylation of
the RASSF1A gene in bladder cancer risk in a Chinese population. J
Int Med Res. 37:1882–1889. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Ouerhani S, Rouissi K, Marrakchi R, et al:
Combined effect of NAT2, MTR and MTHFR genotypes and tobacco on
bladder cancer susceptibility in Tunisian population. Cancer Detect
Prev. 32:395–402. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Wang M, Zhu H, Fu G, Wang M and Zhang Z,
Lu Q, Wang S and Zhang Z: Polymorphisms of
methylenetetrahydrofolate reductase and methionine synthase genes
and bladder cancer risk: a case-control study with meta-analysis.
Clin Exp Med. 9:9–19. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Chung CJ, Pu YS, Su CT, et al:
Polymorphisms in one-carbon metabolism pathway genes, urinary
arsenic profile, and urothelial carcinoma. Cancer Causes Control.
21:1605–1613. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Safarinejad MR, Shafiei N and Safarinejad
S: Genetic susceptibility of methylenetetrahydrofolate reductase
(MTHFR) gene C677T, A1298C, and G1793A polymorphisms with risk for
bladder transitional cell carcinoma in men. Med Oncol. 28(Suppl 1):
S398–S412. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Hirschhorn JN, Lohmueller K, Byrne E and
Hirschhorn K: A comprehensive review of genetic association
studies. Genet Med. 4:45–61. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Munafo MR and Flint J: Meta-analysis of
genetic association studies. Trends Genet. 20:439–444. 2004.
View Article : Google Scholar : PubMed/NCBI
|