Introduction
Primary lung cancer is the leading cause of
mortality among the oncologic patient population. Approximately 1.5
million new cases are diagnosed annually worldwide (1). Despite the advances in early
detection, accurate staging and treatment, the survival rate of
lung cancer patients has not significantly improved over the past
30 years, with an average 5-year survival rate of ∼15% (1,2).
Surgery remains the main curative selection for patients with
early-stage non-small-cell lung cancer (NSCLC). However, not all
patients with resectable tumors are suitable candidates for
surgery, due to certain contraindications. Radiotherapy (RT) and/or
chemotherapy are commonly used for patients who are not considered
surgical candidates. However, these modalities are not usually
curative and are almost always accompanied by various toxic
complications. Thus, there is a need for effective alternatives to
surgery in patients with medically inoperable early-stage lung
cancer.
Intraoperative brachytherapy with radioactive
iodine-125 (125I) seed implantation has been proven to
be an effective therapeutic modality and an alternative to external
beam radiation therapy (EBRT) for patients with lung cancer
(3–6). However, intraoperative
125I seed implantation requires an open-chest approach,
which may result in more prolonged hospitalization and a
significant economic burden for the patients.
Computed tomography (CT)-guided percutaneous
delivery of 125I seeds for brachytherapy of malignant
lung tumors has already been performed (7). However, the conventional CT guidance
exhibits certain disadvantages, such as the lack of real-time
visualization, prolonged procedure time and a high incidence of
complications.
In the present study, we assessed the advantages of
the combined use of computed tomographic fluoroscopy (CTF) guidance
with transthoracic 125I brachytherapy for the treatment
of selected patients with early-stage NSCLC.
Materials and methods
Patient information
Between January, 2006 and March, 2011, 24 patients
with a total of 28 primary lung cancer lesions were enrolled in
this prospective study. All the patients were histopathologically
diagnosed by bronchoscopy and/or transthoracic needle biopsy (TNB)
and staged according to the American Joint Committee for Cancer
Staging manual (7th edition). The inclusion criteria were: i)
patients with stage T1-3N0M0 NSCLC not considered appropriate for
resection due to high-risk factors, such as poor heart and/or lung
function; ii) patients with resectable lung cancer who refused
surgical treatment and; iii) long diameter of the lesion of <8
cm. The patient characteristics are presented in Table I. The protocol for the present
study was approved by our Institutional Review Board. The patients
were informed about the potential risks, benefits and complications
of the procedure and written consent was provided on the day prior
to the treatment.
 | Table I.Patient characteristics prior to
CTF-guided 125I seed implantation. |
Table I.
Patient characteristics prior to
CTF-guided 125I seed implantation.
| Characteristics | Value |
|---|
| Age, years [mean
(range)] | 65.4 (54–81) |
| Gender | |
| Male | 18 |
| Female | 6 |
| Histopathology,
n | |
| Squamous
carcinoma | 9 (11) |
| Adenocarcinoma | 15 (17) |
| Tumor T stage, n | |
| T1 | 7 (8) |
| T2 | 12 (15) |
| T3 | 5 (5) |
| Maximum lesion
diameter, cm [mean (range)] | 4.0±1.5
(2.1–7.6) |
Instruments and implant treatment
planning
A multidetector CT scanner with an 85-cm gantry bore
(Brilliance CT-Big Bore Oncology, Philips Medical Systems
(Cleveland), Inc., Cleveland, OH, USA) was used to guide the
125I seed implantation. A monitor for monitoring the
procedure and a foot pedal for operating the CTF were available
within the scanner room.
The 125I seeds (registered no.,
H20041350) were purchased from Shanghai GMS Pharmaceutical Co.,
Ltd. (Shanghai, China) and approved by the United States Food and
Drug Administration. The 125I isotope was absorbed in
minute silver rods and furnished in 4.5×0.8-mm cylindrical titanium
capsules welded by laser at both ends. The pre-planned
125I seeds were housed into the cartridge chamber of an
implantation gun that provided complete shielding and were
sterilized with auto-claving prior to use.
The pre-implant dosimetric planning was performed
using the Seed Interstitial Radiotherapy Planning System (SIRPS,
KeLinZhong Medical Technique Institute, Beijing, China). The
prescription dose was defined as a minimal peripheral dose of
100–120 Gy. A CT scan spanning the entire lung with a 5-mm slice
thickness was performed in all the patients 1–2 weeks prior to the
seed implantation. The continuous axial images were transferred to
the Treatment Planning System (TPS). The planning target volume,
defined as the gross tumour volume (GTV) with a 0.5–1-cm safety
margin, was outlined on each axial image. The prescribed D90 (the
dose delivered to 90% of the target volume) was calculated through
the TPS. Postoperative dosimetric verification was routinely
performed for all the patients. A chest CT scan with the same
parameters as those of pre-operation one was obtained immediately
after the seed implantation. The axial CT images were transferred
to the TPS. Based on the recommendations of the American
Brachytherapy Society (ABS) (8),
the D90 dose, the isodose curves for each slice and the dose-volume
histograms (DVH) of the target were generated on the TPS.
Implant technique protocol
The patients were placed on the CT table in a
comfortable position that facilitated the pre-planned access route.
A sequential axial CT scan of the region of interest was performed
with a slice thickness of 5 mm. The access path of the puncture
needle was assessed on the axial images combined with the
pre-implant plan. Under local anesthesia, the 18-G implantation
needles (Hakko Medical Co., Ltd, Nagano-ken, Japan) were inserted
through the intercostal space closely below the ribs at the end of
a soft expiration phase and were then advanced into the lesion
under CTF guidance. During the entire procedure, the patients were
instructed to maintain gentle breathing. Four frames of contiguous,
cross-sectional fluoroscopic images with a slice thinkness of 3 or
6 mm were generated as the foot pedal was pressed. The
125I seeds were subsequently deposited while withdrawing
the needle from the distal to the proximal portion of each lesion
at 0.5–1-cm intervals.
After the procedure, a CT scan of the entire chest
was obtained to confirm the seed distribution and exclude any
procedure-related complications. The procedure time was defined as
the duration from the initiation of the CT scan for the
localization of lesion to the successful implantation of all the
125I seeds. Technical success was defined as the
pre-operatively planned 125I seeds being implanted in
the appropriate area within the tumor based on the pre-treatment
plan formulated with the TPS. After the procedure, the patients
were instructed to maintain bed rest for 6 h, lying on the puncture
site, with routine monitoring of the vital signs.
Follow-up assessment and response
criteria
At post-procedure day 1, a chest radiograph was
routinely performed to identify possible complications. A CT scan
was performed when pneumothorax, hemorrhage or other complication
was suspected. Patients were followed up with physical examinations
and thoracic CT scans at 2, 4 and 6 months post-125I
seed implantation. The follow-up period was prolonged by 3–6 months
if there was no evidence of disease progression after the first 6
months post-procedure. CT images were simultaneously reviewed by
all the interventional radiologists involved in this study and a
consensus was obtained for each session of the examination. The
longest diameter of the lesion was measured with calipers on the CT
workstation.
The response criteria were based on the measurement
of the longest diameter of all the target lesions and were
classified as follows: i) complete response (CR), disappearance of
the target lesion; ii) partial response (PR), ≥30% decrease in the
longest diameter of the target lesion; iii) progressive disease
(PD), ≥20% increase in the longest diameter of the target lesion;
and iv) stable disease (SD), neither sufficient shrinkage of the
lesion to qualify for PR nor sufficient increase to qualify for PD
(9). The local tumor control rates
were defined as the percentage of the sum of CR, PR and SD of all
the target lesions. Local control failure was determined by PD.
Cancer-related death was defined as the endpoint.
Statistical analysis
The local tumor control rates, local control failure
rates and complications were documented at the end of the present
study. The statistical analyses were performed with SPSS 19.0
statistical software (SPSS Inc., Chicago, IL, USA). The
Kaplan-Meier method was used to estimate survival curves.
Results
Technical outcomes
All the patients successfully completed the
CTF-guided 125I seed implantation, with a mean procedure
time of 45.7 min (range, 30–75 min). The radioactivity of the
125I seeds was 0.7 mCi. All the required seeds were
deposited in the corresponding areas based on the pre-planned
dosimetry. The median number of needle tracks was 14 (range, 6–53)
and the median number of implanted 125I seeds was 30
(range, 10–100). The post-treatment dosimetric measurement
demonstrated that the actual D90 ranged from 69 to 132 Gy (median,
107 Gy) and the median follow-up time was 31.5 months (range, 8–46
months).
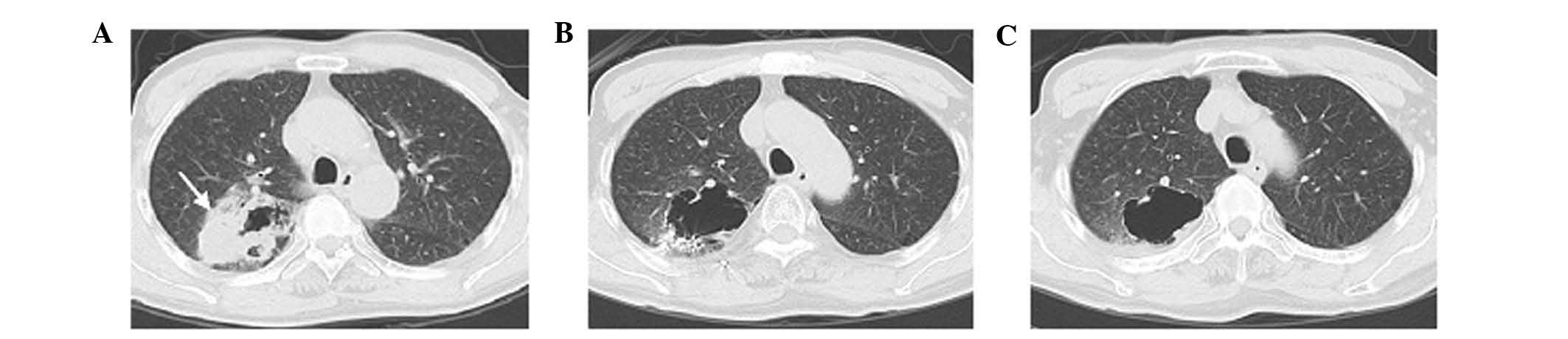
Local control rate (LCR)
At the end of follow-up period, the number of the
target lesions exhibiting CR, PR and SD was 8, 10 and 4,
respectively. Thus, the tumor LCR was 78.6% (22/28) (Figs. 1 and 2). Local control failure (or PD) occurred
in 6 lesions (21.6%, 6/28), demonstrated as either lesion
progression after treatment or local recurrence during the
follow-up period. Distant metastases were confirmed in 3
patients.
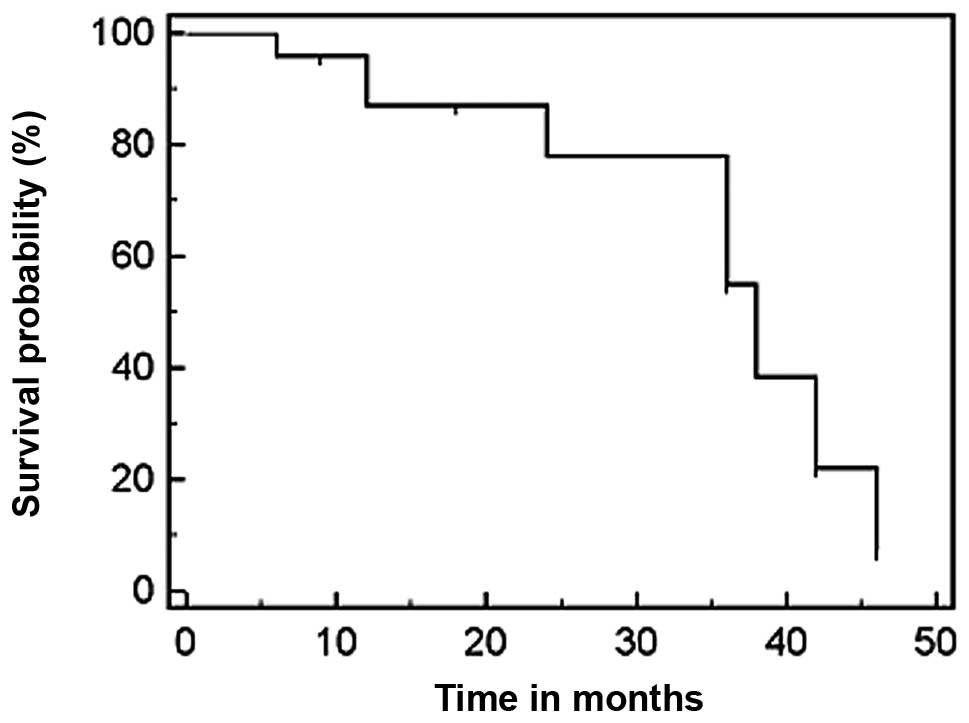
Survival outcomes
The overall 1-, 2- and 3-year survival rate was
95.8, 78 and 55%, respectively. The median survival time was 38
months (range, 8–46 months) (Fig.
3). At the end of the follow-up period, 19 patients had died,
whereas 3 patients were lost to follow-up and 2 patients remained
alive. Of the 19 deceased patients, 14 succumbed to cancer-related
causes, including local recurrence and metastasis, whereas 5
patients succumbed to other diseases.
Complications
No severe complications occurred during the
follow-up period. Of the 24 treated patients, 3 (12.5%) experienced
asymptomatic pneumothorax with a lung volume compression of <10%
and 4 (16.7%) developed mild hemorrhage along the needle tracks
after the procedure, without hemoptysis. The pneumothorax and
hemorrhage were treated conservatively and resolved within 1 week.
The post-procedure chest CT revealed no significant radiation
pneumonitis, whereas regional emphysema was identified in the
location of the brachytherapy seeds in 2 patients, which required
no further treatment. No seed migration was observed.
Discussion
Lung cancer remains one of the leading causes of
mortality worldwide. Although surgery remains the gold standard for
the treatment of early-stage NSCLC, a significant proportion of
patients with otherwise resectable lung cancer may exhibit other
comorbidities, precluding surgical resection. In patients with
medically inoperable early-stage lung cancer, conventional
chemotherapy and/or EBRT is commonly the treatment choice. However,
despite aggressive multiple-drug regimens and the addition of
radiation treatment, survival remains poor without surgery and
recurrence is the rule, regardless of the initial treatment
selection.
Radiofrequency ablation (RFA), a commonly used
thermal ablation technique and stereotactic body radiation therapy
(SBRT) are emerging treatment modalities. These methods have been
applied in high-risk patients with early-stage lung cancer.
However, although these modalities have recently attracted
attention due to their promising results (10), they have certain limitations.
The successful treatment of hepatic tumors using RFA
has resulted in this method being used for other solid tumors, such
as lung cancer. However, regarding lung cancer, available data on
the histomorphological effects of this method are limited. Although
RFA may generally be considered as an effective alternative to
surgical resection for the treatment of stage I NSCLC, it remains
controversial. Early immunohistochemical findings following RFA
revealed complete tumor cell necrosis in only 38% of the cases
(11). The high proportion of
remaining viable tumor cells following ablation casts doubt on RFA
as a curative concept. This approach may be considered with extreme
caution as a palliative treatment option for lung cancer (11). In addition, RFA is not suitable for
lung tumors that are >3 cm in diameter or centrally located
(12–14).
SBRT employs external fixation and hypofractionation
to deliver a high dose per fraction of radiation to a small target
volume. Therefore, it appears to be a valid alternative to
conventional 3D-CRT, with high rates of local control and promising
survival rates according to recent reported series (15–18).
Local failure was associated with tumor size, target definition and
central or pleural proximity (15). The most appropriate tumor size for
SBRT was considered to be ∼2–3 cm. When the GTV was >65
cm3, SBRT was ineffective (16). Although a higher biological
equivalent dose (BED) may result in improved LCR, the optimal BED
range for SBRT was 83.2–146 Gy for stage I NSCLC, due to the
toxicity associated with higher doses (17). Even within this dose range,
however, different types and rates of toxicity have been reported.
A 39.9% rate of adverse effects and 10% of grade 3–4 toxicity
according to the Radiation Therapy Oncology Group (RTOG) were
reported by Baumann et al (15). It was previously reported that
toxicity may be associated with tumor location. Grade 3–5 toxicity
was observed in 10.4 and 27.3% of patients with peripheral and
central lung tumors, respectively (18). Acute ≥grade 2 pulmonary toxicity
developed in 6.5% and symptomatic pneumonia in 10% of the patients
after a median interval of 5 months (19). Furthermore, SBRT may be associated
with significant skin toxicity. Hoppe et al reported that,
after a minimum of 3 months of follow-up, 38% of the patients
developed grade 1, 8% grade 2, 4% grade 3 and 2% grade 4 acute skin
toxicity (20). Additional side
effects, such as fatigue, dyspnea/cough or transient thoracic pain
were recorded in approximately 10% of the patients (21).
Iodine-125 (125I) is a commonly used
radionuclide with a half-life of approximately 60 days, emitting
gamma-rays with a maximum energy of 35 keV. Intraoperative
brachytherapy is an effective therapeutic modality for patients for
whom surgical resection is contraindicated (3,4). The
primary aim of radiation therapy is the eradication of the tumor
without damage to healthy tissue and adjacent organs.
Intraoperative 125I seed implantation is able to deliver
a higher radiation dose to the tumor and a lower radiation dose to
the surrounding healthy tissues compared to EBRT. Intraoperative
implantation of 125I seeds has been used for the
treatment of lung cancer, either as an alternative to or in
combination with surgical resection. The implantation techniques
and purposes may vary according to different studies. Previous
studies reported that a vicryl mesh containing 125I
seeds may be inserted over the tumor bed or the resection margins
following video-assisted thoracoscopic resection (VATR) for
early-stage NSCLC deemed unsuitable for conventional surgery due to
high risk (3,4), whereas others reported that
125I seeds were implanted along the resection margin
following limited resection in NSCLC patients who were not
considered candidates for lobectomy or pneumonectomy (5). It was demonstrated that
intraoperative 125I seed brachytherapy for early-stage
NSCLC patients resulted in improved LCR, decreased local recurrence
and prolonged survival (3–5,22).
However, intraoperative 125I seed implantation exhibits
two disadvantages. First, it lacks the standard pre-implantation
treatment plan indicating the number, location, dose and activity
of the seeds, which is critical for successful brachytherapy.
Second, it is an invasive procedure, involving open-chest surgery,
even with the VATR approach.
CT-guided TNB is currently an established technique
for diagnostic evaluation of pulmonary nodules. The advent of CT
fluoroscopy has rendered TNB more facile. It allows near real-time
monitoring of the placement of the TNB needles and thereby
significantly shortens the duration of the TNB procedure (23). Therefore, CTF may facilitate the
percutaneous implantation of 125I seeds for the
treatment of lung cancer. Until recently, the percutaneous delivery
of 125I seeds for brachytherapy of malignant lung tumors
was performed mainly under conventional CT guidance (7). The disadvantages of conventional
CT-guided 125I seed implantation include lack of
real-time visualization, a high incidence of complications (such as
pneumothorax) and prolonged patient discomfort due to the longer
duration of the procedure (1–2 h).
In the present study, we attempted to combine the
advanced CTF-guidance technique and percutaneous brachytherapy with
125I seed implantation for the treatment of lung cancer,
which achieved near real-time visualization and accurate
localization of the accessed needles and implanted seeds. The
results of our study demonstrated that the mean duration of the
procedure was 45.7 minutes, which was significantly shorter
compared to that under conventional CT-guidance. The incidence of
procedure-related complications was also markedly reduced. It was
previously demonstrated that the most common complications of
conventional CT-guided biopsy and 125I seed implantation
included pneumothorax and hemorrhage in 12.5–31 and 9.2–46.9% of
the treated patients, respectively (7). In our study, small asymptomatic
pneumothorax developed in 3 patients (12.5%) and mild, self-limited
hemorrhage along the needle tracks in 4 patients (16.7%), without
hemoptysis. These complications spontaneously resolved within 1
week after the intervention, without requiring special management.
Under CTF-guidance, the inserted needle may be observed as it
advances. The near real-time monitoring by CTF may help the
operators avoid the puncture of bullae, interlobar fissures and
vessels, decrease the number of pleural punctures, shorten the
duration of the procedure and, thereby, reduce the incidence of
pneumothorax and hemorrhage. Therefore, percutaneous
125I seed implantation may be performed more
conveniently, efficiently and safely under CTF-guidance.
Additionally, radioactive complications, such as lung fibrosis,
loss of pulmonary function and cardiac toxicity, which are common
following EBRT (24,25), have not been reported following
intraoperative 125I brachytherapy.
Although 125I seed implantation has been
applied for the treatment of lung cancer for more than two decades,
the number of studies pertaining to long-term results is limited.
To the best of our knowledge, there are no available studies on the
treatment of early-stage NSCLC with CTF-guided 125I seed
implantation with a curative intent. Zhang et al (7) reported the results of CT-guided
radioactive 125I seed implantation in the treatment of
localized advanced pulmonary carcinoma. The results of that study
demonstrated that the LCR was 78.1% at 2 months of follow-up, with
a 1-year survival rate of 65.0%, which were significantly higher
compared to that of the control group treated by chemotherapy.
Optimal outcomes for early-stage NSCLC have been achieved with SBRT
thus far, with a 3-year LCR of 40-89% and a 3-year overall survival
(OS) of 42.7–57.1% (16,19,22).
In the present study, the lesion LCR was 78.6% at the end of a
median follow-up period of 31.5 months and the 1-, 2- and 3-year OS
for stage T1-3N0 NSCLC was 95.8, 78 and 55%, respectively. In
addition, we prescribed a radiation dose of 100–120 Gy, which was
higher compared to that of conventional EBRT. That dose contributed
to the satisfactory local lesion control, without any evidence of
radiation damage to the surrounding healthy tissues and organs
during the follow-up period.
In conclusion, the present study demonstrated that
CTF is able to provide real-time guidance for percutaneous
implantation of high-dose 125I seeds within the lung
tumor. CTF-guided percutaneous implantation of 125I
seeds appears to be a feasible, safe and effective modality for the
treatment of inoperable early-stage NSCLC. However, our study had
certain limitations and further studies, including larger patient
samples and longer follow-up periods are required.
References
|
1.
|
Spiro SG and Silvestri GA: One hundred
years of lung cancer. Am J Respir Crit Care Med. 172:523–529.
2005.PubMed/NCBI
|
|
2.
|
Collins LG, Haines C, Perkel R and Enck
RE: Lung cancer: diagnosis and management. Am Fam Physician.
75:56–63. 2007.
|
|
3.
|
d’Amato TA, Galloway M, Szydlowski G, Chen
A and Landreneau RJ: Intraoperative brachytherapy following
thoracoscopic wedge resection of stage I lung cancer. Chest.
114:1112–1115. 1998.PubMed/NCBI
|
|
4.
|
Chen A, Galloway M, Landreneau R, et al:
Intraoperative 125I brachytherapy for high-risk stage I
non-small cell lung carcinoma. Int J Radiat Oncol Biol Phys.
44:1057–1063. 1999.
|
|
5.
|
Lee W, Daly BD, DiPetrillo TA, Morelli DM,
Neuschatz AC, Morr J and Rivard MJ: Limited resection for non-small
cell lung cancer: observed local control with implantation of I-125
brachy-therapy seeds. Ann Thorac Surg. 75:237–242. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Pisch J, Belsley SJ, Ashton R, Wang L,
Woode R and Connery C: Placement of 125I implants with
the da Vinci robotic system after video-assisted thoracoscopic
wedge resection: a feasibility study. Int J Radiat Oncol Biol Phys.
60:928–932. 2004.
|
|
7.
|
Zhang FJ, Li CX, Wu PH, Wu YX, Jiao DC,
Liu J and Li YL: CT guided radiazctive 125I seed
implantation in treating localized advanced pulmonary carcinoma.
Zhonghua Yi Xue Za Zhi. 87:3272–3275. 2007.(In Chinese).
|
|
8.
|
Nag S, Beyer D, Friedland J, Grimm P and
Nath R: American Brachytherapy Society (ABS) recommendations for
transperineal permanent brachytherapy of prostate cancer. Int J
Radiat Oncol Biol Phys. 44:789–799. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Eisenhauer EA, Therasse P, Bogaerts J, et
al: New response evaluation criteria in solid tumors: revised
RECIST guideline (version 1.1). Eur J Cancer. 45:228–247. 2009.
View Article : Google Scholar
|
|
10.
|
Das M, Abdelmaksoud MH, Loo BW Jr and
Kothary N: Alternatives to surgery for early stage non-small cell
lung cancer-ready for prime time? Curr Treat Options Oncol.
11:24–35. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Schneider T, Reuss D, Warth A, et al: The
efficacy of bipolar and multipolar radiofrequency ablation of lung
neoplasms - results of an ablate and resect study. Eur J
Cardiothoracic Surg. 39:968–973. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Abbas G, Schuchert MJ, Pennathur A,
Gilbert S and Luketich JD: Ablative treatments for lung tumors:
radiofrequency ablation, stereotactic radiosurgery, and microwave
ablation. Thorac Surg Clin. 17:261–271. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13.
|
Nguyen CL, Scott WJ, Young NA, Rader T,
Giles LR and Goldberg M: Radiofrequency ablation of primary lung
cancer: results from an ablate and resect pilot study. Chest.
128:3507–3511. 2005.PubMed/NCBI
|
|
14.
|
Ambrogi MC, Lucchi M, Dini P, et al:
Percutaneous radiofrequency ablation of lung tumours: results in
the mid-term. Eur J Cardiothorac Surg. 30:177–183. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15.
|
Baumann P, Nyman J, Lax I, et al: Factors
important for efficacy of stereotactic body radiotherapy of
medically inoperable stage I lung cancer. A retrospective analysis
of patients treated in the Nordic countries. Acta Oncol.
45:787–795. 2006. View Article : Google Scholar
|
|
16.
|
Beitler JJ, Badine EA, El-Sayah D, et al:
Stereotactic body radiation therapy for nonmetastatic lung cancer:
an analysis of 75 patients treated over 5 years. Int J Radiat Oncol
Biol Phys. 65:100–106. 2006.PubMed/NCBI
|
|
17.
|
Zhang J, Yang F, Li B, et al: Which is the
optimal biologically effective dose of stereotactic body
radiotherapy for stage I non-small-cell lung cancer? A
meta-analysis. Int J Radiat Oncol Biol Phys. 81:e305–e316. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Fakiris AJ, McGarry RC, Yiannoutsos CT,
Papiez L, Williams M, Henderson MA and Timmerman R: Stereotactic
body radiation therapy for early-stage non-small-cell lung
carcinoma: four-year results of a prospective phase II study. Int J
Radiat Oncol Biol Phys. 75:677–682. 2009.PubMed/NCBI
|
|
19.
|
Guckenberger M, Heilman K, Wulf J, Mueller
G, Beckmann G and Flentje M: Pulmonary injury and tumor response
after stereo-tactic body radiotherapy (SBRT): results of a serial
follow-up CT study. Radiother Oncol. 85:435–442. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
20.
|
Hoppe BS, Laser B, Kowalski AV, et al:
Acute skin toxicity following stereotactic body radiation therapy
for stage I non-small-cell lung cancer: who’s at risk? Int J Radiat
Oncol Biol Phys. 72:1283–1286. 2008.PubMed/NCBI
|
|
21.
|
Ricardi U, Filippi AR, Guarneri A, et al:
Stereotactic body radiation therapy for early stage non-small cell
lung cancer: results of a prospective trial. Lung Cancer. 68:72–77.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Mutyala S, Stewart A, Khan AJ, Cormack RA,
O’Farrell D, Sugarbaker D and Devlin PM: Permanent iodine-125
interstitial planar seed brachytherapy for close or positive
margins for thoracic malignancies. Int J Radiat Oncol Biol Phys.
76:1114–1120. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
23.
|
Templeton PA, White CS, Protopapas Z, et
al: Real-time continuous imaging CT guidance for lung biopsy.
Radiology. 201:2701996.
|
|
24.
|
Slater JD, Ellerbroek NA, Barkley HT,
Mountain C, Oswald MJ, Roth JA and Pepers LJ: Radiation therapy
following resection of non-small cell bronchogenic carcinoma. Int J
Radiat Oncol Biol Phys. 20:945–951. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
25.
|
Choi NC and Kanarek DJ: Toxixity of
thoracic radiotherapy on pulmonary function in lung cancer. Lung
Cancer. 10:S219–S230. 1994. View Article : Google Scholar : PubMed/NCBI
|