Introduction
Merosin-deficient congenital muscular dystrophy type
1A (MDC1A) is characterized by early onset in infancy of critical
muscle weakness, high creatine kinase (CK) levels, and diffuse
white matter changes in the brain. Being non-invasive, muscle
magnetic resonance imaging (MRI) is useful in the diagnosis and
follow-up of patients with MDC1A. Because MDC1A is characterized by
changes in white matter, most patients with this disease are
analyzed by brain MRI. To the best of the authors' knowledge, there
are few studies of patients with MDC1A that have involved muscle
MRI. This report describes a patient with MDC1A who was analyzed by
muscle MRI, and reviews studies summarizing characteristics of
muscle MRI in patients with MDC1A.
Case report
A 1-year-old girl, born at gestational age 39 weeks
and 5 days by natural labor, presented with a 1-year history of
central hypotonia and proximal weakness on March 27, 2015, when
admitted to hospital (The First Affiliated Hospital of Sun Yat-Sen
University, Guangzhou, China). As an infant, she had a weak cry and
floppy limbs. Her developmental milestones were delayed; she first
raised her head at the age of 8 months and first sat independently
at the age of 9 months. However, she was unable to hold her head
while sitting and has been unable to stand or walk, even with the
help of her parents. Her intellectual and speech development was
normal, and her family history was negative for this or a similar
condition.
The study protocol was approved by the Ethics
Committee of Sun Yat-Sen University (Guangzhou, China), and the
patient's family provided written informed consent for publication
of the present study.
Physical examination
Physical examination presented myopathic facies and
a single crease of the right palm, the latter also observed in her
father. Her intellectual and language function was normal. She
could sit without support but could not walk or stand, and her neck
was too floppy for her to hold her head up while sitting. No muscle
atrophy or pseudohypertrophy was observed. Both her upper and lower
limbs reported hypotonia and weakness, which was more proximal than
distal and predominant in her shoulder and pelvic girdle. Muscle
assessment using the standard Medical Research Council scale (grade
0–5) indicated that muscle strength of her four limbs from proximal
to distal was 3/5, 3/5, 4/5 and 4/5, respectively (1). Sensory examination could not be completed
due to patient noncooperation. Her tendon reflexes and Babinski's
sign were negative.
Serum CK levels
Her serum CK levels at ages 3 and 8 months and one
year were 2,959, 1,621 and 1,659 U/l, respectively. At age 1 year,
her blood ammonia concentration was 73.4 mmol/l and her resting
state blood lactic acid concentration was 1.3 mmol/l. Urine and
blood screenings for hereditary metabolic diseases were
unremarkable.
Ultrasound cardiography
Ultrasound cardiography reported patent foramen
ovale at age 1 day, but normal results at age 1 year.
MRI
Brain MRI performed at age 3 months presented
symmetrical, mild T1WI low, mild T2WI and FLAIR high radial pattern
signals in the white matter of the Cornu posterius of the
ventricular lateral. The cortices, ventricles, cerebellum and basal
ganglia were normal.
Muscle MRI performed at age 1 year presented wide
spread abnormalities in the muscle groups of the lower legs,
including thigh and pelvis degeneration, infiltration and fiber
edema. The bilateral posterior tibial, soleus, gastrocnemius and
anterior tibial muscles reported abnormal patterns, including high
signal intensity on T1WI and T2WI and isointensity or
hyperintensity on T2WI-SPAIR. Among the lower leg muscles, the
soleus revealed T2WI-SPAIR hyperintensity (Fig. 1A-1, A-2 and A-3). The bilateral vastus
internus, vastus medialis, vastus lateralis, rectus femoris, biceps
femoris, adductor magnus, semitendinosus and semimembranosus
muscles were atrophied, with T1WI and T2WI showing isointensity or
hyperintensity. In contrast, T2WI-SPAIR presented isointensity of
some muscles, whereas others, including the vastus medialis and
vastus lateralis muscles, showed hyperintensity (Fig. 1B-1, B-2 and B-3). The bilateral gluteus
maximus, gluteus medius and gluteus minimus muscles were atrophied
with T1WI, T2WI and T2WI-SPAIR muscle MRI presenting pinnate
patterns of abnormal hyperintensity (Fig.
1C-1, C-2 and C-3). The bilateral erector spinae muscles showed
hyperintensity on T1WI and T2WI and isointensity on T2WI-SPAIR
(Fig. 1D-1, D-2 and D-3).
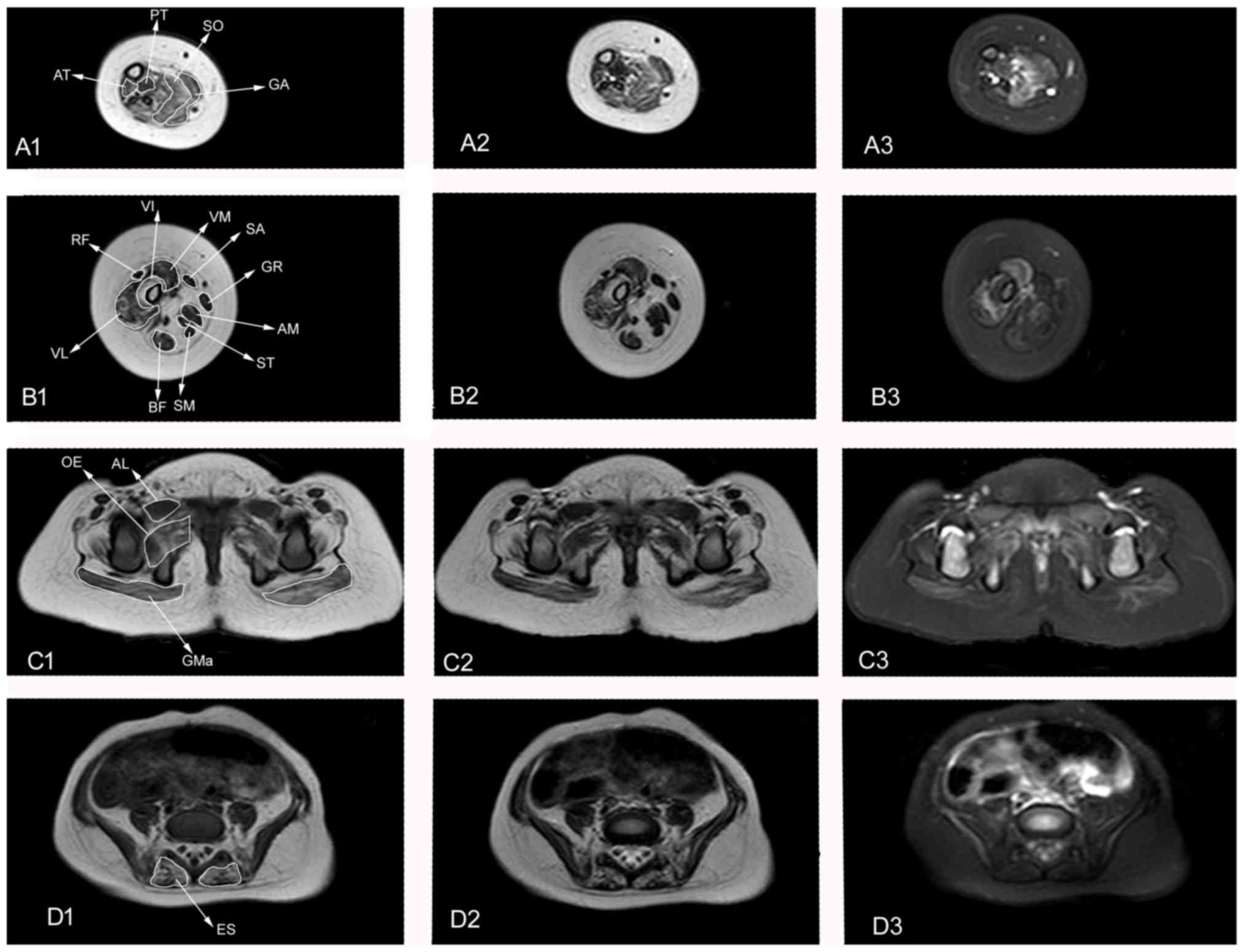 | Figure 1.Muscle MRI of the patient at 1 year of
age. Axial T1WI, T2WI and T2WI SPAIR images of the lower leg, thigh
and pelvis. (A) 1–3: Lower leg muscle MRI presenting PT, SO, GA,
and AT fatty infiltration and edema. (B) 1–3: Thigh muscle MRI
presenting VI, VM, VL, BF, AM, ST and SB atrophy and fatty
infiltration. VM and VL present edema. (C) 1–3 and (D) 1–3: Pelvis
muscle MRI presenting GMa atrophy (C1-3); GMa, OE and ES fatty
infiltration (C1-3, D 1–3); and GMa, AL and OE edema (C1-3, D 1–3).
MRI, magnetic resonance imaging; WI, weighted image; PT, posterior
tibial; SO, soleus; GA, gastrocnemius; AT, anterior tibial; VI,
vastus internus; VM, vastus medialis; SA, sartorius; GR, gracilis;
AM, adductor magnus; ST, semitendinosus; SM, semimembranosus; BF,
biceps femoris; VL, vastus lateralis; RF, rectus femoris; GMa,
gluteus maximus; GP, greater psoas; OE, obturator externus; AL,
adductor longus; ES, erector spinae. |
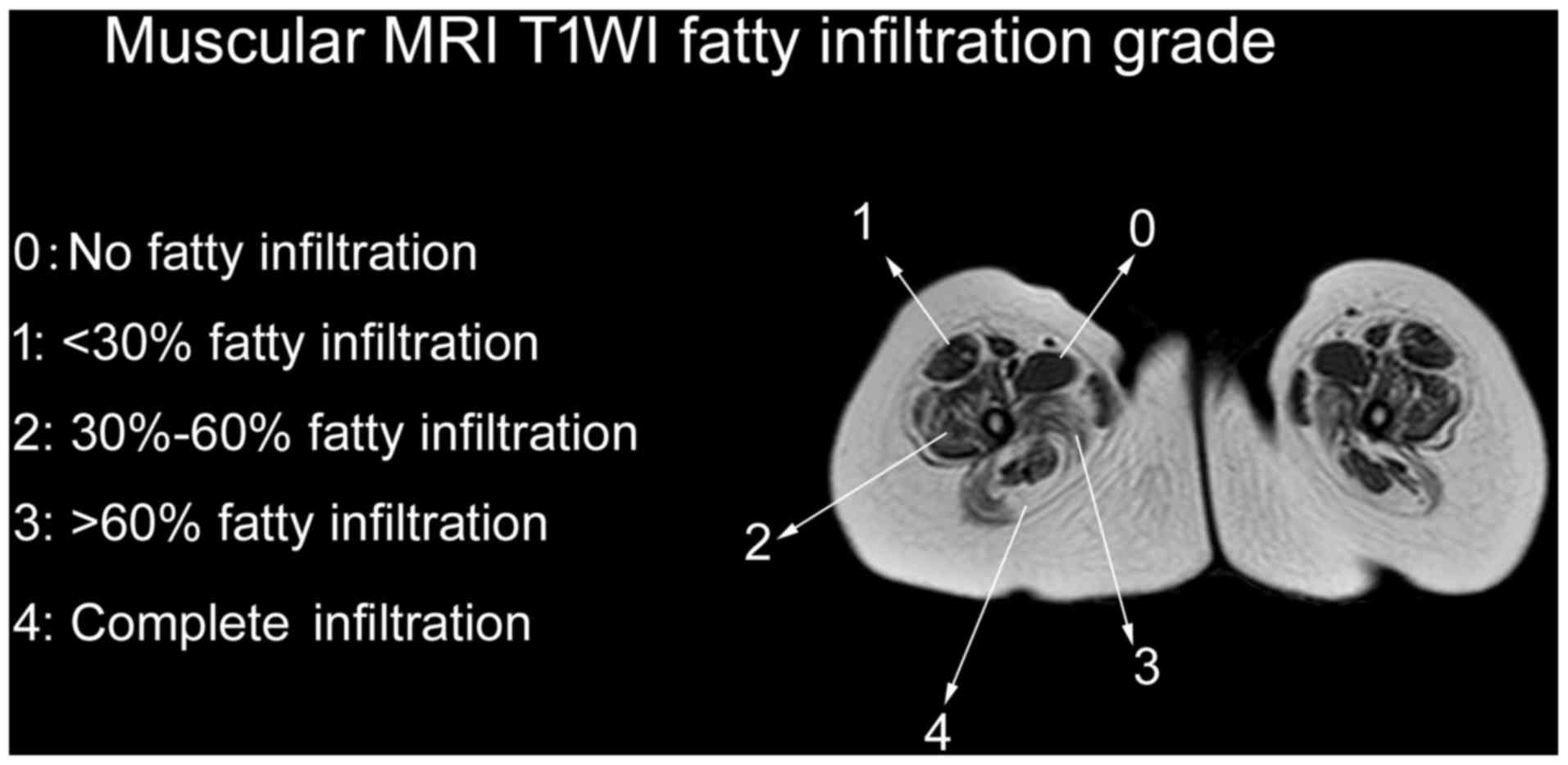
Fatty infiltration of muscles was assessed by the
Mercuri scale, as modified by Fischer et al (2) (Fig. 1). A
total of 28 muscles were assessed, including four lower leg muscles
(gastrocnemius, soleus, posterior tibial and anterior tibial), 11
thigh muscles (adductor magnus, gracilis, adductor longus,
sartorius, rectus femoris, vastus internus, vastus medialis, vastus
lateralis, biceps femoris, semitendinosus and semimembranosus) and
13 pelvis muscles (gluteus maximus, gluteus medius, gluteus
minimus, iliopsoas, piriformis, obturator internus, adductor
brevis, obturator externus, tensor fasciaelatae, pectineus, erector
spinae, psoas major and iliacus). Six muscles (piriformis,
obturator internus, pectineus, adductor longus, adductor brevis and
sartorius) were identified to be grade 0, eight (iliopsoas, psoas
major, iliacus, rectus femoris, semitendinosus, semimembranosus,
gracilis and posterior tibial) were grade 1, four (gluteus minimus,
obturator externus, vastus medialis and biceps femoris) were grade
2, ten (gluteus maximus, gluteus medius, tensor fasciae latae,
erector spinae, vastus lateralis, vastus internus, adductor magnus,
gastrocnemius, soleus and anterior tibial) were grade 3, and none
were grade 4.
Molecular genetic testing
Genomic DNA from the patient was extracted from
peripheral blood leukocytes and high-throughput sequencing
(3–5) was
performed to test abnormalities in 63 genes associated with
neuromuscular disorders. The patient was found to have a
heterozygous frame-shift mutation in the LAMA2 gene, in which the
nucleotides AG at positions 2049–2050were deleted (LAMA2
c.2049_2050delAG), resulting in early protein termination
[p.(Arg683fs)]. Multiplex polymerase chain reaction of the LAMA2
gene of her parents' DNA indicated that her father had the same
mutation, whereas her mother was normal. These findings confirmed
the diagnosis of congenital MDC1A.
Discussion
MDC1A, originally described in 1994 (6), was shown to result from mutations in the
laminin-α2 gene (LAMA2), which encodes the extracellular matrix
protein merosin. Most mutations detected to date have been nonsense
and splicing site point mutations and frame shift mutations
(7). The absence of merosin results in
early weakness, delayed development milestones, high blood levels
of CK and normal cognition with white matter abnormalities on brain
MRI (8,9).
The present study encountered a 1-year old girl who
presented with congenital hypotonia, delayed motor milestones and
weakness. Muscle MRI revealed fatty infiltration and edema of
selected muscles. Testing of myodystrophy genes confirmed the
diagnosis of MDC1A. Muscle MRI, a noninvasive method of assessing
the extent of muscle damage, has become a very useful tool in the
diagnosis and follow-up of patients with muscle diseases, including
muscular dystrophy, inflammatory myopathies and metabolic
myopathies (10,11). Muscle MRI may be under-utilized in
patients with MDC1A.
Similar to the MRI manifestations of other types of
muscular dystrophy (12–14), fatty infiltration is the major abnormal
pattern observed in MDC1A. The patient demonstrated obvious fatty
infiltration into muscles of the pelvis, thigh and lower leg. The
muscles most commonly involved during the early stages of disease
included the gluteus maximus, gluteus medius, erector spinae,
proximal vastus intermedius, proximal vastus lateralis, adductor
magnus, soleus, anterior tibial and gastrocnemius muscles (15). On T1WI, these muscles had a fatty
infiltration grade of 3. The T1WI fatty infiltration grade was
higher for the proximal than the distal quadriceps femoris, being
grades 2–3 for the proximal and grades 1–2 for the distal vastus
intermedius, vastus lateralis and vastus medialis muscles.
Involvement of the piriformis, obturator internus, pectineus,
adductor longus, adductor brevis and sartorius muscles was
relatively uncommon until the terminal stage of disease. In the
patient, the vastus intermedius, vastus lateralis, vastus medialis
and rectus femoris muscles had fatty infiltration grades of 3, 3, 2
and 1, respectively. The vastus intermedius demonstrated earliest
involvement, followed by the vastus lateralis and medialis muscles.
Similar radiological features have been observed in patients with
COL6 Ullrich and laminopathy, which is caused by mutations in genes
encoding extracellular matrix proteins (15). The tested patient presented involvement
of the erector spinae muscle at the onset of MDC1A (Fig. 2D-1, D-2 and D-3) with a fatty
infiltration grade of 3 on T1WI. Involvement of paraspinal muscles
at the onset of disease has been observed in patients with other
muscle diseases, including rigid spine muscular dystrophy and
congenital muscular dystrophy and spinal rigidity (16,17). In
contrast to Duchenne muscular dystrophy, pseudohypertrophy
(18,19)
is not commonly observed during the progression of MDC1A. Rather,
muscular atrophy was indicated to occur early in the patient,
including atrophy of the gluteus maximus, quadriceps femoris,
biceps, adductor magnus, semitendinosus and semimembranosus
muscles.
MDC1A is the most common form of congenital muscular
dystrophy. Most patients with MDC1A are too young to undergo muscle
biopsy. Muscle MRI, an additional tool in the differential
diagnosis of muscle disorders, can help patients delay muscle
biopsy. The findings in our patient indicate that the muscle MRI
features of MDC1A include: i) Fatty infiltration as the major
pattern; ii) common involvement of the gluteus maximus, erector
spinae, vastus intermedius, vastus lateralis, adductor magnus,
soleus and gastrocnemius muscles; iii) mild or no involvement of
the piriformis, obturator internus, pectineus, adductor longus,
adductor brevis and sartorius muscles; iv) fatty infiltration into
the erector spinae during the early stage of disease; and v) onset
of muscle atrophy at the onset of the disease. Additional study is
required, including of patients at different clinical stages.
References
|
1
|
Paternostro-Sluga T, Grim-Stieger M, Posch
M, Schuhfried O, Vacariu G, Mittermaier C, Bittner C and
Fialka-Moser V: Reliability and validity of the Medical Research
Council (MRC) scale and a modified scale for testing muscle
strength in patients with radial palsy. J Rehabil Med. 40:665–671.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Fischer D, Kley RA, Strach K, Meyer C,
Sommer T, Eger K, Rolfs A, Meyer W, Pou A, Pradas J, et al:
Distinct muscle imaging patterns in myofibrillar myopathies.
Neurology. 71:758–765. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Li H and Durbin R: Fast and accurate
long-read alignment with Burrows-Wheeler transform. Bioinformatics.
26:589–595. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Zhang L, Zhang J, Yang J, Ying D, Lau YL
and Yang W: PriVar: a toolkit for prioritizing SNVs and indels from
next-generation sequencing data. Bioinformatics. 29:124–125. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Yang Y, Muzny DM, Reid JG, Bainbridge MN,
Willis A, Ward PA, Braxton A, Beuten J, Xia F, Niu Z, et al:
Clinical whole-exome sequencing for the diagnosis of mendelian
disorders. N Engl J Med. 369:1502–1511. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tomé FM, Evangelista T, Leclerc A, Sunada
Y, Manole E, Estournet B, Barois A, Campbell KP and Fardeau M:
Congenital muscular dystrophy with merosin deficiency. C R AcadSci
III. 317:351–357. 1994.
|
|
7
|
Xiong H, Tan D, Wang S, Song S, Yang H,
Gao K, Liu A, Jiao H, Mao B, Ding J, et al: Genotype/phenotype
analysis in Chinese laminin-α2 deficient congenital muscular
dystrophy patients. Clin Genet. 87:233–243. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Fardeau M, Tomé FM, Helbling-Leclerc A,
Evangelista T, Ottolini A, Chevallay M, Barois A, Estournet B,
Harpey JP, Fauré S, et al: Congenital muscular dystrophy with
merosin deficiency: Clinical, histopathological, immunocytochemical
and genetic analysis. Rev Neurol (Paris). 152:11–19. 1996.(In
French). PubMed/NCBI
|
|
9
|
Incecik F, Herguner OM, Ceylaner S and
Altunbasak S: Merosin-negative congenital muscular dystrophy:
Report of five cases. J Pediatr Neurosci. 10:346–349. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Peters SA, Kohler C, Schara U, Hohendahl
J, Vorgerd M, Nicolas V and Heyer CM: Museular magnetic resonance
imaging for evaluation of myopathies in children. Klin Padiatr.
220:37–46. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Cejas CP, Serra MM, Galvez DFG, Cavassa
EA, Taratuto AL, Vazquez GA, Massaro MEL and Schteinschneider AV:
Muscle MRI in pediatrics: Clinical, pathological and genetic
correlation. Pediatr Radiol. 47:724–735. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Díaz-Manera J, Llauger J, Gallardo E and
Illa I: Muscle MRI in muscular dystrophies. Acta Myol. 34:95–108.
2015.PubMed/NCBI
|
|
13
|
Polavarapu K, Manjunath M, Preethish-Kumar
V, Sekar D, Vengalil S, Thomas P, Sathyaprabha TN, Bharath RD and
Nalini A: Muscle MRI in Duchenne muscular dystrophy: Evidence of a
distinctive pattern. Neuromuscul Disord. 26:768–774. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Fatehi F, Salort-Campana E, Le Troter A,
Bendahan D and Attarian S: Muscle MRI of facioscapulohumeral
dystrophy (FSHD): A growing demand and a promising approach. Rev
Neurol (Paris). 172:566–571. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Harris E, McEntagart M, Topf A, Lochmüller
H, Bushby K, Sewry C and Straub V: Clinical and neuroimaging
findings in two brothers with limb girdle muscular dystrophy due to
LAMA2 mutations. Neuromuscul Disord. 27:170–174. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Mercuri E, Clements E, Offiah A,
Pichiecchio A, Vasco G, Bianco F, Berardinelli A, Manzur A, Pane M,
Messina S, et al: Muscle magnetic resonance imaging involvement in
muscular dystrophies with rigidity of the spine. Ann Neurol.
67:201–208. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Flanigan KM, Kerr L, Bromberg MB, Leonard
C, Tsuruda J, Zhang P, Gonzalez-Gomez I, Cohn R, Campbell KP and
Leppert M: Congenital muscular dystrophy with rigid spine syndrome:
A clinical, pathological, radiological, and genetic study. Ann
Neurol. 47:152–161. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Godi C, Ambrosi A, Nicastro F, Previtali
SC, Santarosa C, Napolitano S, Iadanza A, Scarlato M, Sora MG
Natali, Tettamanti A, et al: Longitudinal MRI quantification of
muscle degeneration in Duchenne muscular dystrophy. Ann Clin Transl
Neurol. 3:607–622. 2016. View
Article : Google Scholar : PubMed/NCBI
|
|
19
|
Vohra RS, Lott D, Mathur S, Senesac C,
Deol J, Germain S, Bendixen R, Forbes SC, Sweeney HL, Walter GA, et
al: Magnetic resonance assessment of hypertrophic and
pseudo-hypertrophic changes in lower leg muscles of boys with
Duchenne muscular dystrophy and their relationship to functional
measurements. PLoS One. 10:e01289152015. View Article : Google Scholar : PubMed/NCBI
|