Introduction
In late December 2019, a cluster of patients with
pneumonia of unknown origin that was epidemiologically linked to a
seafood and wet animal wholesale market in Wuhan, Hubei Province,
was reported in China (1). On
January 7, 2020, the causative pathogen was identified as a novel
β-coronavirus, subsequently named severe acute respiratory syndrome
coronavirus 2 (SARS-CoV-2). In the following weeks the infection
spread from a single city in China to other Chinese cities and
other countries around the world. On March 11, 2020, the World
Health Organization declared SARS-CoV-2 outbreak a global pandemic
(2).
Up until 28th of January, 2022, >370 million
cases of SARS-CoV-2 infections have been reported and almost 5.7
million individuals have died worldwide. So far, a total of
11,542,793 million cases have been reported in Italy, 148,542 of
which have died (3).
COVID-19 presents a highly variable spectrum of
severity of illness, ranging from mild flu-like symptoms to a
severe hypoxic pneumonia, which may require mechanical ventilation.
Life-threatening complications may include acute respiratory
distress syndrome (ARDS), multisystem organ failure, and
ultimately, death (4). Most
infected individuals who develop a symptomatic disease following
SARS-CoV-2 infection exhibit a mild to moderate illness (81%);
however, 14% will be considered to have a serious infection and 5%
progress to severe ARDS, requiring intensive care support (5).
The most common clinical manifestations of COVID-19
include fever, dry cough, headache, fatigue, dyspnea and diarrhea.
Patients can also present non-typical clinical manifestations such
as isolated gastrointestinal, olfactory and/or gustatory
dysfunctions (6). Most patients
exhibit lymphopenia on admission (7). Prothrombin time, D-dimer levels and
hypersensitive troponin I are also higher in intensive care unit
(ICU) patients (8). Multiple organ
dysfunction may occur in COVID-19; complications include impairment
of the heart, brain, lung, liver and kidney function and alteration
of the coagulation system (9).
Venous and arterial thromboembolic events are present in
hospitalized patients with COVID-19 with a variable incidence of
between 10-25% (10).
The mortality rate of COVID-19 continues to increase
across the world. Data regarding predictors of mortality in
patients with COVID-19 are still relatively scarce. Several
comorbidities have been shown to be associated with poor outcomes
in patients with COVID-19, such as hypertension, coronary heart
disease and diabetes. Some laboratory parameters were also examined
as predictors of death; high levels of cardiac troponin, IL-6,
C-reactive protein (CRP) and D-dimer seem to be correlated with
increased mortality. Older age is also associated with a higher
risk of death (11).
Characterization of the epidemiological features of
COVID-19 is crucial for the development and implementation of
effective therapeutic strategies. Here, the results of a
retrospective descriptive study of patients hospitalized in eight
clinical centers in Sicily (Italy), between 1st March and 18th May
2020 are presented.
Patients and methods
Study design and data sources
The present study was a multicenter retrospective
observational study. This multicenter study was coordinated by the
Infectious Diseases Unit of Presidio Ospedaliero Garibaldi Nesima
(Catania, Italy) and involved the Infectious Disease Units of other
seven Sicilian hospitals: Azienda Ospedaliera (AO) Cannizzaro
(Catania, Italy), AO Universitaria (AOU, Italy) Policlinico G.
Martino (Messina, Italy), AO Gravina (Caltagirone, Italy), AO
Umberto I (Enna, Italy), AOU Policlinico P. Giaccone (Palermo,
Italy), AO Umberto I (Siracusa, Italy), AO Maggiore (Modica,
Italy).
Clinical data were obtained from electronic medical
records or charts, and were collected using a centrally designed
electronic worksheet. Collected data included patients'
demographics, laboratory test results, historical and current
medication lists, historical and current diagnoses and clinical
notes. Specifically, the following information for each patient was
obtained: Hospital, date of admission and date of discharge or
death, age, sex, the first recorded inpatient laboratory tests at
admission [(including white blood cells, D-dimer, creatinine, CRP,
ferritin, aspartate aminotransferase (AST), alanine
aminotransferase (ALT), IL-6, lactate dehydrogenase (LDH)]; past
and current diagnoses (heart disease, hypertension, diabetes,
respiratory disease, obesity, chronic kidney disease, others); type
of oxygen therapy started upon hospital admission [nasal cannula
(NC), Venturi mask (VM), continuous positive airway pressure device
(CPAP) or high-flow nasal cannula (HFNC) oxygenation] and current
drug therapies for COVID-19 (hydroxychloroquine, azithromycin,
lopinavir/ritonavir or darunavir/cobicistat, tocilizumab,
corticosteroids and antibiotics). IL-6 levels were only tested in a
limited number of the patients (132 patients of 421).
Acute respiratory distress syndrome has been defined
using the Berlin Definition, as lung injury of acute onset,
bilateral opacities on chest imaging (chest radiograph or computed
tomography) not explained by another lung pathology, respiratory
failure not explained by heart failure or volume overload,
decreased PaO2/FiO2 ratio
(PaO2/FiO2 <300 mmHg) (12).
Study cohort
Hospitalized patients were included in this study if
they fulfilled two primary criteria: Age >18 years and having a
confirmed diagnosis of SARS-CoV-2 infection by a PCR test of a
nasopharyngeal sample. A total of 421 patients were recruited. The
median age of the included patients was 66 years (IQR 55-78 years),
ranging from 18-100 years; 235 (55.8%) were male and 186 were
female (44.2%).
Ethical approval
This research was conducted according to the
Declaration of Helsinki (13). It
was approved as a retrospective minimally invasive experimental
study by the Provincial Review Board of Catania on August 4th, 2020
(approval no. 492). Patients provided signed written informed
consent for the use of their data and samples for research purposes
at admission. All patients were >18 years of age. Each
Infectious Diseases Unit provided data from hospitalized patients
who had a positive test result for the SARS-CoV-2 virus between 1st
March and 18th May 2020. The data were collected by a member of the
medical team who treated the patient and all data were codified and
anonymized before statistical analysis.
Outcomes
The registered epidemiological data, demographics,
signs and symptoms on admission (fever, chills, cough, dyspnea,
ageusia, anosmia), pre-existing comorbidities, baseline laboratory
tests results, chest radiographic findings at baseline and during
follow-up, treatment received for COVID-19, highest level of
respiratory support, and clinical outcomes were recorded. The
primary endpoint was to correlate the clinical outcome of
hospitalized patients with SARS-CoV-2 infection, in terms of
recovery and death, to the clinical-laboratory characteristics of
the disease and the pre-existing comorbidities.
The secondary endpoint was to identify the
predictors of poor outcomes using a machine learning model opening
up the possibility for patient stratification and treatment
allocation.
Data analysis
Continuous variables are presented as the median and
interquartile range (IQR). Categorical variables are expressed as
the number of patients and percentage. The baseline demographic and
clinical-epidemiological characteristics of patients who recovered
and those with worse outcomes (ICU or death) were compared.
P<0.05 was considered to indicate a statistically significant
difference.
A Rényi test was used to compare survival. To
identify potential non-linear relations and interaction effects
among the investigated variables with the risk of death, machine
learning analysis was used to measure the predictive power of a
potential classification algorithm for the risk of death and to
establish variable importance in more complex mortality prediction
models. Risk models have been developed using decision-tree
induction from class-labelled training records and Cox proportional
hazard models. The training set was composed of records in which
one attribute (such as the presence or absence of carotid
atherosclerosis) was the dependent variable, and the remaining
attributes were the predictor variables; the individual records are
the tuples for which the class label is known. To establish the
robustness of predictor variables a K-Fold Cross Validation was
performed. The prediction quality of Decision Tree analysis has
performed using Receiver Operating Characteristic (ROC) curve
analysis. Statistical analysis was performed with the use of tools
for survival analysis and recursive partitioning analysis within
the R Statistical Software (14).
Results
Between March 1st and May 18th 2020, a total of 421
patients diagnosed with COVID-19 and hospitalized at one of eight
clinical centers across Sicily were included in this retrospective
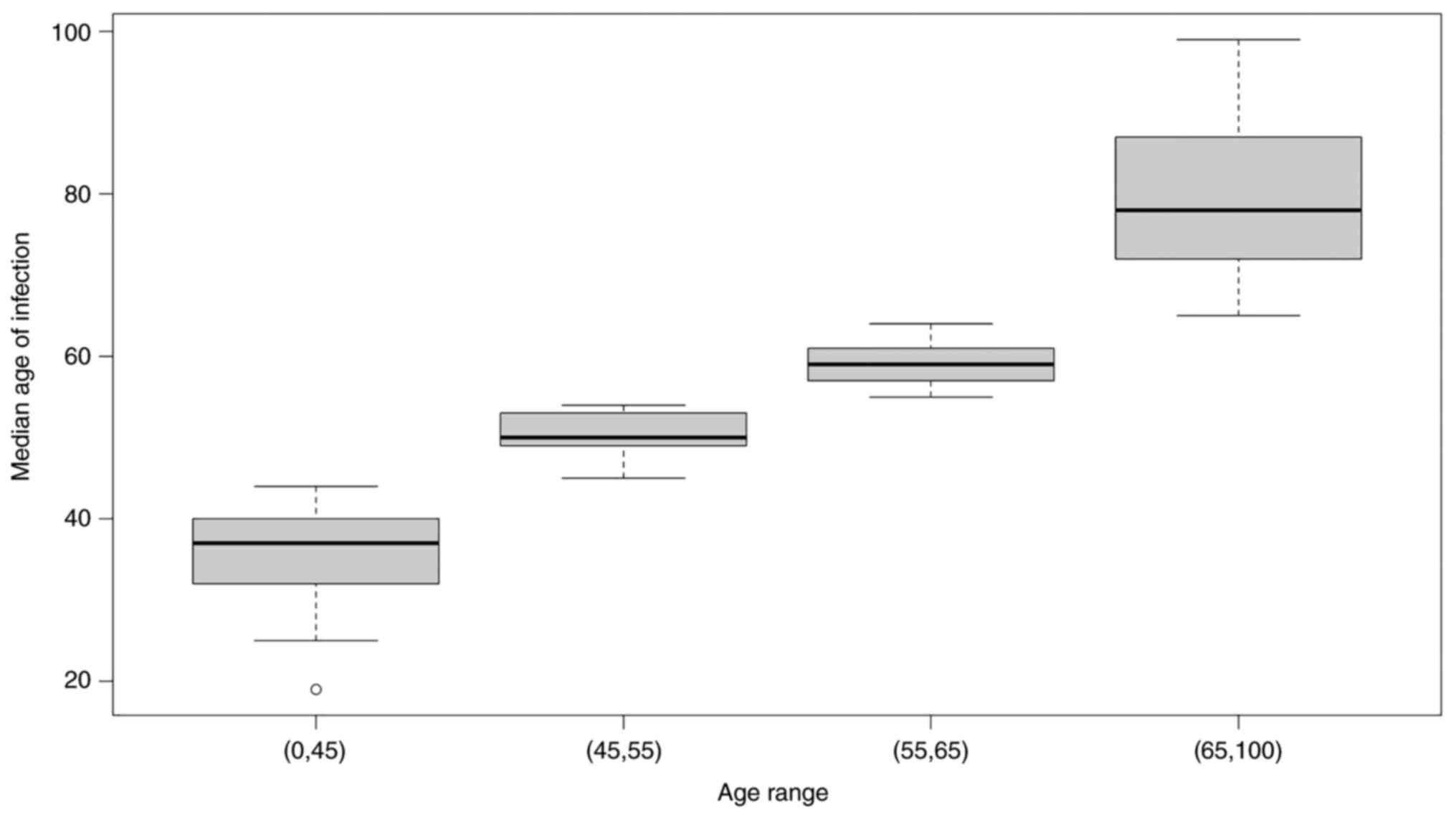
analysis. Table I shows the
baseline characteristics of the patients. Distribution of infected
people and the median age of each group is shown in Fig. 1.
 | Table IBaseline characteristics of patients
hospitalized with COVID-19. |
Table I
Baseline characteristics of patients
hospitalized with COVID-19.
| Parameter | No. (%) |
|---|
| Total N | 421 |
| Age, years, median
(range) | 66 (18-100) |
| Sex | |
|
Female | 186 (44.2%) |
|
Male | 235 (55.8%) |
| Asymptomatic | 47 (11.2%) |
| Symptoms | 373 (88.6%) |
|
Fever | 334 (79.3%) |
|
Dyspnoea | 195 (46.3%) |
|
Asthenia | 120 (28.5%) |
|
Cough | 195 (46.3%) |
|
Ageusia | 10 (2.4%) |
|
Anosmia | 10 (2.4%) |
| Comorbidity | 345 (82%) |
|
Hypertension | 227 (53.9%) |
|
Cardiovascular
disease | 115 (27.3%) |
|
Diabetes | 88 (20.9%) |
|
BPCO | 50 (11.9%) |
|
Chronic
kideney disease | 36 (8.6%) |
|
Obesity | 69 (16.4%) |
|
Others
(cancer, rheumatic disorders, etc.) | 242 (57.4%) |
| Oxygen
Requirement | |
|
Continuous
positive airway pressure | 69 (16.3%) |
|
High flow
nasal cannula | 36 (8.5%) |
|
Venturi mask
or nasal cannula | 284 (67.4%) |
On admission, most patients had fever (n=334,
79.3%), dyspnea (n=195, 46.3%) and fatigue (n=120, 28.5%). The
other symptoms included cough (n=195, 46.3%), ageusia (n=10, 2.4%),
and anosmia (n=10, 2.4%); 47 of 421 (11.2%) patients were
asymptomatic from exposure to admission.
Baseline laboratory findings are shown in Table II. The most common abnormalities in
blood counts included lymphopenia (61.1%) and neutrophilia (27.1%).
Additionally, 55.7% had D-dimer levels above the normal range. High
serum levels were reported for ALT (12.2%), AST (38.8%) and CRP
(83.2%). Ferritin and IL-6 were tested in a limited number of
patients, and high concentrations of these parameters were found in
100 of 137 (73%) and 79 of 136 (58%), respectively.
| Table IILaboratory results of patients
hospitalized with COVID-19. |
Table II
Laboratory results of patients
hospitalized with COVID-19.
| Blood
parameter | Mean | No. (%) | Reference
ranges |
|---|
| White blood cell
count, cells/mm3 | 7,126.75 | 137 (32.5%) | 4,300-10,300 |
|
Neutrophils,
cells/mm3 | 5,143.34 | 95 (27.1%) | 2,100-6,100 |
|
Lymphocytes,
cells/mm3 | 1,216.55 | 248 (61.1%) | 1,300-3,500 |
| C-reactive protein,
mg/dl | 6.95 | 346 (83.2%) | 0.01-0.50 |
| Ferritin,
ng/ml | 758.93 | 100 (73%) | 21-275 |
| Lactate
dehydrogenase, UI/l | 455.27 | 215 (81.4%) | 125-243 |
| Aspartate
aminotransferase, UI/l | 38.79 | 163 (38.8%) | 5-34 |
| Alanine
aminotransferase, UI/l | 37.50 | 51 (12.2%) | 0-55 |
| D-dimer, ng/ml | 1,582.12 | 200 (55.7%) | 0-500 |
| IL-6, pg/ml | 115.15 | 79 (58.0%) | 0-19 |
A total of 312 (74%) patients had findings of
bilateral infiltrates on radiographic imaging, while 28 (6.6%)
patients had unilateral infiltrates; 42 (10%) patients had no
evidence of pneumonia on admission. Of the 421 patients, 289
(68.6%) required oxygen support in the hospital; of these, 69
(16.3%) received oxygen therapy with CPAP, 36 (8.5%) with HFNC, and
284 (67.4%) with VM or NC. During hospitalization, 317 (75%) of the
421 patients developed ARDS, and 21 of these patients with ARDS
were admitted to ICUs; 5 patients died in the Infectious Disease
Units. Overall mortality increased with age (88.6% of deaths
occurred in people >75 years). Of the total cohort, 346 (82.2%)
patients achieved clinical recovery, 31 (7.4%) patients were
transferred to an ICU and 44 (10.4%) died during hospitalization in
the Infectious Disease Unit.
Of the 421 patients recruited, 252 (59.8%) received
treatment with hydroxychloroquine plus azithromycin, 88 (20.9%)
patients received hydroxychloroquine alone, 120 (28.5%) patients
received lopinavir/ritonavir, 78 (18.5%) patients received
darunavir/cobicistat and 86 (20.4%) patients received tocilizumab;
294 (70%) also underwent antibiotic therapy.
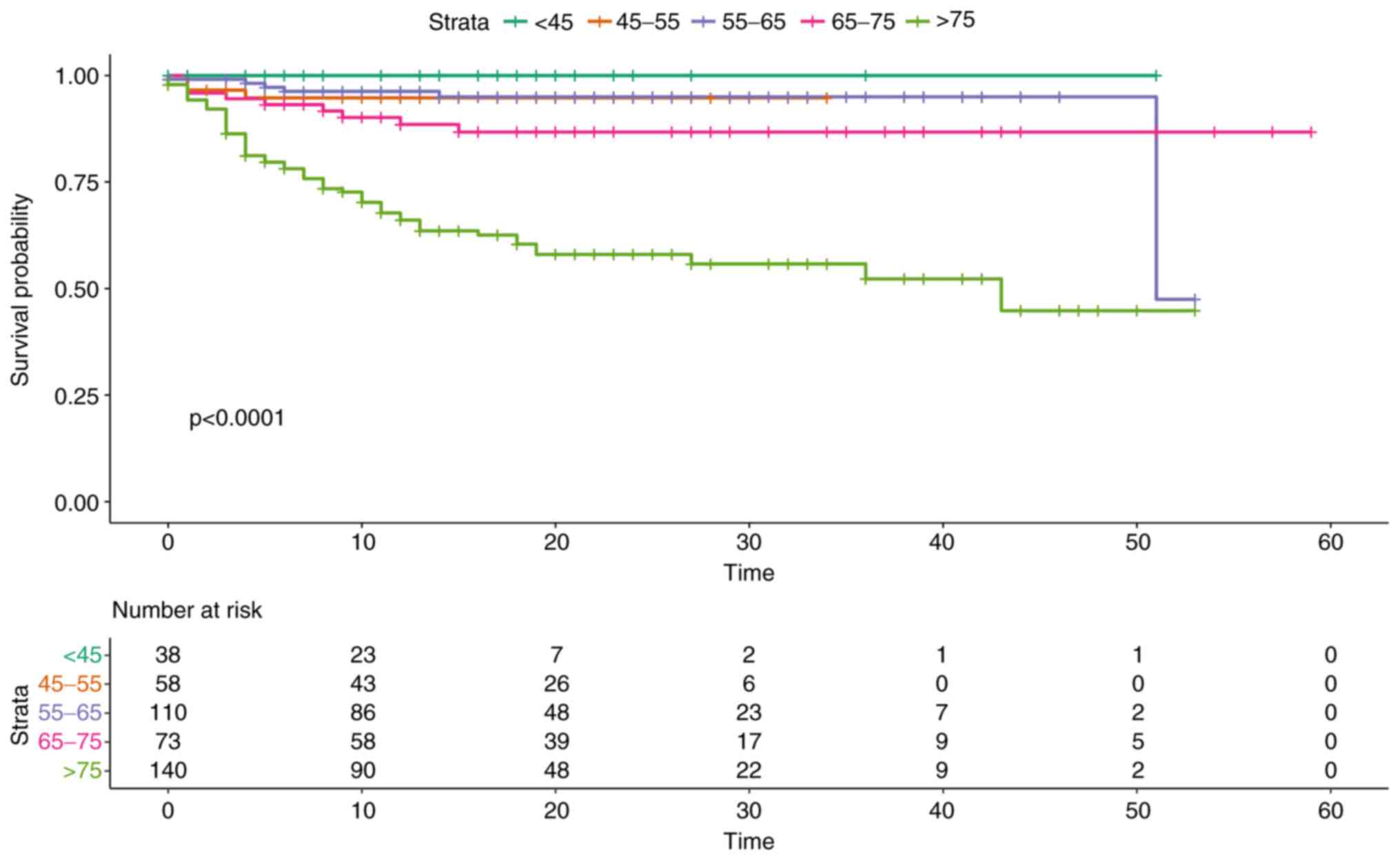
Overall survival did not show statistically
significant differences between the two sexes (P=0.9). Overall
survival in relation to age groups, on the other hand, highlighted
how age represents one of the main predictors of an unfavorable
outcome, with an increased risk for people aged >75 years
(P<0.0001, Fig. 2).
The majority of the patients (n=345, 82%) had at
least one comorbidity, including hypertension (n=227, 53.9%),
cardiovascular diseases (n=115, 27.3%), diabetes (n=88, 20.9%),
chronic obstructive pulmonary disease (COPD) (n=50, 11.9%), chronic
kidney disease (n=36, 8.6%), obesity (n=69, 16.4%), and others
(including cancer, rheumatic disorders, etc.) (n=242, 57.4%). The
presence of comorbidities was associated with a reduced survival in
our population. Specifically, the greatest significance was found
for hypertension (P=0.000091), heart disease (P=0.0008) and chronic
renal failure (P=0.002), while the data analysis showed how the
presence of diabetes is only slightly statistically significant for
worse outcome. (P=0.031).
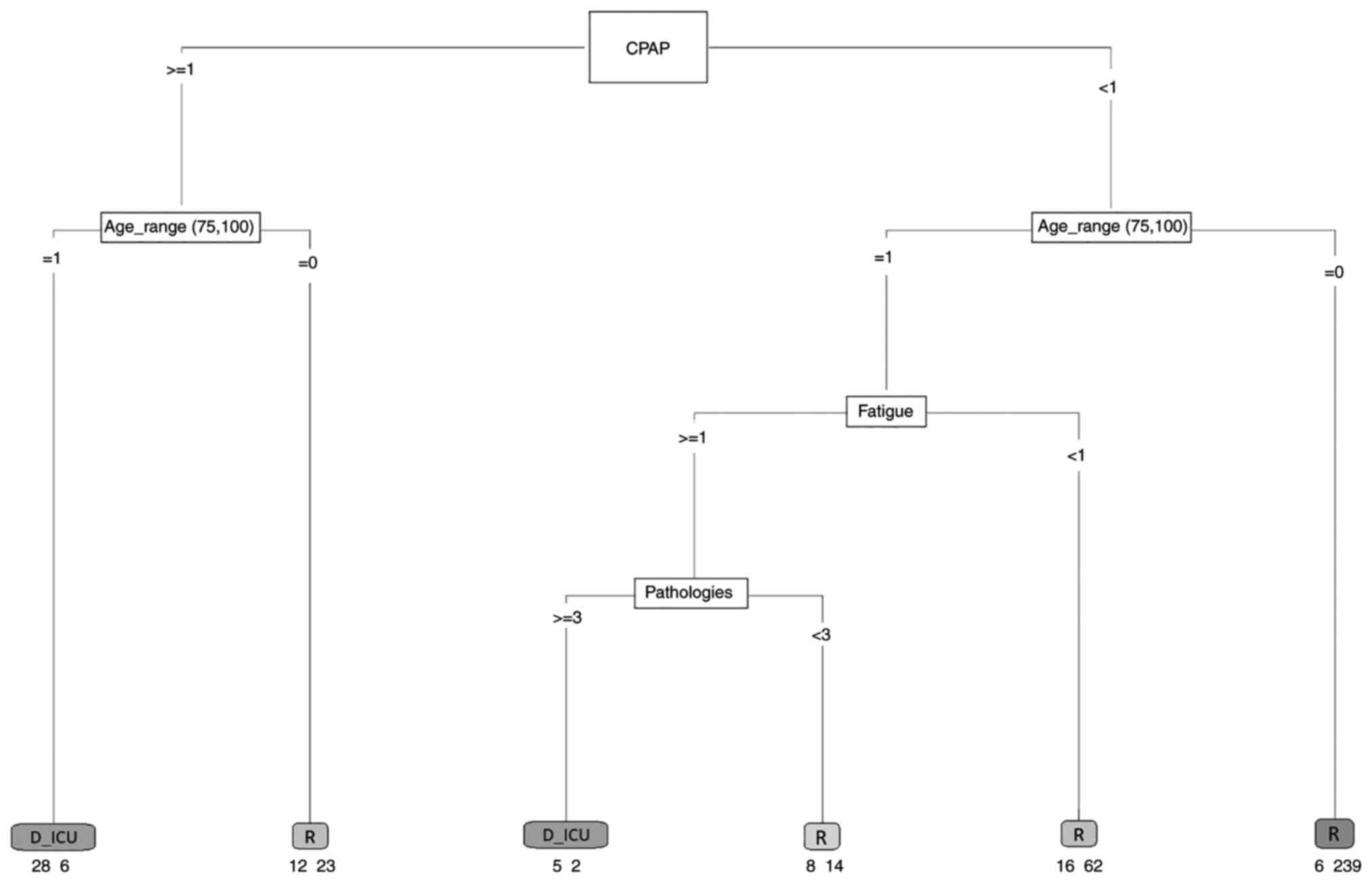
A first risk model was developed to identify those
variables that in the sample mostly influenced the outcome of the
patient. The patients were stratified into two groups: The first
group included those who recovered, and the second group consisted
of patients with a negative outcome (ICU or death). A model
including all the hematological and clinical variables associated
with each patient was developed. To understand the effect of
comorbidities, a variable storing the number of comorbidities each
patient had was defined. Age was stratified as follows: <45
years, 45-55, 56-65 and >66. The variables that significantly
were able to predict the outcome were: Fatigue, CPAP, age and
number of pathologies. The generated model had an area under the
ROC curve of 0.82, a sensitivity of 0.42 and a specificity equal to
0.97. Although the sensitivity of the model is low, the results
show that predicting variables have a clear role in the outcome of
the illness. The results are presented in Fig. 3.
Discussion
More than a year after its onset, the SARS-CoV-2
pandemic still represents a global emergency, and it accounts for
serious clinical complications in 10-20% of infected subjects.
Since the beginning of the pandemic, Italy has been heavily
affected.
Data from Northern Italy have found that patients
with concomitant cardiac disease and COVID-19 have a poor prognosis
compared with subjects without a history of cardiac disease
(15). A study that included 1,761
patients from 13 regions in Italy showed that age and comorbidities
are the most important predictors of death among COVID-19 patients
(16).
The present multicenter retrospective observational
study provides a complete description of the demographic and
clinical characteristics, comorbidities and laboratory
abnormalities in a cohort of 421 hospitalized patients recruited in
eight Infectious Disease Units in Southern Italy (Sicily) and aims
to identify the baseline characteristics predisposing COVID-19
patients to critical illness or death.
The median age of the included patients was 66 years
(IQR 55-78 years), which was similar to that reported in other
studies (17,18). Similar to data from China (19), those collected in the present study
relating to demographic factors showed how old age is significantly
associated with a reduced probability of survival. This evidence
supports research findings that outline how age is one of the most
important predictors of serious illness and mortality. It is likely
that age-related alterations in immunological functions and type 2
cytokine production seem to lead to deficiencies in controlling
SARS-CoV-2 replication and pro-inflammatory responses, as suggested
by Zhou et al (20).
In contrast to other studies, which have suggested
that male sex may be associated with a higher risk of developing
severe and fatal COVID-19, the incidence of illness was similar in
the two sexes in the present study with no significant differences
in terms of overall survival (21).
To date, several studies have reported the important
relationships between COVID-19 severity and mortality and specific
pathologies, partly supporting the present research. A
meta-analysis based on data from 7 studies in China found that
hypertension, diabetes, respiratory system disease and
cardiovascular disease were more frequent in severe patients
(22). Another systematic review of
14 articles involving 4,659 patients, observed that hypertension
increases the risk of death from COVID-19 by >2.5-fold (11). The mechanisms underlying the
association between cardiovascular disease and COVID-19 remain
unclear, but it may be due to infection-related ischemia that
progresses to myocardial injury and/or a viral-induced inflammatory
storm causing shock and the ensuing ischemic-related injury. In
addition, a direct myocardial invasion of the virus mediated by
ACE2 receptors may be involved, and a hypercoagulable state with
thrombotic disorders were observed in certain patients. A possible
association between SARS-CoV-2 infection and cardiovascular events
has been recently hypothesized in a case report of a 59-year-old
woman affected by hypertension and metabolic disorders, treated for
a SARS-CoV-2 infection, who developed cardiac symptoms during the
first days of hospitalization (23).
Diabetes was not significantly associated with
severe COVID-19 infection-associated illness in the present study,
contrary to other meta-analyses (24) that have found how people affected
have a greater risk of severe/critical illness and in-hospital
mortality in diabetics. A possible explanation of this finding is
that there was a large percentage of individuals with undiagnosed
diabetes at admission in our hospitals. Several factors seem to
increase the risk of severe COVID-19 in diabetic subjects:
Diabetics often have compromised innate immunity, and thus, they
are more prone to contracting infections; furthermore, exaggerated
expression of pro-inflammatory cytokines in these subjects may
contribute to the cytokine storm that is observed in severe cases
of COVID-19(25).
Finally, it has been reported that patients with
chronic kidney disease exhibit increased expression of
ACE2(26), which may promote an
increase in viral load; moreover, considering the possibility of
harmful effects of the virus on the renal system, patients with
pre-existing chronic kidney disease have a higher risk of
mortality.
The majority of the patients in the present cohort
had abnormal laboratory tests at baseline. The analysis of the data
showed that patients with sustained systemic inflammatory response
had more unfavorable outcomes. Elevated values of CRP were
associated with a higher risk of death or transfer to an ICU in the
present study. Increased values of LDH and ferritin were not
significantly associated with a poorer outcome in the present
study. In line with these findings, Luo et al (27) found that serum CRP levels upon
admission were independently associated with adverse outcomes of
COVID-19. It has been shown that in pulmonary diseases marked by
inflammatory features, for example there is a typical increase in
serum CRP levels in response to inflammatory cytokines (27). Indeed, in individuals affected by
SARS-CoV-2, there is a dysregulated production of cytokines such as
IL-6, TNF-α and chemokines that can lead to ARDS, MOFS and recall
of inflammatory cells in the lungs with development of oedema and
alveolar damage (28). Elevated
values of IL-6 were associated with a higher risk of death and
transfer to ICU in the present cohort, although IL-6 levels were
only tested in a limited number of the patients (132 patients of
421).
Patients with lymphopenia and abnormal values of
neutrophils at the time of admission, had a worse outcome in the
present study. The baseline neutrophil-to-lymphocyte ratio has been
confirmed as a potential predictor for critical illness of
COVID-19(29). The exact
relationship behind this correlation remains unclear.
To take into account potential non-linear relations
and interaction effects among clinical and demographic risk factors
for severity of COVID-19, an attempt to estimate mortality risk in
COVID-19 patients using a machine learning algorithm was performed.
Although the model exploited a limited sample size and the
sensitivity was low, the results clearly showed that predictive
variables such as age, certain symptoms like fatigue, other
pre-existing pathologies and use of CPAP have a clear role in the
outcome of the illness.
At the beginning of the pandemic, international
guidelines did not recommend the use of CPAP in COVID-19 patients
because of the lack of randomized studies showing its efficacy,
concerns about infection dissemination and a possible delayed
endotracheal intubation. Therefore, CPAP was the object of
conflicting evidence. To date, its value in COVID-19 treatment
remains to be established. Early after the COVID-19 outbreak in
Italy, there was an expert consensus in favor of CPAP and
non-invasive ventilation as first-line treatments for the
associated acute hypoxemic respiratory failure (30). Ashish et al (31) found that use of CPAP early in the
course of a patient's admission is associated with reduced
mortality, whereas use of CPAP in patients with a longer stay in
hospital was associated with increased mortality (31).
Compared with CPAP therapy, the use of HFNC has been
associated in some studies with a lower mortality rate in hypoxemic
respiratory failure and with a decreased need of subsequent
intubation and ICU admission (32).
Furthermore, HFNC has been shown to be associated with a
significantly lower risk of bioaerosol dispersion, reducing the
risk of hospital-acquired infections for health workers (33). Case reports and case series have
demonstrated how patients may achieve a marked improvement in
respiratory function, as well as lower respiratory fatigue, with
better results on arterial gas analysis when treated early with
HFNC (34,35).
Further studies are needed to clarify if CPAP or
High-Flow Nasal Oxygen are clinically effective when compared with
standard oxygen therapy in patients with confirmed COVID-19.
The present study has some limitations that should
be addressed. Firstly, this was an observational, retrospective
analysis. Furthermore, although it was a multicenter study, it
consists of a limited sample size and patients belong to a small
geographic area that could not entirely reflect the international
situation. Finally, certain data regarding the clinical and
laboratory status of patients were missing in the medical
records.
COVID-19 has become a worldwide pandemic affecting
>370 million individuals. In 10-20% of COVID-19 patients, their
condition deteriorates to severe or critical illness, characterized
by ARDS and multiorgan dysfunction syndrome. No effective
treatments for severe patients have yet been identified. Early
identification of patients at risk of adverse outcomes has the
potential to enable more individualized treatment strategies and to
more efficiently utilize health care resources, increasing the
number of lives saved. In the present study, older age,
pre-existing comorbidities (hypertension, heart disease, chronic
renal failure and COPD) and some changes in laboratory markers at
the time of admission (neutrophilia, lymphocytopenia, increased
CRP), were associated with a higher risk of mortality. Male sex, on
the other hand, did not reach statistical significance.
The extensive actions taken by governments have
slowed down the epidemic; and vaccines and monoclonal antibodies
have further curbed the spread of COVID-19 worldwide. Although the
epidemic appears to be in decline in almost all regions of the
world, we may yet face further challenges. Understanding which
factors increase the risk of poor outcome will help us to better
face these challenges.
In conclusion, several prognostic models in
predicting adverse outcomes have been proposed, and the aim of the
present study was to identify the patients who were likely to
develop them. A machine learning model incorporating demographic,
clinical and laboratory variables was established. Symptoms such as
fatigue, older age, number of co-pathologies and use of CPAP were
the most significant contributors in the estimation of clinical
prognosis.
Acknowledgements
We would like to thank Dr Pietro Leanza (University
of Catania, Catania, Italy) for his assistance revising the
manuscript.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
FC wrote the paper. FC, VM, AM, APa, DS, RFDV and DL
collected the data. FB, MG, LL, VB, GV, AZ, AO, CI, SB, LG, AC, AF
and MADR provided clinical assistance to the patients. APu
performed the data analysis. MC, RB, SG, ST and GL searched
literature references. GN, BC and BMC critically revised the
manuscript. All authors have read and approved the final
manuscript. BC and BMC confirm the authenticity of all the raw
data.
Ethics approval and consent to
participate
This research was conducted according to the
Declaration of Helsinki. It was approved as a retrospective
minimally invasive experimental study by the Provincial Review
Board of Catania on August 4th, 2020 (approval no. 492). Patients
provided signed written informed consent for the use of their data
and samples for research purposes at admission.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Zhu N, Zhang D, Wang W, Li X, Yang B, Song
J, Zhao X, Huang B, Shi W, Lu R, et al: A novel coronavirus from
patients with Pneumonia in China, 2019. N Engl J Med. 382:727–733.
2020.PubMed/NCBI View Article : Google Scholar
|
|
2
|
World Health Organization (WHO): Rolling
updates on coronavirus disease (COVID-19). In: Events as they
happen. World Health Organization, Geneva, Switzerland, 2020.
|
|
3
|
World Health Organization (WHO): Novel
Coronavirus (COVID-19). In: Situation reports. World Health
Organization, Geneva, Switzerland, 2020.
|
|
4
|
Epidemiology Working Group for NCIP
Epidemic Response, Chinese Center for Disease Control and
Prevention. The epidemiological characteristics of an outbreak of
2019 novel coronavirus diseases (COVID-19) in China. Zhonghua Liu
Xing Bing Xue Za Zhi. 41:145–151. 2020.PubMed/NCBI View Article : Google Scholar : (In Chinese).
|
|
5
|
Wu Z and McGoogan JM: Characteristics of
and important lessons from the coronavirus disease 2019 (COVID-19)
outbreak in China: Summary of a Report of 72 314 cases from the
Chinese center for disease control and prevention. JAMA.
323:1239–1242. 2020.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Cevik M, Kuppalli K, Kindrachuk J and
Peiris M: Virology, transmission, and pathogenesis of SARS-CoV-2.
BMJ. 371(m3862)2020.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Henry B, Cheruiyot I, Vikse J, Mutua V,
Kipkorir V, Benoit J, Plebani M, Bragazzi N and Lippi G:
Lymphopenia and neutrophilia at admission predicts severity and
mortality in patients with COVID-19: A meta-analysis. Acta Biomed.
91(e2020008)2020.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J,
Wang B, Xiang H, Cheng Z, Xiong Y, et al: Clinical characteristics
of 138 hospitalized patients with 2019 novel coronavirus-infected
Pneumonia in Wuhan, China. JAMA. 323:1061–1069. 2020.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Zaim S, Chong JH, Sankaranarayanan V and
Harky A: COVID-19 and multiorgan response. Curr Probl Cardiol.
45(100618)2020.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Wiersinga WJ, Rhodes A, Cheng AC, Peacock
SJ and Prescott HC: Pathophysiology, transmission, diagnosis, and
treatment of coronavirus disease 2019 (COVID-19): A review. JAMA.
324:782–793. 2020.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Tian W, Jiang W, Yao J, Nicholson CJ, Li
RH, Sigurslid HH, Wooster L, Rotter JI, Guo X and Malhotra R:
Predictors of mortality in hospitalized COVID-19 patients: A
systematic review and meta-analysis. J Med Virol. 92:1875–1883.
2020.PubMed/NCBI View Article : Google Scholar
|
|
12
|
ARDS Definition Task Force. Ranieri VM,
Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E,
Camporota L and Slutsky AS: Acute respiratory distress syndrome:
The Berlin definition. JAMA. 307:2526–2533. 2012.PubMed/NCBI View Article : Google Scholar
|
|
13
|
World Medical Association. World Medical
Association Declaration of Helsinki: Ethical principles for medical
research involving human subjects. JAMA. 310:2191–2194.
2013.PubMed/NCBI View Article : Google Scholar
|
|
14
|
RStudio Team: Integrated development for
R. RStudio, Inc., Boston MA, 2015. http://www.rstudio.com/.
|
|
15
|
Inciardi RM, Adamo M, Lupi L, Cani DS, Di
Pasquale M, Tomasoni D, Italia L, Zaccone G, Tedino C, Fabbricatore
D, et al: Characteristics and outcomes of patients hospitalized for
COVID-19 and cardiac disease in Northern Italy. Eur Heart J.
41:1821–1829. 2020.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Iaccarino G, Grassi G, Borghi C, Ferri C,
Salvetti M and Volpe M: SARS-RAS Investigators. Age and
Multimorbidity Predict Death Among COVID-19 Patients: Results of
the SARS-RAS Study of the Italian Society of Hypertension.
Hypertension. 76:366–372. 2020.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Richardson S, Hirsch JS, Narasimhan M,
Crawford JM, McGinn T and Davidson KW: The Northwell COVID-19
Research Consortium. Barnaby DP, Becker LB, Chelico JD, et al:
Presenting characteristics, comorbidities, and outcomes among 5700
patients hospitalized with COVID-19 in the New York City Area.
JAMA. 323:2052–2059. 2020.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Giacomelli A, Ridolfo AL, Milazzo L, Oreni
L, Bernacchia D, Siano M, Bonazzetti C, Covizzi A, Schiuma M,
Passerini M, et al: 30-day mortality in patients hospitalized with
COVID-19 during the first wave of the Italian epidemic: A
prospective cohort study. Pharmacol Res. 158(104931)2020.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Wu C, Chen X, Cai Y, Xia J, Zhou X, Xu S,
Huang H, Zhang L, Zhou X, Du C, et al: Risk factors associated with
acute respiratory distress syndrome and death in patients with
coronavirus disease 2019 Pneumonia in Wuhan, China. JAMA Intern
Med. 180:934–943. 2020.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z,
Xiang J, Wang Y, Song B, Gu X, et al: Clinical course and risk
factors for mortality of adult inpatients with COVID-19 in Wuhan,
China: A retrospective cohort study. Lancet. 395:1054–1062.
2020.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Wenham C, Smith J and Morgan R: Gender and
COVID-19 Working Group. COVID-19: The gendered impacts of the
outbreak. Lancet. 395:846–848. 2020.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Yang J, Zheng Y, Gou X, Pu K, Chen Z, Guo
Q, Ji R, Wang H, Wang Y and Zhou Y: Prevalence of comorbidities and
its effects in patients infected with SARS-CoV-2: A systematic
review and meta-analysis. Int J Infect Dis. 94:91–95.
2020.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Ceccarelli M, Marino A, Cosentino F,
Moscatt V, Celesia BM, Gussio M, Bruno R, Rullo EV, Nunnari G and
Cacopardo BS: Post-infectious ST elevation myocardial infarction
following a COVID-19 infection: A case report. Biomed Rep.
16(10)2022.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Gold MS, Sehayek D, Gabrielli S, Zhang X,
McCusker C and Ben-Shoshan M: COVID-19 and comorbidities: A
systematic review and meta-analysis. Postgrad Med. 132:749–755.
2020.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Mantovani A, Byrne CD, Zheng MH and
Targher G: Diabetes as a risk factor for greater COVID-19 severity
and in-hospital death: A meta-analysis of observational studies.
Nutr Metab Cardiovasc Dis. 30:1236–1248. 2020.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Ejaz H, Alsrhani A, Zafar A, Javed H,
Junaid K, Abdalla AE, Abosalif KOA, Ahmed Z and Younas S: COVID-19
and comorbidities: Deleterious impact on infected patients. J
Infect Public Health. 13:1833–1839. 2020.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Luo X, Zhou W, Yan X, Guo T, Wang B, Xia
H, Ye L, Xiong J, Jiang Z, Liu Y, et al: Prognostic Value of
C-Reactive Protein in Patients with Coronavirus 2019. Clin Infect
Dis. 71:2174–2179. 2020.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Shah VK, Firmal P, Alam A, Ganguly D and
Chattopadhyay S: Overview of immune response during SARS-CoV-2
infection: Lessons from the past. Front Immunol.
11(1949)2020.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Liu J, Liu Y, Xiang P, Pu L, Xiong H, Li
C, Zhang M, Tan J, Xu Y, Song R, et al: Neutrophil-to-lymphocyte
ratio predicts critical illness patients with 2019 coronavirus
disease in the early stage. J Transl Med. 18(206)2020.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Vitacca M, Nava S, Santus P and Harari S:
Early consensus management for non-ICU acute respiratory failure
SARS-CoV-2 emergency in Italy: From ward to trenches. Eur Respir J.
55(2000632)2020.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Ashish A, Unsworth A, Martindale J, Sundar
R, Kavuri K, Sedda L and Farrier M: CPAP management of COVID-19
respiratory failure: A first quantitative analysis from an
inpatient service evaluation. BMJ Open Respir Res.
7(e000692)2020.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Rochwerg B, Granton D, Wang DX, Helviz Y,
Einav S, Frat JP, Mekontso-Dessap A, Schreiber A, Azoulay E, Mercat
A, et al: High flow nasal cannula compared with conventional oxygen
therapy for acute hypoxemic respiratory failure: A systematic
review and meta-analysis. Intensive Care Med. 45:563–572.
2019.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Li J, Fink JB and Ehrmann S: High-flow
nasal cannula for COVID-19 patients: Low risk of bio-aerosol
dispersion. Eur Respir J. 55(2000892)2020.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Marino A, Pampaloni A, Scuderi D,
Cosentino F, Moscatt V, Ceccarelli M, Gussio M, Celesia BM, Bruno
R, Borraccino S, et al: High-flow nasal cannula oxygenation and
tocilizumab administration in patients critically ill with
COVID-19: A report of three cases and a literature review. World
Acad Sci J. 2(23)2020.
|
|
35
|
Marino A, Cosentino F, Pampaloni A,
Scuderi D, Moscatt V, Ceccarelli M, Gussio M, Onorante A, Zagami A,
Torrisi S, et al: Role of tocilizumab and high flow nasal cannula
in the clinical management of severe covid-19. J Clin Trials.
10(427)2020.
|