Introduction
Statins are cholesterol-lowering agents that act by
inhibiting the enzyme 3-hydroxy-3-methylglutaryl coenzyme A
(HMG-CoA) reductase. In addition, statins are also widely used in
the primary as well as secondary prevention of cardiovascular
diseases, especially hypercholesterolemia (1,2).
They reduce long-term cerebrovascular events, particularly after an
initial coronary event (3). Beyond
their lipid-lowering effects, statins have also been shown to
exhibit anti-inflammatory (4) and
antineoplastic (5) activities.
Although the precise mechanisms by which these activities occur are
unknown, they seem to correlate with the inhibitory effects of
statins on the mevalonate pathway. By inhibiting HMG-CoA reductase
and controlling mevalonate synthesis, statins affect cholesterol
biosynthesis and control the production of several additional major
products, including dolichol, geranyl pyro- and farnesyl
pyrophosphate (4–6). This process may be relevant for the
induction of antitumor responses, as these agents have effects on
various additional cell functions, including DNA synthesis, cell
cycle progression and apoptosis (5). Consistent with these observations,
statins have been shown to exert regulatory effects on cell cycle
progression and to induce apoptosis of malignant cells (5,7).
Statins have also been recognized for their activity
against various types of cancer. The use of statins as anticancer
agents is based on pre-clinical evidence of their
anti-proliferative, pro-apoptotic, anti-invasive and
radiosensitizing properties (8).
Statins exhibit in vitro anti-neoplastic activities against
a variety of malignant cells of diverse origin (7,9).
Progress has been noted with regard to the effects of statins
against various types of malignancy. However, information is scarce
on the effects of these agents against renal cell carcinoma (RCC)
(7). The aim of this study was to
investigate the effect of statins on the recurrence and progression
of RCC.
Patients and methods
Patients
A retrospective analysis was conducted on patients
diagnosed with RCC who presented at our hospital between January 1,
2006 and June 30, 2012. Of the 306 RCC patients, a total of 115
patients who had radical or partial nephrectomy (open or
laparoscopic) for non-distant metastatic (any TN0-1M0) RCC were
included in the present study. No patient had a known history of
von Hippel-Lindau disease, contralateral nephrectomy for RCC or
synchronous bilateral RCC. Informed consent was obtained from all
patients.
Patients were divided into the statin and non-statin
groups. Patients taking a statin following the diagnosis of RCC
were excluded from the statin group. The dose and type of statin
used and compliance were not factored in the analysis.
Statistical analysis
Statistical analysis was performed with SPSS ver.
16.0 (SPSS, Chicago, IL, USA). The correlation between gender,
pathologic characteristics including Fuhrman grade, cell type and
tumor, node, metastasis (TNM) stage of the two groups were analyzed
using the Chi-square test. The correlation between age and body
mass index (BMI) of the two groups was analyzed using the Student’s
t-test. Multivariate analysis was performed using Cox’s regression
model to determine the effect of confounding variables. The
Kaplan-Meier survival test was used to determine the association
between recurrence and progression of the two groups. P<0.05 was
considered to indicate a statistically significant difference.
Results
Of the total of 115 patients [male, 72 (63%) and
female, 43 (37%)], the statin group comprised 21 (18%) patients
taking statins, while the non-statin group comprised 94
(82%)patients not taking statins. Patient clinical characteristics
are shown in Table I. The clear
cell type was the most common RCC type, comprising 96 (83%)
patients. Other types included the chromophobe, papillary,
collecting duct and sarcomatoid comprising 11 (10%), 4 (3%), 2 (2%)
and 2 (2%) patients, respectively. T1a was the most common T stage,
followed by T1b, comprising 61 (53%) and 29 (25%) patients,
respectively. N0 was identified in 112 (97%) and N1 in 3 (3%)
patients. During the follow-up, 8 (7%) and 4 (3%) patients
exhibited recurrence and progressive disease, respectively.
 | Table IClinical characteristics and
correlation between the two groups. |
Table I
Clinical characteristics and
correlation between the two groups.
| Characteristics | Statin group | Non-statin group | Total | P-value |
|---|
| Gender | | | | 0.039 |
| Male | 63 | 9 | 72 | |
| Female | 31 | 12 | 43 | |
| Age (years) | 58.95±12.33 | 65.24±6.82 | | 0.002 |
| BMI | 24.24±3.35 | 26.17±2.96 | | 0.017 |
| Cancer type | | | | 0.71 |
| Clear cell | 78 | 18 | 96 | |
| Papillary | 4 | 0 | 4 | |
| Chromophobe | 9 | 2 | 11 | |
| Collecting
duct | 2 | 0 | 2 | |
| Sarcomatoid | 1 | 1 | 2 | |
| T stage | | | | 0.935 |
| T1a | 47 | 14 | 61 | |
| T1b | 25 | 4 | 29 | |
| T2a | 5 | 1 | 6 | |
| T2b | 5 | 1 | 6 | |
| T3a | 9 | 1 | 10 | |
| T3b | 2 | 0 | 2 | |
| T4 | 1 | 0 | 1 | |
| N stage | | | | 0.628 |
| N0 | 91 | 21 | 112 | |
| N1 | 3 | 0 | 3 | |
Male gender was identified significantly more
frequently in the statin group, compared with the non-statin group
(P=0.039). The RCC type and TNM stage did not vary in the two
groups. Mean age was higher in the statin compared with the
non-statin group [65.24 (±6.82) and 58.95 (±12.33), respectively]
(P=0.002). Mean BMI was higher in the statin compared with the
non-statin group [24.24 (±3.35) and 26.17 (±2.96), respectively]
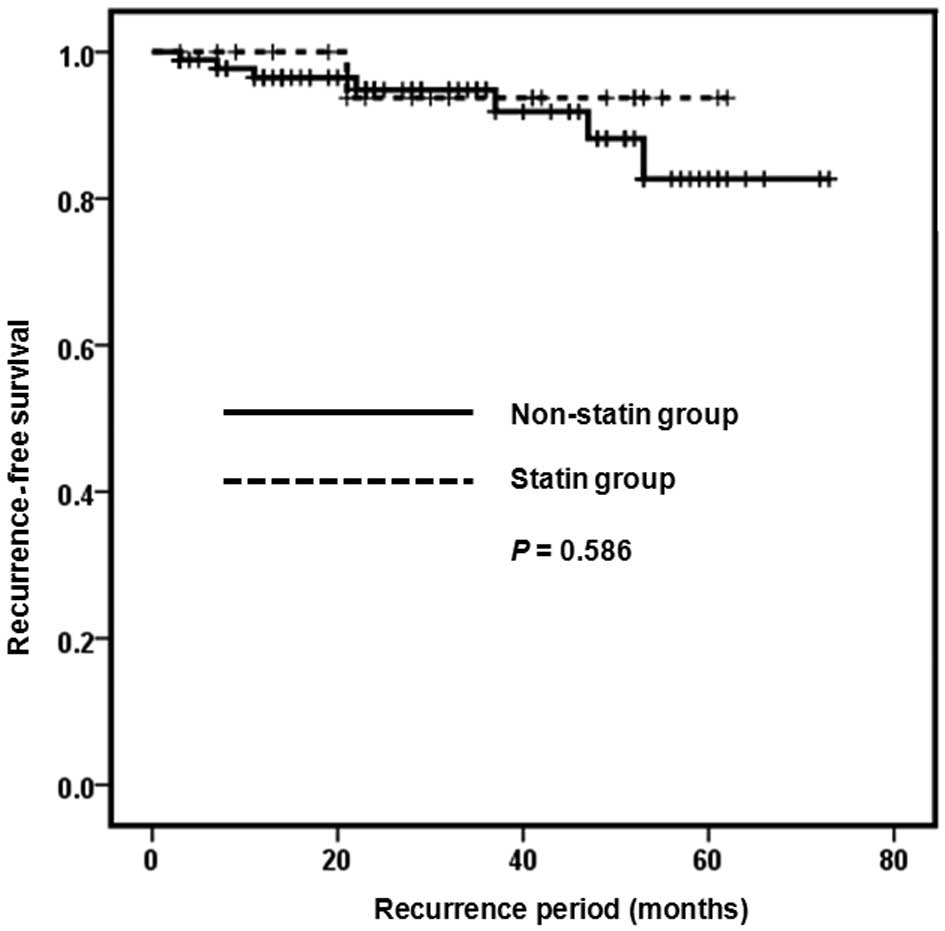
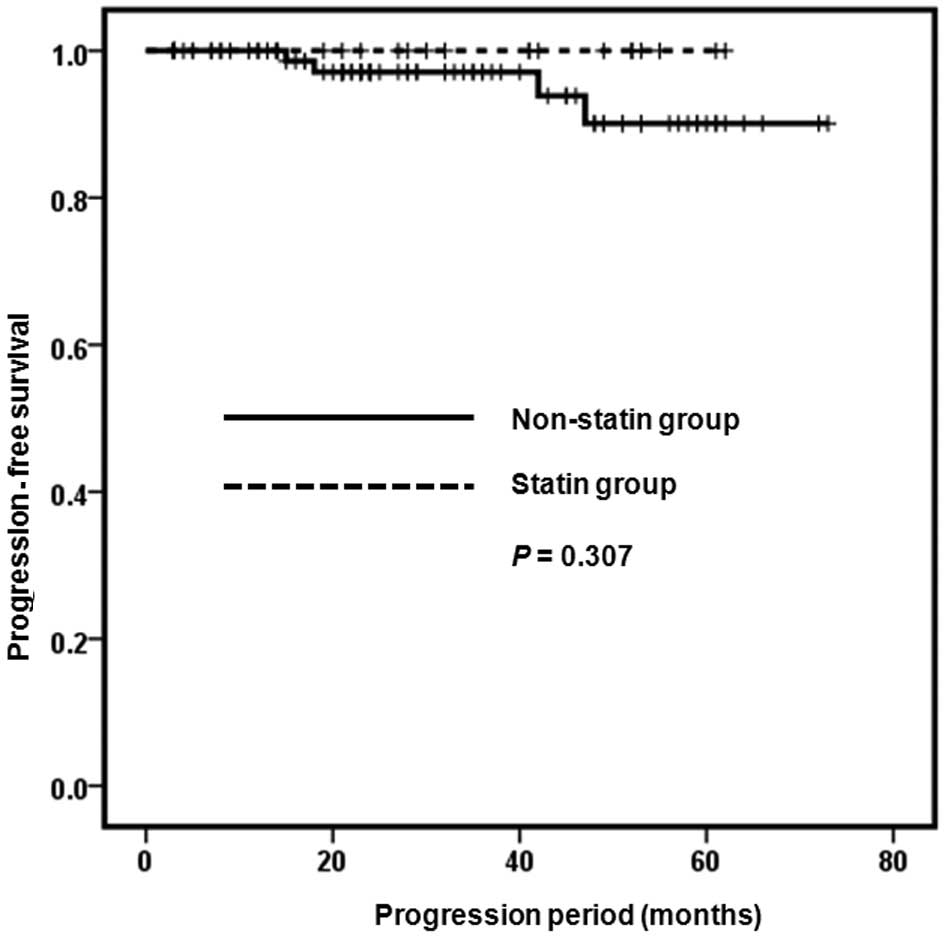
(P=0.026) (Table I). When assessed
using the Kaplan-Meier survival analysis, the recurrence and
progression-free survival rate of the two groups showed no
statistically significant difference (P=0.586 and P=0.307)
(Figs. 1 and 2). The effects of gender, age, BMI and
statins on recurrence and progression were examined, using Cox’s
regression model. However, the effects were not statistically
significant (Table II).
| Table IIResults of the effects of gender, age,
BMI and statins on recurrence and progression.a |
Table II
Results of the effects of gender, age,
BMI and statins on recurrence and progression.a
| Characteristics | Exp (B) | P-value |
|---|
| Gender | 1.322 | 0.770 |
| Age | 0.968 | 0.260 |
| BMI | 1.065 | 0.572 |
| Statins | 0.787 | 0.846 |
Discussion
Statins have a lowering effect of low-density
lipoprotein (LDL) cholesterol by inhibiting HMG-CoA reductase.
Mevalonate is a limiting factor in hepatic cholesterol biosynthesis
as it is an essential precursor (6). Thus, statins were prescribed for
hypercholesterolemic patients. Statins were also administered to
patients with cardiovascular diseases, including myocardial
infarction and atrial fibrillation (2,10–12).
The underlying mechanisms of the lowering effect of
statins on the incidence of cerebrovascular disease have yet to be
elucidated. However, several studies suggest that the metabolites
of statins have certain regulatory effects on the endothelial,
platelet and leukocyte function. Their function is regulated by
G-proteins, such as Rho, Rac and Ras, and intermediates of HMG-CoA
reductase are essential for their post-translational modification
(13,14). Additionally, statins modulate
vascular remodeling by inhibiting extracellular matrix
metalloproteinases and transcription factors, such as nuclear
factor-κB (14). Statins have been
shown to attenuate vasoconstriction by increasing endothelial
nitric oxide activity (15). Thus,
they have pleiotropic cardiovascular and anti-atherosclerotic
effects, including improvement of endothelial function, reduction
of free radical formation, stabilization of plaques and inhibition
of endothelial inflammatory reactions, which contribute to other
potential benefits for patients at risk of cardiovascular disease,
regardless of cholesterol levels (8,16).
The mechanisms of these antitumor effects have yet
to be fully elucidated. Findings of previous studies suggest that
statins have antitumor effects by inhibiting tumor cell growth,
angiogenesis and induction of apoptosis. Statins block tumor cell
growth in vitro and in vivo, thus inhibiting
dolichol, geranyl pyro- and farnesyl pyrophosphate production, Ras-
and Rho-mediated cell proliferation and the stabilization of the
cell cycle kinase inhibitors p21 and p27 (17). Although statins have been reported
to stimulate and inhibit angiogenesis, they inhibit capillary tube
formation and decrease vascular endothelial growth factor release
(18). Statins exert pro-apoptotic
properties in a variety of tumor cells, by which they upregulate
pro-apoptotic proteins, decrease anti-apoptotic proteins and
activate certain types of caspases (19,20).
Statins impair the metastatic potential of tumor cells by
inhibiting cell migration, attachment to the extracellular matrix
and invasion of basement membrane (21).
However, clinical data regarding the antitumor
effects of statins are conflicting. In certain studies, statins
apparently have pro-carcinogenic effects. Coogan et al
(22) conducted a case control
study on 1,132 women with breast cancer and 1,009 men with prostate
cancer. Controls included 1,331 women and 1,387 men who presented
with conditions unrelated to statin use. The odds ratio (OR) for
breast cancer among statin users was 1.5 (95% CI, 1.0–2.3), largely
accounted for by an OR of 1.8 (95% CI, 0.9–3.6) among cases with
carcinoma in situ. Among the invasive cases, the OR was 1.2
(95% CI, 0.7–2.0). The OR for prostate cancer overall was 1.2 (95%
CI, 0.8–1.7) and 1.4 (95% CI, 0.7–2.5). A retrospective analysis of
2,463 women showed an increased risk of breast cancer among statin
users of 5.2% (11).
Several other studies maintain that statins have an
anti-tumor effect. Poynter et al (23) conducted a population-based
case-control study on 1,953 patients with colorectal cancer and
2,015 controls. Their results showed that the use of statins for at
least five years (vs. the non-use of statins) was associated with a
significantly reduced relative risk of colorectal cancer (OR=0.50;
95% CI, 0.40–0.63). Khurana et al (8) performed a retrospective nested
case-control study of 500,000 veteran patients and observed that
statin use is associated with a 44% risk reduction of RCC. Liu
et al (1) performed a
retrospective analysis of data of two US cohorts, and confirmed the
beneficial effect of statin use on the risk of RCC. Authors of that
study suggested that the use of statins was associated with a
reduced risk of RCC in women. The association was statistically
significant in women with no history of hypertension. In men, a
reduced risk was identified only among individuals with no history
of hypertension.
Findings of the present study have shown that
statins have no significant effects on recurrence and progression
in patients that have undergone radical nephrectomy following
diagnosis with RCC. A randomized double-blind trial of mortality
and incidence of cancer during a 10-year follow-up of the
Scandinavian Simvastatin Survival Study has shown no difference in
mortality from and incidence of cancer between the simvastatin and
placebo groups (24). Several
studies have found a similar relative risk for cancer development
(25,26), the results of which are partly
consistent with our findings.
At present, available studies (1,8,23)
have focused on the antitumor effect of statins and the risk of
cancers, which varies from our study. In this study, we focused on
the effects of statins on recurrence and progression of already
diagnosed RCC. To the best of our knowledge, studies on the effects
of statins on recurrence and progression-free survival of diagnosed
RCC are rare.
Our study has certain limitations. It is a
retrospective study that may have some biases. Due to the small
population size, our results are difficult to generalize to other
RCC patients. Comorbidities of the patients were not analyzed in
this study, nor were the dose, type of statin used or the
compliance.
In conclusion, statins do not have a marked effect
on recurrence and progression-free survival of non-distant
metastatic RCC patients. Additional, well-designed studies on large
populations and with a long-term follow up are necessary to assess
the effects on statins of these patients.
References
|
1
|
Liu W, Choueiri TK and Cho E: Statin use
and the risk of renal cell carcinoma in 2 prospective US cohorts.
Cancer. 118797–803. 2012.PubMed/NCBI
|
|
2
|
Heart Protection Study Collaborative
Group: MRC/BHF Heart Protection Study of cholesterol lowering with
simvastatin in 20,536 high-risk individuals: a randomised
placebo-controlled trial. Lancet. 360:7–22. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Hebert PR, Gaziano JM, Chan KS and
Hennekens CH: Cholesterol lowering with statin drugs, risk of
stroke, and total mortality. An overview of randomized trials.
JAMA. 278:313–321. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Forrester JS and Libby P: The inflammation
hypothesis and its potential relevance to statin therapy. Am J
Cardiol. 99:732–738. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Demierre MF, Higgins PD, Gruber SB, Hawk E
and Lippman SM: Statins and cancer prevention. Nat Rev Cancer.
5:930–942. 2005. View
Article : Google Scholar : PubMed/NCBI
|
|
6
|
Goldstein JL and Brown MS: Regulation of
the mevalonate pathway. Nature. 343:425–430. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Woodard J, Sassano A, Hay N and Platanias
LC: Statin-dependent suppression of the Akt/mammalian target of
rapamycin signaling cascade and programmed cell death 4
up-regulation in renal cell carcinoma. Clin Cancer Res.
14:4640–4649. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Khurana V, Caldito G and Ankem M: Statins
might reduce risk of renal cell carcinoma in humans: case-control
study of 500,000 veterans. Urology. 71:118–122. 2008. View Article : Google Scholar
|
|
9
|
Sivaprasad U, Abbas T and Dutta A:
Differential efficacy of 3-hydroxy-3-methylglutaryl CoA reductase
inhibitors on the cell cycle of prostate cancer cells. Mol Cancer
Ther. 5:2310–2316. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Shepherd J, Cobbe SM, Ford I, et al:
Prevention of coronary heart disease with pravastatin in men with
hypercholesterolemia. West of Scotland Coronary Prevention Study
Group. N Engl J Med. 333:1301–1307. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Sacks FM, Pfeffer MA, Moye LA, et al: The
effect of pravastatin on coronary events after myocardial
infarction in patients with average cholesterol levels. Cholesterol
and Recurrent Events Trial investigators. N Engl J Med.
335:1001–1009. 1996. View Article : Google Scholar
|
|
12
|
Young-Xu Y, Jabbour S, Goldberg R, et al:
Usefulness of statin drugs in protecting against atrial
fibrillation in patients with coronary artery disease. Am J
Cardiol. 92:1379–1383. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Cipollone F, Fazia M, Iezzi A, et al:
Suppression of the functionally coupled
cyclooxygenase-2/prostaglandin E synthase as a basis of
simvastatin-dependent plaque stabilization in humans. Circulation.
107:1479–1485. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Krupski WC, Layug EL, Reilly LM, et al:
Comparison of cardiac morbidity between aortic and infrainguinal
operations. Study of Perioperative Ischemia (SPI) Research Group. J
Vasc Surg. 15:354–365. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Bax L, Mali WP, Buskens E, et al: The
benefit of STent placement and blood pressure and lipid-lowering
for the prevention of progression of renal dysfunction caused by
Atherosclerotic ostial stenosis of the Renal artery. The
STAR-study: rationale and study design. J Nephrol. 16:807–812.
2003.
|
|
16
|
Farmer JA: Pleiotropic effects of statins.
Curr Atheroscler Rep. 2:208–217. 2000. View Article : Google Scholar
|
|
17
|
Rao S, Lowe M, Herliczek TW, et al:
Lovastatin mediated G1 arrest in normal and tumor breast cells is
through inhibition of CDK2 activity and redistribution of p21 and
p27, independent of p53. Oncogene. 17:2393–2402. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Vincent L, Chen W, Hong L, et al:
Inhibition of endothelial cell migration by cerivastatin, an
HMG-CoA reductase inhibitor: contribution to its anti-angiogenic
effect. FEBS Lett. 495:159–166. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Cafforio P, Dammacco F, Gernone A, et al:
Statins activate the mitochondrial pathway of apoptosis in human
lymphoblasts and myeloma cells. Carcinogenesis. 26:883–891. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Marcelli M, Cunningham GR, Haidacher SJ,
et al: Caspase-7 is activated during lovastatin-induced apoptosis
of the prostate cancer cell line LNCaP. Cancer Res. 58:76–83.
1998.PubMed/NCBI
|
|
21
|
Hindler K, Cleeland CS, Rivera E and
Collard CD: The role of statins in cancer therapy. Oncologist.
11:306–315. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Coogan PF, Rosenberg L, Palmer JR, et al:
Statin use and the risk of breast and prostate cancer.
Epidemiology. 13:262–267. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Poynter JN, Gruber SB, Higgins PD, et al:
Statins and the risk of colorectal cancer. N Engl J Med.
352:2184–2192. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Strandberg TE, Pyorala K, Cook TJ, et al:
Mortality and incidence of cancer during 10-year follow-up of the
Scandinavian Simvastatin Survival Study (4S). Lancet. 364:771–777.
2004.PubMed/NCBI
|
|
25
|
ALLHAT Officers and Coordinators for the
ALLHAT Collaborative Research Group: Major outcomes in moderately
hypercholesterolemic, hypertensive patients randomized to
pravastatin vs. usual care: the Antihypertensive and Lipid-Lowering
Treatment to Prevent Heart Attack Trial (ALLHAT-LLT). JAMA.
288:2998–3007. 2002. View Article : Google Scholar
|
|
26
|
Simes RJ, Marschner IC, Hunt D, et al:
Relationship between lipid levels and clinical outcomes in the
Long-term Intervention with Pravastatin in Ischemic Disease (LIPID)
Trial: to what extent is the reduction in coronary events with
pravastatin explained by on-study lipid levels? Circulation.
105:1162–1169. 2002. View Article : Google Scholar
|