Introduction
Thin sections from formalin-fixed and
paraffin-embedded (FFPE) human cancer tissues are obtained by
surgery or biopsy and are routinely used, not only for pathological
diagnosis but also for next-generation sequencing (NGS) analysis in
clinical genetic laboratories. Thin-sliced sections are typically
stained with hematoxylin and eosin (H&E) for observation by
light microscopy, which enables pathological diagnosis based on
World Health Organization (WHO) classification and TNM staging.
Accordingly, FFPE tissue blocks are archived from all cancer
patients. The present study hypothesized that certain
histopathological characteristics of thin-sliced sections may be
more or less suitable for downstream NGS, thereby affecting their
application in precision medicine.
The methods for nucleic acid extraction from FFPE
tissue specimens have dramatically improved. Consequently, genomic
DNA is increasingly being used for NGS instead of Sanger sequencing
to detect genetic variants, as well as for quantitative PCR (qPCR)
to detect fusion genes. Specific qualitative factors such as the ∆
crossing point (Cp) value are reported to be indicative of DNA
quality and various quantitative variables have been shown to
affect the integrity of genomic DNA (1). ∆Cp is defined as the cycle number at
detection threshold (crossing point). In brief, the measured Cp is
the cycle at which PCR amplification begins its exponential phase
and is considered, the point that is most reliably proportional to
the initial concentration. Several studies have demonstrated that
the quality of the genomic DNA extracted from FFPE tissue specimens
is critical for performing optimal NGS in a clinical laboratory
setting and these studies cite various important factors affecting
the yield and quality of the DNA, including fixation conditions and
specimen storage time; however, histopathological factors are not
discussed (2-5).
In addition, previous studies have shown that the low quality of
genomic DNA extracted from FFPE tissue specimens poses the risk of
introducing critical errors in downstream clinical analyses
(6-9).
However, it remains unclear whether histopathological factors
observed under a light microscope using H&E-stained sections
cut from FFPE tissue blocks have any impact on the success of
NGS.
The authors previously conducted the collaborative
Biomarker Research for Anti-EGFR Monoclonal Antibodies by
Comprehensive Cancer Genomics (BREAC) study, which involved several
institutes and used NGS to identify a predictive biomarker for the
efficacy of cetuximab treatment (10). This study used FFPE tissue samples and
genomic DNA was successfully extracted from all specimens and was
suitable for NGS analysis. However, to the best of our knowledge
there exists no published study that clarifies the relationship
between the quality of DNA extracted from FFPE tissue blocks and
the histopathological factors identified by microscopic observation
using thin-sliced sections stained with H&E during routine
pathological diagnosis.
The aim of the present study was to characterize the
histopathological factors affecting the level of DNA quality
required for NGS and then to standardize the macrodissection method
of FFPE tissue blocks based on these histopathological factors to
enable the selection of appropriate tissue blocks for NGS during
routine pathological diagnosis.
Materials and methods
Patient characteristics
FFPE tissue specimens from 218 patients, including
neoplastic tissues, were submitted for the BREAC study (10). A total of 298 patients (age range,
28-85 years) were recruited from seven institutions, including
Cancer Institute Hospital of Japanese Foundation for Cancer
Research (Tokyo, Japan), Aichi Cancer Center Hospital (Nagoya,
Japan), National Cancer Center Hospital East (Kashiwa, Japan),
Saitama Cancer Center (Saitama, Japan), Shikoku Cancer Center
(Matsuyama, Japan), Shizuoka Cancer Center (Shizuoka, Japan) and
Hokkaido University Hospital (Sapporo, Japan), between April 2012
and May 2013 and were initially registered in the present study.
Patients with insufficient FFPE tissue specimens (11 patients),
target re-sequencing failure (36 patients) and ineligible patients
(9 patients) were excluded from the BREAC study according to the
eligibility criteria (10). Biopsy
specimens from 24 patients were also excluded from this study.
Baseline characteristics of the patients were registered with the
Office of Translational Research of the Exploratory Oncology
Research and Clinical Trial Center (EPOC), National Cancer Center,
(Chiba, Japan), by the investigators of each of the participating
facilities. Genomic DNA from all specimens was successfully
extracted and subjected to whole-genome sequencing. The study was
approved by the Ethics Committee of each of the seven institutes
[approval numbers: 2011-137 (National Cancer Center Hospital East),
13-009 (Hokkaido University Hospital), 24-15-24-1-5 (Shizuoka
Cancer Center), H23-no2 (Shikoku Cancer Center), 2011-1084 (Cancer
Institute Hospital of Japanese Foundation for Cancer Research),
20110903 (Saitama Cancer Center), 2016-1-122 (Aichi Cancer Center
Hospital)] and the study conformed with the guidelines of the
Declaration of Helsinki. Written informed consent was obtained from
patients who were alive when initiating this study. For deceased
patients and their relatives at that time, the study design on the
website of each center was disclosed and the relatives were allowed
to approve or deny inclusion in the study. This study was conducted
in accordance with the Ethical Guidelines for the human genome and
genetic analysis research of the Ministry of Education, Culture,
Sports, Science and Technology, Ministry of Health, Labor and
Welfare and Ministry of Economy, Trade and Industry.
DNA extraction from the FFPE tissue
specimens
Archived FFPE tissue specimens collected during the
BREAC study before anti-EGFR antibody treatment were used for DNA
extraction. Specimens from either biopsied or surgically resected
tissues were submitted to the Division of Translational Research,
EPOC. Central pathological diagnosis of thin sections from all FFPE
tissue specimens submitted from all seven institutions was
conducted by the authorized pathologist (S.F.) under microscopic
observation, using the slides stained with H&E (hematoxylin, 7
min and eosin, 2 min at both at room temperature).
As part of the BREAC study, the H&E stained
sections were observed with a light microscope to determine whether
areas of the tissue exhibiting unfavorable histopathology for high
DNA quality could be selectively removed to some extent. These
histopathological factors included necrosis, mucous pools, tumor
budding, desmoplasia, excessive inflammatory cells, microabscess,
poor fixation and burning effect. The region to be used for DNA
extraction was determined and marked on the glass slide with a
color pen, and then macrodissection of the microscopically
specified regions was performed. Genomic DNA was then extracted
from both the carcinoma cells and normal cells from the thin-sliced
sections (10 µm) with the Absolutely RNA FFPE kit using a modified
version of the manufacturer's protocol for DNA extraction (Agilent
Technologies, Inc.). For the present study, DNA quality was then
determined by estimating the dsDNA/total nucleic acid ratio and ∆Cp
value. A NanoDrop 2000 spectrophotometer (Thermo Fisher Scientific,
Inc.) was used to quantify the total nucleic acids and the Quant-iT
PicoGreen dsDNA Reagent and kit (Thermo Fisher Scientific, Inc.)
was used to quantify the dsDNA. The Infinium HD FFPE QC kit (cat.
no. WG-321-1001; Illumina, Inc.) was used for qPCR to determine the
∆Cp value [Cp(intact DNA) – Cp(FFPE tissue DNA)] between the test
samples extracted from the FFPE tissue specimens and control intact
genomic DNA so as to evaluate the quality of the extracted DNA
according to the manufacturer's instructions. The relationships
between the ∆Cp value and the dsDNA/total nucleic acid ratio and
the histopathological factors of each cancer specimen were then
investigated. The thermocycling conditions were as follows: 95˚C
for 5 min, followed by 40 cycles of 95˚C for 30 sec, 57˚C for 30
sec and 72˚C for 30 sec.
Histopathological factors presumed to
affect DNA quality
The present study focused on the histopathological
factors suspected to affect the quality of DNA extracted from the
cancer cells and, in turn, the quality of the downstream target
sequencing data. The studied histopathological factors were as
follows: Intra-tubular necrosis, extra-tubular necrosis, mucus
pools, tumor budding, histological differentiation, histological
grading according to the WHO classification, desmoplasia, excessive
infiltration of inflammatory cells, microabscesses, burning effect,
the ratio of tumor cells to the total number of cells, metastatic
tumors, the area (mm2) of the tumor region taken from
the FFPE section for DNA extraction, the use of laser
microdissection and the length of storage of the FFPE tissue
specimens. These exploratory variables were then observed under a
light microscope by the same authorized pathologist (S.F.) who
undertook the central pathological diagnosis in the BREAC study
(10). Sections were then selected
for high tumor cell ratio, a low number of denatured tumor cells
and the exclusion of the histopathological factors that may have a
detrimental effect on NGS.
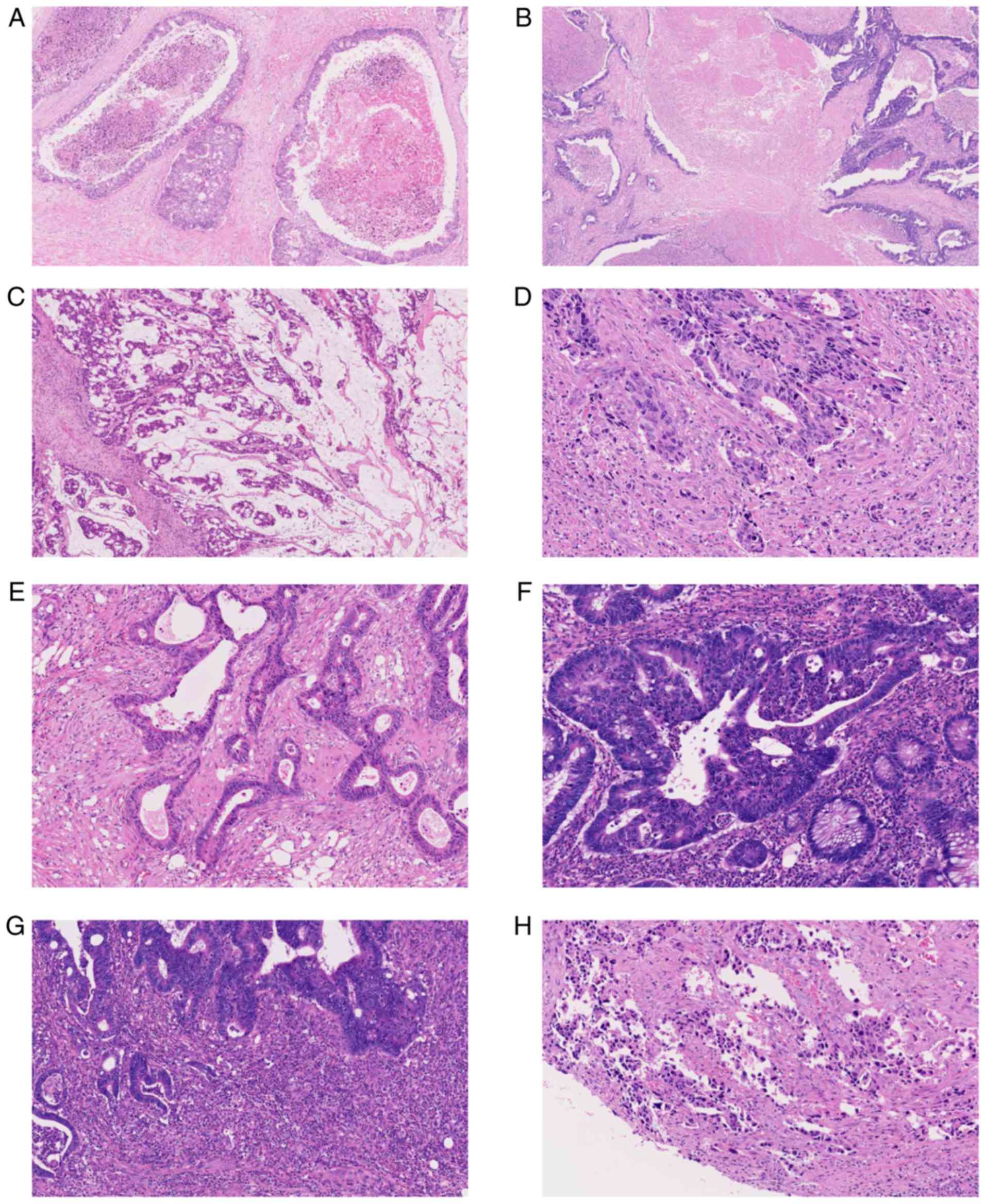
Micrographs of representative histopathological
factors presumed to affect DNA quality are shown in Fig. 1. Intra-tubular necrosis refers to
localized necrosis in the neoplastic duct formed by tumor cells
(Fig. 1A). Extra-tubular necrosis
occurs when necrosis does not remain only in the neoplastic ducts
formed by the tumor cells and necrotic materials leak out of these
ducts and are observed extensively in tumor tissue (Fig. 1B). Mucous pools refer to tumor cells
floating within the neoplastic mucus (Fig. 1C). Tumor budding is a process during
which individual or small clusters of up to five tumor cells detach
from the main tumor mass and invade the surrounding stroma
(11) (Fig.
1D). Desmoplasia refers to stromal myofibroblastic
proliferation attributable to infiltrating tumor cells (Fig. 1E). Excessive infiltration of
inflammatory cells refers to a high degree of inflammatory cell
infiltration into the tumor cells; these inflammatory cells are
difficult to separate out even by microdissection (Fig. 1F). Microabscesses are a collection of
neutrophils (Fig. 1G), whereas the
burning effect occurs when tumor cells are degenerated by
artificial heat (Fig. 1H).
The region to be used for DNA extraction was
demarcated by excluding areas containing these histopathological
factors as far as possible and then macrodissection was
performed.
Statistical analysis
The present study first investigated whether there
was a difference between the seven participating institutes in
terms of the quality of the DNA they extracted. Summary statistics
and graphical methods (box plots and histograms) were used to
compare the ∆Cp values and dsDNA quality.
Continuous variables, including ∆Cp value and dsDNA
quality, were dichotomized according to their median since the aim
of this study was to explore the histopathological factors related
to poor DNA quality. The dichotomized outcome indicators were
modeled using univariate and multivariate logistic regression
analyses with forward stepwise selection (entry and removal
criterion of P<0.05) for the ∆Cp value and dsDNA quality,
respectively. Patients with missing outcome variables were
excluded. To determine the favorable length of storage of FFPE
specimens, the best cut-off value was investigated to discriminate
the dichotomized ∆Cp values and dsDNA quality using Fisher's exact
test. For the continuous collection area, logarithmic
transformation was applied and modeled as itself because no
clinically acceptable cut-off value was determined.
All statistical analyses including Fisher's exact
test were performed with SAS 9.4 Software (SAS Institute, Inc.).
All P-values were obtained from two-tailed statistical tests.
P<0.05 was considered to indicate at statically significant
difference.
Results
Patient characteristics
The patient characteristics are shown in Table I. All studied specimens were
surgically resected from the 218 patients. Among these specimens,
180 (82.6%) were primary tumors and 38 (17.4%) were metastatic.
Sites of metastasis were the liver, lungs or lymph nodes and the
number of each of these metastatic sites was 32 (84.2%), 4 (10.5%),
and 2 (5.3%), respectively.
 | Table IPatient characteristics. |
Table I
Patient characteristics.
| Characteristic | Patients (n) | Patients (%) |
|---|
| Total number | 218 | 100.0 |
| Median age (range),
years | 61 (28-85) | 100.0 |
| Gender |
|
Male | 129 | 59.2 |
|
Female | 89 | 40.8 |
| Specimen |
|
Surgical | 218 | 100.0 |
|
Biopsy | 0 | 0.0 |
| Tumor |
|
Primary | 180 | 82.6 |
|
Metastatic | 38 | 17.4 |
| Primary tumor site
(n=180) |
|
Colon
(n=133) | | |
|
Ascending
colon | 21 | 11.7 |
|
Transverse
colon | 12 | 6.7 |
|
Descending
colon | 7 | 3.9 |
|
Sigmoid
colon | 73 | 40.5 |
|
Rectosigmoid
colon | 20 | 11.1 |
|
Rectum | 42 | 23.3 |
|
Unknown | 5 | 2.8 |
| Metastatic tumor site
(n=38) |
|
Liver | 32 | 84.2 |
|
Lung | 4 | 10.5 |
|
Lymph
nodes | 2 | 5.3 |
| Tumor
differentiation |
|
Good | 93 | 42.7 |
|
Moderate | 110 | 50.4 |
|
Poor | 15 | 6.9 |
No difference is observed in the mean
dsDNA quality and ∆Cp value among the different institutes
participating in the BREAC study
It was necessary to first verify whether there were
any differences in the mean dsDNA/total nucleic acid ratio and ∆Cp
value among the institutes participating in the BREAC study.
Statistical analysis revealed that there was no significant
difference in these values among the seven institutes, as shown in
Table II, implying that the
processes adopted for preparing FFPE tissue blocks at each facility
did not affect dsDNA quality or the ∆Cp value and that none of the
facilities used irregular fixation or storage methods. Therefore,
it was concluded that a total of 218 FFPE tissue specimens were
available for the analyses in this study.
| Table IIFacility-dependent dsDNA quantity, ∆Cp
value and fixation method. |
Table II
Facility-dependent dsDNA quantity, ∆Cp
value and fixation method.
| | dsDNAa | ∆Cpb | Formalin
fixation |
|---|
| Facility | Mean ± SD | Median (range) | Mean ± SD | Median (range) | Concentration
(%) | pH | Fixation time
(h) |
|---|
| 1 | 9.853±2.752 | 10.223
(3.916-19.006) | -1.641±1.390 | -1.726
(-4.605-1.135) | 20 | 7.4 | 48-72 |
| 2 | 13.083±3.710 | 12.266
(5.829-23.350) | -1.886±1.411 | -1.997
(-6.760-0.670) | 10c | 7.0 | 24-36 |
| 3 | 12.387±5.904 | 11.605
(3.592-28.807) | -1.832±1.221 | -1.430
[-5.570-(-0.077)] | 10 | 7.0 | 24-36 |
| 4 | 15.287±2.723 | 14.424
(11.237-21.515) | -1.389±0.950 | -1.048
[-4.160-(-0.013)] | 20c | 7.4 | 36-48 |
| 5 | 13.929±4.363 | 13.409
(4.288-23.984) | -1.880±0.934 | -1.653
[-4.630-(-0.673)] | 15 | 7.4 | 24 |
| 6 | 12.485±3.435 | 12.007
(7.141-22.570) | -1.150±0.867 | -1.108
(-3.203-0.733) | 10 | 7.0 | 24-102 |
| 7 | 13.074±3.187 | 13.487
(5.545-17.032) | -1.566±0.762 | -1.600
[-3.283-(-0.180)] | 10 | 7.4 | 24-48 |
Determination of cut-off values for
the dsDNA/total nucleic acid ratio and ∆Cp value
The median and average of the dsDNA/total nucleic
acid ratio were 12.17 and 12.61, respectively. The samples with
dsDNA quality less than the median value were defined as samples
with a lower quality of genomic DNA. The median and average of the
∆Cp value were -1.48 and -1.63, respectively. Samples with a ∆Cp
lower than the median were defined as samples with a lower quality
of genomic DNA. The four patients with missing ∆Cp values were
excluded. Therefore, in subsequent analyses, the present study
analyzed the relationship between ∆Cp and the histopathological
factors in specimens from the remaining 214 patients.
Relationships between the storage
period of the FFPE tissue specimens and variables such as dsDNA
quality and ∆Cp value
The relationships between the storage period of the
FFPE tissue specimens and dsDNA quality and ∆Cp value were assessed
using Fisher's exact test, as shown in Table III. The results showed that both
dichotomized values became significantly smaller when the storage
period was ≥3 years (P<0.001). The cut-off for the storage
period was, therefore, set to 3 years for this study.
| Table IIIStorage time cut-offs for FFPE tissue
blocks based on dsDNA quantity (n=218) and ∆Cp value (n=214). |
Table III
Storage time cut-offs for FFPE tissue
blocks based on dsDNA quantity (n=218) and ∆Cp value (n=214).
| A. Depending on
dsDNA quantity (n=218). |
|---|
| | N (%) | dsDNA ≥ median
(%) | |
|---|
| Cut-off
(years) | <Cut-off | ≥Cut-off | <Cut-off | ≥Cut-off | P-value |
|---|
| 2 | 6 (2.75) | 212 (97.25) | 83.3 | 49.1 | 0.1061 |
| 3 | 35 (16.06) | 183 (83.94) | 77.1 | 44.8 | 0.0004 |
| 4 | 73 (33.49) | 145 (66.51) | 69.9 | 40.0 | <0.0001 |
| 5 | 123 (56.42) | 95 (43.58) | 59.4 | 40.7 | 0.0013 |
| 6 | 172 (78.90) | 46 (21.10) | 51.7 | 43.5 | 0.2034 |
| 7 | 192 (88.07) | 26 (11.93) | 50.5 | 46.2 | 0.4174 |
| 8 | 205 (94.00) | 13 (5.96) | 51.2 | 30.8 | 0.1260 |
| B. Depending on ∆Cp
value (n=214). |
| | N (%) | ΔCp ≥ median
(%) | |
| Cut-off
(years) | <Cut-off | ≥Cut-off | <Cut-off | ≥Cut-off | P-value |
| 2 | 6 (2.80) | 208 (97.20) | 100.0 | 48.6 | 0.0145 |
| 3 | 34 (15.89) | 180 (84.11) | 79.4 | 44.4 | 0.0001 |
| 4 | 71 (33.18) | 143 (66.82) | 64.8 | 42.7 | 0.0018 |
| 5 | 120 (56.07) | 94 (43.93) | 60.0 | 37.2 | 0.0007 |
| 6 | 168 (78.50) | 46 (21.50) | 53.6 | 37.0 | 0.3322 |
| 7 | 188 (87.85) | 26 (12.15) | 53.2 | 26.9 | 0.0100 |
| 8 | 201 (93.93) | 13 (6.07) | 51.2 | 30.8 | 0.1259 |
Histopathological factors influencing
dsDNA quality
The regions of the FFPE sections used for DNA
extraction were selected based on the presence of as few negative
histological factors as possible. Nevertheless, a certain amount of
these factors were inevitably included in the regions used for
macrodissection. The subsequent analysis was, therefore, still able
to elucidate the relationship between the histological factors
included in the DNA extraction region and DNA quality.
Univariate and multivariate logistic regression
analyses were performed to identify variables influencing dsDNA
quality (Table IV). Multivariate
regression analysis revealed that the storage of FFPE specimens for
≥3 years was significantly associated with a lower dsDNA/total
nucleic acid ratio (P=0.0007, OR: 4.30, 95% CI: 1.85-10.04).
Contrary to the hypothesis that some of the histopathological
factors analyzed in this study are responsible for poor DNA
quality, the presence of mucus pools appeared to be a positive
factor in a favorable dsDNA/total nucleic acid ratio (P=0.0308, OR:
0.23, 95% CI: 0.06-0.87). In addition, there was a non-negligible
difference in the proportion of samples with a higher dsDNA/total
nucleic acid ratio between samples with and without a mucus pool
(Fisher's exact test, P=0.0496; Table
V). However, there was no difference in the proportion of
samples with a higher ∆Cp value between samples with and without a
mucus pool (Table SI). These results
confirmed that mucus pools are significantly correlated only with
dsDNA quality.
| Table IVVariables influencing dsDNA quality
determined using univariate and multivariate analyses (Cox
proportional hazard model). |
Table IV
Variables influencing dsDNA quality
determined using univariate and multivariate analyses (Cox
proportional hazard model).
| | Univariate
analysis | Multivariate
analysis |
|---|
| Variable | Cases
(n=218)a | OR | 95% CI | P-value | OR | 95% CI | P-value |
|---|
| Intra-tubular
necrosis | | 1.71 | 0.68-4.31 | 0.2553 | | | |
|
Absence | 21 | | | | | | |
|
Presence | 197 | | | | | | |
| Extra-tubular
necrosis | | 1.20 | 0.71-2.05 | 0.4975 | | | |
|
Absence | 117 | | | | | | |
|
Presence | 101 | | | | | | |
| Mucus pool | | 0.25 | 0.07-0.93 | 0.0386 | 0.23 | 0.06-0.87 | 0.0308 |
|
Absence | 204 | | | | | | |
|
Presence | 14 | | | | | | |
| Tumor budding | | 0.57 | 0.23-1.38 | 0.2006 | | | |
|
Grade 1 | 148 | | | | | | |
|
Grade 2 | 46 | | | | | | |
|
Grade 3 | 24 | | | | | | |
| Histological
differentiation | | 1.15 | 0.40-3.30 | 0.7895 | | | |
|
Well/Moderate | 203 | | | | | | |
|
Poor/Undifferentiated | 15 | | | | | | |
| Grading (WHO
classification) | | 1.15 | 0.40-3.30 | 0.7895 | | | |
|
Grade
1/2 | 203 | | | | | | |
|
Grade
3/4 | 15 | | | | | | |
| Desmoplasia | | 0.89 | 0.51-1.55 | 0.6709 | | | |
|
Absence | 141 | | | | | | |
|
Presence | 77 | | | | | | |
| Excessive
infiltration of inflammatory cells | | 0.70 | 0.36-1.38 | 0.3042 | | | |
|
Absence | 176 | | | | | | |
|
Presence | 42 | | | | | | |
| Microabscess | | 0.65 | 0.33-1.30 | 0.2269 | | | |
|
Absence | 177 | | | | | | |
|
Presence | 41 | | | | | | |
| Burning effect | | 0.61 | 0.23-1.64 | 0.3288 | | | |
|
Absence | 200 | | | | | | |
|
Presence | 18 | | | | | | |
| RTCb | | 2.15 | 0.83-5.55 | 0.1147 | | | |
|
>50% | 21 | | | | | | |
|
≤50% | 197 | | | | | | |
| Metastatic
tumor | | 2.20 | 1.06-4.57 | 0.0349 | | | |
|
No | 180 | | | | | | |
|
Yes | 38 | | | | | | |
| Tumor area using
log-scale (mm2) | | 0.84 | 0.63-1.12 | 0.2429 | | | |
| Laser
microdissection | | 0.74 | 0.16-3.40 | 0.7018 | | | |
|
No | 211 | | | | | | |
|
Yes | 7 | | | | | | |
| FFPE storage time
(years) | | 4.19 | 1.79-9.64 | 0.0009 | 4.30 | 1.85-10.04 | 0.0007 |
|
>3 | 35 | | | | | | |
|
≤3 | 183 | | | | | | |
| Table VAssociation of the presence of mucus
pools with the dsDNA quantity. |
Table V
Association of the presence of mucus
pools with the dsDNA quantity.
| | Quantitative ratio
of dsDNA to total nucleic acids (n) | | |
|---|
| Mucus pool | ≤Median | ≥Median | Total (n) | P-value |
|---|
|
Presence | 11 | 3 | 14 | 0.0496 |
|
Absence | 98 | 106 | 204 | |
| Total (n) | 109 | 109 | 218 | |
Histopathological factors influencing
the ∆Cp value
Univariate and multivariate logistic regression
analyses were performed on samples from 214 patients to identify
variables influencing DNA quality based on the ∆Cp value (Table VI). Multivariate analysis revealed
that metastatic tumors and the storage of FFPE specimen for ≥3
years were significantly associated with a lower ∆Cp value
(Metastatic tumor: P=0.0007, OR: 4.43, 95% CI: 1.87-10.49, storage
period of FFPE specimen: P=0.0003, OR: 5.51, 95% CI:
2.18-13.95).
| Table VIVariables influencing ∆Cp values
determined using univariate and multivariate analyses (Cox
proportional hazard model). |
Table VI
Variables influencing ∆Cp values
determined using univariate and multivariate analyses (Cox
proportional hazard model).
| | Univariate
analysis | Multivariate
analysis |
|---|
| Variable | Cases
(n=214)a | OR | 95% CI | P-value | OR | 95% CI | P-value |
|---|
| Intra-tubular
necrosis | | 2.15 | 0.83-5.56 | 0.1143 | | | |
|
Absence | 21 | | | | | | |
|
Presence | 193 | | | | | | |
| Extra-tubular
necrosis | | 1.51 | 0.88-2.60 | 0.1322 | | | |
|
Absence | 115 | | | | | | |
|
Presence | 99 | | | | | | |
| Mucus pool | | 1.00 | 0.34-2.96 | 1.0000 | | | |
|
Absence | 200 | | | | | | |
|
Presence | 14 | | | | | | |
| Tumor Budding | | 0.77 | 0.32-1.83 | 0.8152 | | | |
|
Grade 1 | 145 | | | | | | |
|
Grade 2 | 45 | | | | | | |
|
Grade 3 | 24 | | | | | | |
| Histological
differentiation | | 1.55 | 0.53-4.51 | 0.4248 | | | |
|
Well/Moderate | 199 | | | | | | |
|
Poor/Undifferentiated | 15 | | | | | | |
| Grading (WHO
classification) | | 1.55 | 0.53-4.51 | 0.4248 | | | |
|
Grade
1/2 | 199 | | | | | | |
|
Grade
3/4 | 15 | | | | | | |
| Desmoplasia | | 0.75 | 0.43-1.32 | 0.3164 | | | |
|
Absence | 139 | | | | | | |
|
Presence | 75 | | | | | | |
| Excessive
infiltration of inflammatory cells | | 0.83 | 0.42-1.65 | 0.6031 | | | |
|
Absence | 173 | | | | | | |
|
Presence | 41 | | | | | | |
| Microabscess | | 0.83 | 0.41-1.66 | 0.5962 | | | |
|
Absence | 175 | | | | | | |
|
Presence | 39 | | | | | | |
| Burning effect | | 1.28 | 0.48-3.37 | 0.6230 | | | |
|
Absence | 196 | | | | | | |
|
Presence | 18 | | | | | | |
| RTCb | | 0.73 | 0.29-1.80 | 0.4920 | | | |
|
>50% | 21 | | | | | | |
|
≤50% | 193 | | | | | | |
| Metastatic
tumor | | 3.86 | 1.72-8.65 | 0.0010 | 4.43 | 1.87-10.49 | 0.0007 |
|
No | 177 | | | | | | |
|
Yes | 37 | | | | | | |
| Tumor area using
log-scale (mm2) | | 0.87 | 0.65-1.16 | 0.3307 | | | |
|
>58.1 | | | | | | | |
|
≤58.1 | | | | | | | |
| Laser
microdissection | | 0.49 | 0.09-2.74 | 0.4167 | | | |
|
No | 208 | | | | | | |
|
Yes | 6 | | | | | | |
| Storage time
(years) | | 4.82 | 2.00-11.64 | 0.0005 | 5.51 | 2.18-13.95 | 0.0003 |
|
>3 | 34 | | | | | | |
|
≤3 | 180 | | | | | | |
Discussion
In the BREAC study, DNA extraction from each FFPE
tissue specimen was carried out such that the histopathological
factors determined through microscopic observation, including
necrosis, mucus pools, tumor budding, desmoplasia, excessive
inflammatory cells, microabscesses, poor fixation, and burning
effect, were excluded as much as possible from the tumor area from
which the DNA was extracted (10).
However, it was difficult to eliminate these histopathological
factors from the tumor area for DNA extraction, which allowed the
evaluation of their effect in the present study. The results of the
present study on these archived specimens showed that metastatic
tumors and FFPE specimen storage of ≥3 years were strongly
associated with poor DNA quality. Thus, it would be preferable to
extract DNA for NGS purposes from tumor regions where these
histopathological factors have been excluded as far as possible by
macrodissection. These findings should be incorporated into future
standard operating procedures; current guidelines published in
several countries, including the USA (http://jmd.amjpathol.org/article/S1525-1578(17)30025-9/fulltext#sec1.2.1),
Australia (http://jmd.amjpathol.org/article/S1525-1578(17)30025-9/fulltext#sec1.2.1)
and Japan (http://jccls.org/active/MM6-A1_agenda.pdf and
http://pathology.or.jp/genome_med/elearning.html)
do not include standards for the proper removal of
histopathological factors affecting the quality of DNA for NGS from
FFPE tissue specimens.
A total of three factors significantly affecting the
quality of DNA were identified in this study. Interestingly, mucus
pools comprised a positive factor correlated with the extraction of
better-quality DNA for NGS. However, it is not yet known how mucus
pools exert this effect. To the best of our knowledge, there are no
studies on the relationship between mucus pools and DNA quality.
Further investigation is, therefore, needed.
In contrast, metastatic tumors comprised an
independent negative factor affecting the ∆Cp value. Although the
presence of metastatic tumors was not an independent negative
factor affecting the dsDNA/total nucleic acid ratio based on
multivariate analysis, it was a negative factor for this ratio
based on univariate analysis. Advanced colorectal cancer generally
shows metastasis to the liver and lung. It is also well known that
extensive necrosis is generally observed in metastatic lesions of
colorectal cancer. It was difficult to determine the area for DNA
extraction in metastatic tumor specimens from which necrosis had
been completely excluded, which explains one of the reasons for
this contradictory outcome in the current study. Based on this
result, it is recommended to select a region with as little
necrosis as possible when FFPE specimens of metastatic tumors are
processed for DNA extraction.
Storage of the FFPE tissue block for ≥3 years was a
negative factor related to DNA quality, as indicated by both the
dsDNA/total nucleic acid ratio and the ∆Cp value. A previous study
suggested that FFPE specimens stored for several years may have a
poorer quality of DNA (5). FFPE
tissues are one of the most widely available clinical specimens and
have potential utility as a source of DNA for NGS. Archived FFPE
tissue specimens are required not only for clinical trials but also
for population-based studies. Since older FFPE tissue specimens may
be required, especially from patients suffering from cancer for a
long time, it is necessary to establish an improved method for
storing these specimens that can be incorporated into routine
pathological practice. However, methods of targeted NGS using
low-quality DNA are constantly improving, which will likely lead to
further improvement in the application of NGS to damaged DNA
extracted from old FFPE tissue specimens in the future.
The reasons for dividing the samples into two groups
based on the median were the following; i) There is no definitive,
published cutoff value for dsDNA or ΔCp and the significance
associated with fluctuations in these values is unknown. ii)
Relatively high-quality specimens were collected in the BREAC
trial. Rather than subgrouping a heterogeneous population with the
median, in the present study a homogeneous population has been
subgrouped with the median. This method was considered to be
sensitive enough to search for factors affecting the dsDNA and ΔCp
values. iii) The ability to extract factors with statistically
higher power when the outcome variables are segregated based on the
median and the sample sizes are equal. From the results of this
study, it cannot be concluded that the samples judged to be of low
quality in this study are completely unsuitable for NGS. However,
this study indicated useful guidelines for the optimal extraction
of DNA for NGS.
There are several limitations to this study. First,
this was a retrospective study. Detailed information of all the
specimens from the time the specimens were submitted until they
became FFPE tissue specimens used in the present study could not be
obtained at each institute, although there was no disparity among
these facilities in terms of the quality of extracted DNA. DNA
extraction was carried out by first removing the studied
histological factors as much as possible. If any of the
histopathological factors were quantitatively included, there is a
possibility that the quality of DNA was influenced by these
factors. In addition, the sequencing parameters were optimized for
individual DNA samples, such as the pre- and post-capture PCR
cycles, to maximize the gathered genomic data. Therefore, it is
impossible to compare the parameters related to the success of DNA
sequencing in the BREAC study and the histopathological factors
investigated in this study. Finally, only one central pathologist
investigated all the tissue specimens in this study. In the near
future, the findings of this study should be validated by other
pathologists.
The proposal of the present study is that
macrodissection of microtomed sections should be performed after
the removal of as many negative histological factors as possible
and that the use of old FFPE tissue blocks stored for ≥3 years
should be avoided. This is all possible during routine observation
of H&E-stained sections under a light microscope and it would
enable the extraction of high-quality DNA suitable for downstream
NGS.
Supplementary Material
Association between presence of mucus
pool and the value of ΔCp to control.
Acknowledgements
The authors would like to thank Dr. Wataru Okamoto
and Ms. Izumi Miki (Office of Translational Research of the
Exploratory Oncology Research and Clinical Trial Center, National
Cancer Center, Kashiwa, Chiba, Japan) for organizing the registered
patients' information in the BREAC trial.
Funding
The BREAC study was supported by the Adaptable and
Seamless Technology Transfer Program through target-driven R&D,
Practical Application Development by SME Start-up, the Japan
Science and Technology Agency, the National Cancer Center Research
and Development Fund (23-A-2), G & G Science Co., Ltd., and
Medical & Biological Laboratories Co., Ltd.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
SF, TYo, KT, KMa, YS, KA, HE, MS, NN, MM, YK, YA and
AO conceived and designed the study. ES, KYamaz, TYa, KMu, TN,
KYamag, SY, KS and HB provided study materials or patients. SN and
TYo collected and analyzed the data. SM, CN and KT performed genome
sequencing. SF, TYa, KT and SN undertook data analysis and
interpretation. SF, KT, SN and TYo wrote the manuscript. All
authors read and approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
each of the seven institutes [approval numbers: 2011-137 (National
Cancer Center Hospital East), 13-009 (Hokkaido University
Hospital), 24-15-24-1-5 (Shizuoka Cancer Center), H23-no2 (Shikoku
Cancer Center), 2011-1084 (Cancer Institute Hospital of Japanese
Foundation for Cancer Research), 20110903 (Saitama Cancer Center),
2016-1-122 (Aichi Cancer Center Hospital)] and the study conformed
with the guidelines of the Declaration of Helsinki. Written
informed consent was obtained from patients who were alive when
initiating this study. For deceased patients and their relatives at
that time, the study design on the website of each center was
disclosed and the relatives were allowed to approve or deny
inclusion in the study. This study was conducted in accordance with
the Ethical Guidelines for the human genome and genetic analysis
research of the Ministry of Education, Culture, Sports, Science and
Technology, Ministry of Health, Labour and Welfare and Ministry of
Economy, Trade and Industry.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Treece AL, Montgomery ND, Patel NM,
Civalier CJ, Dodd LG, Gulley ML, Booker JK and Weck KE: FNA smears
as a potential source of DNA for targeted next-generation
sequencing of lung adenocarcinomas. Cancer Cytopathol. 124:406–414.
2016.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Nagahashi M, Shimada Y, Ichikawa H,
Nakagawa S, Sato N, Kaneko K, Homma K, Kawasaki T, Kodama K, Lyle
S, et al: Formalin-fixed paraffin-embedded sample conditions for
deep next generation sequencing. J Surg Res. 220:125–132.
2017.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Einaga N, Yoshida A, Noda H, Suemitsu M,
Nakayama Y, Sakurada A, Kawaji Y, Yamaguchi H, Sasaki Y, Tokino T
and Esumi M: Assessment of the quality of DNA from various
formalin-fixed paraffin-embedded (FFPE) tissues and the use of this
DNA for next-generation sequencing (NGS) with no artifactual
mutation. PLoS One. 12(e0176280)2017.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Cho M, Ahn S, Hong M, Bang H, Van Vrancken
M, Kim S, Lee J, Park SH, Park JO, Park YS, et al: Tissue
recommendations for precision cancer therapy using next generation
sequencing: A comprehensive single cancer center's experiences.
Oncotarget. 8:42478–42486. 2017.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Carrick DM, Mehaffey MG, Sachs MC,
Altekruse S, Camalier C, Chuaqui R, Cozen W, Das B, Hernandez BY,
Lih CJ, et al: Robustness of next generation sequencing on older
formalin-fixed paraffin-embedded tissue. PLoS One.
10(e0127353)2015.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Bettoni F, Koyama FC, de Avelar Carpinetti
P, Galante PAF, Camargo AA and Asprino PF: A straightforward assay
to evaluate DNA integrity and optimize next-generation sequencing
for clinical diagnosis in oncology. Exp Mol Pathol. 103:294–299.
2017.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Bonfiglio S, Vanni I, Rossella V, Truini
A, Lazarevic D, Dal Bello MG, Alama A, Mora M, Rijavec E, Genova C,
et al: Performance comparison of two commercial human whole-exome
capture systems on formalin-fixed paraffin-embedded lung
adenocarcinoma samples. BMC Cancer. 16(692)2016.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Dumur CI, Almenara JA, Powers CN and
Ferreira-Gonzalez A: Quality control material for the detection of
somatic mutations in fixed clinical specimens by next-generation
sequencing. Diagn Pathol. 10(169)2015.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Kim S, Park C, Ji Y, Kim DG, Bae H, van
Vrancken M, Kim DH and Kim KM: Deamination effects in
formalin-fixed, paraffin-embedded tissue samples in the era of
precision medicine. J Mol Diagn. 19:137–146. 2017.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Shinozaki E, Yoshino T, Yamazaki K, Muro
K, Yamaguchi K, Nishina T, Yuki S, Shitara K, Bando H, Mimaki S, et
al: Clinical significance of BRAF non-V600E mutations on the
therapeutic effects of anti-EGFR monoclonal antibody treatment in
patients with pretreated metastatic colorectal cancer: The
biomarker research for anti-EGFR monoclonal antibodies by
comprehensive cancer genomics (BREAC) study. Br J Cancer.
117:1450–1458. 2017.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Ueno H, Murphy J, Jass JR, Mochizuki H and
Talbot IC: Tumour ‘budding’ as an index to estimate the potential
of aggressiveness in rectal cancer. Histopathology. 40:127–132.
2002.PubMed/NCBI View Article : Google Scholar
|