Introduction
The recent advances in cancer treatment have
improved patient survival. Cancers that have metastasized to the
bones are considered to be at an advanced stage. Metastatic bone
tumors often promote skeletal-related events (SREs), which include
pathological fractures, neurological complications caused by
compression of the spinal cord or cauda equina, or hypercalcemia,
as well as the need for radiotherapy or surgery of the bone
metastasis (1,2). Although the prognosis of patients
with certain types of cancer has improved with the recent advances
in chemotherapy and radiotherapy, patients with metastatic bone
tumors require treatment of the primary lesion as well as anti-SRE
assessment, in order to improve their quality of life and
prognosis.
Metastatic bone tumors are treated by
multidisciplinary teams, in which orthopaedic surgeons play an
important role in the diagnosis and treatment of the bone
metastasis, as well as in the detection of the primary cancer
lesion. A delay in the diagnosis increases the risk of SREs and
negatively affects the prognosis. In this regard, we investigated
the background of patients with bone metastasis and the factors
associated with prognosis. We investigated 145 cases of metastatic
bone tumors with respect to the primary lesion, affected bone site
and frequency of SREs and evaluated the effectiveness of a single
computed tomography (CT) scan of the chest/abdomen/pelvis against
that of 18F-fluoro-2-deoxyglucose (18F-FDG)
positron emission tomography (PET)-CT scan in detecting the primary
lesion of a metastatic bone tumor.
Materials and methods
Patients
In this retrospective study, we reviewed the medical
records and imaging results of 145 patients with metastatic bone
tumors who were referred to the Department of Orthopaedic Surgery,
Kagoshima University, between 2006 and 2011. The patients included
81 men and 64 women, with a mean age of 65 years (range, 29–87
years) and a mean follow-up of 9 months. A bone scan was performed
on 97 patients.
The study protocol was approved by the Ethics
Committee on Clinical Research at the Kagoshima University Hospital
and all the patients provided written informed consent prior to
inclusion.
Evaluation of imaging modalities and
patient survival
Two well-trained radiologists reviewed all the bone
scan results and compared them with radiographs, CT or magnetic
resonance imaging (MRI) scans. The results of the imaging
modalities were assessed taking into account clinical symptoms and
any positive findings that indicated bone metastasis. To identify
the primary lesion, a single chest/abdominal/pelvic CT,
18F-FDG PET-CT and Tl scan were performed on each
patient. Following an initial detection of the primary lesion,
roentgenogram, MRI, biopsy and formal clinical follow-up were
performed to obtain a definitive diagnosis. We examined the
frequency of each primary tumor, bone metastatic site and incidence
of SREs; we also estimated the survival rate and the detection rate
of the original lesion using clinical examinations and evaluated
the factors affecting survival. The survival rate was analyzed
according to the Kaplan-Meier method. The clinical examinations
that were performed to locate the original tumor were also
evaluated.
Statistical analysis
Statistical analysis was performed using the
Student’s t-test or the Chi-square test and analyzed using
Microsoft Office Excel software (Microsoft, Redmond, WA, USA).
Kaplan-Meier analysis was performed using Kaplan 97 software.
P<0.05 was considered to indicate statistically significant
differences.
Results
Primary lesion and bone metastatic
site
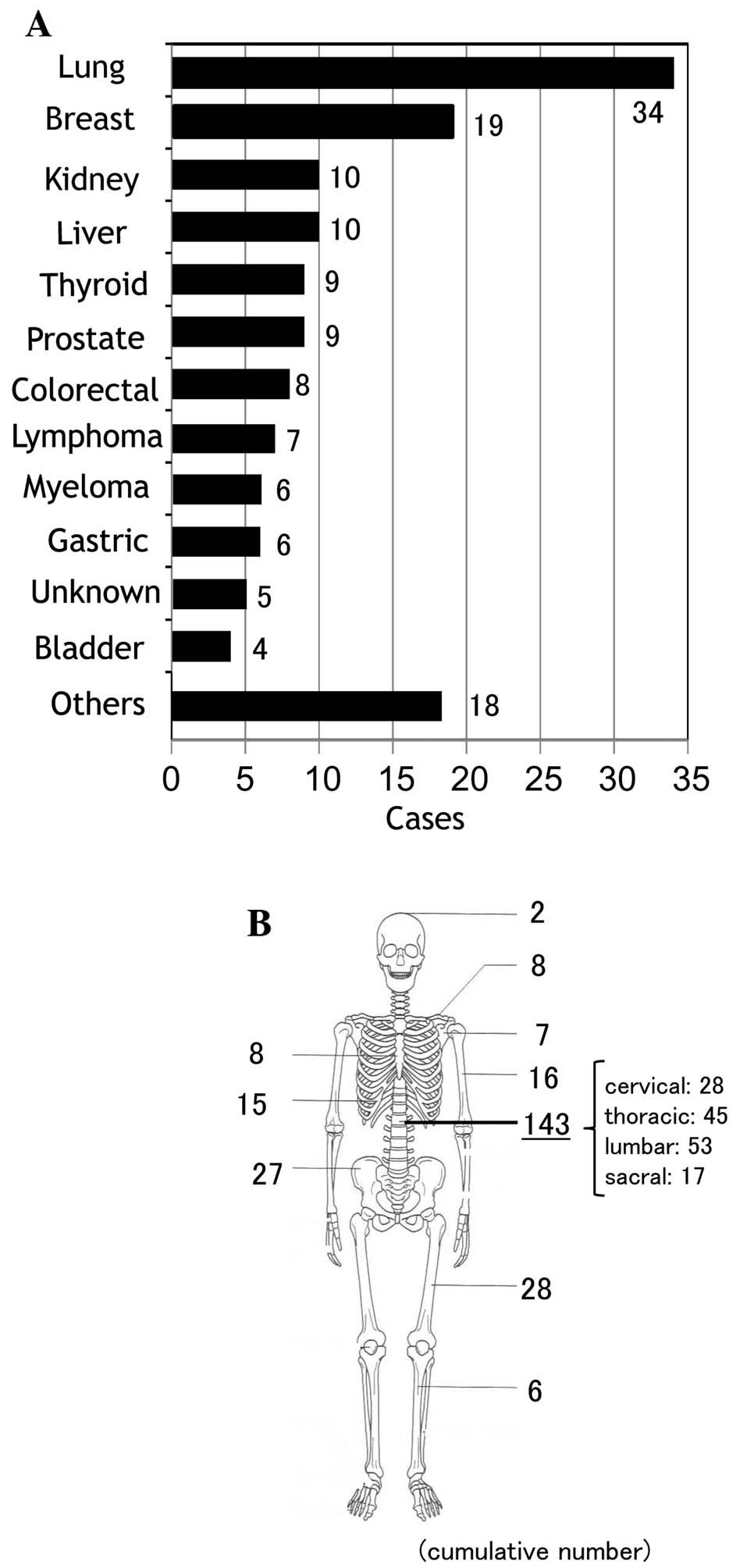
We examined the origin of all metastatic bone tumors
(145 cases). The most frequent origin of bone metastasis was lung
cancer (34 cases, 23%), followed by breast cancer (19 cases, 13%),
kidney cancer (10 cases, 7%), liver cancer (10 cases, 7%), thyroid
cancer (9 cases, 6%), prostate cancer (9 cases, 6%), colorectal
cancer (8 cases, 6%), malignant lymphoma (7 cases, 5%), multiple
myeloma (6 cases, 4%), gastric cancer (6 cases, 4%), and bladder
cancer (4 cases, 3%), as previously reported (3–5). The
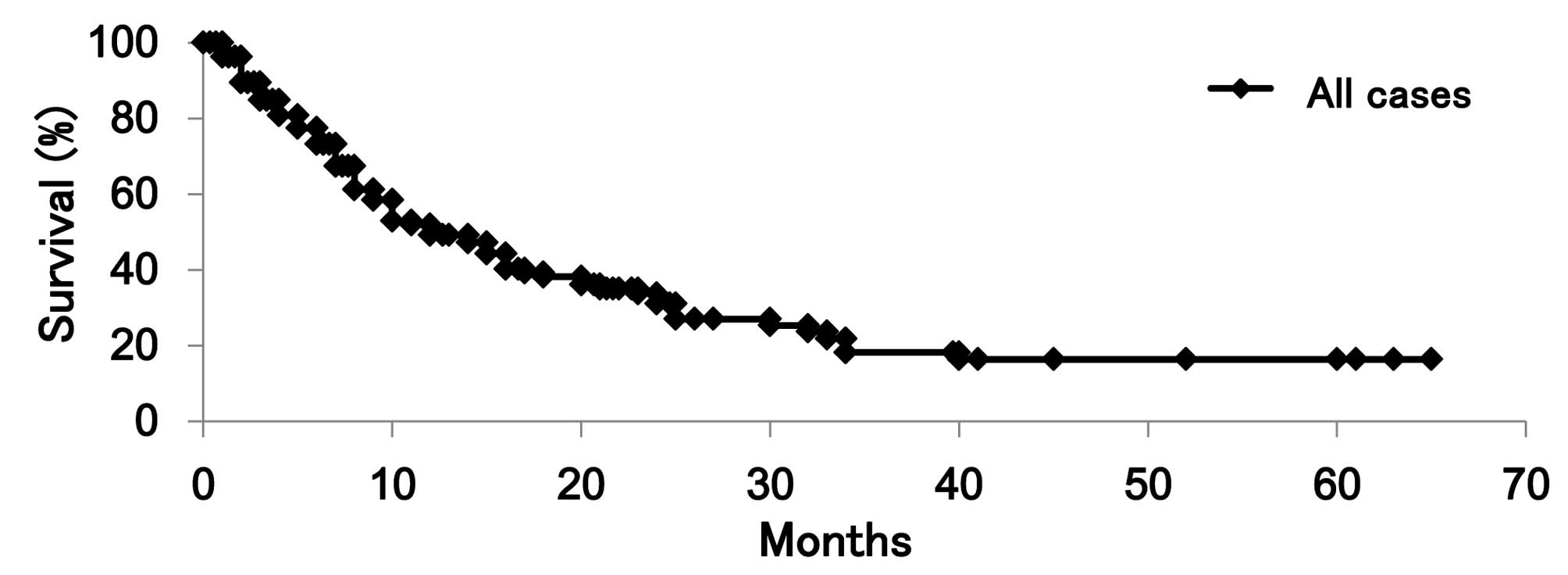
primary tumor could not be identified in 5 cases (3%; Fig. 1A). The Kaplan-Meier analysis
demonstrated that the 1-, 2- and 3-year survival rate was 49, 34
and 18%, respectively, among all patients with bone metastasis
(Fig. 2).
The most frequent bone metastatic site was the spine
(143 cases), including the cervical vertebrae (28 sites), thoracic
vertebrae (45 sites), lumbar vertebrae (53 sites) and sacrum (17
sites). Other sites of metastasis included the femur (28 cases),
pelvis (27 cases), humerus (16 cases) and ribs (15 cases) (Fig. 1B). Our findings revealed that the
most frequent spinal metastatic site was the lumbar spine, followed
by the thoracic and cervical spine. It was previously reported that
the most frequent metastatic site was the thoracic spine, followed
by the lumbar and cervical spine (6–9). To
explain this discrepancy, we compared the primary malignant tumor
between the lumbar and thoracic metastatic groups. We identified no
statistically significant difference in the primary lesion between
these two groups.
The primary tumor site distribution was compared
between patients with a known primary lesion and those with unknown
primary lesion at the first visit. In the primary-known group
(n=84), the primary tumors were breast (18 cases, 21%), lung (11
cases, 13%), liver (9 cases, 11%), thyroid (7 cases, 8%) and kidney
cancer (6 cases, 7%). In the primary-unknown group (n=61), the
primary tumors were lung cancer (23 cases, 38%), myeloma (5 cases,
8%), kidney and prostate cancer and malignant lymphoma (4 cases
each, 7%) (Table I). During the
follow-up period, the primary lesion was not identified in 5 cases.
The number of breast cancer cases was statistically significantly
lower in the primary-unknown group. However, the number of myeloma
was significantly higher in the primary-unknown group.
 | Table IComparison of the primary tumor site
between groups with known and unknown origin at initial visit. |
Table I
Comparison of the primary tumor site
between groups with known and unknown origin at initial visit.
| Origin known at
initial visit | Cases | Origin unknown (%) →
diagnosed | Cases (%) |
|---|
| Breast | 18a (21) | Lung | 23 (38) |
| Lung | 11 (13) | Myeloma | 5b (8) |
| Liver | 9 (11) | Kidney | 4 (7) |
| Thyroid | 7 (8) | Prostate | 4 (7) |
| Kidney | 6 (7) | Lymphoma | 4 (7) |
| Prostate | 5 (6) | Gastric | 3 (5) |
| Colorectal | 5 (6) | Colorectal | 3 (5) |
| Lymphoma | 3 (4) | Thyroid | 2 (3) |
| Esophagus | 3 (4) | Pancreas | 2 (3) |
| Gastric | 3 (4) | Bladder | 2 (3) |
| Uterus | 3 (4) | Breast | 1a (2) |
| Tongue | 2 (2) | Others | 8 (12) |
| Bladder | 2 (2) | | |
| Myeloma | 1b (1) | | |
| Others | 6 (7) | | |
| Total | 84 (100) | Total | 61 (100) |
Factors affecting the prognosis of bone
metastasis
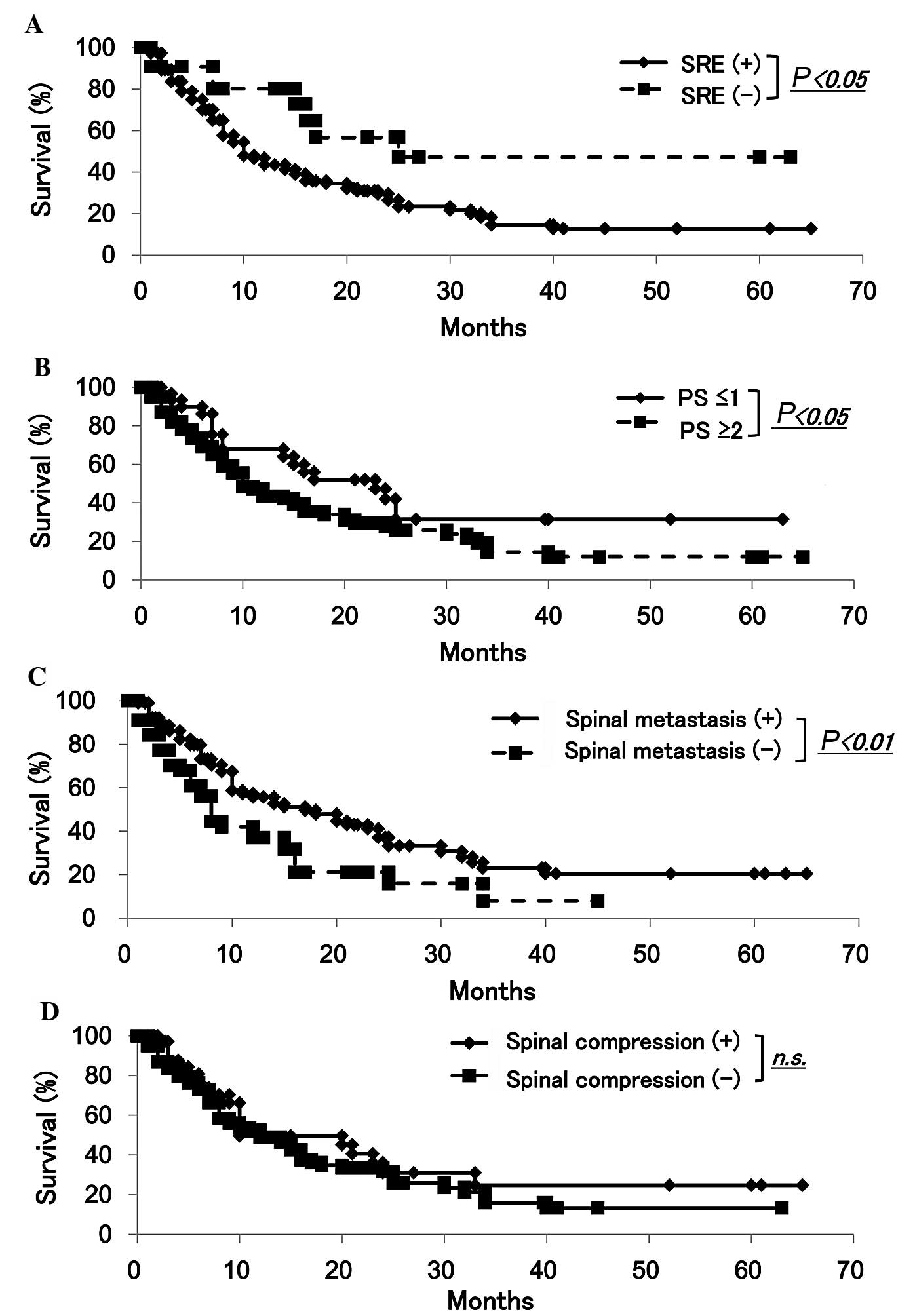
We first investigated the association between
prognosis and SREs and observed that survival was significantly
lower in the SREs compared to that in the non-SREs group (Fig. 3A). In addition, PS was found to be
an important factor for the selection of the appropriate
chemotherapeutic regimen and, therefore, we investigated the
association between patient prognosis and PS (10,11)
and survival was found to be significantly lower in the PS≥2
compared to that in the PS≤1 group (Fig. 3B). Since the most frequent bone
metastatic site was the spine, we investigated the association
between spinal metastasis and patient prognosis. The Kaplan-Meier
analysis revealed that the 1- and 3-year survival rates for
patients with spinal metastases was 56 and 23%, respectively.
Furthermore, the 1- and 3-year survival rates for patients with
non-spinal metastases were 37 and 8%, respectively. Therefore,
survival rates were significantly lower in the non-spinal compared
to those in the spinal metastatic group (Fig. 3C). To determine which factors were
associated with a favorable prognosis in patients with spinal
metastasis, we investigated the association between prognosis and
neurological complications caused by compression of the spinal cord
or cauda equina. The Kaplan-Meier analysis revealed that
neurological complications did not exert a significant effect on
survival for any of the patients with bone metastasis (Fig. 3D). We next investigated the primary
lesion in the non-spinal and spinal metastatic groups and found
that the number of breast cancer patients was higher in the spinal
metastatic group (Table II).
| Table IIComparison of the primary tumor site
between groups with and without spinal metastasis. |
Table II
Comparison of the primary tumor site
between groups with and without spinal metastasis.
| Spinal metastasis
(+) | Cases | Spinal metastasis
(−) | Cases |
|---|
| Lung | 22 | Lung | 12 |
| Breast | 17a | Kidney | 5 |
| Liver | 8 | Thyroid | 4 |
| Prostate | 7 | Liver | 4 |
| Colorectal | 6 | Bladder | 4 |
| Thyroid | 5 | Lymphoma | 3 |
| Kidney | 5 | Esophagus | 2 |
| Myeloma | 5 | Gastric | 2 |
| Gastric | 4 | Breast | 2a |
| Lymphoma | 4 | Prostate | 2 |
| Pancreas | 3 | Colorectal | 2 |
| Tongue | 2 | Others | 4 |
| Others | 11 | | |
| Total | 99 | Total | 46 |
Association between SREs and prognosis or
PS
We demonstrated that the survival rate was
significantly lower in the PS≥2 compared to that in the PS≤1 group
(Fig. 3B). We investigated the
association between SREs and PS. The incidence of SREs among all
the bone metastatic cases was 107 (74%). Hypercalcemia (serum
calcium levels, 10.4–12.6 mg/dl; normal range, 8.5–10.3 mg/dl)
occurred in 8 cases (5.5%) and was accompanied by renal dysfunction
in 4 of the 8 cases (Table
IIIA). Symptoms caused by compression of the spinal cord or
cauda equina were observed in 36 cases (24.8%), including symptoms
of the cervical (11 cases), thoracic (15 cases) and lumbar segments
(10 cases) (Table IIIA and B).
Pathological fractures were detected in 23 cases (15.9%), including
fractures of the extremities (femur, 9 cases; and humerus, 5
cases); thoracic vertebrae, 3 cases; and lumbar vertebrae, 2 cases
(Table IIIC). Surgery for SREs
was performed in 26 cases (18%), including internal fixation (10
cases), resection plus reconstruction (9 cases), spinal
decompression (2 cases), spinal fusion (4 cases) and total en bloc
spondylectomy (1 case) (Table
IIID). Radiotherapy for bone metastasis was performed in 75
cases (51.7%).
| Table IIIAnalysis of SREs. |
Table III
Analysis of SREs.
| A, Number of cases
per SRE |
|---|
|
|---|
| Cases | Fracture | Hypercalcemia | Spinal
compression | Radiation therapy
for bone metastasis | Surgery for bone
metastasis | Total cases with
SREs |
|---|
| No. (%) | 23 (15.9) | 8 (5.5) | 36 (24.8) | 75 (51.7) | 26 (17.9) | 107 (73.8) |
|
| B, Distribution of
spinal metastases in patients with symptoms caused by compression
of spinal cord or cauda equina |
|
| Cases | Cervical spine | Thoracic spine | Lumbar spine | Total |
|
| No. (%) | 11 (30.5) | 15 (41.7) | 10 (27.8) | 36 (100) |
|
| C, Pathological
fractures |
|
| Cases | Femur | Humerus | Thoracic spine | Lumbar spine | Others | Total |
|
| No. (%) | 9 (39.1) | 5 (21.7) | 3 (13.0) | 2 (8.7) | 4 (17.5) | 23 (100) |
|
| D, Type of surgery
for pathological fractures |
|
| Cases | Resection plus
reconstruction | Internal
fixation | Spinal fusion | Spinal
decompression | Total en bloc
spondylectomy | Total |
|
| No. (%) | 9 (34.6) | 10 (38.5) | 4 (15.4) | 2 (7.7) | 1 (3.8) | 26 (100) |
|
| E, Incidence of
SREs in groups with better (≤1) and worse (≥2) PS |
|
| Cases, no. (%) | Fracture | Hypercalcemia | Spinal
compression | Radiation therapy
for bone metastasis | Surgery for bone
metastasis |
|
| PS≤1 (n=32) | 3 (9.4) | 2 (6.3) | 3 (9.4)a | 14 (43.8) | 4 (12.5) |
| PS≥2 (n=113) | 20 (17.7) | 6 (5.3) | 33 (29.2)a | 70 (61.9) | 24 (21.2) |
In the group with better PS scores (≤1, n=32),
pathological fractures were detected in 3 cases (9.4%),
neurological complications were observed in 3 cases (9.4%),
hypercalcemia occurred in 2 cases (6.3%), surgery for SREs was
performed in 4 cases (12.5%) and radiotherapy was performed in 14
cases (43.8%). In the group with poor PS scores (≥2, n=113),
pathological fractures were detected in 20 cases (17.7%),
neurological complications caused by compression of the spinal cord
or cauda equina were observed in 33 cases (29.2%), hypercalcemia
occurred in 6 cases (5.3%), surgery for SREs was performed in 24
cases (21.2%) and radiotherapy was performed in 70 cases (61.9%).
Among the 5 SREs, only neurological complications were found to be
significantly increased in the group with a PS score of ≥2 compared
to that with a PS score of ≤1 (Table
IIIE).
Identification of the primary lesion
using imaging studies
The primary tumor site was identified using
diagnostic imaging in 49 cases, which included CT (32 cases) and
18F-FDG PET-CT (17 cases) (Table IVA). Whole-body bone scans and Tl
scans could not identify the primary lesion. CT was performed on 55
patients (90%) in whom the primary tumor was not identified during
the first visit to the hospital. The time interval from the first
visit until the CT scan was performed was 3.6 days.
18F-FDG PET-CT was performed on 39 patients (64%) with
unidentified primary tumors. The time interval from the first visit
until the 18F-FDG PET-CT was performed was 7.2 days. CT
scans helped identify the following primary cancers: lung (16
cases), kidney (3 cases), thyroid (2 cases), pancreatic (2 cases)
and bladder cancer (2 cases), myeloma (2 cases) and others (5
cases). 18F-FDG PET-CT scans identified the following
primary cancers: lung (6 cases), prostate (4 cases), colorectum (2
cases) and others (5 cases) (Table
IVB). A CT scan alone was able to identify primary tumors of
the bladder (2 cases), myeloma (2 cases) and thyroid cancer (1
case) that could not be identified using 18F-FDG PET-CT
imaging. However, a 18F-FDG PET-CT scan alone was able
to identify primary lung cancer (1 case), myeloma (1 case) and
colorectal cancer (1 case) (Table
IVB). Although there were no significant differences between CT
and 18F-FDG PET-CT scans in the detection of primary
lesions, CT scans were found to be more useful in determining the
primary lesion of a bone metastasis in a timelier manner.
| Table IVComparison of imaging modalities for
the identification of the primary lesion in patients with bone
metastasis. |
Table IV
Comparison of imaging modalities for
the identification of the primary lesion in patients with bone
metastasis.
| A, Time interval
for detection of the primary lesion with different imaging
modalities |
|---|
|
|---|
| Imaging
modality | Detection of
primary lesion/total number of patients | Interval between
first visit and examination (days) |
|---|
| CT scan | 32/55 | 3.6 |
| PET-CT | 17/39 | 7.2 |
| Bone scan | 0/43 | 6.3 |
| Tl scan | 0/13 | 5.5 |
|
| B, Number of cases
with different primary lesions detected with CT or PET-CT |
|
| Method of
identification of primary lesion |
|
|
| Primary lesion | CT | PET | CT alone | PET alone |
|
| Lung | 16 | 6 | 0 | 1 |
| Kidney | 3 | 1 | 0 | 0 |
| Thyroid | 2 | 0 | 1 | 0 |
| Bladder | 2 | 0 | 2 | 0 |
| Pancreas | 2 | 0 | 0 | 0 |
| Myeloma | 2 | 1 | 2 | 1 |
| Gastric | 1 | 1 | 0 | 0 |
| Liver | 1 | 1 | 0 | 0 |
| Colorectal | 1 | 2 | 0 | 1 |
| Lymphoma | 1 | 0 | 0 | 0 |
| GIST | 1 | 0 | 0 | 0 |
| Prostate | 0 | 4 | 0 | 0 |
| Breast | 0 | 1 | 0 | 0 |
| Total | 32 | 17 | 5 | 3 |
Discussion
Over the last few years, the number of cancer
patients has increased. The majority of patients who are diagnosed
with bone metastasis are referred to an orthopaedic surgeon to
evaluate the bone metastasis and its progression, locate the
primary lesion and decide upon treatment options.
We demonstrated that metastasis to the spine was the
most frequent, followed by the femur and pelvic bone, as previously
reported (6). Of the total bone
metastases, the ratio of spinal metastasis was 54.7% (141/258
lesions). Our findings revealed that the number of bone metastases
to the spine was lower compared to what was previously reported; in
addition, the incidence of lumbar metastasis was relatively high
compared to previous reports (6–9,12).
Overall survival depends mainly on the type of the primary tumor.
We did not identify a statistically significant difference
regarding the type of primary tumor between the lumbar and thoracic
metastatic groups. The relatively low number of spinal metastases
may be the cause of this discrepancy. However, further studies are
required to elucidate this issue.
It has been reported that the median overall
survival of patients with spinal metastases is 7 months. In
addition, only 10–20% of patients with spinal metastases remained
alive at 2 years after diagnosis (12). We found that the 1-year survival
rate was 49% and the 3-year survival rate was 18% among all
patients with bone metastasis. Our results indicated a relatively
good prognosis compared to those of a previous study (12). In addition, the survival rates were
significantly lower in patients in the non-spinal compared with
those in the spinal metastatic group, which included all the
patients with bone metastasis. Furthermore, our findings revealed
that the number of breast cancer patients was higher in the spinal
compared to that in the non-spinal metastatic group. Survival was
significantly increased in breast cancer patients with bone
metastasis compared to those with other primary lesions with bone
metastasis (data not shown). These findings suggest that
differences in the origin of the cancer may affect prognosis,
depending on whether bone metastasis occurs in the spine or
elsewhere.
We demonstrated that SREs exert a significant
negative effect on survival. Although neurological complications
did not appear to exert a statistically significant effect on
survival in patients with spinal metastasis, the number of patients
with neurological complications was statistically different between
the PS≤1 and PS≥2 groups. These findings suggest that the incidence
of neurological complications was increased in the group with PS≥2
and negatively affected survival. In addition, Katagiri et
al (11) reported that PS
scores of 3 or 4 were a significant poor prognostic factor. Our
findings suggest that a PS score of 2 may also exert a negative
effect on prognosis in patients with bone metastasis.
We observed that the primary lesion distribution
differed depending on whether the primary tumor was known or
unknown at the initial visit. In the primary-known group, the most
frequent primary cancer was breast cancer, followed by lung, liver
and thyroid cancer. Our findings suggest the significance of the
follow-up of cancer patients with bone metastasis. In the
primary-unknown group, the most frequent primary cancer was lung
cancer, followed by myeloma, kidney and prostate cancer. Consistent
with our results, Iizuka et al (4) reported that myeloma was the most
common primary malignancy in cases with spinal metastasis of
unknown origin, followed by lung and prostate cancer. Destombe
et al (3) reported that the
most frequent primary cancer was lung, followed by breast cancer.
These findings suggest that, when evaluating bone metastatic
patients with unknown primary tumors, clinical examinations should
be performed taking into consideration the possibility of
diagnosing these primary cancers. During the follow-up period, the
primary lesion was not identified in 5 cases. It was reported that
lung and pancreatic cancer were the most frequent primary lesions
in autopsy studies (13,14). Our findings demonstrated that
pancreatic cancer was diagnosed as the primary lesion in only 2
cases (3%) in the primary-unknown group. These findings suggest
that more detailed examinations, including magnetic resonance
cholangiopancreatography or endoscopic retrograde
cholangiopancreatography, may be required for bone metastatic
patients in whom the primary lesion was not identified.
Although biopsy of the most accessible osseous
lesion was routine during the examination, the proportion of an
accurate final diagnosis in solid and hematopoietic tumors was low
(4,5,15).
In addition, biopsy requires invasive procedures.
18F-FDG PET-CT whole-body imaging is non-invasive and
highly sensitive. It has been reported that 18F-FDG
PET-CT should be used as a first-line imaging examination for
patients with a primary carcinoma of unknown origin, rather than
after other diagnostic procedures have failed to identify the
primary lesion (16). Although
18F-FDG PET-CT is useful in helping physicians locate
the primary lesion, patients were required to wait an average of
7.2 days for an 18F-FDG PET-CT examination, due to the
long waiting list. We demonstrated that CT scans helped identify 32
of the 55 (58%) primary lesions within 3.6 days from the time of
the patient’s first visit. Therefore, a CT scan is a rapid
examination, valuable for the identification of the primary lesion
of a bone metastasis. In addition, we did not observe a
statistically significant difference in utility between CT and
18F-FDG PET-CT in establishing the origin of a bone
metastasis. Our findings suggest that a CT scan should be performed
prior to an 18F-FDG PET-CT scan, particularly if the
latter requires a waiting period of several days.
To improve the prognosis of patients with metastatic
bone tumors, a team approach is required, comprising an orthopaedic
surgeon along with a specialist to manage treatment of the primary
tumor, a radiologist, rehabilitation staff and a palliative care
team (17). Collaboration is
essential to developing a treatment strategy that may be tailored
to the individual patient (18).
In this regard, our department has established a bone metastasis
registration system that encompasses all specialties in our
hospital and is accessible to each specialty.
In conclusion, our findings demonstrated that
several factors may be related to patient prognosis and the
effectiveness of CT; these factors may prove useful in determining
the origin of the primary lesion. Further examination of prognostic
factors and advancements in diagnostic imaging may improve the
treatment of patients with bone metastasis.
References
|
1
|
Coleman RE: Bisphosphonates: clinical
experience. Oncologist. 9(Suppl 4): 14–27. 2004. View Article : Google Scholar
|
|
2
|
Lipton A, Colombo-Berra A, Bukowski RM,
Rosen L, Zheng M and Urbanowitz G: Skeletal complications in
patients with bone metastases from renal cell carcinoma and
therapeutic benefits of zoledronic acid. Clin Cancer Res.
10:6397S–6403S. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Destombe C, Botton E, Le Gal G, et al:
Investigations for bone metastasis from an unknown primary. Joint
Bone Spine. 74:85–89. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Iizuka Y, Iizuka H, Tsutsumi S, et al:
Diagnosis of a previously unidentified primary site in patients
with spinal metastasis: diagnostic usefulness of laboratory
analysis, CT scanning and CT-guided biopsy. Eur Spine J.
18:1431–1435. 2009. View Article : Google Scholar
|
|
5
|
Katagiri H, Takahashi M, Inagaki J,
Sugiura H, Ito S and Iwata H: Determining the site of the primary
cancer in patients with skeletal metastasis of unknown origin: a
retrospective study. Cancer. 86:533–537. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kakhki VR, Anvari K, Sadeghi R, Mahmoudian
AS and Torabian-Kakhki M: Pattern and distribution of bone
metastases in common malignant tumors. Nucl Med Rev Cent East Eur.
16:66–69. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Bartels RH, van der Linden YM and van der
Graaf WT: Spinal extradural metastasis: review of current treatment
options. CA Cancer J Clin. 58:245–259. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Harel R and Angelov L: Spine metastases:
current treatments and future directions. Eur J Cancer.
46:2696–2707. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Sutcliffe P, Connock M, Shyangdan D, Court
R, Kandala NB and Clarke A: A systematic review of evidence on
malignant spinal metastases: natural history and technologies for
identifying patients at high risk of vertebral fracture and spinal
cord compression. Health Technol Assess. 17:1–274. 2013. View Article : Google Scholar
|
|
10
|
Oken MM, Creech RH, Tormey DC, et al:
Toxicity and response criteria of the Eastern Cooperative Oncology
Group. Am J Clin Oncol. 5:649–655. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Katagiri H, Takahashi M, Wakai K, Sugiura
H, Kataoka T and Nakanishi K: Prognostic factors and a scoring
system for patients with skeletal metastasis. J Bone Joint Surg Br.
87:698–703. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Delank KS, Wendtner C, Eich HT and Eysel
P: The treatment of spinal metastases. Dtsch Arztebl Int.
108:71–80. 2011.
|
|
13
|
Al-Brahim N, Ross C, Carter B and
Chorneyko K: The value of postmortem examination in cases of
metastasis of unknown origin - 20-year retrospective data from a
tertiary care center. Ann Diagn Pathol. 9:77–80. 2005.PubMed/NCBI
|
|
14
|
Blaszyk H, Hartmann A and Bjornsson J:
Cancer of unknown primary: clinicopathologic correlations. APMIS.
111:1089–1094. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Rougraff BT, Kneisl JS and Simon MA:
Skeletal metastases of unknown origin. A prospective study of a
diagnostic strategy. J Bone Joint Surg Am. 75:1276–1281.
1993.PubMed/NCBI
|
|
16
|
Han A, Xue J, Hu M, Zheng J and Wang X:
Clinical value of 18F-FDG PET-CT in detecting primary
tumor for patients with carcinoma of unknown primary. Cancer
Epidemiol. 36:470–475. 2012.
|
|
17
|
Ecker RD, Endo T, Wetjen NM and Krauss WE:
Diagnosis and treatment of vertebral column metastases. Mayo Clin
Proc. 80:1177–1186. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Sciubba DM, Petteys RJ, Dekutoski MB, et
al: Diagnosis and management of metastatic spine disease. A review.
J Neurosurg Spine. 13:94–108. 2010. View Article : Google Scholar
|