Introduction
Osteoarthritis (OA) is the most common chronic
degenerative joint disease and its prevalence has grown by 113.25%
worldwide from 247.51 million cases in 1990 to 527.81 million cases
in 2019. It characterized by degenerative changes of cartilage,
bone and synovial tissue, and leading to disability, in particular
knee OA (1,2). Symptoms of OA include stiffness,
crepitus and swelling and joint pain is the hallmark of OA which
tends to worsen with physical activity (3). OA is defined by imbalance between
mechanical strain on cartilage and resistance (4) OA is a multifactorial disease,
including factors such as age, sex, obesity, genetic
predisposition, occupational knee-bending and joint trauma, but the
actual cause of OA remains unclear (5). Thus, the primary purpose of OA
treatment is to reduce pain and stiffness, slow disease progression
and improve joint function (6).
There are several treatment options available to patients with OA,
such as physical modalities and exercise, pharmacological
treatment, intra-articular (IA) injection of corticosteroids and
surgery, depending on the symptoms and severity of the disease
(7).
IA corticosteroids are administered into the joint
space and are used as an alternative therapeutic option for the
treatment of OA when oral medications are not effective to relieve
symptoms (8). IA injection of
corticosteroids has been widely used for >50 years to treat
patients with knee OA for pain relief and control of local
inflammation (9-11).
It acts directly on nuclear steroid receptors to alter synthesis of
cytokines and enzymes and to inhibit phospholipase A2, resulting in
a decrease in proinflammatory derivatives of arachidonic acid
(12). Moreover, corticosteroids
inhibit synthesis of prostaglandin and decrease the activity of
collagenase and production of interleukin-1 and tumour necrosis
factor α, which can degrade the cartilage (8). Nevertheless, use of corticosteroids is
still controversial due to their side effects, particularly when
used as a long-term treatment or used repeatedly (10).
The effects of corticosteroids on the articular
cartilage have been reported. Several studies have showed that both
short- and long-term IA injection of corticosteroids or its
combination with anaesthetics have no detrimental effect and do not
cause chondrocyte death in Macaca irus monkeys and patients
with OA (10,13,14).
On the other hand, adverse effects of corticosteroids on articular
chondrocytes have been reported. A decrease in chondrocyte density
has been reported in male Sprague-Dawley rats following 6 months of
corticosteroid injection (15).
Chondrocyte apoptosis induced by corticosteroids has been reported
in both mice transplanted with human articular cartilage and in
human chondrocyte cultures (15,16).
Moreover, the rate of apoptosis is increased both in in
vitro chondrocyte cultures and in osteochondral ex vivo
specimens when treated with combined corticosteroids and local
anaesthetics (17). Corticosteroids
are suggested to increase oxidative stress and alter expression of
cyclin-dependent kinase inhibitor 1A, growth differentiation factor
15 and protein c-Fos genes, which are involved in cell death and
chondrotoxicity (18). Moreover,
corticosteroids may inhibit proteoglycan metabolism by decreasing
aggrecan expression and proteoglycan concentration (19). Concerning the effects in patients, a
transient decrease of meniscal thickness and joint space width is
observed in the knee medial compartment of patients with knee OA
who receive corticosteroid injections for 1 year (20). Triamcinolone acetonide (TA),
methylprednisolone acetate, prednisolone acetate and betamethasone
are used to treat patients with OA and exhibit similar general
efficacies (21). These
corticosteroids provide good results for pain relief, especially TA
which is shown to be more effective than other corticosteroids
(22). On the other hand, viability
of both human and canine OA chondrocytes is significantly reduced
upon being treated with TA in a concentration-dependent manner
(18,23). Moreover, TA significantly increases
MMP-3 mRNA expression in chondrocytes, a gene involved in the
degradation of cartilage (24).
In addition to corticosteroids, hyaluronic acid (HA)
is commonly administered via IA injection to treat knee OA. HA is a
linear non-sulphated glycosaminoglycan that is composed of
repeating D-glucuronic acid and N-acetylglucosamine units (25,26).
It is found in multiple types of animal tissue, especially in the
extracellular and pericellular matrix of soft connective tissue
(25,26). HA provides viscoelasticity and
lubrication to synovial fluid and has an anti-inflammatory effect
(25). Moreover, exogenous HA
increases proteoglycan and chondrocyte HA synthesis, decreases
activity and production of MMPs and proinflammatory mediators and
acts as an immune regulator (26,27).
There are several studies on the effect of HA injection: Certain
studies have showed no significant differences following HA
injections and placebo in patients with knee OA (28,29),
while others have reported that IA HA injections increase the
short-term improvements in patients with early to moderate-onset
knee OA with a modest effect that peaks at ~6-18 weeks after
injection (30,31). Furthermore, a comparison between the
effects of corticosteroids and HA reported no differences when
comparing the Western Ontario and McMaster Universities Arthritis
Index (WOMAC) scores of patients treated with either
corticosteroids or HA at 6-month follow-up (32). However, at 6 months after injection,
HA is reported to be more effective than corticosteroids,
especially for movement restriction relief (33), while corticosteroids are reported to
be superior in reducing pain (33,34).
Although HA has become widely adopted to treat patients with OA,
whether it decreases pain remains unclear.
To the best of our knowledge, although IA injections
of corticosteroid and HA are widely used in patients with knee OA,
the effects of these drugs have been compared only by a limited
number of studies (7-13).
Moreover, the comparison of the IA knee injection effects of TA and
HA has not been studied. Therefore, the present study aimed to
assess the effects of IA corticosteroids or HA on the articular
cartilage of patients with knee OA. The structures and components
of articular cartilage and proteoglycan levels, as well as levels
of apoptosis and empty lacunae in chondrocytes, were analysed.
Materials and methods
Sample collection
In the present study, fresh knee articular
cartilages were collected from patients with knee OA who were
diagnosed with grade 3-4 on the Kellgren-Lawrence radiographic
grading scale (35) at the
Department of Orthopaedic Surgery, Faculty of Medicine, Thammasat
University Hospital (August 2019-March 2021). Demographic data is
presented in Table I. Patients were
separated into three groups depending on their clinical history.
Patients who had received IA injection of 40 mg Kanolone-F (TA
extended-release injectable suspension; L.B.S. Laboratory Limited)
within 6 months before total knee arthroplasty (TKA) were included
in the TA group (n=12). The HA group (n=7) included patients who
received IA injection of Synvisc® (Hylan G-F 20; Sanofi
S.A.) in the 6 months before TKA. Lastly, patients who had not
received IA injections with either TA and/or HA within 6 months
before TKA were included in the untreated group (n=12). After TKA,
eight knee articular cartilage samples from each patient, including
posterior lateral, posterior medial, anterior lateral, anterior
medial, tibia lateral, tibia medial, distal lateral and distal
medial, were collected and immediately soaked in 10% neutral
buffered formalin (Bio Optica Milano SpA) for 24 h at room
temperature. Other clinical data including age, sex, affected knee
side, weight and height were collected from all patients. All
procedures were approved by the Ethics Committee for Research in
Human Subjects, Faculty of Medicine, Thammasat University (approval
no. MTU-EC-OT-4-233/62; Pathumthani, Thailand) and conducted in
accordance with the Declaration of Helsinki. Written informed
consent was obtained from all patients.
 | Table ICharacteristics of participants in
TA, HA, and untreated groups. |
Table I
Characteristics of participants in
TA, HA, and untreated groups.
| Characteristic | TA (n=12) | HA (n=7) | Untreated
(n=12) | P-value |
|---|
| Male:female
(%) | 3:9
(25.00:75.00) | 2:5
(28.57:71.43) | 6:6
(50.00:50.00) | 0.4012 |
| Median age, years
(range) | 66 (49-87) | 76 (63-83) | 73 (59-82) | 0.2360 |
| Left:right knee
(%) | 4:8
(33.33:66.67) | 4:3
(57.14:42.86) | 5:7
(41.67:58.33) | 0.5975 |
| Median BMI,
kg/m2 (range) | 25.50
(18.70-28.90) | 27.00
(20.70-29.40) | 26.00
(20.90-36.40) | 0.3933 |
|
Normal:overweight:obese (%) | 5:7:0
(41.67:58.33:0) | 2:5:0
(28.57:71.43:0) | 3:6:3
(25.00:50.00:25.00) | 0.2265 |
Sample preparation
Formalin-fixed articular cartilage samples were cut
into 2x1x1 cm3 and were decalcified using 10% EDTA with
a commercial ultrasonic machine (Cavitator® ultrasonic
cleaner; Mettler Electronics Corp.; power, 85 watts; frequency, 67
kHz) for 8 h at room temperature (36). Then, the decalcified articular
cartilage samples were embedded in paraffin wax using a tissue
embedding machine (Leica Biosystems) according to a standard
histological protocol (37).
Haematoxylin and eosin (H&E) and
Alcian blue staining
A total of 16 slides of 3-µm paraffin-embedded
sections for each patient were prepared. Alcian blue staining
(Bio-Optica Milano SpA); Alcian blue 0.1 g in 100 ml of 3% acetic
acid was performed for 30 min while H&E staining (C.V.
Laboratories Co., Ltd.) was carried out according to the
manufacturer's procedure (1 g haematoxylin in 10 ml of ethanol).
Both staining steps were conducted at room temperature. H&E
staining was utilized to study the overall structure and components
of articular cartilage and chondrocytes using OA Research Society
International 0-6 histologic features grading (13,38).
The paraffin-embedded sections were mounted and scanned using
Aperio CS2 Scanscope (Leica Microsystems, Inc.) at 40X
magnification. All slides were graded by three operators (NK, TC,
and PC). The overall structure and components were graded as
follows: Grade 0, intact surface and cartilage morphology; grade 1,
intact surface; grade 2, surface discontinuity; grade 3, vertical
fissures; grade 4, erosion; grade 5, denudation and grade 6,
deformation (8). The grading score
was calculated based on the grade (0, grade 0-2; 1, grade 3-4 and
2, grade 5-6). A grading score <1 was interpreted as low
deformation while a grading score ≥1 was interpreted as high
deformation.
To study the proteoglycan levels in the articular
cartilage, 8 paraffin-embedded section from each patient was
stained with Alcian blue according to a standard histological
protocol (13). The
paraffin-embedded sections were mounted and scanned, as
aforementioned. The proteoglycan levels were graded as 0-10
staining intensity (0; no stain, 1; extremely weak, 2; very weak,
3; weak, 4; below average, 5; average, 6; above average, 7;
intense, 8; very intense, 9; extremely intense, 10; dark).
TUNEL assay
8 paraffin-embedded sections from each patient were
stained with TUNEL reagent to study the apoptosis of chondrocytes
and empty lacunae. ApopTag® Plus Peroxidase in
situ Apoptosis Detection kit (MilliporeSigma; cat. no. S7101)
was used according to a modified protocol. Briefly, the sections
were treated with proteinase K for 10 min at room temperature
following deparaffinization for nucleic acid retrieval. For
peroxidase blocking, the sections were treated with hydrogen
peroxide for 5 min at room temperature. Subsequently, the sections
were treated with equilibration buffer and terminal
deoxynucleotidyl transferase enzyme for 2 h in a hybridizer at
37˚C. The sections were washed with stop solution for 10 min and
treated with anti-digoxigenin peroxidase for 30 min at room
temperature. For colour development, the sections were treated with
3,3'-diaminobenzidine for 10 min at room temperature. Both
apoptosis and empty lacunae were graded as follows: 0, none; 1-24,
low; 25-75, moderate and 76-100%, high. Empty lacunae grading score
was classified as follows: 0, none/low; 1, moderate and high, 2. A
grading score <1 was interpreted as low levels of empty lacunae
while a grading score ≥1 was interpreted as high levels of empty
lacunae.
Statistical analysis
Clinical data of all patients, including age, sex,
affected knee side, weight and height, were recorded in Microsoft
Excel software (version 2021; Microsoft Corporation) and
statistical analysis was performed using GraphPad Prism (version no
9; GraphPad Software, Inc.). Data are presented as the mean ± SD.
The entire experiments were independently duplicate. All data were
tested for parametric distribution by Shapiro-Wilk test. Data such
as sex, affected knee side, overall structure, apoptosis, and empty
lacunae were analysed using χ2 test whereas age, BMI,
thickness of cartilage and proteoglycan levels were analysed using
Kruskal-Wallis's test followed by Dunn's multiple comparison for
comparisons between the three groups. Bonferroni's correction was
used for all statistical adjustment. P<0.05 was considered to
indicate a statistically significant difference.
Results
Clinical data of participants
The present study involved 31 patients with knee OA
who were separated into three groups: TA (38.71); HA (22.59) and
untreated (38.71%). Patients comprised 11 males and 20 females,
aged 49-87 years with a BMI range of 18.7-36.4 kg/m2. A
total of 13 patients were diagnosed with knee OA on the left side
and 18 with knee OA on the right side. No significant differences
between TA, HA and untreated groups were found in sex, age, knee
side, BMI and BMI category (Table
I).
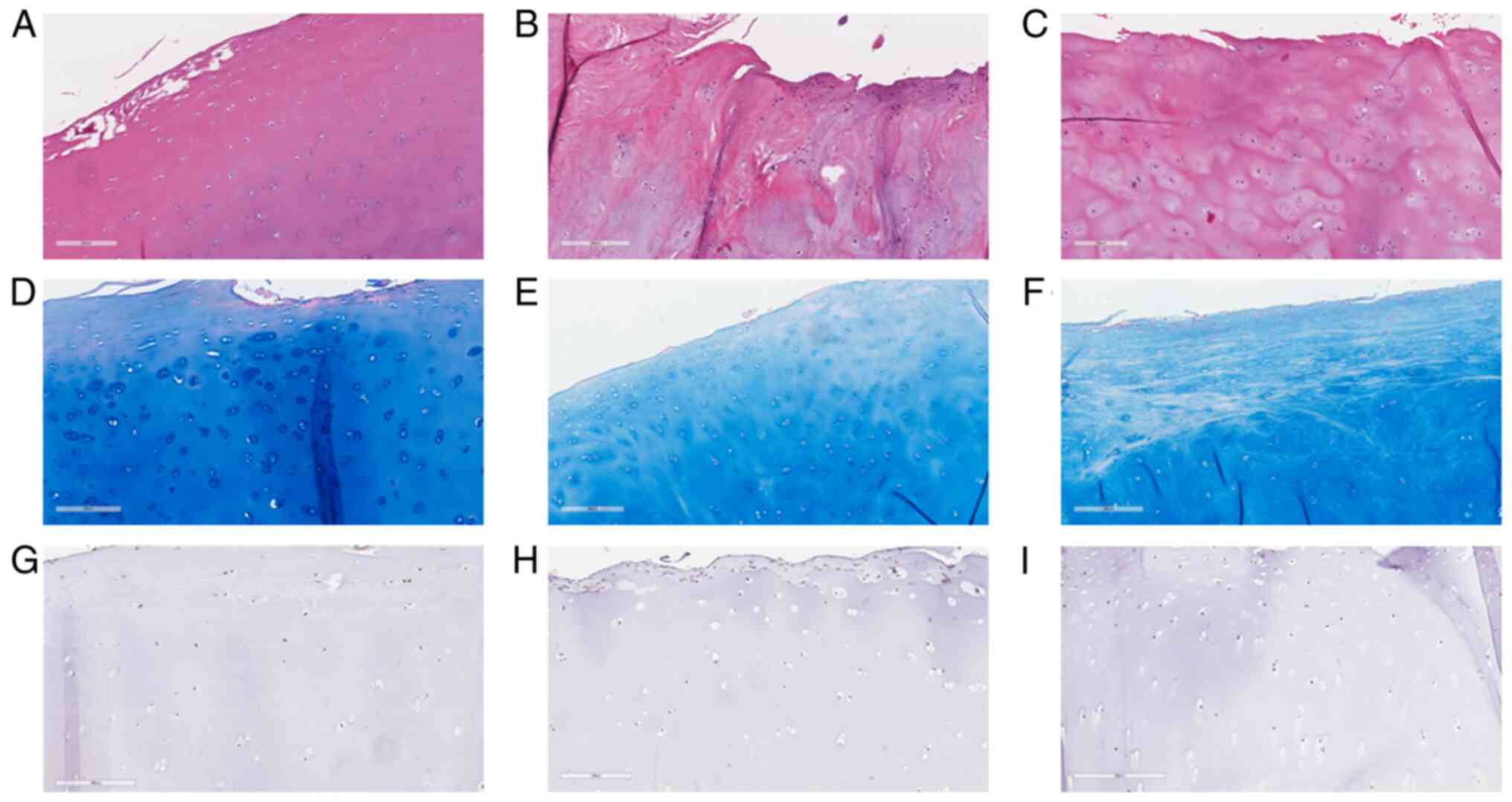
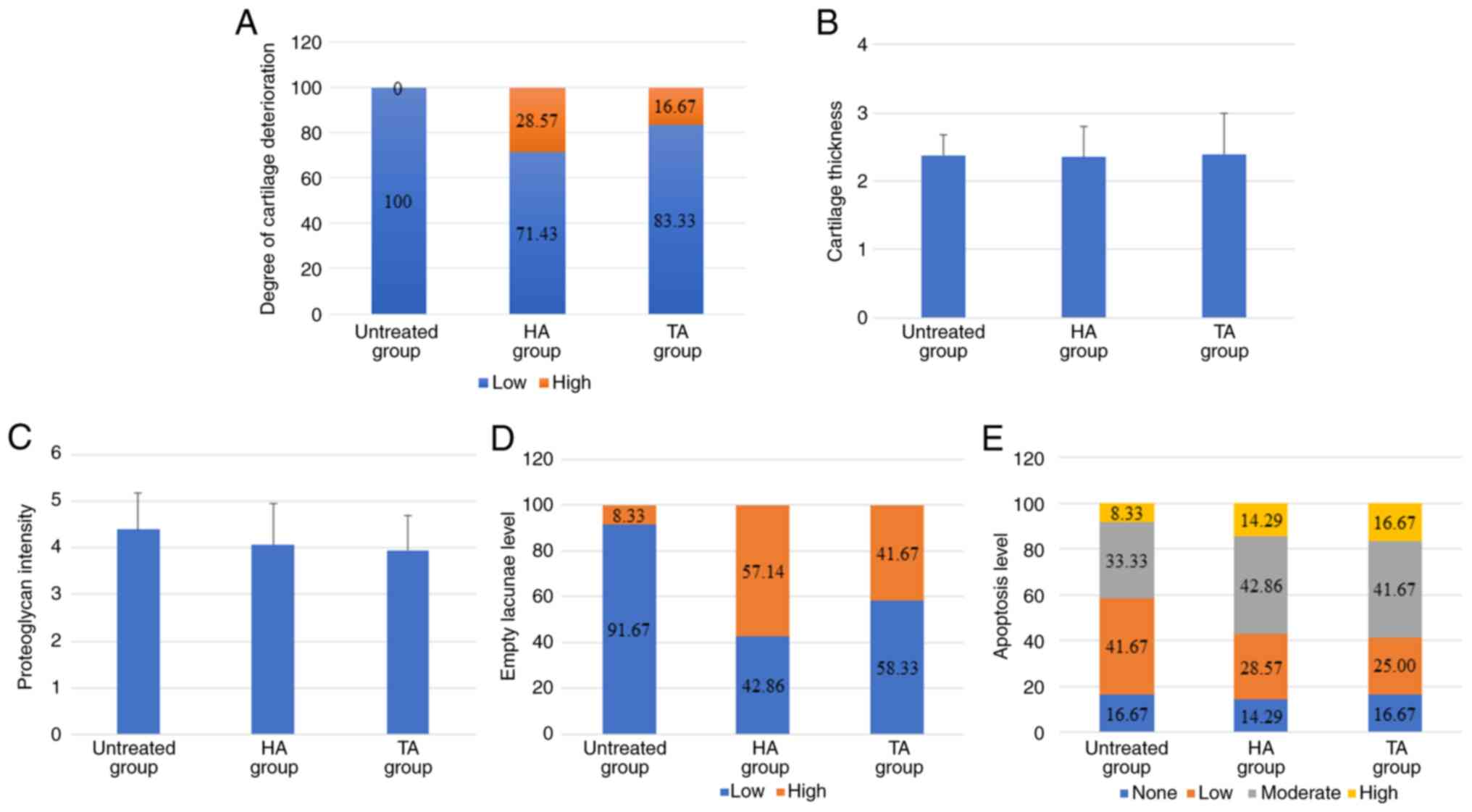
Histological observation
All the results exhibited non-parametric
distribution (Table SI). Almost
all the articular cartilage samples deterioration (Fig. 1). However, high levels of
deterioration were observed in both TA and HA groups (16.67 and
28.57% of patients, respectively) but not in the untreated group
(Figs. 1A-C and 2A). The TA group showed the highest
thickness of articular cartilage, while the HA group showed the
lowest thickness. No significant differences were found between the
three groups in both the overall structure and thickness of
articular cartilage (Fig. 2B). The
proteoglycan levels were analysed using Alcian blue staining
(Fig. 1D-F). The proteoglycan
levels in the TA and HA groups were decreased compared with those
in the untreated group, while those in the TA group were decreased
compared with those in the HA group, although no significant
difference was found between the three groups (Fig. 2C). Apoptosis and empty lacunae in
articular cartilage were studied by TUNEL assay (Fig. 1G-I). Between the three groups, there
were no statistically significant differences in empty lacunae and
apoptosis. The levels of empty lacunae in the HA group were
increased compared with that in the TA group while the level of
apoptosis showed no significant difference in these groups
(Fig. 2D and E).
Histological observations between
medial and lateral sides in 3 groups
In both TA and HA groups, no significant differences
between medial and lateral sides were observed in terms of
thickness and proteoglycan, empty lacunae, and apoptosis levels.
The deterioration of the medial side was significantly increased
compared with that of the lateral side in both TA and HA groups
(Table II). No significant
difference between medial and lateral sides was observed in
thickness, proteoglycan, and apoptosis levels in the untreated
group. The deterioration and empty lacunae levels of the medial
side were higher than those of the lateral side in the untreated
group (Table II).
| Table IIHistological features. |
Table II
Histological features.
| A, Triamcinolone
acetonide |
|---|
| Histological
feature | DM (n=9) | TM (n=6) | PM (n=8) | AM (n=7) | M (n=30) | DL (n=6) | TL (n=6) | PL (n=9) | AL (n=7) | L (n=28) |
P-valuea |
P-valueb |
|---|
| Median cartilage
thickness, mm (range) | 2.255
(1.048-4.632) | 2.550
(1.240-3.850) | 2.299
(1.927-3.853) | 2.676
(0.542-4.007) | 2.255
(0.542-4.632) | 1.825
(1.030-2.619) | 2.693
(1.777-4.531) | 2.554
(1.567-3.550) | 3.024
(1.602-3.885) | 2.367
(1.030-4.531) | 0.4535 | 0.9343 |
| Low:moderate:high
deterioration | 3:4:2 | 3:3:0 | 3:5:0 | 0:5:2 | 9:17:4 | 5:0:1 | 4:2:0 | 6:3:0 | 6:1:0 | 21:6:1 | 0.0551 | 0.0009 |
| Proteogylcan
intensity score | 3.778 | 4.375 | 3.813 | 3.286 | 3.806 | 3.958 | 4.042 | 4.222 | 4.036 | 4.025 | 0.8143 | 0.5925 |
| Low:moderate:high
levels of empty lacunae | 5:3:1 | 1:5:0 | 4:4:0 | 2:4:1 | 12:16:2 | 1:5:0 | 3:2:1 | 1:4:4 | 2:4:1 | 7:15:6 | 0.2398 | 0.1920 |
| Apoptosis (%) | 22.220 | 16.670 | 12.500 | 85.710 | 32.260 | 50.000 | 16.670 | 33.330 | 57.140 | 40.000 | 0.0017 | 0.2386 |
| B, Hyaluronic
acid |
| Histological
feature | DM (n=7) | TM (n=6) | PM (n=6) | AM (n=3) | M (n=22) | DL (n=6) | TL (n=2) | PL (n=6) | AL (n=3) | L (n=17) |
P-valuea |
P-valueb |
| Median cartilage
thickness, mm (range) | 2.046
(1.292-4.981) | 2.578
(1.621-3.779) | 2.184
(1.431-3.182) | 3.144
(2.090-3.375) | 2.288
(1.233-4.981) | 2.457
(1.702-3.300) | 2.168
(1.455-2.880) | 2.627
(1.862-4.476) | 2.882
(2.185-3.496) | 2.589
(1.455-4.476) | 0.6456 | 0.4617 |
| Low:moderate:high
deterioration | 1:4:2 | 3:2:1 | 0:6:0 | 0:3:0 | 4:15:3 | 5:1:0 | 0:2:0 | 3:3:0 | 3:0:0 | 11:6:0 | 0.0230 | 0.0081 |
| Proteogylcan
intensity score | 3.964 | 4.125 | 3.875 | 3.917 | 3.977 | 5.083 | 4.375 | 3.583 | 3.917 | 4.265 | 0.8111 | 0.4242 |
| Low:moderate:high
levels of empty lacunae | 3:4:0 | 0:5:1 | 2:4:0 | 1:1:1 | 6:14:2 | 1:4:1 | 1:0:1 | 2:2:2 | 1:1:1 | 5:7:5 | 0.6505 | 0.2101 |
| Apoptosis (%) | 42.860 | 33.330 | 16.670 | 33.330 | 31.820 | 33.330 | 50.000 | 66.670 | 0 | 41.180 | 0.0017 | 0.3175 |
| C, Untreated |
| Histological
feature | DM (n=11) | TM (n=9) | PM (n=11) | AM (n=4) | M (n=35) | DL (n=9) | TL (n=12) | PL (n=10) | AL (n=11) | L (n=42) |
P-valuea |
P-valueb |
| Median cartilage
thickness, mm (range) | 2.137
(1.380-4.902) | 2.283
(0.469-3.312) | 2.640
(0.778-4.218) | 2.686
(1.916-3.425) | 2.283
(0.469-4.902) | 2.344
(1.936-2.655) | 2.389
(1.274-3.845) | 2.604
(2.198-4.061) | 3.308
(1.829-4.436) | 2.5075
(1.274-4.436) | 0.1023 | 0.0843 |
| Low:moderate:high
deterioration | 7:4:0 | 5:4:0 | 5:6:0 | 2:2:0 | 19:16:0 | 9:0:0 | 11:1:0 | 7:3:0 | 10:1:0 | 37:5:0 | 0.0448 | 0.0041 |
| Proteogylcan
intensity score | 4.674 | 4.907 | 4.098 | 4.146 | 4.493 | 4.889 | 4.111 | 3.858 | 4.576 | 4.339 | 0.7214 | 0.4991 |
| Low:moderate:high
levels of empty lacunae | 9:1:1 | 8:1:0 | 6:2:3 | 2:1:1 | 25:5:5 | 6:3:0 | 7:5:0 | 4:6:0 | 9:2:0 | 26:16:0 | 0.0495 | 0.0060 |
| Apoptosis (%) | 25.910 | 34.890 | 12.730 | 40.000 | 48.900 | 42.890 | 50.000 | 33.330 | 70.910 | 41.180 | 0.0017 | 0.5575 |
Discussion
Knee OA is a degenerative joint disease
characterized by cartilage degeneration leading to disability in
the final stage. The primary goal in treating patients with knee OA
is to relieve pain (10). IA
injection is used to treat patients with knee OA when oral drugs
are not effective (39). IA
corticosteroid injections are typically used to treat patients with
knee OA to increase joint mobility, decrease joint inflammation and
reduce acute pain and swelling, although several adverse side
effects that have been reported (40). Several studies have reported the
side effects of corticosteroids on chondrocytes: Corticosteroids
induce chondrocyte apoptosis and decrease chondrocyte density at 6
months after administration (15-17).
Because of the adverse effects of corticosteroids,
IA HA injections are used to treat patients with knee OA. High
molecular weight HA is a component of synovial fluid that provides
joint lubrication and hyalin cartilage nutrients (41). Several animal models and clinical
trials have showed that IA HA injections are a more effective and
safer symptom-modifying therapy for decreasing pain of patients
with knee OA compared with steroids in short- and mid-term
(41,42). In addition, IA HA injection
significantly decrease chondrocyte apoptosis rate immediately after
administration in a rabbit model (43). However, to the best of our
knowledge, the are no studies comparing the effects of
corticosteroids and HA IA knee injections in patients with knee OA.
The present study aimed to compare the overall structure and
components of articular cartilage and proteoglycan, apoptosis, and
empty lacunae levels in the articular cartilage of patients with
knee OA.
The present study used human articular cartilage
from patients with knee OA who underwent TKA as these cartilage
samples can accurately represent the pathological conditions of
patients with OA. Patients in the TA group received IA injection of
Kanolone-F within 6 months prior to TKA, while patients in the HA
group received IA injection of Synvisc® within 6 months
prior to TKA. Patients in the untreated group did not receive TA or
HA within 6 months before TKA. TA is a classical corticosteroid
that is used to decrease pain in patients with OA and is more
effective than other corticosteroids for pain relief (22,44).
Moreover, TA injections activate anti-inflammatory macrophages by
inducing CD163+ and Folate receptor β expression.
Because of macrophage activation, osteophyte formation is prevented
and IL-10 production is reduced (22). By contrast, TA increases oxidative
stress and alters expression of cell death signals, leading to
chondrotoxicity (18). Moreover, TA
induces chondrocyte apoptosis both in cartilage layers and in
cultured chondrocytes (16). HA is
a linear polysaccharide composed of disaccharide repeats of
N-acetyl-glucosamine and glucuronic acid
[(1→3)-β-D-GlcNAc-(1→4)-β-D-GlcA-] and is found in the
extracellular matrix (26). HA
serves as a lubricant that can reduce friction between cartilage,
especially in its high molecular weight form (45). Patients with knee OA injected with 6
ml Hylan G-F 20 do not show greater pain relief compared with a
placebo group over a period of 26 weeks using WOMAC scores
(46). By contrast, certain studies
found that Hylan G-F 20 exerts better symptom improvement in the
early stage of knee OA compared with placebo and sodium hyaluronate
using Visual Analogue Scale and WOMAC scores (47,48).
Moreover, TA shows increased pain relief and knee functional
improvement compared with Hylan G-F 20 in the first and second
week, respectively; however, at 6 months follow-up, TA and Hylan
G-F 20 show similar results in pain relief, function and range of
motion (49). However, to the best
of our knowledge, side effects in patients, in particular apoptosis
rate, between corticosteroids and HA remains unclear.
Results from the present study revealed no
significant differences in all histological results including
deterioration, cartilage thickness and proteoglycan, empty lacunae
and apoptosis levels between TA and HA groups (Table III). To the best of our knowledge,
previous studies (7-13)
have focused mostly on TA and HA efficacy; however, the present
study aimed to investigate histological features of articular
cartilage treated with TA or HA injection. The present results
indicated that TA and HA were comparable in histological features.
Although TA induces apoptosis in chondrocyte culture and apoptosis
is observed in the superficial and middle layer of severe combined
immunodeficiency mouse cartilage (16), the present results indicated that
there was no difference in apoptosis levels following treatment
with TA or HA. Stove et al (19) showed that the corticosteroid
dexamethasone decreases proteoglycan concentration in vitro.
On this basis, the present study compared the proteoglycan levels
and showed that these were comparable between TA, HA and untreated
groups. Moreover, the cost of HA is higher than TA, which presents
a disadvantage (Table III)
(3,38). Conversely, the side effects are the
biggest disadvantage of TA. TA exerts rapid pain relief compared
with HA (34,50). Cost-effectiveness is a key concern.
The present results can assist doctors in choosing the suitable
treatment for patients with OA. Moreover, the present results
showed that the deterioration on the medial side was significantly
higher than on the lateral side in the untreated, HA and TA groups.
Consistent with this, knee OA most often presents in the medial
compartment of the joint with a prevalence 5-10 times higher than
in the lateral compartment because during walking, 60% of the load
goes through the medial side of the knee (51-53).
| Table IIIComparison of TA and HA for knee
osteoarthritis treatment (3,5-13). |
Table III
Comparison of TA and HA for knee
osteoarthritis treatment (3,5-13).
| Factor | TA vs. HA |
|---|
| Availability | TA>HA |
| Cost | TA<HA |
| Side effects | TA>HA |
| Histology | |
|
Deterioration | TA=HA |
|
Cartilage
thickness | TA=HA |
|
Proteoglycan
intensity | TA=HA |
|
Empty
lacunae | TA=HA |
|
Apoptosis | TA=HA |
In conclusion, the present histological results
showed that the TA and HA groups were comparable in terms of
deterioration, cartilage thickness and levels of proteoglycan,
empty lacunae, and apoptosis. The present results may inform
decisions about whether to use TA or HA in the treatment of knee
OA, but patient financial and health status should be
considered.
Supplementary Material
Parametric distribution.
Acknowledgements
Not applicable.
Funding
Funding: The present study was supported by the 90th Anniversary
of Chulalongkorn University Fund (Ratchadaphiseksomphot Endowment
Fund; grant no. 3/2563) and the 100th Anniversary Chulalongkorn
University Fund for Doctoral Scholarship (grant no. 2/2560).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
PC and NK conceived the study, designed experiments,
analyzed and interpreted data, and wrote the manuscript. PC, RT,
TC, and NT interpreted data. PC and NK confirm the authenticity of
all the raw data. All authors have read and approved the final
manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethic
Committee for Research in Human Subjects, Faculty of Medicine,
Thammasat University (approval no. MTU-EC-OT-4-233/62; Pathumthani,
Thailand) and conducted in accordance with the Declaration of
Helsinki. All participants provided written informed consent.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Plotnikoff R, Karunamuni N, Lytvyak E,
Penfold C, Schopflocher D, Imayama I, Johnson ST and Raine K:
Osteoarthritis prevalence and modifiable factors: A population
study. BMC Public Health. 15(1195)2015.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Braun HJ and Gold GE: Diagnosis of
Osteoarthritis: Imaging. Bone. 51:278–288. 2012.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Sinusas K: Osteoarthritis: Diagnosis and
treatment. Am Fam Physician. 85:49–56. 2012.PubMed/NCBI
|
|
4
|
Sulzbacher I: Osteoarthritis: Histology
and pathogenesis. Wien Med Wochenschr. 163:212–219. 2013.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Das SK and Farooqi A: Osteoarthritis. Best
Pract Res Clin Rheumatol. 22:657–675. 2008.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Arya RK and Jain V: Osteoarthritis of the
knee joint: An overview. Indian Acad Clin Med. 14:154–162.
2013.
|
|
7
|
Ringdahl E and Pandit S: Treatment of knee
osteoarthritis. Am Fam Physician. 83:1287–1292. 2011.PubMed/NCBI
|
|
8
|
Neustadt DH: Intra-articular injections
for osteoarthritis of the knee. Cleve Clin J Med. 73:897–898.
901–904. 906–911. 2006.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Nguyen C and Rannou F: The safety of intra
articular injections for the treatment of knee osteoarthritis: A
critical narrative review. Expert Opin Drug Saf. 16:897–902.
2017.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Raynauld JP, Buckland-Wright C, Ward R,
Choquette D, Haraoui B, Martel-Pelletier J, Uthman I, Khy V,
Tremblay JL, Bertrand C and Pelletier JP: Safety and efficacy of
long-term intraarticular steroid injections in osteoarthritis of
the knee A randomized, double-blind, placebo-controlled trial.
Arthritis Rheum. 48:370–377. 2003.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Takagi S and Blaha JD: The suitable use of
intra-articular corticosteroid injection in knee osteoarthritis.
Osteoarthritis and Cartilage. 26 (Suppl 1)(S291)2018.
|
|
12
|
Creamer P: Intra-articular corticosteroid
injections in osteoarthritis: Do they work and if so, how? Ann
Rheum Dis. 56:634–636. 1997.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Gibson T, Burry HC, Poswillo D and Glass
J: Effect of intra-articular corticosteroid injections on primate
cartilage. Ann Rheum Dis. 36:74–79. 1976.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Syed HM, Green L, Bianski B, Jobe CM and
Wongworawat MD: Bupivacaine and triamcinolone may be toxic to human
chondrocytes: A pilot study. Clin Orthop Relat Res. 469:2941–2947.
2011.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Chu CR, Coyle CH, Chu CT, Szczodry M,
Seshadri V, Karpie JC, Cieslak KM and Pringle EK: In vivo effects
of single intra-articular injection of 0.5% bupivacaine on
articular cartilage. J Bone Joint Surg Am. 92:599–608.
2010.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Nakazawa F, Matsuno H, Yudoh K, Watanabe
Y, Katayama R and Kimura T: Corticosteroid treatment induces
chondrocyte apoptosis in an experimental arthritis model and in
chondrocyte cultures. Clin Exp Rheumatol. 20:773–781.
2002.PubMed/NCBI
|
|
17
|
Farkas B, Kvell K, Czompoly T, Illes T and
Bardos T: Increased chondrocyte death after steroid and local
anesthetic combination. Clin Orthop Relat Res. 468:3112–3120.
2010.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Suntiparpluacha M, Tammachote N and
Tammachote R: Triamcinolone acetonide reduces viability, induces
oxidative stress, and alters gene expressions of human
chondrocytes. Eur Rev Med Pharmacol Sci. 20:4985–4992.
2016.PubMed/NCBI
|
|
19
|
Stove J, Schöniger R, Huch K, Brenner R,
Günther KP, Puhl W and Scharf HP: Effects of dexamethasone on
proteoglycan content and gene expression of IL-1beta-stimulated
osteoarthrotic chondrocytes in vitro. Acta Orthop Scand.
73:562–567. 2002.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Pelletier JP, Raynauld JP, Abram F, Dorais
M, Paiement P and Martel-Pelletier J: Intra-articular
corticosteroid knee injection induces a reduction in meniscal
thickness with no treatment effect on cartilage volume: A
case-control study. Sci Rep. 10(13789)2020.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Uthman I, Raynauld JP and Haraoui B:
Intra-articular therapy in osteoarthritis. Postgrad Med J.
79:449–453. 2003.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Siebelt M, Korthagen N, Wei W, Groen H,
Bastiaansen-Jenniskens Y, Müller C, Waarsing JH, de Jong M and
Weinans H: Triamcinolone acetonide activates an anti-inflammatory
and folate receptor-positive macrophage that prevents osteophytosis
in vivo. Arthritis Res Ther. 17(352)2015.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Euppayo T, Siengdee P, Buddhachat K,
Pradit W, Chomdej S, Ongchai S and Nganvongpanit K: In vitro
effects of triamcinolone acetonide and in combination with
hyaluronan on canine normal and spontaneous osteoarthritis
articular cartilage. In Vitro Cell Dev Biol Anim. 52:723–735.
2016.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Suntiparpluacha M, Tammachote N and
Tammachote R: Triamcinolone acetonide alters expressions of matrix
metalloproteinase-3 gene in primary human chondrocytes. Genomics
and Genetics. 9:66–71. 2016.
|
|
25
|
Altman RD, Manjoo A, Fierlinger A, Niazi F
and Nicholls M: The mechanism of action for hyaluronic acid
treatment in the osteoarthritic knee: A systematic review. BMC
Musculoskelet Disord. 16(321)2015.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Necas J, Bartosikova L, Brauner P and
Kolar J: Hyaluronic acid (hyaluronan): A review. Veterinarni
Medicina. 53:397–411. 2008.
|
|
27
|
Moreland LW: Intra-articular hyaluronan
(hyaluronic acid) and hylans for the treatment of osteoarthritis:
Mechanisms of action. Arthritis Res Ther. 5:54–67. 2003.PubMed/NCBI View
Article : Google Scholar
|
|
28
|
Neustadt D, Caldwell J, Bell M, Wade J and
Gimbel J: Clinical effects of intraarticular injection of high
molecular weight hyaluronan (Orthovisc) in osteoarthritis of the
knee: A randomized, controlled, multicenter trial. J Rheumatol.
32:1928–1936. 2005.PubMed/NCBI
|
|
29
|
Diracoglu D, Vural M, Baskent A, Dikici F
and Aksoy C: The effect of viscosupplementation on neuromuscular
control of the knee in patients with osteoarthritis. J Back
Musculoskelet Rehabil. 22:1–9. 2009.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Day R, Brooks P, Conaghan PG and Petersen
M: Multicenter Trial Group. A double blind, randomized,
multicenter, parallel group study of the effectiveness and
tolerance of intraarticular hyaluronan in osteoarthritis of the
knee. J Rheumatol. 31:775–782. 2004.PubMed/NCBI
|
|
31
|
Trigkilidas D and Anand A: The
effectiveness of hyaluronic acid intra-articular injections in
managing osteoarthritic knee pain. Ann R Coll Surg Engl.
95:545–551. 2013.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Leopold SS, Redd BB, Warme WJ, Wehrle PA,
Pettis PD and Shott S: Corticosteroid compared with hyaluronic acid
injections for the treatment of osteoarthritis of the knee. A
prospective, randomized trial. J Bone Joint Surg Am. 85:1197–1203.
2003.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Jones AC, Pattrick M, Doherty S and
Doherty M: Intra-articular hyaluronic acid compared to
intra-articular triamcinolone hexacetonide in inflammatory knee
osteoarthritis. Osteoarthritis Cartilage. 3:269–273.
1995.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Abedi M, Kamkar P, Afshari M and Mirkazemi
M: Comparison of the effectiveness of intra-articular injections of
hyaluronic acid and corticosteroid in the treatment of patients
with knee osteoarthritis symptomse. Ortho & Rheum Open Access
J. 7(555704)2017.
|
|
35
|
Kohn MD, Sassoon AA and Fernando ND:
Classifications in Brief: Kellgren-Lawrence classification of
osteoarthritis. Clin Orthop Relat Res. 474:1886–1893.
2016.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Charnwichai P, Kitkumthorn N,
Ruangvejvorachai P, Wongphoom J, Meesakul T, Tammachote N and
Tammachote R: Rapid decalcification of articular cartilage and
subchondral bone using an ultrasonic cleaner with EDTA. Acta
Histochem. 125(152009)2023.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Al-Sabaawy HB, Rahawi AM and Al-Mahmood
SS: Standard techniques for formalin-fixed paraffin-embedded
tissue: A Pathologist's perspective. Iraqi J Veter Sci. 35:127–135.
2021.
|
|
38
|
Pritzker KP, Gay S, Jimenez SA, Ostergaard
K, Pelletier JP, Revell PA, Salter D and van den Berg WB:
Osteoarthritis cartilage histopathology: grading and staging.
Osteoarthritis Cartilage. 14:13–29. 2006.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Ayhan E, Kesmezacar H and Akgun I:
Intraarticular injections (corticosteroid,hyaluronic acid,platelet
rich plasma) for the knee osteoarthritis. World J Orthop.
5:351–361. 2014.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Brooks EM, Hu CH, Kingston KA and Matzkin
EG: Corticosteroid Injections: A review of sex-related side
effects. Orthopedics. 40:e211–e215. 2017.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Vaishya R, Pandit R, Agarwal AK and Vijay
V: Intra-articular hyaluronic acid is superior to steroids in knee
osteoarthritis: A comparative, randomized study. J Clin Orthop
Trauma. 8:85–88. 2017.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Migliore A and Granata M: Intra-articular
use of hyaluronic acid in the treatment of osteoarthitis. Clin
Interv Aging. 3:365–369. 2008.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Barreto RB, Sadigursky D, Rezende MU and
Hernandez AJ: Effect of hyaluronic acid on chondrocyte apoptosis.
Acta Ortop Bras. 23:90–93. 2015.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Rudnik-Jansen I, Schrijver K, Woike N,
Tellegen A, Versteeg S, Emans P, Mihov G, Thies J, Eijkelkamp N,
Tryfonidou M and Creemers L: Intra-articular injection of
triamcinolone acetonide releasing biomaterial microspheres inhibits
pain and inflammation in an acute arthritis model. Drug Deliv.
26:226–236. 2019.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Temple-Wong MM, Ren S, Quach P, Hansen BC,
Chen AC, Hasegawa A, D'Lima DD, Koziol J, Masuda KL, Lotz MK and
Sah RL: Hyaluronan concentration and size distribution in human
knee synovial fluid: Variations with age and cartilage
degeneration. Arthritis Res Ther. 18(18)2016.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Ke Y, Jiang W, Xu Y, Chen Y, Zhang Q, Xue
Q, Lin J, Ngai W, Nian G, Fazeli MS, et al: Efficacy and safety of
a single intra-articular injection of 6 ml Hylan G-F 20 compared to
placebo in Chinese patients with symptomatic knee osteoarthritis.
C-SOUND study, a 26-week multicenter double-blind randomized
placebo-controlled trial in China. BMC Musculoskelet Disord.
22(428)2021.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Chevalier X, Jerosch J, Goupille P, van
Dijk N, Luyten FP, Scott DL, Bailleul F and Pavelka K: Single,
intra-articular treatment with 6 ml hylan G-F 20 in patients with
symptomatic primary osteoarthitis of the knee: A randomised,
multicentre, double-blind, placebo controlled trail. Ann Rheum Dis.
69:113–119. 2010.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Chou CW, Lue KH, Lee HS, Lin RC and Lu KH:
Hylan G-F 20 has better pain Relief and cost-effectiveness than
sodium hyaluronate in treating early osteoarthritic knee in Taiwan.
J Formos Med Assoc. 108:663–672. 2009.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Tammachote N, Kanitnate S, Yakumpor T and
Panichkul P: Intra-Articular, Single-Shot Hylan G-F 20 hyaluronic
acid injection compared with corticosteroid in knee osteoarthritis.
A Double-Blind, Randomized Controlled Trial. J Bone Joint Surg Am.
98:885–892. 2016.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Penning LI, de Bie RA and Walenkamp GH:
Subacromial triamcinolone acetonide, hyaluronic acid and saline
injections for shoulder pain an RCT investigating the effectiveness
in the first days. BMC Musculoskelet Disord. 15(352)2014.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Jones RK, Chapman GJ, Findlow AH, Forsythe
L, Parkes MJ, Sultan J and Felson DT: A new approach to prevention
of knee osteoarthritis: Reducing medial load in the contralateral
knee. J Rheumatol. 40:309–315. 2013.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Felson DT, Nevitt MC, Zhang Y, Aliabadi P,
Baumer B, Gale D, Li W, Yu W and Xu L: High prevalence of lateral
knee osteoarthritis in Beijing Chinese compared with framingham
caucasian subjects. Arthritis Rheum. 46:1217–1222. 2002.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Prodromos CC, Andriacchi TP and Galante
JO: A relationship between gait and clinical changes following high
tibial osteotomyit. J Bone Joint Surg Am. 67:1188–1194.
1985.PubMed/NCBI
|