Introduction
In operable breast cancer, anthracycline-based
chemotherapy (1) and, more
recently, taxane-containing regimens (2–4) have
been effective in improving disease-free survival (DFS) and overall
survival (OS). Breast cancer comprises at least two different
entities that are defined according to estrogen receptor (ER)
expression. Numerous published studies (5–10)
have shown that the efficacy of chemotherapy is lower in patients
with ER-positive disease compared to patients with ER-negative
disease. Findings of previous studies (1,11)
suggested that, although less chemosensitive, ER-positive disease
includes a subset of patients who significantly benefit from
adjuvant chemotherapy. Although certain predictors are able to
identify which ER-positive patients derive benefits from
cyclophosphamide, methotrexate and fluorouracil (CMF), few data are
currently available (12–14) about how to predict the efficacy of
anthracyclines and either docetaxel or paclitaxel in this
group.
Various biological parameters have been studied
clinically for their ability to predict responses to anticancer
drugs, including: i) efflux (p-glycoprotein) (15) and metabolism (CYP3A4) (16,17);
ii) β-tubulin (somatic mutation of β-tubulin and change in
β-tubulin isotype levels) (18,19);
iii) cell cycle [human epidermal growth factor receptor 2 (HER2),
topIIα, Aurora-A] (20,21) and iv) apoptosis (p53, BCL2 and
thioredoxin) (22–24). The nuclear protein Ki67, which is
present in cycling cells, is an indicator of tumor proliferation.
Ki67 has shown strong prognostic effects and has been predictive of
a greater response to most chemotherapies (25–29).
The 2009 St. Gallen Consensus (30) recommended using markers of
proliferation, such as Ki67, to determine the optimal treatment for
early breast cancer.
The collagen gel droplet-embedded culture-drug
sensitivity test (CD-DST) is a newly developed in vitro
chemosensitivity test that has several advantages over conventional
tests, such as the human tumor clonogenic assay (HTCA), the
thymidine incorporation assay (TIA), the
3-(4,5-dimethylethiazol-2-yl)-2,5-dephenyltetrazolium bromide assay
(MTT), the differential staining cytotoxicity (DiSC) assay, the
histoculture drug response assay (HDRA) and the succinate
dehydrogenase inhibition test (SDI). The CD-DST exhibits a high
success rate in primary culture, requires a small number of cells,
eliminates contamination by fibroblasts using image analysis,
maintains the original growth characteristics and permits
evaluation by using physiological concentrations of drugs.
Feasibility of the CD-DST has been reported in breast (31), pancreatic and biliary tract
(32) as well as lung cancers
(33). One study (34) reported that the CD-DST is able to
predict the response to chemotherapy with high accuracy in breast
cancer patients.
In the present study, we examined the correlation
between Ki67 expression and CD-DST to evaluate the efficacy of
anthracyclines and taxanes in patients with ER-positive breast
cancer.
Materials and methods
Patients
CD-DST was performed in 68 patients with ER-positive
and HER2-negative invasive breast cancer who underwent surgery
between August 2001 and November 2006. The surgically resected
specimens were used for the CD-DST. Informed consent was obtained
from each patient and the study was approved by the Ethics
Committee of Gunma University.
CD-DST
Four anticancer drugs [adriamycin (ADM), epirubicin
(EPI), docetaxel (DOC) and paclitaxel (PTX)] were used for the
CD-DST. CD-DST was performed using a CD-DST kit
(Primaster®; Kurabou, Inc., Osaka, Japan), according to
a previously described method (31). In brief, each fresh breast tumor
specimen was minced with a scalpel, suspended in Hanks’ balanced
salt solution (HBSS), treated with Dispersion Enzyme Cocktail EZ
(including 1.0% collagenase; Kurabou, Inc.) and digested at 37°C
for 2 h. The dispersed cancer cells were collected by
centrifugation at 250 × g for 3 min, filtered through a
300-μm nylon mesh, washed in HBSS, suspended in PCM-1 medium
(Kurabou, Inc.) and incubated in a collagen gel-coated flask
(CG-flask; Kurabou, Inc.) in a CO2 incubator at 37°C for
24 h. The collagen gel in the CG-flask was dissolved in the cell
dispersion enzyme EZ. Consequently, only the viable cells that
adhered to the collagen gel were collected and used for sensitivity
tests. Type I collagen (Cellmatrix Type CD; Nitta Gelatin, Inc.,
Osaka, Japan), 10X F-12 medium and reconstitution buffer were mixed
together in ice water at a ratio of 8:1:1. The prepared tumor cell
suspension was added to the collagen solution so that the former
did not exceed 1/10 of the latter solution, with the final density
at 1×105 cells/ml. Three drops of the collagen-cell
mixture (30 μl/drop) were placed in each well of a 6-well
multiplate on ice and allowed to gel at 37°C in a CO2
incubator; the final concentration was ∼3×103
cells/collagen gel droplet. DF medium (3 ml) (Gibco-BRL,
Gaithersburg, MD, USA) was overlaid on each well 1 h later and
incubated in a CO2 incubator at 37°C overnight.
To predict the response to each agent, the
anticancer drugs were added (Table
I). Following removal of the medium containing the anticancer
drugs, each well was rinsed with 3 ml of HBSS twice, overlaid with
4 ml of PCM-2 (serum-free medium; Kurabou, Inc.) and incubated for
a further 7 days. On the 4th day of incubation the medium was
changed once. At the end of the incubation, neutral red was added
to each well at a final concentration of 50 μg/ml and
colonies in the collagen gel droplets were stained for 2 h. Each
collagen droplet was fixed with neutral formalin buffer, washed in
water and quantified by image analysis. The growth rates of the
control incubations were calculated as the total volume on Day
7/total volume on Day 0. In vitro sensitivity was expressed
as the percentage T/C ratio, where T was the total volume of the
treated group and C was the total volume of the control group; a
T/C ratio of ≤50% was considered to demonstrate in vitro
sensitivity. For this reason, tumors were dichotomized into
chemotherapy-sensitive and -resistant groups using a cut-off value
of 50% (T/C ratio).
 | Table IExposure conditions in CD-DST. |
Table I
Exposure conditions in CD-DST.
| Drug | Concentration
(μg/ml) | Exposure time
(h) | Clinical dose
(mg/m2) | AUC (in
vitro/human)a |
|---|
| ADM | 0.02 | 24 | 60 | 0.98 |
| EPI | 0.1 | 24 | 40 | 1.20 |
| DOC | 0.1 | 24 | 60 | 0.83 |
| PTX | 1.0 | 24 | 210 | 1.03 |
Immunohistochemical assay
Paraffin-embedded blocks from primary tumor
specimens were evaluated for ER and PgR by immunohistochemistry
(IHC), and for HER2 by IHC and fluorescent in situ
hybridization (FISH). Tumors were considered to express ER or PgR
if they showed at least 1% immunoreactive cells. Tumors were
considered to be HER2-positive if IHC was 3+, or in a few cases
with IHC 2+ results, if amplified by FISH. Ki67 expression was
assessed by IHC using the MIB-1 monoclonal antibody (1:200
dilution; Dako, Glostrup, Denmark). Immunostaining was performed
using an automated immunostainer (Autostainer; Dako) and the
results were assessed without the use of an image analysis system.
The percentage of cells showing definite nuclear immunoreactivity
among 2,000 invasive neoplastic cells in randomly selected,
high-power (magnification, ×400) fields at the periphery of the
tumor was recorded and the Ki67 labeling index (LI) was calculated.
Tumors were dichotomized into Ki67-high and -low tumors using the
arbitrary cut-off value of 30% in this study.
Statistical analysis
Statistical analysis was performed using
StatView® version 5.0. (SAS Institute, Inc.).
Associations between CD-DST and Ki67 expression were assessed using
Student’s t-test and Chi-square or Fischer’s exact tests in the
case of 2×2 variables.
Results
Patient characteristics
Patient characteristics are shown in Table II. The median age was 50 years
(range, 30–86 years). The proportion of patients with premenopausal
status (58.8%) was higher than that of patients with postmenopausal
status. More than half of the patients had a breast tumor of
>2.0 cm and were positive for lymph node metastasis.
| Table IIPatient characteristics. |
Table II
Patient characteristics.
| Total patients (n=68)
|
|---|
| Variables | No. | % |
|---|
| Age (years) | | |
| Median | 50 | |
| Range | 30–86 | |
| Menopausal
status | | |
| Pre- | 40 | 58.8 |
| Post- | 28 | 41.2 |
| ER (%) | | |
| <1 | 0 | 0 |
| ≥1 | 68 | 100 |
| PgR (%) | | |
| <1 | 9 | 13.2 |
| ≥1 | 59 | 86.8 |
| Tumor size
(cm) | | |
| ≤2.0 | 15 | 22.1 |
| >2.0 | 53 | 77.9 |
| Lymph node
metastasis | | |
| Negative | 27 | 39.7 |
| Positive | 41 | 60.3 |
| Nuclear grade | | |
| 1/2 | 42 | 61.8 |
| 3 | 26 | 38.2 |
| Ki67 LI | | |
| Low (≤30%) | 51 | 75.0 |
| High
(>30%) | 17 | 25.0 |
| LVI | | |
| 0/1 | 47 | 69.1 |
| 2/3 | 21 | 30.9 |
CD-DST
CD-DST was performed in 68 patients with ER-positive
and HER2-negative invasive breast cancer. Results for each
anticancer drug were as follows: ADM, 59 cases (86.8%); EPI, 56
cases (82.4%); DOC, 39 cases (57.3.%) and PTX, 39 cases (57.3%).
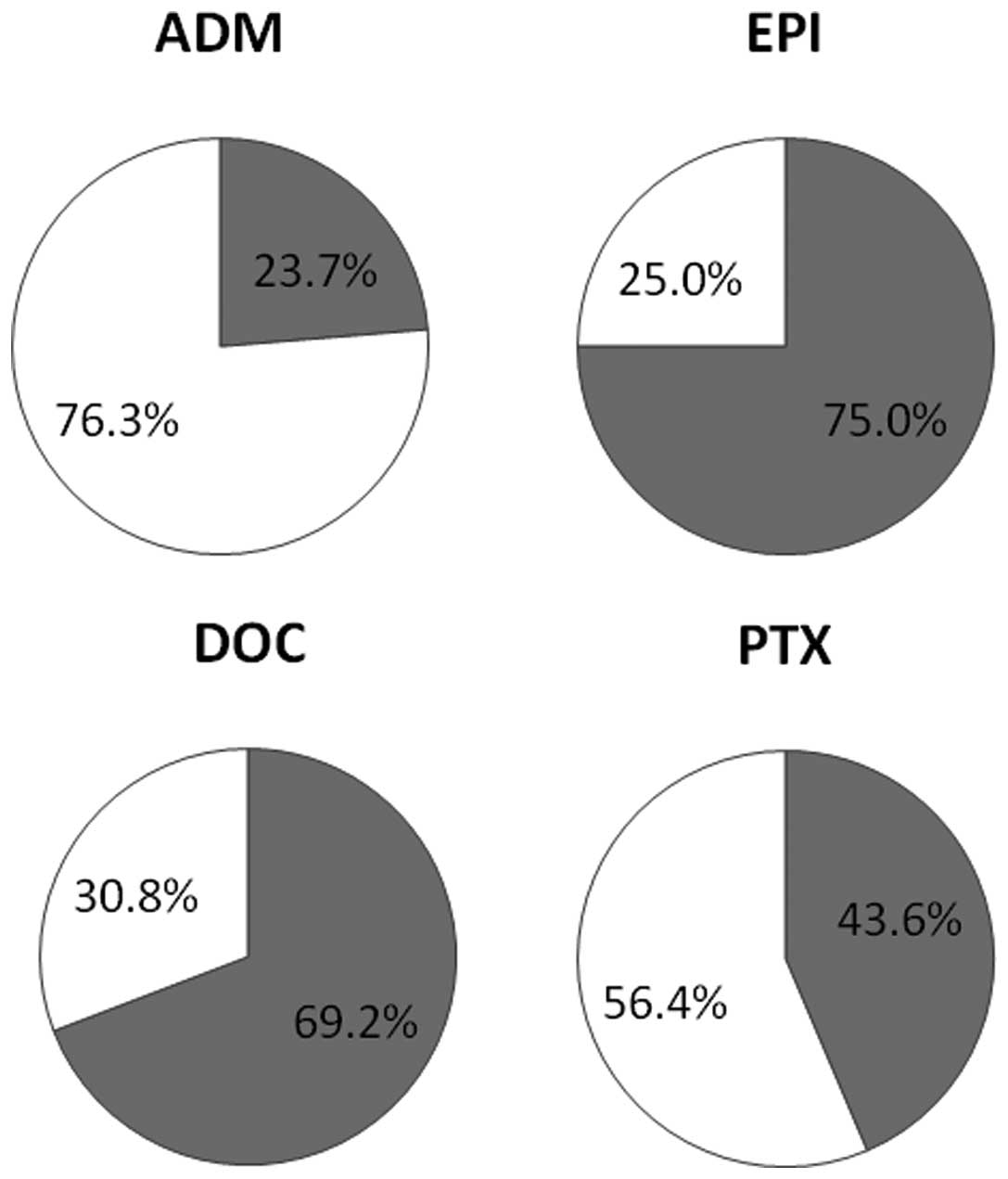
The chemosensitivities to each anti-cancer drug based on the CD-CST
were as follows: ADM, 23.7%; EPI, 75.0%; DOC, 69.2% and PTX, 43.6%
(Fig. 1).
Correlation between Ki67 expression and
clinicopathological variables
Comparisons between Ki67 expression and
clinicopathological variables are shown in Table III. A significant relationship
between Ki67 expression and a higher nuclear grade was
observed.
| Table IIICorrelation between KI67 and
clinicopathological variables. |
Table III
Correlation between KI67 and
clinicopathological variables.
| Ki67 labeling index
|
|---|
| Variables | High | Low | P-value |
|---|
| Menopausal
status | | | |
| Pre- | 10 | 30 | |
| Post- | 7 | 21 | |
| ER (%) | | | |
| <1 | 0 | 0 | |
| ≥1 | 17 | 51 | |
| PgR (%) | | | |
| <1 | 1 | 8 | 0.3016 |
| ≥1 | 16 | 43 | |
| Tumor size
(cm) | | | |
| ≤2.0 | 4 | 11 | 0.8659 |
| > 2.0 | 13 | 40 | |
| Lymph node
metastasis | | | |
| Positive | 10 | 31 | 0.8862 |
| Negative | 7 | 20 | |
| Nuclear grade | | | |
| 1/2 | 6 | 36 | 0.0095 |
| 3 | 11 | 15 | |
| LVI | | | |
| 0/1 | 12 | 35 | 0.8795 |
| 2/3 | 5 | 16 | |
Correlation between CD-DST and
clinicopathological variables
Table IV shows the
relationship between CD-DST and clinicopathological variables in
relation to the anticancer drugs. In the Chi-square test or
Fischer’s exact test in the case of 2×2 variables, no significant
differences were evident in the relationship between the CD-DST and
clinicopathological variables, with the exception of the
relationship between CD-DST and Ki67 expression with PTX.
| Table IVCorrelation between CD-DST and
clinicopathological variables (ADM, EPI, DOC and PTX). |
Table IV
Correlation between CD-DST and
clinicopathological variables (ADM, EPI, DOC and PTX).
A, ADM.
|
|---|
| CD-DST
|
|---|
| Variables | Sensitive | Resistant | P-value |
|---|
| Menopausal
status | | | |
| Pre- | 8 | 28 | 0.7336 |
| Post- | 6 | 17 | |
| PgR (%) | | | |
| <1 | 1 | 7 | 0.4220 |
| ≥1 | 13 | 38 | |
| Tumor size
(cm) | | | |
| ≤2.0 | 3 | 9 | 0.9077 |
| >2.0 | 11 | 36 | |
| Lymph node
metastasis | | | |
| Positive | 11 | 23 | 0.0694 |
| Negative | 3 | 22 | |
| Nuclear grade | | | |
| 1/2 | 9 | 26 | 0.6651 |
| 3 | 5 | 19 | |
| LVI | | | |
| 0/1 | 11 | 32 | 0.5835 |
| 2/3 | 3 | 13 | |
| Ki67 LI | | | |
| High | 5 | 10 | 0.3113 |
| Low | 9 | 35 | |
B, EPI.
|
|---|
| CD-DST |
|---|
| Variables | Sensitive | Resistant | P-value |
|---|
| Menopausal
status | | | |
| Pre- | 28 | 7 | 0.2646 |
| Post- | 14 | 7 | |
| PgR (%) | | | |
| <1 | 4 | 3 | 0.2434 |
| ≥1 | 38 | 11 | |
| Tumor size
(cm) | | | |
| ≤2.0 | 10 | 2 | 0.4520 |
| >2.0 | 32 | 12 | |
| Lymph node
metastasis | | | |
| Positive | 23 | 8 | 0.8767 |
| Negative | 19 | 6 | |
| Nuclear grade | | | |
| 1/2 | 26 | 8 | 0.7520 |
| 3 | 16 | 6 | |
| LVI | | | |
| 0/1 | 31 | 10 | 0.8617 |
| 2/3 | 11 | 4 | |
| Ki67 LI | | | |
| High | 11 | 3 | 0.7216 |
| Low | 31 | 11 | |
C, DOC.
|
|---|
| CD-DST
|
|---|
| Variables | Sensitive | Resistant | P-value |
|---|
| Menopausal
status | | | |
| Pre- | 17 | 6 | 0.4475 |
| Post- | 10 | 6 | |
| PgR (%) | | | |
| <1 | 3 | 1 | 0.7919 |
| ≥1 | 24 | 11 | |
| Tumor size
(cm) | | | |
| ≤2.0 | 7 | 3 | 0.9513 |
| >2.0 | 20 | 9 | |
| Lymph node
metastasis | | | |
| Positive | 14 | 6 | 0.9150 |
| Negative | 13 | 6 | |
| Nuclear grade | | | |
| 1/2 | 14 | 8 | 0.3892 |
| 3 | 13 | 4 | |
| LVI | | | |
| 0/1 | 20 | 9 | 0.9513 |
| 2/3 | 7 | 3 | |
| Ki67 LI | | | |
| High | 10 | 2 | 0.2033 |
| Low | 17 | 10 | |
D, PTX.
|
|---|
| CD-DST
|
|---|
| Variables | Sensitive | Resistant | P-value |
|---|
| Menopausal
status | | | |
| Pre- | 10 | 12 | 0.7893 |
| Post- | 7 | 10 | |
| PgR (%) | | | |
| <1 | 2 | 2 | 0.7894 |
| ≥1 | 15 | 20 | |
| Tumor size
(cm) | | | |
| ≤2.0 | 5 | 5 | 0.6355 |
| >2.0 | 12 | 17 | |
| Lymph node
metastasis | | | |
| Positive | 12 | 9 | 0.0652 |
| Negative | 5 | 13 | |
| Nuclear grade | | | |
| 1/2 | 10 | 12 | 0.7893 |
| 3 | 7 | 10 | |
| LVI | | | |
| 0/1 | 13 | 16 | 0.7906 |
| 2/3 | 4 | 6 | |
| Ki67 LI | | | |
| High | 8 | 3 | 0.0214 |
| Low | 9 | 19 | |
Correlation between Ki67 and CD-DST
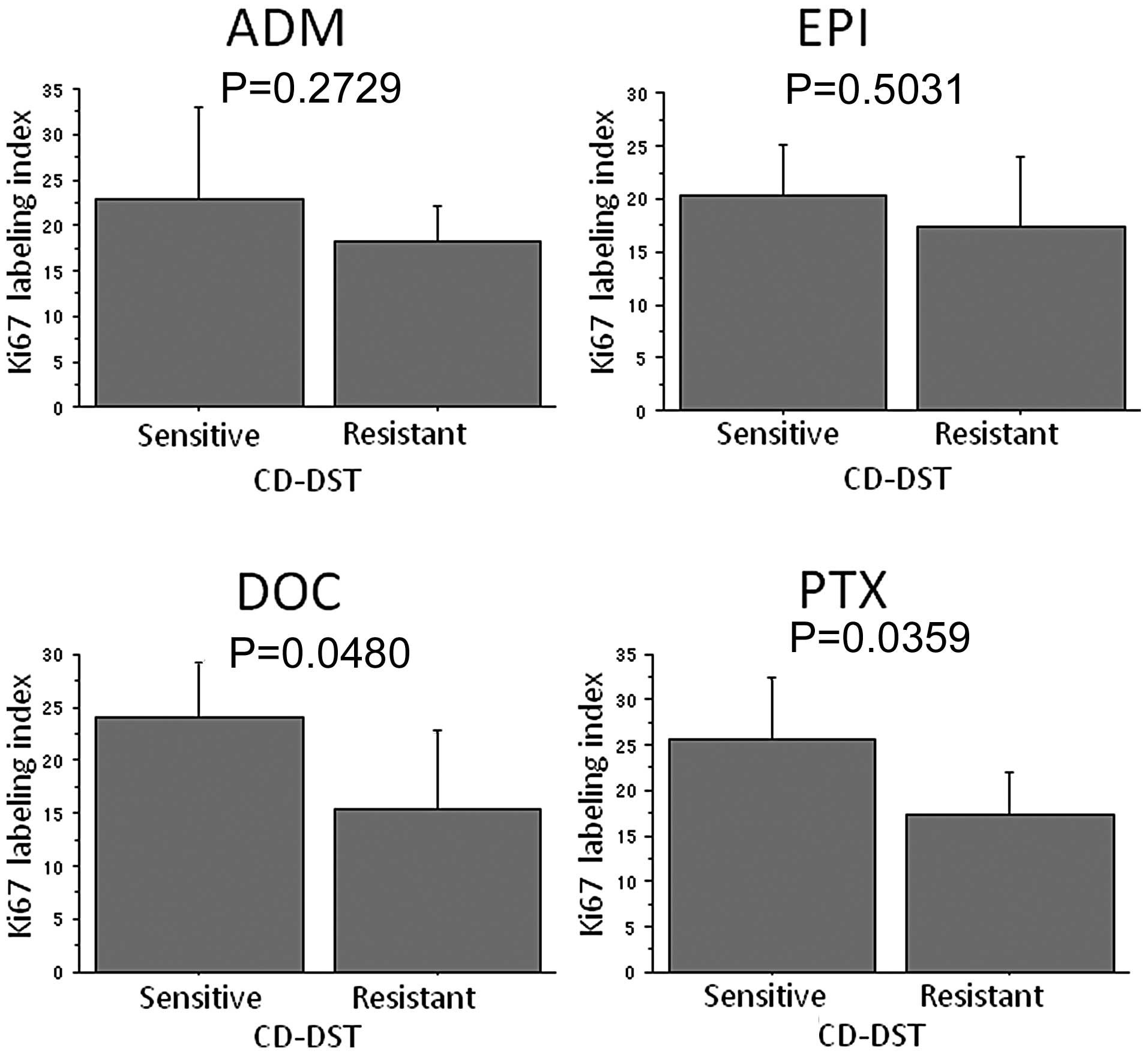
Ki67 LI was significantly higher in the group that
was sensitive to DOC compared to the group that was resistant to
DOC (P=0.0480) and PTX (P=0.0359) (Fig. 2). Regarding ADM and EPI, Ki67 LI
tended to be higher in the sensitive group than in the resistant
group, although there were no significant differences. Of the 11
Ki67-high tumors, 8 (72.7%) were diagnosed as PTX-sensitive by the
CD-DST, and 9 (32.1%) of the 28 Ki67-low tumors were diagnosed as
PTX-sensitive by the CD-DST (P=0.0214) (Table IVD). No significant differences
were observed with respect to the other anticancer drugs.
Discussion
The development of accurate predictors of
chemotherapeutic responses in order to establish personalized
treatment for breast cancer patients is crucial. For effective
chemotherapy, the chemosensitivity testing of anticancer drugs
should be performed with fresh surgical specimens or biopsy
specimens obtained from the breast cancer. Various in vitro
chemosensitivity tests have been studied and developed. These
include HTCA (35), TIA (36), SDI test (37), MTT assay (38), DiSC assay (39), three-dimensional agarose-based EDRA
(40) and HDRA (41). However, these tests are not widely
used in clinical practice for several reasons. The HTCA and TIA
tests require a large sample volume; the HTCA, SDI and MTT tests
have a low success rate in primary culture; and HDRA requires an
extremely high concentration of drugs in the culture medium. CD-DST
is a newly developed in vitro chemosensitivity test that has
several advantages over conventional tests. CD-DST exhibits a high
success rate in primary culture, requires a small number of cells,
eliminates contamination by fibroblasts using image analysis,
maintains the original growth characteristics and permits
evaluation using physiological concentrations of drugs.
Takamura et al(34) demonstrated that CD-DST may be a
predictive marker for chemotherapy. In their study, biopsy
specimens of patients with primary breast cancers or locally
recurrent breast cancers before chemotherapy were used for CD-DST
and examined for sensitivity to cyclophosphamide and epirubicin
(CE) therapy or DOC therapy. These authors investigated the
correlation between CD-DST and clinical chemotherapeutic responses
and reported that CD-DST was able to predict a response to CE and
DOC therapy with high accuracy in breast cancer patients.
We investigated chemosensitivity to ADM, EPI, DOC
and PTX using CD-DST. In this study, the chemosensitivity values
were found to be ADM, 23.7%; EPI, 75.0%; DOC, 69.2% and PTX, 43.6%.
Yamamoto et al(42)
reported that the chemo-sensitivity values were 30.8, 53.8 and
46.2% for ADM, DOC and PTX, respectively. Takamura et
al(34) reported that the
chemosensitivity values were 65.2 and 38.9% for CE and DOC,
respectively. Yamamoto et al(42) investigated the sensitivity to ADM
in 13 breast cancers using CD-DST. Of 13 tumors, 8 were
HER2-positive, and 4 of these 8 HER2-positive tumors were sensitive
to ADM. Thus, patients with HER2-positive breast cancer reportedly
derive benefits from ADM (43).
The sensitivity to EPI was the highest among these 4 anticancer
drugs. Anthracycline-based chemotherapy may be a standard regimen
even for patients with ER-positive and HER2-negative breast cancer.
The sensitivity to DOC and PTX in this study was 69.2 and 43.6%,
respectively. The sensitivity to PTX was similar to that reported
above (46.2%). However, the sensitivity to DOC was higher than
those values reported above (38.9 and 53.8%). We selected
ER-positive and HER2-negative breast cancers in this study. In
general, the efficacy of chemotherapy is lower in patients with
ER-positive tumors as compared with patients with ER-negative
tumors (5,6). Henderson et al(44) reported improved DFS as a result of
adding PTX to adriamycin and cyclophosphamide (AC) for patients
with ER-negative tumors, but not for those with ER-positive tumors
in the adjuvant setting. Bear et al(8) showed that the pCR rate of ER-negative
tumors is higher (22.8%) than that of ER-positive tumors (14.1%) in
the neoadjuvant setting by evaluating the effect of the addition of
DOC to AC in an NSABP B-27 trial. By contrast, Tham et
al(45) reported that the DOC
response rate of ER-positive tumors is higher (90%) than that of
ER-negative tumors (50%) in neoadjuvant chemotherapy. Results of an
investigation by Learn et al(46) of the effect of adding DOC to AC
suggested that ER-positive tumors are more likely to respond to DOC
than are ER-negative tumors in the neoadjuvant setting. Although
the predictive value of ER or HER2 status for the response to DOC
or PTX remains to be established, patients with ER-positive and
HER2-negative breast cancer may derive benefits from DOC rather
than PTX.
The precise role and indications for chemotherapy
for ER-positive breast cancer are controversial. Ki67 has been
investigated as a predictive marker for chemotherapy using clinical
and pathological responses as endpoints. Previous reports (31,34)
have demonstrated that CD-DST may predict a response to
chemotherapy with high accuracy in breast cancer. We investigated
the association between CD-DST and Ki67 expression in ER-positive
and HER2-negative breast cancer. Higher levels of Ki67 expression
tended to be sensitive to DOC and PTX. Although there is no
standard pathological assessment for Ki67, the panel of experts at
the St. Gallen Consensus in 2009 considered Ki67 LI to be crucial
in selecting additional chemotherapy beyond endocrine therapy for
patients with hormone receptor-positive breast tumors. The patients
were divided into low-, intermediate- and highly-proliferating
groups according to the value of Ki67 LI (≤15, 16–30% and >30%,
respectively). Tumors were dichotomized into Ki67-positive and
-negative tumors using the arbitrary cut-off value of 30% (Ki67 LI)
in this study. We found that highly proliferating tumors were
significantly more sensitive to PTX compared to the low ones.
In The Breast Cancer International Research Group
(BCIRG) 001 trial, investigators stratified the hormone
receptor-positive breast cancers into two subtypes: luminal A
(hormone receptor-positive, HER2-negative and Ki67 ≤11%) and
luminal B (hormone receptor-positive, HER2-positive and/or Ki67
>11%). Taxane-containing therapy showed a significant benefit
for patients in the luminal B group, with a 3-year DFS. Thus, high
levels of Ki67 expression may be a predictive marker for
taxane-containing therapy (13).
In the PACS01 study (14), using a
cut-off value of >20% for positive Ki67, the hazard ratio for
relapse associated with DOC was 0.51 (95% CI, 0.26–1.01) in
patients with ER-positive/Ki67-positive tumors and 1.03 (0.69–1.55)
in the ER-positive/Ki67-negative tumors. The investigators
concluded that Ki67 identified a subset of DOC-sensitive,
ER-positive breast cancers.
In this study, high-Ki67 tumors were found to be
sensitive to taxane therapy in patients with ER-positive breast
cancer. Results of recent studies (13,14)
have shown an association between Ki67 and sensitivity to DOC;
however, no report on PTX has been published. We showed that
high-Ki67 tumors were sensitive to both PTX and DOC. The
association between anticancer drug sensitivity and
clinicopathological variables has been evaluated, but no
significant association was obtained. Although anthracyclines,
particularly EPI, may be effective for patients with ER-positive
breast cancer, the risk of a cardiac event is likely to be severe.
If Ki67 level is high, taxanes may replace anthracyclines in
patients with low cardiac function.
The possible use of Ki67 as a prognostic marker for
breast cancer has been investigated (47–50).
In their study, Cheang et al(48) reported that luminal breast cancers
with a Ki67 level of ≥14% had a worse prognosis for both breast
cancer recurrence and death as compared to tumors with a Ki67 level
<14%. The 21-gene assay (Oncotype DX™) and the 70-gene profile
(Mammaprint®) are new prognostic tools that have the
potential to greatly improve risk assessment and treatment
decision-making for early breast cancer (51,52).
Oncotype DX™, including the Ki67 gene, was developed specifically
for patients with ER-positive breast cancer and has been shown to
predict distant recurrence more accurately than classical
clinicopathologic features in patients with ER-positive breast
cancer and negative axillary nodes treated with adjuvant tamoxifen.
The prospective validation of these assays is currently ongoing
through the TAILORx and MINDACT trials (53,54).
CD-DST is known to predict the response to chemotherapy with high
accuracy in breast cancer (31,34).
However, no report has been published regarding the association
between CD-DST and the prognosis of breast cancer. A prospective
study is therefore required to investigate the association between
CD-DST and the prognosis of breast cancer. In conclusion, the
CD-DST and Ki67 expression levels are capable of identifying a
subset of patients who are potentially sensitive to
chemotherapy.
References
|
1.
|
Early Breast Cancer Trialists’
Collaborative Group (EBCTCG): Effects of chemotherapy and hormonal
therapy for early breast cancer on recurrence and 15-year survival:
an overview of the randomized trials. Lancet. 365:1687–1717.
2005.
|
|
2.
|
Martin M, Pienkowski T, Mackey J, et al:
Breast Cancer International Research Group 001 Investigators:
Adjuvant docetaxel for node-positive breast cancer. N Engl J Med.
352:2302–2313. 2005.
|
|
3.
|
Martin M, Segui MA, Anton A, et al: Breast
Cancer International Research Group 001 Investigators: Adjuvant
docetaxel for node-positive breast cancer. N Engl J Med.
363:2200–2210. 2010.
|
|
4.
|
Sparano JA, Wang M, Martino S, et al:
Weekly paclitaxel in the adjuvant treatment of breast cancer. N
Engl J Med. 358:1663–1671. 2008.
|
|
5.
|
Conforti R, Boulet T, Tomasic G, et al:
Breast cancer molecular subclassification and estrogen receptor
expression to predict efficacy of adjuvant anthracyclines-based
chemotherapy: a biomarker study from two randomized trials. Ann
Oncol. 18:1477–1483. 2007.
|
|
6.
|
Berry DA, Cirrincione C, Henderson IC, et
al: Estrogen-receptor status and outcomes of modern chemotherapy
for patients with node-positive breast cancer. JAMA. 295:1658–1667.
2006.
|
|
7.
|
Regan MM, Viale G, Mastropasqua MG, et al:
Re-evaluating adjuvant breast cancer trials: assessing hormone
receptor status by immunohistochemical versus extraction assays. J
Natl Cancer Inst. 98:1571–1581. 2006.
|
|
8.
|
Bear HD, Anderson S, Brown A, et al: The
effect on tumor response adding sequential preoperative docetaxel
to preoperative doxorubicin and cyclophosphamide: preliminary
results from national surgical adjuvant breast and bowel project
protocol B-27. J Clin Oncol. 21:4165–4174. 2003.
|
|
9.
|
Stearns V, Singh B, Tsangaris T, et al: A
prospective randomized pilot study to evaluate predictors of
response in serial core biopsies to single agent neoadjuvant
doxorubicin or paclitaxel for patients with locally advanced breast
cancer. Clin Cancer Res. 9:124–133. 2003.
|
|
10.
|
Kuerer HM, Newman LA, Smith TL, et al:
Clinical course of breast cancer patients with complete pathologic
primary tumor and axillary lymph node response to doxorubicin-based
neoadjuvant chemotherapy. J Clin Oncol. 17:460–469. 1999.
|
|
11.
|
Paik S, Tang G, Shak S, et al: Gene
expression and benefit of chemotherapy in women with node negative,
estrogen receptor-positive breast cancer. J Clin Oncol.
24:3726–3734. 2006.
|
|
12.
|
Hayes DF, Thor AD, Dressler LG, et al;
Cancer and Leukemia Group B (CALGB) Investigators: HER2 and
response to paclitaxel in node-positive breast cancer. N Engl J
Med. 357:1496–1506. 2007.
|
|
13.
|
Hugh J, Hanson J, Cheang MCU, et al:
Breast cancer subtypes and response to docetaxel in node-positive
breast cancer: use of an immunohistochemical definition in the
BCIRG 001 trial. J Clin Oncol. 27:1168–1176. 2009.
|
|
14.
|
Penault-Llorca F, Andre F, Sagan C, et al:
Ki67 expression and docetaxel efficacy in patients with estrogen
receptor-positive breast cancer. J Clin Oncol. 27:2809–2815.
2009.
|
|
15.
|
Litman T, Druley TE, Stein WD, et al: From
MDR to MXR: new understanding of multidrug resistance systems,
their properties and clinical significance. Cell Mol Life Sci.
58:931–959. 2001.
|
|
16.
|
Yamamoto N, Tamura T, Murakami H, et al:
Randomized pharmacokinetic and pharmacodynamic study of docetaxel:
dosing based on body-surface area compared with individualized
dosing based on cytochrome P450 activity estimated using a urinary
metabolite of exogenous cortisol. J Clin Oncol. 23:1061–1069.
2005.
|
|
17.
|
Miyoshi Y, Taguchi T, Kim SJ, et al:
Prediction of response to docetaxel by immunohistochemical analysis
of CYP3A4 expression in human breast cancers. Breast Cancer.
12:11–15. 2005.
|
|
18.
|
Hasegawa S, Miyoshi Y, Egawa C, et al:
Mutational analysis of the class I beta-tubulin gene in human
breast cancer. Int J Cancer. 101:46–51. 2002.
|
|
19.
|
Burkhart CA, Kavallaris M and Band Horwitz
S: The role of beta-tubulin isotype in resistance to antimitotic
drugs. Biochim Biophys Acta. 1471:1–9. 2001.
|
|
20.
|
Coon JS, Marcus E, Gupta-Burt S, et al:
Amplification and overexpression of topoisomerase IIα predict
response to anthracycline-based therapy in locally advanced breast
cancer. Clin Cancer Res. 8:1061–1067. 2002.
|
|
21.
|
Anand S, Penrhyn-Lowe S and Venkitaraman
AR: AURORA-A amplification overrides the mitotic spindle assembly
checkpoint, inducing resistance to taxol. Cancer Cell. 3:51–62.
2003.
|
|
22.
|
Sjostrom J, Blomqvist C, Heikkila P, et
al: Predictive value of p53, mdm-2, p21, and mib-1 for chemotherapy
response in advanced breast cancer. Clin Cancer Res. 6:3103–3110.
2000.
|
|
23.
|
Sjostrom J, Blomqvist C, von Boguslawski
K, et al: The predictive value of bcl-2, bax, bcl-xL, bag-1, fas,
and fasL for chemotherapy response in advanced breast cancer. Clin
Cancer Res. 8:811–816. 2002.
|
|
24.
|
Yokomizo A, Ono M, Nanri H, et al:
Cellular levels of thioredoxin associated with drug sensitivity to
cisplatin, mitomycin C, doxorubicin, and etoposide. Cancer Res.
55:4293–4296. 1995.
|
|
25.
|
Sahin AA, Ro J, Ro JY, et al: Ki67
immunostaining in node negative stage I/II breast carcinoma.
Significant correlation with prognosis. Cancer. 68:549–557.
1991.
|
|
26.
|
Domagala W, Markiewski M, Harezga B, et
al: Prognostic significance of tumor cell proliferation rate as
determined by the MIB-1 antibody in breast carcinoma: its
relationship with vimentin and p53 protein. Clin Cancer Res.
2:147–154. 1996.
|
|
27.
|
Trihia H, Murray S, Price K, et al: Ki67
expression in breast carcinoma. Its association with grading
systems, clinical parameters, and other prognostic factors - a
surrogate marker? Cancer. 97:1321–1331. 2003.
|
|
28.
|
Chang J, Ormerod M, Powles TJ, et al:
Apoptosis and proliferation as predictors of chemotherapy response
in patients with breast carcinoma. Cancer. 89:2145–2152. 2000.
|
|
29.
|
Archer CD, Parton M, Smith IE, et al:
Early changes in apoptosis and proliferation following primary
chemotherapy for breast cancer. Br J Cancer. 89:1035–1041.
2003.
|
|
30.
|
Goldhhirsch A, Ingle JN, Gelber RD, et al:
Thresholds for therapies: highlights of the St Gallen international
expert consensus on primary therapy early breast cancer. Ann Oncol.
20:1319–1329. 2009.
|
|
31.
|
Kobayashi H: Development of a new in vitro
chemosensitivity test using collagen gel droplet embedded culture
and image analysis for clinical usefulness. Recent Results Cancer
Res. 161:48–61. 2003.
|
|
32.
|
Yasuda H, Takada T, Wada K, et al: A new
in-vitro drug sensitivity test (collagen-gel droplet
embedded-culture drug sensitivity test) in carcinomas of pancreas
and biliary tract: possible clinical utility. J Hepatobiliary
Pancreat Surg. 5:261–268. 1998.
|
|
33.
|
Higashiyama M, Kodama K, Yokouchi H, et
al: Immunohistochemical p53 protein status in nonsmall cell lung
cancer is a promising indicator in determining in vitro
chemosensitivity to some anticancer drugs. J Surg Oncol. 68:19–24.
1998.
|
|
34.
|
Takamura Y, Kobayashi H, Taguchi T, et al:
Prediction of chemotherapeutic response by collagen gel droplet
embedded culture-drug sensitivity test in human breast cancers. Int
J Cancer. 98:450–455. 2002.
|
|
35.
|
Von Hoff DD: He’s not going to talk about
in vitro predictive assay again, is he? J Natl Cancer Inst.
82:96–101. 1990.
|
|
36.
|
Kern DH, Drogemuller CR, Kennedy MC, et
al: Development of miniaturized, improved nucleic acid precursor
incorporation assay for chemosensitivity testing of human solid
tumors. Cancer Res. 45:5436–5441. 1985.
|
|
37.
|
Fruehauf JP and Bosanquet AG: In vitro
determination of drug response: a discussion of clinical
applications. Principles Prac Oncol Updates. 7:121993.
|
|
38.
|
Carmichael J, De Graff WG, Gazdar AF, et
al: Evaluation of a tetrazolium-based semiautomated colorimetric
assay: assessment of chemosensitivity testing. Cancer Res.
47:936–942. 1987.
|
|
39.
|
Wilbur DW, Camacho ES, Hilliard DA, et al:
Chemotherapy of non-small cell lung carcinoma guided by an in vitro
drug resistance assay measuring total tumour cell kill. Br J
Cancer. 65:27–32. 1992.
|
|
40.
|
Mechetner E, Kyshtoobayeva A, Zonis S, et
al: Levels of multidrug resistance (MDR1) P-glycoprotein expression
by human breast cancer correlate with in vitro resistance to taxol
and doxorubicin. Clin Cancer Res. 4:389–398. 1998.
|
|
41.
|
Furukawa T, Kubota T and Hoffman RM:
Clinical application of the histoculture drug response assay. Clin
Cancer Res. 1:305–311. 1995.
|
|
42.
|
Yamamoto Y, Watanabe Y, Ishida N, et al:
Collagen gel droplet-embedded culture drug sensitivity test in
human breast cancer. Gan To Kagaku Ryoho. 35:793–796. 2008.(In
Japanese).
|
|
43.
|
Paik S, Bryant J, Park C, et al: erbB-2
and response to doxorubicin in patients with axillary lymph
node-positive, hormone receptor-negative breast cancer. J Natl
Cancer Inst. 90:1361–1370. 1998.
|
|
44.
|
Henderson IC, Berry DA, Demetri GD, et al:
Improved outcomes from adding sequential paclitaxel but not from
escalating doxorubicin dose in an adjuvant chemotherapy regimen for
patients with node-positive primary breast cancer. J Clin Oncol.
21:976–983. 2003.
|
|
45.
|
Tham YL, Gomez LF, Mohsin S, et al:
Clinical response to neoadjuvant docetaxel predicts improved
outcome in patients with large locally advanced breast cancers.
Breast Cancer Res Treat. 94:279–284. 2005.
|
|
46.
|
Learn PA, Yeh IT, McNutt M, et al:
HER-2/neu expression as a predictor of response to neoadjuvant
docetaxel in patients with operable breast carcinoma. Cancer.
103:2252–2260. 2005.
|
|
47.
|
de Azambuja E, Cardoso F, de Castro G Jr,
et al: Ki67 as prognostic marker in early breast cancer: a
meta-analysis of published studies involving 12,155 patients. Br J
Cancer. 96:1504–1513. 2007.
|
|
48.
|
Cheang MC, Chia SK, Voduc D, et al: Ki67
index, HER2 status, and prognosis of patients with luminal B breast
cancer. J Natl Cancer Inst. 101:736–750. 2009.
|
|
49.
|
Stuart-Harris R, Caldas C, Pinder SE and
Pharoah P: Proliferation markers and survival in early breast
cancer: a systematic review and meta-analysis of 85 studies in
32,825 patients. Breast. 17:323–334. 2008.
|
|
50.
|
Urruticoechea A, Smith IE and Dowsett M:
Proliferation marker Ki-67 in early breast cancer. J Clin Oncol.
23:7212–7220. 2005.
|
|
51.
|
Paik S, Shak S, Tang G, et al: A multigene
assay to predict recurrence of tamoxifen-treated, node-negative
breast cancer. N Engl J Med. 351:2817–2826. 2004.
|
|
52.
|
van de Vijver MJ, He YD, van’t Veer LJ, et
al: A gene-expression signature as a predictor of survival in
breast cancer. N Engl J Med. 347:1999–2009. 2002.
|
|
53.
|
Sparano JA and Paik S: Development of the
21-gene assay and its application in clinical practice and clinical
trials. J Clin Oncol. 26:721–728. 2008.
|
|
54.
|
Cardoso F, van’t Veer L, Rutgers E, et al:
Clinical application of the 70-gene profile: the MINDACT trial. J
Clin Oncol. 26:729–735. 2008.
|