Introduction
Patients with completely resected non-small cell
lung cancer (NSCLC) are at risk of relapse. Distant recurrence is a
leading form of relapse in 15% of stage IA and in 60% of stage IIIA
NSCLC patients (1). Previous
meta-analyses of adjuvant chemotherapies have shown that the
chemotherapies have survival benefit in patients with completely
resected NSCLC (2,3). Cisplatin (CDDP)-based chemotherapies
are recommended as the adjuvant chemotherapy in surgically resected
stage II and IIIA NSCLC (4,5).
Among the CDDP-based combination chemotherapies, chemotherapy with
CDDP and vinorelbine haveproven to be beneficial for survival in
NSCLC (6). Kato et
al(7) and Hamada et
al(8) demonstrated that
tegafur-uracil (UFT) adjuvant therapy improved the overall survival
period in stage I lung adenocarcinoma, however, this result has not
yet been proven worldwide.
Adjuvant chemotherapies have increased survival
rates by approximately 5% in 5 years in NSCLC, which does not
appear to be satisfactory (3,9).
Severe toxicities are occasionally observed in patients treated
with CDDP-based chemotherapies, and chemotherapy-related death has
been one of the major problems with adjuvant chemotherapies.
Accordingly, development of a novel therapeutic strategy that is
both safe and efficient is essential for patients with completely
resected NSCLC.
S-1 is an oral 5-fluorouracil-(5-FU)-based agent
containing tegafur, a 5-FU pro-drug, 5-chloro-2,4-dihydroxypyridine
(CDHP), and potassium oxonate (Oxo) (10). CDHP is an inhibitor of
dihydropyrimidine dehydrogenase, which degrades 5-FU. Oxo is
distributed in the gastrointestinal tract and inhibits orotate
phosphoribosyltransferase, a phosphoenzyme for 5-FU. Adjuvant
chemotherapy with the single-agent S-1 has been proven to have a
survival benefit in gastric cancer patients with a gastrectomy
(11). S-1 is administered to
patients for four weeks followed by a two-week rest period
(conventional schedule). A modified schedule, in which S-1 is
administered for two weeks followed by a one-week rest period
(modified schedule), is used if patients on the conventional
regimen experience severe toxicities (12).
Kim et al(13) reported that gastrectomy affected
the pharmacokinetics of S-1 in patients with gastric cancer. By
contrast, Kochi et al(14)
demonstrated that gastrectomy had no effect on the plasma
concentrations of 5-FU in patients treated with S-1. The effect of
gastrectomy on the pharmacokinetics of S-1 remains controversial,
while the pharmacokinetics of S-1 in patients with resected NSCLC
is likely to be different compared to patients with resected
gastric cancer.
In patients with advanced NSCLC, single-agent S-1
(conventional schedule) has been demonstrated to have a 22%
response rate and to add 10.5 months to the median survival period
(15). The feasibility of S-1
therapy was favorable to patients. Yano et al(16) reported that adjuvant chemotherapy
with S-1 was feasible in patients with completely resected NSCLC.
In that study, however, the conventional schedule of S-1
administration was not employed, and the schedule was modified. The
feasibility of the conventional schedule of S-1 has, therefore, not
previously evaluated in patients with completely resected
NSCLC.
Considering that, as described above, the
conventional administration schedule of S-1 has demonstrated
efficacy in the treatment of advanced NSCLC (15), we hypothesized that the
conventional schedule is likely to be efficient and feasible in
patients with completely resected NSCLC. Consequently, the present
study was conducted to evaluate the safety and efficacy of the
conventional schedule of S-1 adjuvant chemotherapy in patients with
completely resected NSCLC.
Materials and methods
Study design
The present study was designed as a multi-center,
single-arm, clinical phase II study to evaluate the feasibility of
S-1 adjuvant chemotherapy in patients with completely resected
NSCLC, and was undertaken between May 2007 and October 2010 in
Japan. The primary endpoint was relative dose intensity (RDI),
representing the actual dose-planned dose ratio of S-1. The
secondary endpoints were the safety and probability of 1-year
disease-free survival (1y-DFS). The present study was designed to
have 90% power for testing that RDI was not <50% at a one-side
5% significance level, if the actual RDI was >80%. Based on that
design, the minimum sample size was calculated to be 21 patients,
using the mathematical formula of one-stage phase II design of the
South West Oncology Group (http://www.swogstat.org/statoolsout.html). Thirty
patients were scheduled to enroll in the present study, while the
study population was selected from three hospitals in Hokkaido,
Japan. The present study was conducted in accordance with the
Declaration of Helsinki. The protocol was approved by the local
Institutional Review Board.
Patients
The present study comprised patients, who underwent
curative resection with ND2a lymphadenectomy for NSCLC between 2007
and 2009, with diagnoses of pathological stage IB-IIIA NSCLC. The
patients provided their signed written informed consent.
Eligible patients i) were 20–75 years old, ii) had
an Eastern Cooperative Oncology Group (ECOG) performance status of
0 or 1, iii) had adequate organ function [leukocyte count
>3.5×109 cells/l, platelet count
>100×109 cells/l, hemoglobin >9.0 g/dl, aspartate
and alanine aminotransferases (ASTs and ALTs) <2.0 × upper limit
of normal (ULN), serum bilirubin <2.0 x ULN, serum creatinine
<1.0 x ULN, BUN <25 mg/dl, creatinine clearance (CCr, which
was calculated by the Cockcroft-Gault equation) >60 ml/min,
PaO2>70 mmHg], iv) had undergone no prior
chemotherapy for NSCLC, v), were within 8 weeks of surgery and vi )
had a life expectancy of >3 months.
Treatment
S-1 was administered to patients within 8 weeks of
surgery. Patients received 40 mg/m2 S-1 orally twice
daily; the dose was 80 mg/body/day when the body surface area was
<1.25 m2, 100 mg/body/day for 1.25–1.50 m2
and 120 mg/body/day for >1.50 m2. S-1 was
administered for 4 weeks followed by a two-week rest period. These
cycles were repeated every 6 weeks, while the maximum treatment was
8 cycles.
Administration of S-1 was delayed if a patient had
any of the following toxicities on Day 1: leukocyte count
<3.0×109 cells/l, neutrophil count
<1.5×109 cells/l, platelet count
<100×109 cells/l, hemoglobin <8.0 g/dl, ASTs and
ALTs >2.0 x ULN, serum bilirubin >2.0 x ULN, serum creatinine
>1.0 x ULN or other non-hematological toxicities >grade
2.
The conventional schedule of S-1 was replaced by the
modified schedule, consisting of a two-week administration of S-1
and a one-week rest period, when a patient had one of the following
toxicities: leukocyte count <2.0x109 cells/l,
neutrophil count <1.0x109 cells/l, platelet count
<75x109 cells/l, hemoglobin <8.0 g/dl, ASTs and
ALTs >2.0 x ULN, serum bilirubin >2.0 x ULN, serum creatinine
>1.0 x ULN or other non-hematological toxicities >grade 3. In
the modified schedule, the cycles were repeated every three weeks,
while 2 cycles of the modified schedule were considered to be
equivalent to 1 cycle of the conventional regimen.
When patients had suffered from the above-mentioned
toxicities twice, the S-1 dose was reduced to 50 mg/body/day for
<1.25 m2, 80 mg/body/day for 1.25–1.5 m2
and 100 mg/body/day for >1.5 m2. Patients received
S-1 chemotherapy unless experiencing a relapse or was experienced
the following discontinuation criteria presented: i) suffered from
a third round of the indicated toxicities, ii) grade 4
hematological toxicities, iii) the creatinine increased to grade 2
or worse, iv) ASTs and ALTs increased to grade 3 or worse, v) other
non-hematological toxicities at grade 4 or vi) the next
chemotherapy cycle was delayed for >28 days.
Assessment of patients
Pathological stages of NSCLC were determined using
the 6th edition of the Union for International Cancer Control
Manual of Clinical Oncology (17).
Toxicities were assessed according to the National Cancer Institute
Common Terminology Criteria for Adverse Events version 3.0
(http://ctep.cancer.gov/reporting/ctc.html) (18). Adverse events were evaluated and
blood tests were carried out at each cycle. Screening tests
included hematology, blood chemistry and urinalysis. Disease-free
survival (DFS) was determined by the time period between enrollment
and recurrence. Computed tomography and tumor marker tests were
performed at least every 6 months subsequent to enrollment. DFS in
each patient was analyzed 1 year after surgery.
Statistical analysis
In the present study, P-values and confidence
intervals (CI) were two-sided, and P<0.05 was considered to
indicate a statistically significant difference. In the subgroup
analysis, the median values of RDI were compared using the
Mann-Whitney U test. The probability of 1y-DFS was estimated using
the Kaplan-Meier method. The correlation between the two variables
(RDI and age, RDI and CCr) was analyzed using the Spearman’s rank
correlation test. The difference between CCr in older (>65
years) and younger (<65 years) groups was analyzed using the
Student’s t-test. Statistical analysis was carried out using SPSS
Statistics version 19.0.0 (IBM, Tokyo, Japan).
Results
Patient characteristics
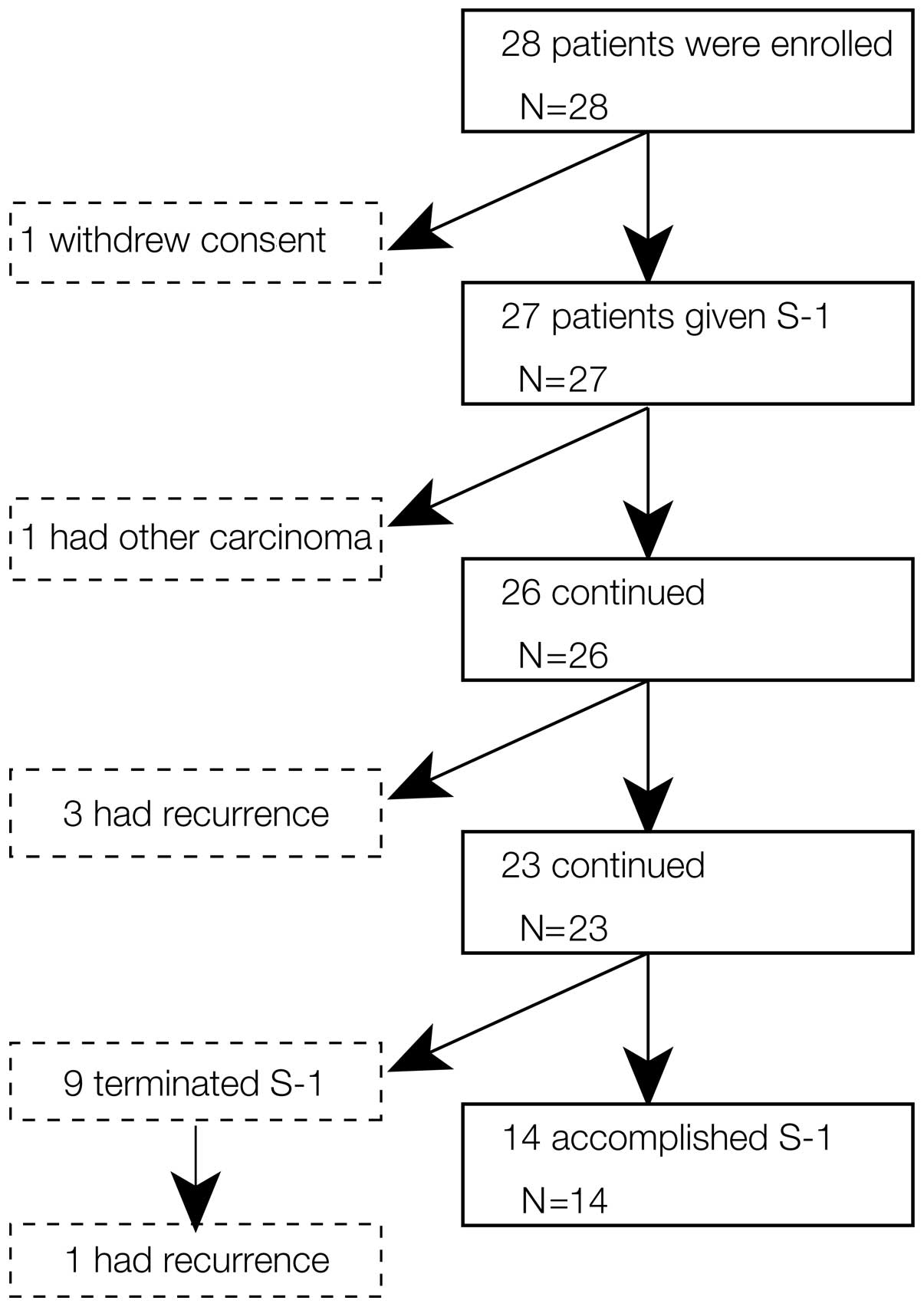
Between May 2007 and October 2009, 28 patients (22
male and 6 female) were enrolled in the present study (Fig. 1 and Table I). The enrollment was terminated
after interim analysis was carried out and RDI was confirmed not to
meet the expectations.
 | Table IPatient characteristics. |
Table I
Patient characteristics.
| Characteristics | Value |
|---|
| Age (years) | |
| Median | 67.0 |
| Range | 51–75 |
| Gender (n=28) | |
| Male | 22 |
| Female | 6 |
| Pathological
stage | |
| IB | 15 |
| IIA | 3 |
| IIB | 5 |
| IIIA | 5 |
| ECOG-PSa | |
| 0 | 6 |
| 1 | 22 |
| Histological
type | |
| Adenocarcinoma | 18 |
| Squamous cell
carcinoma | 7 |
| Others | 3 |
In the present study, one of the 28 patients refused
to be treated with S-1 after enrollment, thus never receiving S-1.
This patient was included in the analysis of RDI and 1-y DFS, but
excluded from the subgroup analysis. The median age of patients was
67.0 years, while 78.6% of the enrolled patients were males
(Table I). In this study, 15
patients had a diagnosis of NSCLC at the pathological stage IB and
18 had adenocarcinoma.
Feasibility of S-1 chemotherapy
The relative dose intensity for 28 patients was
63.1% (95% CI, 48.6–77.7). Fourteen patients (50.0%) completed all
8 planned courses of S-1, whereas the remaining patients received
an incomplete adjuvant chemotherapy. The average number of
completed courses was 5.3 (95% CI, 4.1–6.5). A schedule
modification was required for 10 patients (35.7%). Additionally,
the dose was reduced for 7 (70.0%) of the 10 patients, requiring a
schedule modification.
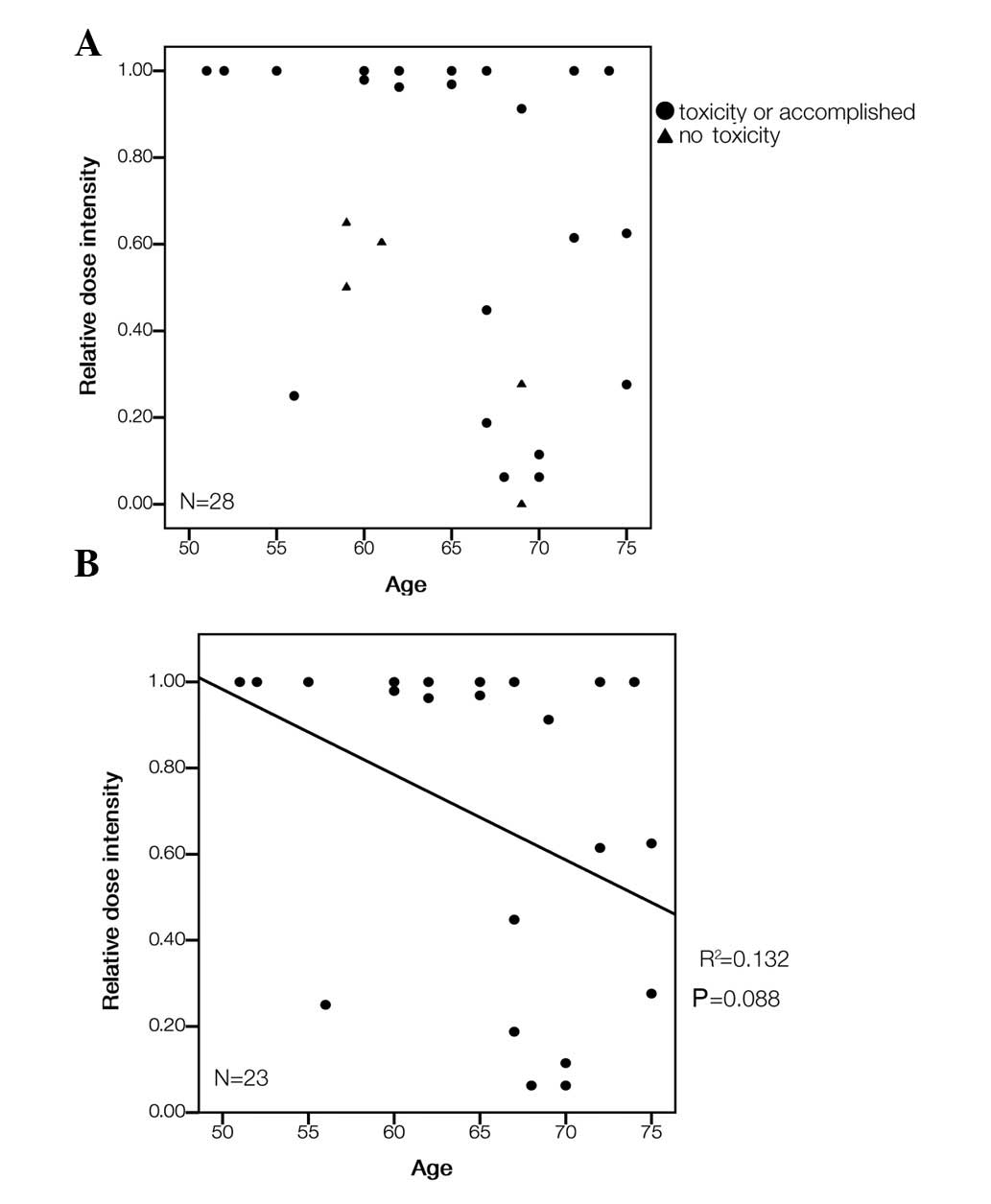
Fig. 2A shows a
scatter diagram of the correlation between age and RDI in the 28
patients. Fig. 2B shows a scatter
diagram of 23 patients, while 5 patients were excluded from the
analysis for reasons other than toxicities: 4 patients terminated
chemotherapy due to a recurrence or a simultaneous carcinoma; 1
patient refused to receive S-1 chemotherapy (excluded patients are
represented as triangles in Fig.
2A). Considering the distribution in the scatter diagram, the
RDI seemed to be lower in patients >65 years
(R2=0.132; P=0.088; Spearman’s rank correlation test)
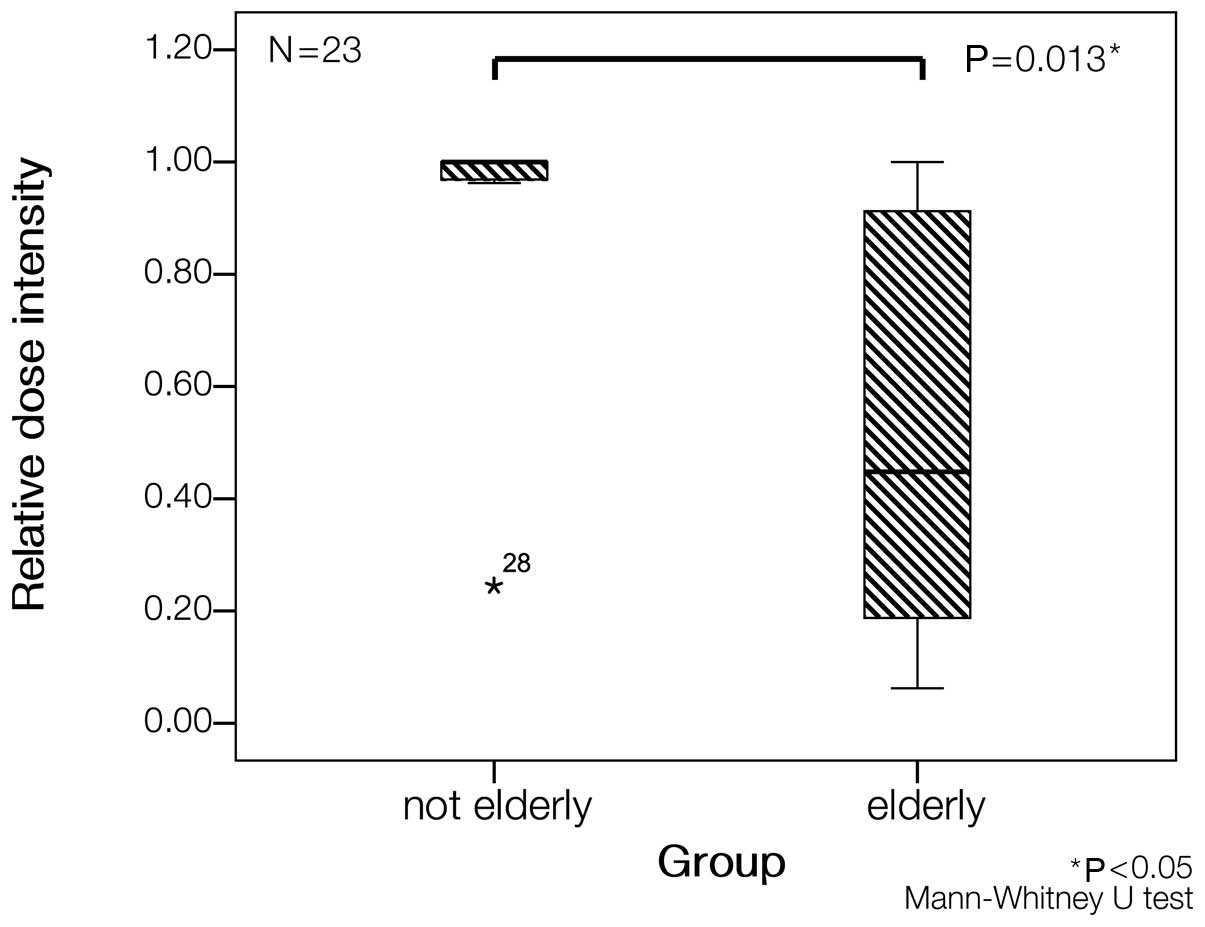
(Fig. 2B). The patients were
divided into groups of older (age >65 years) and younger
patients (age ≤65 years), showing that the median RDI in the older
patients was markedly lower compared to the younger patients (44.8
vs. 100%; P=0.013; Mann-Whitney U test) (Fig. 3).
Toxicity profiles
Adverse events in 27 eligible patients were
analyzed. No grade 4 or 5 toxicity was observed (Table II), while 4 patients had grade 3
adverse events including anorexia, extrapyramidal disorder,
pneumonitis and elevated serum amylase. In particular, 3/4 of
patients had grade 3 non-hematological toxicities on Days 15–29. No
grade 3 or worse hematological toxicity was observed in the present
study. The most common adverse events were anorexia, fatigue,
diarrhea and skin hyperpigmentation.
| Table IIToxicities. |
Table II
Toxicities.
| Event | Grade 1 | Grade 2 | Grade 3 | Grade 4 |
|---|
| Hematological | | | | |
| Leukopenia | 5 | 1 | 0 | 0 |
| Neutropenia | 4 | 1 | 0 | 0 |
| Anemia | 11 | 2 | 0 | 0 |
| Platelet | 9 | 2 | 0 | 0 |
|
Non-hematological | | | | |
| Skin
hyperpigmentation | 15 | 0 | 0 | 0 |
| Rash | 3 | 2 | 0 | 0 |
| Diarrhea | 10 | 1 | 0 | 0 |
| Nausea | 3 | 4 | 0 | 0 |
| Anorexia | 13 | 4 | 1 | 0 |
| AST or ALT | 7 | 2 | 0 | 0 |
| Creatinine | 1 | 1 | 0 | 0 |
| Fatigue | 13 | 3 | 0 | 0 |
| Dysgeusia | 2 | 1 | 0 | 0 |
| Oral
mucositis | 1 | 0 | 0 | 0 |
| Peripheral
neuropathy | 1 | 1 | 0 | 0 |
| Pyramidal
syndrome | 0 | 0 | 1 | 0 |
| Pneumonitis | 0 | 0 | 1 | 0 |
| Serum K
increased | 1 | 1 | 0 | 0 |
| Serum AMY
increased | 0 | 0 | 1 | 0 |
| Dizziness | 1 | 0 | 0 | 0 |
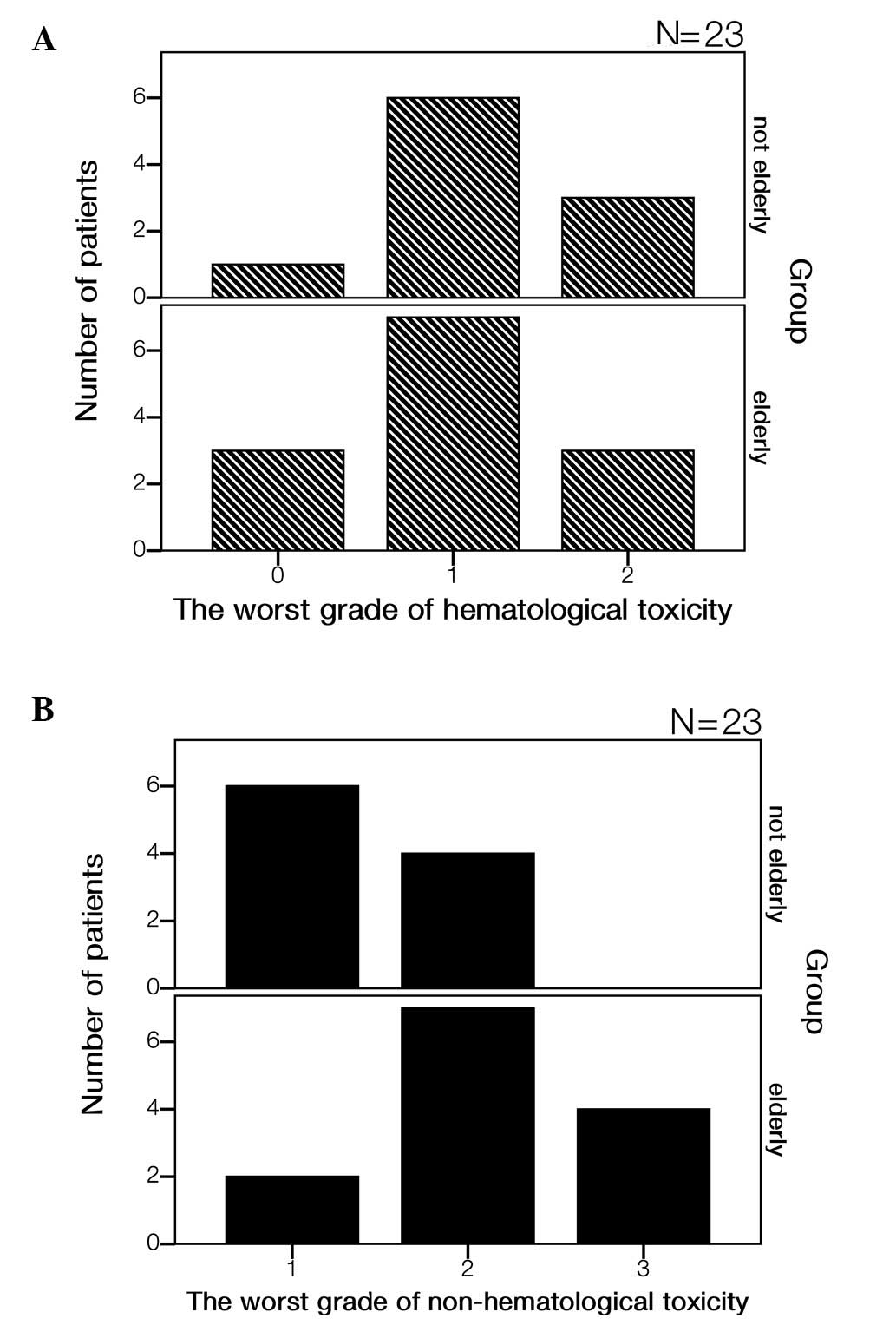
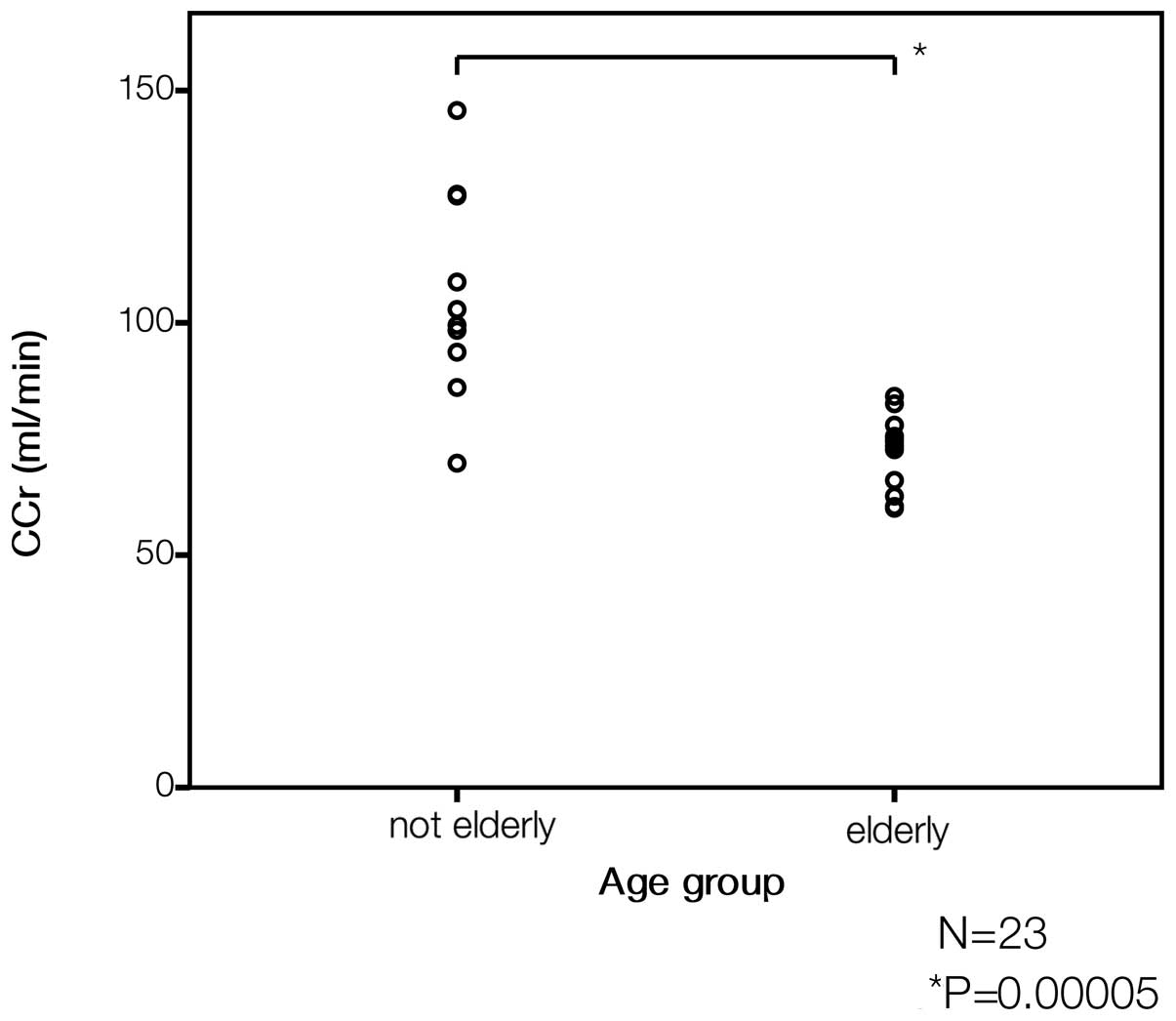
When the patients were divided by age as described
above, grade 2 and 3 non-hematological events were more likely to
be observed in the older compared to the younger group (Fig. 4). By contrast, the frequencies of
hematological toxicities in the older and younger groups were
similar. To determine the factor responsible for those differences,
CCr was analyzed in each group. CCr values in older patients were
lower compared to younger patients (Fig. 5), while CCr appeared to be
correlated with RDI (P=0.07; R2=0.128; Spearman’s rank
correlation test) (Fig. 6).
One-year DFS
The probability of DFS at 1 year was 85.7% (95% CI,
72.8–98.6) (Fig. 7). The average
of 1y-DFS period was 343.4 days (95% CI, 323.1–363.6). Relapse was
observed in 4 patients (14.3%). Of the 4 patients, 2 had stage IB
NSCLC and 2 had stage IIB and IIIA.
Discussion
In the present study, the feasibility of
chemotherapy with S-1 in patients with completely resected NSCLC
was evaluated. When a novel agent is employed in an adjuvant
chemotherapy, both efficacy and safety are of great interest. S-1
is an oral agent that was administered on an outpatient basis. It
is reasonable to use S-1 in adjuvant chemotherapy of NSCLC, if S-1
has a favorable feasibility and efficacy equivalent to that of
platinum-based chemotherapy. In the present study, four major
findings were reported: i) the average of RDI was 63.1%, while a
low S-1 RDI was observed in patients >65 years, ii) no grade 4
or worse toxicity was observed, although the older subgroup was
more likely to have non-hematological grade 2 and 3 toxicities,
iii) low CCr was observed in the older patients, possibly
accounting for both the increase in non-hematological toxicities
and the low RDI in the older patients and v) the 86% probability of
1y-DFS in the present study was acceptable.
In the present study, the RDI of S-1 was 63.1%,
although only 50% of the patients completed chemotherapy with S-1,
which was not satisfactory. In gastric cancer, Sakuramoto et
al(11) demonstrated the
survival benefit of adjuvant chemotherapy with S-1, as delineated
above. In their large-scale study, 66% of patients completed
chemotherapy with S-1, while 40% of patients required modification
of the treatment schedule (11,12).
The RDI in the present study seemed to be inferior to that in the
large-scale study.
The subgroup analysis of our results revealed that
patients >65 years had a markedly lower RDI compared to the
remaining patients (Figs. 2 and
3). Aoyama et al (19) reported that in gastric cancer no
difference was observed in the RDI of the adjuvant chemotherapy
with S-1 in older (≥70 years old) and younger (<70 years old)
patients with gastrectomy. However, Tsushima et al(20) demonstrated that median RDI in
younger (≤65 years old) patients was likely to be lower compared to
older (>65 years old) patients, including patients with
unresectable gastric cancer. The conventional schedule of S-1
administration was employed in the two studies. Since the present
study comprised no patients with gastrectomy, we referred to the
results reported by Tsushima et al(20). These results suggest that age is
likely to affect RDI in the conventional S-1 schedule in NSCLC.
Moreover, no grade 4 or worse toxicity was observed
in the present study (Table II).
The present toxicity profile appeared to be comparable to other
studies, suggesting that S-1 may be used in outpatients with
completely resected NSCLC. However, results of the present study
suggest that the older patients were more likely to have grade 3
non-hematological toxicities, while the incidence of hematological
toxicities was similar (Fig.
4).
In addition, lower CCr in elderly patients was
likely to be associated with lower RDI (Figs. 5 and 6). Tsushima et al(20) reported that CCr affected the dose
intensity of S-1 in advanced gastric cancer (12). Several studies have demonstrated
that approximately 50% of CDHP, a component of S-1 preventing
degradation of 5-FU, was excreted in urine, and that renal function
affects 5-FU concentrations in patients with solid tumors (21–23).
Moreover, Fujita et al(24)
reported that the area under the curve for CDHP was significantly
higher in older (≥75 years) compared to younger patients, due to
reduced renal function. Accordingly, we hypothecized that lower CCr
in older patients is likely to have affected the toxicity profile
and RDI in the present study.
In order to increase RDI in elderly patients, we
referred to studies in which S-1 schedule or dose modification was
employed. Several studies demonstrated that schedule- or
dose-modified S-1 therapy increased RDI in adjuvant chemotherapy
with S-1 (25–28). Shin et al(29) reported a modified schedule in which
S-1 was administered for two weeks followed by a one-week rest
period to be preferable for older patients with advanced colorectal
cancer. However, a phase I study of S-1 demonstrated that the
recommended dose of S-1 was 30 mg/m2 for North American
patients with advanced upper gastrointestinal cancer (30). Yano et al (16) demonstrated that in patients with
resected NSCLC, the modified schedule of S-1 generated a preferable
RDI (73.9%), as delineated above. Currently, most patients with
NSCLC are >65 years, and a schedule or dose modification may be
preferable for the adjuvant chemotherapy with S-1.
In the present study, the probability of 1y-DFS was
85.7% (Fig. 7), thus not lower
than the outcome reported in the post-operative course (31). However, this study included
patients with stage IB-IIIA NSCLC. We hypothesized that eligibility
might slightly affect the probability of 1y-DFS, although the
sample size was too small to estimate the survival benefit of
chemotherapy with S-1. As described above, single-agent S-1 has
been shown to provide a preferable response rate in advanced NSCLC,
although the adverse effects appear to be slightly less severe
compared to those of platinum-based chemotherapy, including
combination chemotherapy with a platinum agent and S-1 (15,32–35).
Thus, single-agent S-1 may be appropriate for patients with stage I
NSCLC.
In conclusion, the present data suggest that
single-agent S-1 in adjuvant chemotherapy often requires schedule
or dose modification. The conventional S-1 schedule is not likely
to be feasible in patients with completely resected NSCLC.
Acknowledgements
The authors thank Drs Yoshinori
Minami, Satoshi Endoh, Satoshi Hayashi, Kiyoko Shibukawa, Kaori
Ohnishi (Respiratory Center, Asahikawa Medical University,
Asahikawa, Japan), Drs Kensuke Ishida, Shoko Takeuchi, Eri
Toyoshima, Yasushi Yamamoto, Toshiyuki Ogasa, Shinobu Osanai (First
Department of Internal Medicine, Asahikawa Medical University,
Asahikawa, Japan), Drs Satoshi Hirata (Department of Operation,
Asahikawa Medical University), and Dr Hiroyuki Aoki (Department of
Respiratory Surgery, National Hospital Organization, Asahikawa
Medical Center, Asahikawa, Japan) for their support and for the
enrollment of patients in the present study.
References
|
1.
|
Pisters KM and Le Chevalier T: Adjuvant
chemotherapy in completely resected non-small-cell lung cancer. J
Clin Oncol. 23:3270–3278. 2005.
|
|
2.
|
Pignon JP, Tribodet H, Scagliotti GV, et
al: Lung adjuvant cisplatin evaluation: a pooled analysis by the
LACE Collaborative Group. J Clin Oncol. 26:3552–3559. 2008.
|
|
3.
|
Arriagada R, Auperin A, Burdett S, et al:
Adjuvant chemotherapy, with or without postoperative radiotherapy,
in operable non-small-cell lung cancer: two meta-analyses of
individual patient data. Lancet. 375:1267–1277. 2010.
|
|
4.
|
Pisters KM, Evans WK, Azzoli CG, et al:
Cancer Care Ontario and American Society of Clinical Oncology
adjuvant chemotherapy and adjuvant radiation therapy for stages
I-IIIA resectable non small-cell lung cancer guideline. J Clin
Oncol. 25:5506–5518. 2007.
|
|
5.
|
Crino L, Weder W, van Meerbeeck J and
Felip E: Early stage and locally advanced (non-metastatic)
non-small-cell lung cancer: ESMO Clinical Practice Guidelines for
diagnosis, treatment and follow-up. Ann Oncol. 21:v103–v115.
2010.
|
|
6.
|
Douillard JY, Tribodet H, Aubert D, et al:
Adjuvant cisplatin and vinorelbine for completely resected
non-small cell lung cancer: subgroup analysis of the Lung Adjuvant
Cisplatin Evaluation. J Thorac Oncol. 5:220–228. 2010.
|
|
7.
|
Kato H, Ichinose Y, Ohta M, et al: A
randomized trial of adjuvant chemotherapy with uracil-tegafur for
adenocarcinoma of the lung. N Engl J Med. 350:1713–1721. 2004.
|
|
8.
|
Hamada C, Tsuboi M, Ohta M, et al: Effect
of postoperative adjuvant chemotherapy with tegafur-uracil on
survival in patients with stage IA non-small cell lung cancer: an
exploratory analysis from a meta-analysis of six randomized
controlled trials. J Thorac Oncol. 4:1511–1516. 2009.
|
|
9.
|
Fruh M, Rolland E, Pignon JP, et al:
Pooled analysis of the effect of age on adjuvant cisplatin-based
chemotherapy for completely resected non-small-cell lung cancer. J
Clin Oncol. 26:3573–3581. 2008.
|
|
10.
|
Shirasaka T, Nakano K, Takechi T, et al:
Antitumor activity of 1 M tegafur-0.4 M
5-chloro-2,4-dihydroxypyridine-1 M potassium oxonate (S-1) against
human colon carcinoma ortho-topically implanted into nude rats.
Cancer Res. 56:2602–2606. 1996.
|
|
11.
|
Sakuramoto S, Sasako M, Yamaguchi T, et
al: Adjuvant chemotherapy for gastric cancer with S-1, an oral
fluoropyrimidine. N Engl J Med. 357:1810–1820. 2007.
|
|
12.
|
Iwasa S, Yamada Y, Fukagawa T, et al:
Management of adjuvant S-1 therapy after curative resection of
gastric cancer: dose reduction and treatment schedule modification.
Gastric Cancer. 14:28–34. 2011.
|
|
13.
|
Kim WY, Nakata B and Hirakawa K:
Alternative pharmacokinetics of S-1 components, 5-fluorouracil,
dihydrofluorouracil and alpha-fluoro-beta-alanine after oral
administration of S-1 following total gastrectomy. Cancer Sci.
98:1604–1608. 2007.
|
|
14.
|
Kochi M, Fujii M, Kanamori N, et al:
Effect of gastrectomy on the pharmacokinetics of S-1, an oral
fluoropyrimidine, in resectable gastric cancer patients. Cancer
Chemother Pharmacol. 60:693–701. 2007.
|
|
15.
|
Kawahara M, Furuse K, Segawa Y, et al:
Phase II study of S-1, a novel oral fluorouracil, in advanced
non-small-cell lung cancer. Br J Cancer. 85:939–943. 2001.
|
|
16.
|
Yano T, Yamazaki K, Maruyama R, et al:
Feasibility study of postoperative adjuvant chemotherapy with S-1
(tegaful, gimeracil, oteracil potassium) for non-small cell lung
cancer-LOGIK 0601 study. Lung Cancer. 67:184–187. 2010.
|
|
17.
|
Sobin L and Witthekind C: TNM
Classification of Malignant Tumours. 6th edition. Wiley-Liss; New
York: pp. 99–103. 2002
|
|
18.
|
Trotti A, Colevas AD, Setser A, et al:
CTCAE v3.0: development of a comprehensive grading system for the
adverse effects of cancer treatment. Semin Radiat Oncol.
13:176–181. 2003.
|
|
19.
|
Aoyama T, Yoshikawa T, Watanabe T, et al:
Safety and feasibility of S-1 adjuvant chemotherapy for gastric
cancer in elderly patients. Gastric Cancer. 15:76–82. 2011.
|
|
20.
|
Tsushima T, Hironaka S, Boku N, et al:
Safety and efficacy of S-1 monotherapy in elderly patients with
advanced gastric cancer. Gastric Cancer. 13:245–250. 2010.
|
|
21.
|
Hirata K, Horikoshi N, Aiba K, et al:
Pharmacokinetic study of S-1, a novel oral fluorouracil antitumor
drug. Clin Cancer Res. 5:2000–2005. 1999.
|
|
22.
|
Fujita K, Yamamoto W, Endo S, et al:
CYP2A6 and the plasma level of 5-chloro-2, 4-dihydroxypyridine are
determinants of the pharmacokinetic variability of tegafur and
5-fluorouracil, respectively, in Japanese patients with cancer
given S-1. Cancer Sci. 99:1049–1054. 2008.
|
|
23.
|
Ikeda M, Furukawa H, Imamura H, et al:
Pharmacokinetic study of S-1, a novel oral fluorouracil antitumor
agent in animal model and in patients with impaired renal function.
Cancer Chemother Pharmacol. 50:25–32. 2002.
|
|
24.
|
Fujita K, Nakayama H, Ichikawa W, et al:
Pharmacokinetics of 5-fluorouracil in elderly Japanese patients
with cancer treated with S-1 (a combination of tegafur and
dihydropyrimidine dehydrogenase inhibitor
5-chloro-2,4-dihydroxypyridine). Drug Metab Dispos. 37:1375–1377.
2009.
|
|
25.
|
Kimura Y, Kikkawa N, Iijima S, et al: A
new regimen for S-1 therapy aiming at adverse reaction mitigation
and prolonged medication by introducing a 1-week drug-free interval
after each 2-week dosing session: efficacy and feasibility in
clinical practice. Gastric Cancer. 6:34–39. 2003.
|
|
26.
|
Tsukuda M, Kida A, Fujii M, et al:
Randomized scheduling feasibility study of S-1 for adjuvant
chemotherapy in advanced head and neck cancer. Br J Cancer.
93:884–889. 2005.
|
|
27.
|
Sakuma K, Hosoya Y, Arai W, et al:
Alternate-day treatment with S-1 in patients with gastric cancer: a
retrospective study of strategies for reducing toxicity. Int J Clin
Oncol. 15:166–171. 2010.
|
|
28.
|
Arai W, Hosoya Y, Hyodo M, et al:
Alternate-day oral therapy with TS-1 for advanced gastric cancer.
Int J Clin Oncol. 9:143–148. 2004.
|
|
29.
|
Shin SJ, Jeong JH, Park YS, et al: Phase
II trial of S-1 mono-therapy in elderly or frail patients with
metastatic colorectal cancer. Invest New Drugs. 29:1073–1080.
2010.
|
|
30.
|
Zhu AX, Clark JW, Ryan DP, et al: Phase I
and pharmacokinetic study of S-1 administered for 14 days in a
21-day cycle in patients with advanced upper gastrointestinal
cancer. Cancer Chemother Pharmacol. 59:285–293. 2007.
|
|
31.
|
Hanagiri T, Baba T, So T, et al: Time
trends of surgical outcome in patients with non-small cell lung
cancer. J Thorac Oncol. 5:825–829. 2010.
|
|
32.
|
Schiller JH, Harrington D, Belani CP, et
al: Comparison of four chemotherapy regimens for advanced
non-small-cell lung cancer. N Engl J Med. 346:92–98. 2002.
|
|
33.
|
Ohe Y, Ohashi Y, Kubota K, et al:
Randomized phase III study of cisplatin plus irinotecan versus
carboplatin plus paclitaxel, cisplatin plus gemcitabine, and
cisplatin plus vinorelbine for advanced non-small-cell lung cancer:
Four-Arm Cooperative Study in Japan. Ann Oncol. 18:317–323.
2007.
|
|
34.
|
Okamoto I, Yoshioka H, Morita S, et al:
Phase III trial comparing oral S-1 plus carboplatin with paclitaxel
plus carboplatin in chemotherapy-naive patients with advanced
non-small-cell lung cancer: results of a west Japan oncology group
study. J Clin Oncol. 28:5240–5246. 2010.
|
|
35.
|
Kubota K, Sakai H, Yamamoto N, et al: A
multi-institution phase I/II trial of triweekly regimen with S-1
plus cisplatin in patients with advanced non-small cell lung
cancer. J Thorac Oncol. 5:702–706. 2010.
|