Introduction
Polycystic ovarian syndrome (PCOS) is an endocrine
disorder that occurs in women of reproductive age (1). According to the Rotterdam guidelines,
diagnosis with PCOS requires the presence of at least two of the
following; irregular periods, increased androgen secretion and/or
polycystic ovaries (2). Although not
included in the diagnostic criteria, the majority of women with
PCOS are insulin resistant (3).
Insulin resistance (IR) in women with PCOS increases their risk of
type 2 diabetes mellitus and other co-morbidities (3). Furthermore, IR in these women appears to
contribute to PCOS development (4).
Indeed, weight loss (known to increase insulin sensitivity) is
associated with a reduction in PCOS co-morbidities or even disease
resolution (5).
In addition to the dysregulation of insulin
levels/activity, IR is associated with altered levels of a number
of other hormones including adiponectin (6), leptin (7)
and irisin (8). It is therefore
unsurprising that IR causes dysregularities in carbohydrate, fat
and protein metabolism. For example, homocysteine and the
branched-chain amino acids (BCAAs) (isoleucine, leucine and valine)
are often elevated in the serum of individuals with increased IR
(9,10). The function of homocysteine in IR has
received attention recently as it is atherogenic and prothrombotic
and may contribute to the increased prevalence of cardiovascular
complications in individuals with IR (11).
Homocysteine is synthesized from methionine
(12). Once formed, homocysteine may
be methylated back into methionine through a reaction that requires
5-methyltetrahydrofolate (5-MTHF) and the methylcobalamin form of
vitamin B12 (12).
Alternatively, through a transsulfuration reaction, the sulfur
group of homocysteine may be transferred to serine to form cysteine
and α-ketobutyrate (12).
Transsulfuration of homocysteine requires the activity of two
enzymes; cystathionine synthase and cystathionine lyase (12). The above two enzymes use a
pyridoxal-phosphate (i.e., vitamin B6) as a cofactor
(13). Increased insulin levels, a
feature of IR, are believed to raise homocysteine levels by
inhibiting the activity of the hepatic cystathionine synthase
(14). However, the exact mechanism
underlying the association between IR and higher homocysteine
levels is yet to be completely understood.
Homocysteine levels in the blood may additionally be
influenced by the activity of the enzyme methylenetetrahydrofolate
reductase (MTHFR), the rate-limiting enzyme of the methyl cycle
(15). MTHFR catalyzes the conversion
of 5,10-methylenetetrahydrofolate to 5-MTHF, a co-substrate of the
reaction that converts homocysteine to methionine (15). This explains why individuals that have
MTHFR variants with low activity levels often have higher
homocysteine levels (15). One of the
most commonly investigated variants of MTHFR is caused by a single
nucleotide polymorphism in the coding region ‘C677T’ (16). Higher homocysteine levels caused by
this variant may thus increase the risk of PCOS.
Given the association between IR and PCOS and the
association between hyperinsulinemia and increased levels of blood
homocysteine, previous studies have investigated the association
between PCOS and homocysteine with conflicting results (17–19). In
the present study, the association between homocysteine, the C677T
MTHFR variant was assessed in individuals with PCOS in a Jordanian
population. The strength of the association of homocysteine with
PCOS relative to other metabolites known to be involved with IR
(leptin, adiponectin and BCAAs) were additionally assessed.
Materials and methods
Study design and patients
This was a prospective frequency matched
case-control study. The study population was previously used to
establish an association between lower levels of serum adiponectin
and PCOS (20). The project was
ethically approved by the appropriate Institutional Review Boards
(290/2016) affiliated with the Jordan University of Science and
Technology (Irbid, Jordan). Patients provided written informed
consent required for participation in the present study.
Patients with PCOS were recruited from the
Gynecology clinic of the King Abdullah University Hospital (KAUH)
between September 2016 and March 2017. KAUH is a tertiary hospital
affiliated with Jordan University of Science and Technology.
Normally menstruating women were recruited from
other clinics within KAUH provided they met the eligibility
criteria described below. To participate in the study, women with
PCOS had to have been diagnosed with PCOS by at least two
gynecologists from KAUH according to the Rotterdam guidelines
(21). Normally menstruating women
had a regular menstrual cycle in terms of duration and quantity for
at least six months prior to enrollment, and had no clinical or
biochemical signs of hyperandrogenism. Additionally, their ovaries
were free of follicles upon a mandatory ultrasound examination
performed by the study gynecologist. Women who were affected with
any of the following: Cushing's syndrome, syndromes of severe IR,
androgen secreting neoplasms, thyroid dysfunction, congenital
adrenal hyperplasia or hyperprolactinemia were excluded from the
study. The height, weight and age of the patients were recorded at
the time of the patient visit and interview. The following formula:
body mass index (BMI) = weight (kg)/[height (m)]2 was
used for BMI calculation.
A total of 154 women with PCOS (mean age, 23.9±5.1
years old) and 151 normally menstruating women (mean age, 24.2±5.1
years old) agreed to participate in the study. The age range of the
subjects was between 14 and 34 years. The study aimed to detect a
difference of 5 units (equivalent to a small effect size) in
homocysteine between the two groups assuming that the common
standard deviation is 11 and the level of significance (P<0.05)
exceeded 80% (power=93%). The power analysis was calculated using
G*Power software version 3.1.9 (Department of Psychology,
University of Düsseldorf, Düsseldorf, Germany) (22) and Epicalc 2000 software version 1.5
(Prince of Songkla University, Hat Yai, Thailand) (23).
Collection of blood and serum
samples
Blood withdrawal was performed subsequent to an
overnight fast of 12 h. Blood samples were distributed into an EDTA
tube (Al-Hanoof Factory, Amman, Jordan) and a plain tube with gel
clot activator (Al-Hanoof Factory). Blood in the EDTA tubes was
directly used for DNA extraction while blood in the plain tubes was
used for the recovery of serum following centrifugation at 4,000 ×
g for 7 min at room temperature. The recovered serum was stored at
−80°C until it was further used to determine the levels of
homocysteine, 5-MTHF, leptin, adiponectin and BCAAs.
Biochemical measurements
Serum homocysteine, 5-MTHF, leptin and adiponectin
levels were measured using enzyme-linked immunosorbent assay
(ELISA) kits according to the manufacturer's protocol. The
homocysteine ELISA kit was purchased from Cell Biolabs, Inc. (cat
no. STA-670; San Diego, CA, USA), the 5-MTHF ELISA kit was
purchased from Cusabio Technology LLC (cat no. CSB-E17109h;
Houston, TX, USA) while the leptin (cat no. DY398) and adiponectin
(cat no. DY1065) ELISA kits were purchased from R&D Systems,
Inc. (Minneapolis, MN, USA). To measure homocysteine levels, serum
samples were diluted 10-fold. Serum samples were diluted 100-fold
to measure the 5-MTHF and leptin levels, and were diluted
8,000-fold to measure adiponectin levels. All dilutions were
prepared in phosphate buffer saline containing 0.1% bovine serum
albumin (cat no. P3688; Sigma-Aldrich; Merck KGaA, Darmstadt,
Germany).
On the other hand, serum BCAAs levels were measured
using a commercially available kit purchased from Sigma-Aldrich
(Merck KGaA) with leucine used as the standard. The assay used a
coupled enzymatic reaction to determine the concentration of all
three BCAAs, resulting in a colorimetric product. For all ELISAs
performed, the absorbance was measured using an ELx800 microplate
reader (BioTek Instruments, Inc., Winooski, VT, USA). A wavelength
of 450 nm was used for the measurements.
DNA extraction and genotyping
Genomic DNA was purified from blood samples in EDTA
tubes using a QIAamp DNA Blood Mini kit purchased from Qiagen GmbH
(Hilden, Germany) according to the manufacturer's protocol.
Following DNA extraction, the final DNA concentration was measured
spectrophotometrically using an ND-2000 Nanodrop (Thermo Fisher
Scientific, Inc., Waltham, MA, USA). Polymerase chain
reaction-restriction fragment length polymorphism (PCR-RFLP) was
used to genotype the C677T variant of the MTHFR gene. The final
volume of the PCR reaction was 25 µl. The reaction mixture
contained GoTaq® Green Master Mix (Promega Corporation,
Madison, WI, USA), 5 ng DNA and 0.4 µM primers (forward and
reverse). The sequence of the C677T variant of the MTHFR gene
forward primer was 5′-GTCGGTGCATGCCTTCAC′-3 while the sequence of
the reverse primer was 5′-AGCATATCAGTCATGAGCCC′-3. The PCR was run
under the following thermocycling conditions: Initial denaturation
at 95°C for 3 min, followed by 34 cycles of denaturation at 95°C
for 3 min, annealing at 65°C for 30 sec and extension at 72°C for
one min and a final extension at 72°C for 5 min. The above PCR
reaction produced an amplicon 333 bps in length. In order to
genotype the patients for the different genotype categories of
C677T, the above PCR amplicon was digested with TaqαI (New England
BioLabs, Inc., Ipswitch, MA, USA) at 65°C for 1 h. The undigested
PCR amplicons and the products following restriction enzyme
digestion were electrophoresed on 3% agarose gel containing
ethidium bromide (cat no. 1613024; Bio-Rad Laboratories, Inc.,
Hercules, CA, USA). Ultraviolet light was used to visualize the
products. Direct Sanger sequencing was performed at the Princess
Haya Biotechnology Center (KAUH, Irbid, Jordan) to confirm the
genotyping results.
Statistical analysis
The Statistical Package for Social Studies (SPSS)
software version 22 (SPSS, Inc., Chicago, IL, USA) was used to
conduct all statistical analyses. The data were presented as the
mean ± standard deviation. An unpaired Student's t-test was used to
examine if a statistically significant difference was present in
serum homocysteine, 5-MTHF, leptin, adiponectin, BCAAs, age or BMI
between normally menstruating and PCOS women. A Pearson's
χ2 was used to examine if an association existed between
the different genotype categories of C677T with PCOS. To assess if
significant differences existed in homocysteine or 5-MTHF serum
levels between the different genotype classes of MTHFR C677T (CC,
CT or TT), one-way analysis of variance followed by a post hoc
Tukey's test was used.
To assess the strength of the association of
homocysteine with PCOS, multivariate logistic regression analysis
was used with the following variables in the model: Age, BMI,
homocysteine, 5-MTHF, leptin, adiponectin, BCAAs and the C677T
different genotypes. A receiver operating curve (ROC) analysis was
used to evaluate the performance of homocysteine as a diagnostic
test for PCOS. P<0.05 was considered to indicate a statistically
significant difference.
Results
Patient characteristics and
biochemical profiles
A total of 154 PCOS and 151 normally menstruating
women consented to participate in the present study. Their ages
ranged between 14 and 34 years. Fasting serum homocysteine levels
were significantly higher in patients with PCOS compared with
normally menstruating women (P<0.0001; Table I). On the other hand, women with PCOS
had significantly lower levels of fasting leptin (P=0.027),
adiponectin (P=0.010) and 5-MTHF (P=0.024; Table I) compared with normally menstruating
women.
 | Table I.Baseline characteristics of the study
participants. |
Table I.
Baseline characteristics of the study
participants.
| Variable | Normal menstruating
patients | Patients with
PCOS | P-value |
|---|
| Age, years | 24.35±5.10 | 23.85±5.12 | 0.3971 |
| BMI,
kg/m2 | 26.23±5.82 | 26.57±5.98 | 0.5812 |
| BCAAs, µmol/l | 373.68±78.72 | 385.23±89.93 | 0.2423 |
| Leptin, ng/ml |
27.72±22.10 |
22.77±16.15 | 0.0270 |
| Adiponectin,
µg/dl |
7.87±4.79 |
6.61±3.54 | 0.0103 |
| 5-MTHF, ng/ml | 13.79±4.88 | 12.61±3.96 | 0.0243 |
| Homocysteine,
µmol/l | 14.23±5.53 |
29.03±11.80 | <0.0001 |
Associations between homocysteine and
PCOS
The present study aimed to assess whether the serum
homocysteine levels remained significantly associated with PCOS
subsequent to adjusting for other co-variables. To achieve this,
multivariate logistic regression analysis was used and it was
revealed that serum homocysteine increased the risk of and
demonstrated the strongest association with PCOS [P<0.0001; odds
ratio, 1.217; 95% confidence interval (CI), 1.157–1.280; Table II].
| Table II.Multivariate analysis with age, BMI,
BCAA, leptin, adiponectin, 5-MTHF and homocysteine as variables in
the model. |
Table II.
Multivariate analysis with age, BMI,
BCAA, leptin, adiponectin, 5-MTHF and homocysteine as variables in
the model.
| Variable | OR | 95% CI | P-value |
|---|
| Age, years | 0.961 | 0.897–1.029 |
0.2531 |
| BMI,
kg/m2 | 1.072 | 0.993–1.157 |
0.0763 |
| BCAA, µmol/l | 1.000 | 0.995–1.004 |
0.8742 |
| Leptin, ng/ml | 0.960 | 0.934–0.986 |
0.0031 |
| Adiponectin,
µg/ml | 0.984 | 0.899–1.076 |
0.7203 |
| 5-MTHF, ng/ml | 0.954 | 0.884–1.031 |
0.2343 |
| Homocysteine,
µmol/l | 1.217 | 1.157–1.280 | <0.0001 |
Correlation between homocysteine and
5-MTHF
Serum homocysteine levels were expected to be
negatively correlated with 5-MTHF levels. In order to assess this
association, correlation analysis was performed to determine any
correlation between homocysteine and the other variables in the
population (including age, BMI, BCAA, leptin, adiponectin and
5-MTHF levels). The results revealed that a significant negative
correlation existed between homocysteine and 5-MTHF (r=−0.168,
P=0.005), and between homocysteine and adiponectin (r=−0.172,
P=0.004). On the other hand, a positive significant correlation
existed between homocysteine and BCAAs (r=0.149, P=0.012; Table III).
| Table III.Correlation between homocysteine and
other variables. |
Table III.
Correlation between homocysteine and
other variables.
| Variable | Age, years | BMI,
kg/m2 | BCAAs, µmol/l | Leptin, ng/ml | Adiponectin,
µg/ml | 5-MTHF, ng/ml |
|---|
| Homocysteine,
µmol/l |
|
r-value | −0.037 | 0.064 | 0.149 | 0.005 | −0.172 | −0.168 |
|
P-value |
0.530 | 0.283 | 0.012 | 0.934 |
0.004 |
0.005 |
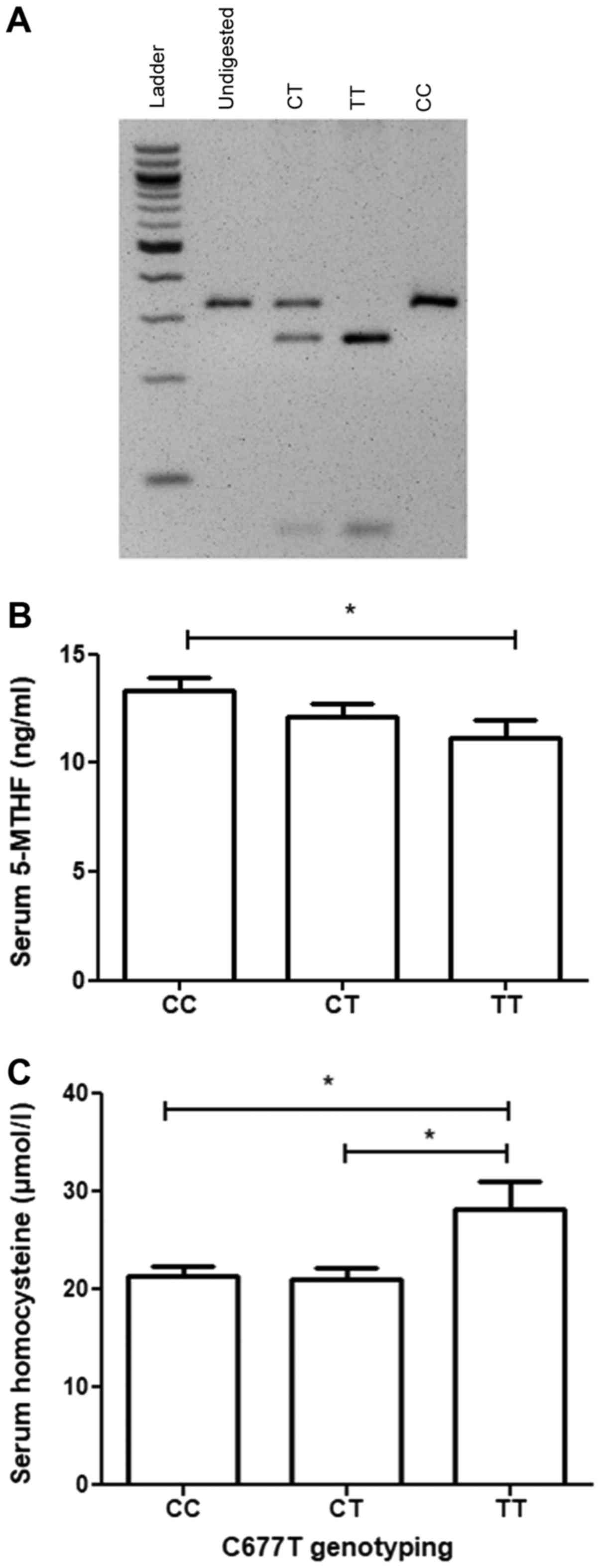
Effect of the MTHFR C677T polymorphism
on the serum levels of homocysteine and 5-MTHF
5-MTHF levels may be affected by the activity of
MTHFR. To assess whether the C677T MTHFR variant that may affect
the activity of MTHF is associated with PCOS and/or affects 5-MTHF
and homocysteine levels, a PCR-RFLP strategy was developed to
genotype the study participants for the C677T MTHFR variant
(Fig. 1A). The results revealed that
the TT genotype of C677T was associated with significantly lower
levels of serum 5-MTHF compared with the CC genotype (P=0.0186;
Fig. 1B). Furthermore, the TT
genotype of C677T was associated with significantly higher levels
of serum homocysteine compared with the CT genotype (P=0.0369) or
the CC genotype (P=0.007; Fig. 1C).
No significant association existed between any of the C677T
genotypes and PCOS (P=0.505; Table
IV).
| Table IV.Genotype frequencies of rs1801133 in
normal menstruating women and women with PCOS. |
Table IV.
Genotype frequencies of rs1801133 in
normal menstruating women and women with PCOS.
| Genotype | Normal menstruating
(n=149) | PCOS (n=154) | P-value |
|---|
| CC | 70
(46.4%) | 77 (50.0%) | 0.505 |
| CT | 69
(45.7%) | 61 (39.6%) |
|
| TT | 12 (7.9%) | 16 (10.4%) |
|
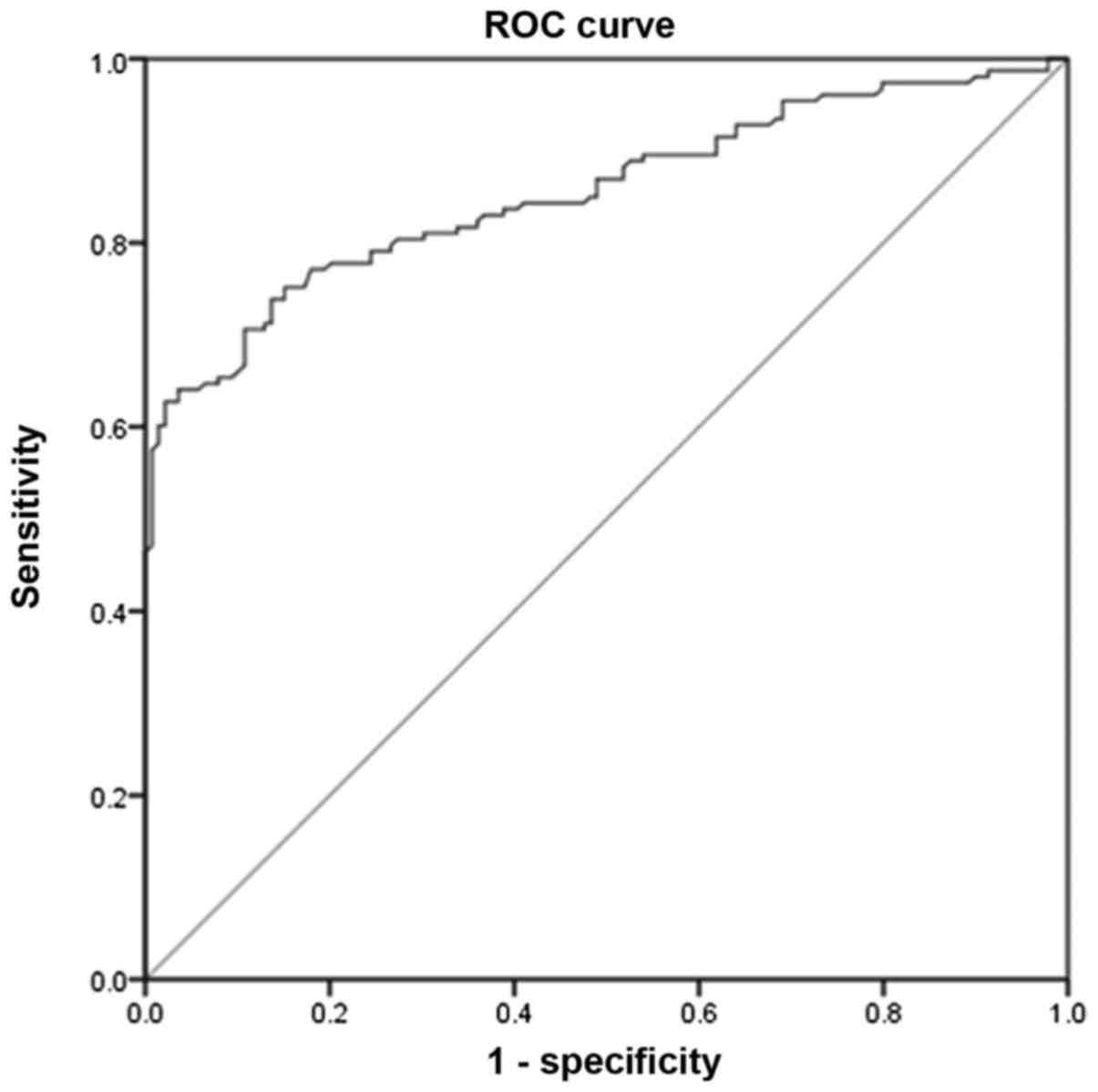
Evaluation of the accuracy of using
serum homocysteine in PCOS diagnosis
Given the results of the present study, the accuracy
of serum homocysteine as a predictor for PCOS was further examined.
To achieve this, ROC analysis was performed (Fig. 2). With an area under the curve of
0.855 (95% CI, 0.811–0.898) and a cut-off level of 20.05 µmol/l,
the results revealed that serum homocysteine levels are a good
predictor for PCOS if diagnosis is based on the Rotterdam
guidelines. The analysis revealed that at the cut-off value, serum
homocysteine has a sensitivity of 73.65% and a specificity of
86.33% in predicting PCOS.
Discussion
The results of the present study provide a tentative
link between homocysteine metabolism and PCOS. If such a link is
validated in larger studies, this will underscore approaches that
may be utilized to better manage the disease and/or its associated
co-morbidities. The most notable result was that the serum levels
of homocysteine were dramatically elevated in women with PCOS.
Importantly, it was observed that higher homocysteine levels remain
associated with PCOS even subsequent to adjusting for other
potentially confounding variables (including age, BMI, BCAAs,
adiponectin and leptin) previously reported to be associated with
PCOS. Furthermore, it was revealed that homocysteine levels were
negatively correlated with 5-MTHF levels and were affected by the
C677T polymorphism of the MTHFR enzyme; a polymorphism known to
affect MTHFR activity and therefore affect 5-MTHF levels (24).
Although IR is not required to establish PCOS
diagnosis, it is a common feature of PCOS and appears to be
involved in the pathogenesis of this disorder (25). Indeed, women with PCOS benefit from
weight reduction and other lifestyle changes that increase insulin
sensitivity (25). The precise cause
behind IR in PCOS appears to be multifactorial. Dysregulation in
the levels of a number of biochemical markers (including leptin,
adiponectin and BCAAs) was proposed to serve a role in establishing
and/or maintaining the PCOS phenotype with conflicting evidence
which either supports or refutes the association (25). The strength of the association of
these biochemical markers with PCOS was not adequately assessed
previously. The present study revealed that relative to leptin,
adiponectin and BCAAs, homocysteine is the most strongly associated
with PCOS. The importance of this observation for PCOS diagnosis
and treatment requires further investigation. For example, it
remains to be determined whether the elevation that was observed in
homocysteine levels in women with PCOS is involved in the disease
pathogenesis or is simply an outcome of this disorder. The answer
to this question requires experiments in PCOS animal models, where
the effect of altering the levels of homocysteine on PCOS may be
investigated in vivo (26). If
higher homocysteine levels are confirmed to be directly or
indirectly involved in PCOS development, this will encourage
therapeutic approaches to mitigate PCOS through lowering serum
homocysteine levels. Indeed, the effective lowering of homocysteine
levels may be achieved through the administration of 5-MTHF,
methylcobalamin (vitamin B12) and/or pyridoxal phosphate
(vitamin B6) combinations (27). This approach may have utility in women
with PCOS, as the present study revealed that homocysteine levels
are negatively correlated with 5-MTHF levels indicating that the
administration of 5-MTHF may lower homocysteine levels and
potentially affect PCOS and/or its co-morbidities; this requires
formal testing in well-designed clinical trials.
Metabolic dysfunction observed in women with PCOS is
associated with an increase in cardiovascular disease risk markers
(28). Whether this increase reflects
a higher prevalence of cardiovascular morbidity and mortality among
women with PCOS remains a matter of debate (28). A number of studies have reported an
association between serum homocysteine levels and an increased
prevalence of cardiovascular morbidity and mortality (29–31). Given
this association, it is plausible that women with higher serum
homocysteine levels may have a higher prevalence of
cardiovascular-associated morbidity and mortality, particularly
women that have inactivating base substitutions in the MTHFR gene.
This association, however, requires formal testing and is an
ongoing effort.
Ethnic differences exist in the clinical and
biochemical presentation of PCOS. For example, Asian women that
have PCOS are often shorter in height, have a lower BMI and a less
severe hyperandrogenic phenotype (32). On the contrary, women with PCOS of
Hispanic origin are usually more likely to be obese and have a
predilection to type 2 diabetes mellitus and the metabolic syndrome
(33). In the present investigation,
it was revealed that women with PCOS of Middle Eastern origin have
dramatically elevated levels of serum homocysteine. Further
investigations are required to test if this elevation is common
among women with PCOS of different ethnicities. Of note, a previous
meta-analysis of 34 studies, which included 1,718 women with PCOS
and 1,399 controls from populations of various ethnicities and
genetic backgrounds, revealed that serum homocysteine levels are
elevated in women with PCOS even subsequent to adjustment for
obesity, IR and androgen levels (34). The results of the present study
combined with the results of the aforementioned study provide
strong support to the argument that ethnic variation may not
influence the association between PCOS and elevated serum
homocysteine levels.
PCOS is a disorder of heterogeneous clinical and
biochemical presentation. Consensus on diagnostic criteria for PCOS
was only reached in 2003 and was mainly based on expert opinions
(21). Furthermore, ethnic
differences exist in disease presentation (35). All of these factors result in the
diagnosis of PCOS being a challenging task and there are a number
of reports where women with PCOS have expressed their
dissatisfaction with the time it took to reach diagnosis and with
the lack of adequate education on the disease (36,37).
Diagnosis of PCOS is particularly challenging among adolescents for
the following reasons; i) acne not associated with PCOS is common
among this age group; and ii) irregularities in the menstrual cycle
are prevalent in the first years that follow menarche (38). A number of experts have suggested
continuous refinement of the biochemical and clinical criteria
required to establish PCOS diagnosis (39). In the present investigation, ROC
analysis revealed that serum homocysteine is a good biomarker for
diagnosis. However, this result requires larger studies among
different ethnicities and different age groups to validate the
potential use of serum homocysteine as a diagnostic biomarker for
PCOS, at least in Jordan. Interestingly, however, given the
meta-analysis performed by Meng et al (34) and described above which revealed that
serum homocysteine levels were elevated in women with PCOS of
various ethnicities, serum homocysteine may prove to be a universal
diagnostic biomarker of PCOS.
The TT genotype of the C677T polymorphism of MTHFR
was associated with higher levels of serum homocysteine in the
present study and serum homocysteine was associated with PCOS;
however, no association was detected between the aforementioned
polymorphism of MTHFR with PCOS. This may be explained by the
sample size of patients used in this study, which may not have been
large enough to detect such an association, particularly as the
total number of individuals that carried the TT genotype in the
present study was only 28. Additionally, the presence of other
polymorphisms associated with the C677T polymorphism may have
cancelled the effect of the C677T polymorphism on PCOS risk.
Although not the primary goal of the present study,
it was revealed that serum leptin levels were lower in women with
PCOS compared with normally menstruating women. This association
remained significant even subsequent to adjusting for age, BMI,
leptin, adiponectin and BCAAs in multivariate analysis. Leptin is a
hormone secreted from the adipocytes (40). Leptin and its receptor serve an
important role in regulating appetite, food intake and energy
expenditure through its effect on the hypothalamic pituitary axis
(41), with higher levels of leptin
primarily associated with appetite suppression. This may explain
why women with PCOS in the present study, who usually have a
tendency to gain weight and develop IR, had lower levels of leptin
and presumably a greater appetite. This result is not in agreement
with the results of Houjeghani et al (42) who revealed that women with PCOS had
higher levels of leptin. The present study, however, was performed
on a larger population. The difference in the association between
leptin and PCOS in the present investigation compared with other
studies may result from ethnic differences in the patients with
PCOS.
In conclusion, to the best of our knowledge, the
present study was the first to demonstrate that serum homocysteine
levels are elevated in women with PCOS in Jordan. It was
additionally revealed that compared with other metabolites
previously reported to be associated with PCOS, including
adiponectin, leptin and BCAAs, serum homocysteine is the most
strongly associated with the PCOS phenotype. These results imply
that lowering serum homocysteine may be used for the management of
PCOS and/or aid in its diagnosis. This requires, however, larger
studies across multiple institutions in the country.
Acknowledgements
Not applicable.
Funding
The present study was supported by the Deanship of
Research at Jordan University of Science and Technology (grants
nos. 214/2017 and 283/2017).
Availability of data and materials
The datasets generated and/or analyzed during the
current study are available from the corresponding author on
reasonable request.
Authors' contributions
All the authors participated in the design, analysis
of the data and final review of the manuscript. MAA and NS
conceived the study. HM, AD and MN helped with data collection. YSK
and RS performed the statistical analysis. HM performed all the
biochemical measurements. MAA and NS drafted the manuscript. All
authors read and approved the final manuscript.
Ethical approval and consent to
participate
All procedures performed in studies involving human
participants were in accordance with the ethical standards of
Jordan University of Science and Technology and King Abdullah
University Hospital institutional review board and with the 1964
Helsinki declaration and its later amendments or comparable ethical
standards. Informed consent was obtained from all individual
participants included in the study.
Patient consent for publication
Written informed consent was obtained from all
individual participants included in the study.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
PCOS
|
polycystic ovarian syndrome
|
|
IR
|
insulin resistance
|
|
BCAAs
|
branched-chain amino acids
|
|
5-MTHF
|
5-methyltetrahydrofolate
|
|
MTHFR
|
methylenetetrahydrofolate
reductase
|
|
KAUH
|
King Abdullah University Hospital
|
|
ELISA
|
enzyme-linked immunosorbent assay
|
|
PCR
|
polymerase chain reaction
|
|
RFLP
|
restriction fragment length
polymorphism
|
|
ROC
|
receiver operating characteristic
|
References
|
1
|
Norman RJ, Dewailly D, Legro RS and Hickey
TE: Polycystic ovary syndrome. Lancet. 370:685–697. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Lizneva D, Suturina L, Walker W, Brakta S,
Gavrilova-Jordan L and Azziz R: Criteria, prevalence, and
phenotypes of polycystic ovary syndrome. Fertil Steril. 106:6–15.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Moran LJ, Misso ML, Wild RA and Norman RJ:
Impaired glucose tolerance, type 2 diabetes and metabolic syndrome
in polycystic ovary syndrome: A systematic review and
meta-analysis. Hum Reprod Update. 16:347–363. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Diamanti-Kandarakis E and Dunaif A:
Insulin resistance and the polycystic ovary syndrome revisited: An
update on mechanisms and implications. Endocr Rev. 33:981–1030.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Badawy A and Elnashar A: Treatment options
for polycystic ovary syndrome. Int J Womens Health. 3:25–35. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Toulis KA, Goulis DG, Farmakiotis D,
Georgopoulos NA, Katsikis I, Tarlatzis BC, Papadimas I and Panidis
D: Adiponectin levels in women with polycystic ovary syndrome: A
systematic review and a meta-analysis. Hum Reprod Update.
15:297–307. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Telli MH, Yildirim M and Noyan V: Serum
leptin levels in patients with polycystic ovary syndrome. Fertil
Steril. 77:932–935. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Li M, Yang M, Zhou X, Fang X, Hu W, Zhu W,
Wang C, Liu D, Li S, Liu H, et al: Elevated circulating levels of
irisin and the effect of metformin treatment in women with
polycystic ovary syndrome. J Clin Endocrinol Metab. 100:1485–1493.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lynch CJ and Adams SH: Branched-chain
amino acids in metabolic signalling and insulin resistance. Nat Rev
Endocrinol. 10:723–736. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Meigs JB, Jacques PF, Selhub J, Singer DE,
Nathan DM, Rifai N, D'Agostino RB Sr and Wilson PW: Framingham
Offspring Study: Fasting plasma homocysteine levels in the insulin
resistance syndrome: The Framingham offspring study. Diabetes Care.
24:1403–1410. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Buysschaert M, Dramais AS, Wallemacq PE
and Hermans MP: Hyperhomocysteinemia in type 2 diabetes:
Relationship to macroangiopathy, nephropathy, and insulin
resistance. Diabetes Care. 23:1816–1822. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Selhub J: Homocysteine metabolism. Annu
Rev Nutr. 19:217–246. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Finkelstein JD: The metabolism of
homocysteine: Pathways and regulation. Eur J Pediatr. 157 Suppl
2:S40–S44. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Chiang EPI, Wang YC, Chen WW and Tang FY:
Effects of insulin and glucose on cellular metabolic fluxes in
homocysteine transsulfuration, remethylation, S-adenosylmethionine
synthesis, and global deoxyribonucleic acid methylation. J Clin
Endocrinol Metab. 94:1017–1025. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lievers KJ, Boers GH, Verhoef P, den
Heijer M, Kluijtmans LA, van der Put NM, Trijbels FJ and Blom HJ: A
second common variant in the methylenetetrahydrofolate reductase
(MTHFR) gene and its relationship to MTHFR enzyme activity,
homocysteine, and cardiovascular disease risk. J Mol Med (Berl).
79:522–528. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Liew SC and Gupta ED:
Methylenetetrahydrofolate reductase (MTHFR) C677T polymorphism:
Epidemiology, metabolism and the associated diseases. Eur J Med
Genet. 58:1–10. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Grodnitskaya EE and Kurtser MA:
Homocysteine metabolism in polycystic ovary syndrome. Gynecol
Endocrinol. 28:186–189. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Salehpour S, Manzor-Al-Ajdad O, Samani EN
and Abadi A: Evaluation of homocysteine levels in patients with
polycystic ovarian syndrome. Int J Fertil Steril. 4:168–171.
2011.PubMed/NCBI
|
|
19
|
Orio F Jr, Palomba S, Di Biase S, Colao A,
Tauchmanova L, Savastano S, Labella D, Russo T, Zullo F and
Lombardi G: Homocysteine levels and C677T polymorphism of
methylenetetrahydrofolate reductase in women with polycystic ovary
syndrome. J Clin Endocrinol Metab. 88:673–679. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Alfaqih MA, Khader YS, Al-Dwairi AN,
Alzoubi A, Al-Shboul O and Hatim A: Lower Levels of Serum
Adiponectin and the T Allele of rs1501299 of the ADIPOQ Gene Are
Protective against Polycystic Ovarian Syndrome in Jordan. Korean J
Fam Med. 39:108–113. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Rotterdam ESHRE/ASRM-Sponsored PCOS
consensus workshop group, . Revised 2003 consensus on diagnostic
criteria and long-term health risks related to polycystic ovary
syndrome (PCOS). Hum Reprod. 19:41–47. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Faul F, Erdfelder E, Lang A-G and Buchner
A: G*Power 3: A flexible statistical power analysis program for the
social, behavioral, and biomedical sciences. Behav Res Methods.
39:175–191. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Chongsuvivatwong V: Analysis of
epidemiological data using R and Epicalc. Epidemiology Unit, Prince
of Songkla University; Thailand: pp. 3282008
|
|
24
|
Brown KS, Kluijtmans LAJ, Young IS, Murray
L, McMaster D, Woodside JV, Yarnell JW, Boreham CA, McNulty H,
Strain JJ, et al: The 5,10-methylenetetrahydrofolate reductase
C677T polymorphism interacts with smoking to increase homocysteine.
Atherosclerosis. 174:315–322. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Diamanti-Kandarakis E and Christakou CD:
Insulin resistance in PCOSDiagnosis and Management of Polycystic
Ovary Syndrome. Springer; New York, NY: pp. 35–61. 2009
|
|
26
|
Padmanabhan V and Veiga-Lopez A: Animal
models of the polycystic ovary syndrome phenotype. Steroids.
78:734–740. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Toole JF, Malinow MR, Chambless LE, Spence
JD, Pettigrew LC, Howard VJ, Sides EG, Wang CH and Stampfer M:
Lowering homocysteine in patients with ischemic stroke to prevent
recurrent stroke, myocardial infarction, and death: The Vitamin
Intervention for Stroke Prevention (VISP) randomized controlled
trial. JAMA. 291:565–575. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Toulis KA, Goulis DG, Mintziori G,
Kintiraki E, Eukarpidis E, Mouratoglou SA, Pavlaki A, Stergianos S,
Poulasouchidou M, Tzellos TG, et al: Meta-analysis of
cardiovascular disease risk markers in women with polycystic ovary
syndrome. Hum Reprod Update. 17:741–760. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Moustapha A, Naso A, Nahlawi M, Gupta A,
Arheart KL, Jacobsen DW, Robinson K and Dennis VW: Prospective
study of hyperhomocysteinemia as an adverse cardiovascular risk
factor in end-stage renal disease. Circulation. 97:138–141. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Wald DS, Law M and Morris JK: Homocysteine
and cardiovascular disease: Evidence on causality from a
meta-analysis. BMJ. 325:1202–1206. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Brattström L and Wilcken DE: Homocysteine
and cardiovascular disease: Cause or effect? Am J Clin Nutr.
72:315–323. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Wijeyaratne CN, Seneviratne RA, Dahanayake
S, Kumarapeli V, Palipane E, Kuruppu N, Yapa C, Seneviratne RA and
Balen AH: Phenotype and metabolic profile of South Asian women with
polycystic ovary syndrome (PCOS): Results of a large database from
a specialist Endocrine Clinic. Hum Reprod. 26:202–213. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Dunaif A, Sorbara L, Delson R and Green G:
Ethnicity and polycystic ovary syndrome are associated with
independent and additive decreases in insulin action in
Caribbean-Hispanic women. Diabetes. 42:1462–1468. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Meng Y, Chen X, Peng Z, Liu X, Sun Y and
Dai S: Association between high serum homocysteine levels and
biochemical characteristics in women with polycystic ovarian
syndrome: A systematic review and meta-analysis. PLoS One.
11:e01573892016. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Zhao Y and Qiao J: Ethnic differences in
the phenotypic expression of polycystic ovary syndrome. Steroids.
78:755–760. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Gibson-Helm M, Teede H, Dunaif A and
Dokras A: Delayed diagnosis and a lack of information associated
with dissatisfaction in women with polycystic ovary syndrome. J
Clin Endocrinol Metab. 102:604–612. 2017.PubMed/NCBI
|
|
37
|
Cree-Green M: Worldwide dissatisfaction
with the diagnostic process and initial treatment of PCOS. J Clin
Endocrinol Metab. 102:375–378. 2017.PubMed/NCBI
|
|
38
|
Fulghesu AM, Porru C and Canu E: Diagnosis
of Polycystic Ovarian Syndrome in AdolescenceGood Practice in
Pediatric and Adolescent Gynecology. Springer; pp. 143–159. 2018,
View Article : Google Scholar
|
|
39
|
Boyle JA and Teede HJ: PCOS: Refining
diagnostic features in PCOS to optimize health outcomes. Nat Rev
Endocrinol. 12:630–631. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Cammisotto PG and Bendayan M: Leptin
secretion by white adipose tissue and gastric mucosa. Histol
Histopathol. 22:199–210. 2007.PubMed/NCBI
|
|
41
|
Klok MD, Jakobsdottir S and Drent ML: The
role of leptin and ghrelin in the regulation of food intake and
body weight in humans: A review. Obes Rev. 8:21–34. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Houjeghani S, Gargari Pourghassem B and
Farzadi L: Serum leptin and ghrelin levels in women with polycystic
ovary syndrome: Correlation with anthropometric, metabolic, and
endocrine parameters. Int J Fertil Steril. 6:117–126.
2012.PubMed/NCBI
|