Introduction
African American (AA) men exhibit the highest
incidence and mortality from prostate cancer (CaP) compared to
other races in the United States (1). While socioeconomic factors contribute
to CaP outcomes among men of different ethnicities (2), it has also been recognized that AA
men have more advanced CaP at diagnosis (3). Although there remains controversy
over the role of biological differences between prostate tumors in
AA and Caucasian American (CA) men, emerging data suggest the
presence of differences in somatic and germline alterations
(4,5).
One of the most common and validated CaP genome
alterations represents fusion of the protein-coding sequences of
erythroblast transformation-specific (ETS)-related
transcription factors [predominantly ETS-related gene
(ERG)] with promoter sequences of androgen-regulated genes
[predominantly transmembrane protease serine 2 (TMPRSS2)
gene] (6–9). The highly prevalent ERG
fusions, present in over half of all CaPs in Western countries,
result in androgen-dependent and prostate tumor-specific expression
of the ERG fusion transcripts and a near-full-length ERG
protein with a 32-amino acid deletion at the amino terminus
(6–9). Evaluations of the ERG alterations at
the genomic, transcriptional and protein levels have continued to
suggest lower frequencies of ERG in AA CaP in comparison to CA CaP
(10–13). Almost complete concordance between
the detection of ERG gene fusions by fluorescence in
situ hybridization and ERG protein detection by
immunohistochemistry (IHC), has significantly accelerated the
evaluation of the ERG protein as the surrogate of this common CaP
genome alteration in pathological specimens (14–17).
Studies from our and other groups indicate that the overall
frequency of ERG alterations in CaP varies significantly among
different ethnicities: It is highest in CA, intermediate in AA and
lowest in Asian CaP patients (4,5). Our
recent evaluations of representative whole-mount prostate sections
from a matched cohort of 91 CA and 91 AA men demonstrated a
significant difference (P<0.0001) in the prevalence of the ERG
oncoprotein in index tumors of CA (63%) and AA (29%) men (13). Our preliminary data also suggested
that the majority of higher-grade tumors in AA patients may be
ERG-negative (13). The present
study focuses on comparative evaluations of ERG in higher-grade
tumors in CA and AA CaP patients.
Materials and methods
Specimens and study criteria
The Center for Prostate Disease Research database
was queried to identify CaP patients who were enrolled in the
Institutional Review Board-approved protocol from Walter Reed
National Military Medical Center. The CaP patients underwent
radical prostatectomy (RP) between 1994 and 2011. Archived
clinicopathological data were evaluated for 1,304 patients who
self-identified their race. The study sample was powered for ERG
evaluation. A total of 63 AA and 63 CA patients matched for age at
RP and Gleason scores of 8–10 and 4+3 of prostate tumors met the
study inclusion criteria.
IHC analyses of the ERG
Representative whole-mount 4-μm cross-sections from
each prostatectomy specimen were selected. The index tumor
consisting of the largest tumor with the highest grade was
identified along with all other tumor foci in each specimen.
Specimens for ERG IHC were cut and stained with a highly specific
anti-ERG monoclonal antibody (clone 9FY; Biocare Medical Inc.,
Concord, CA, USA) as previously described (13,14).
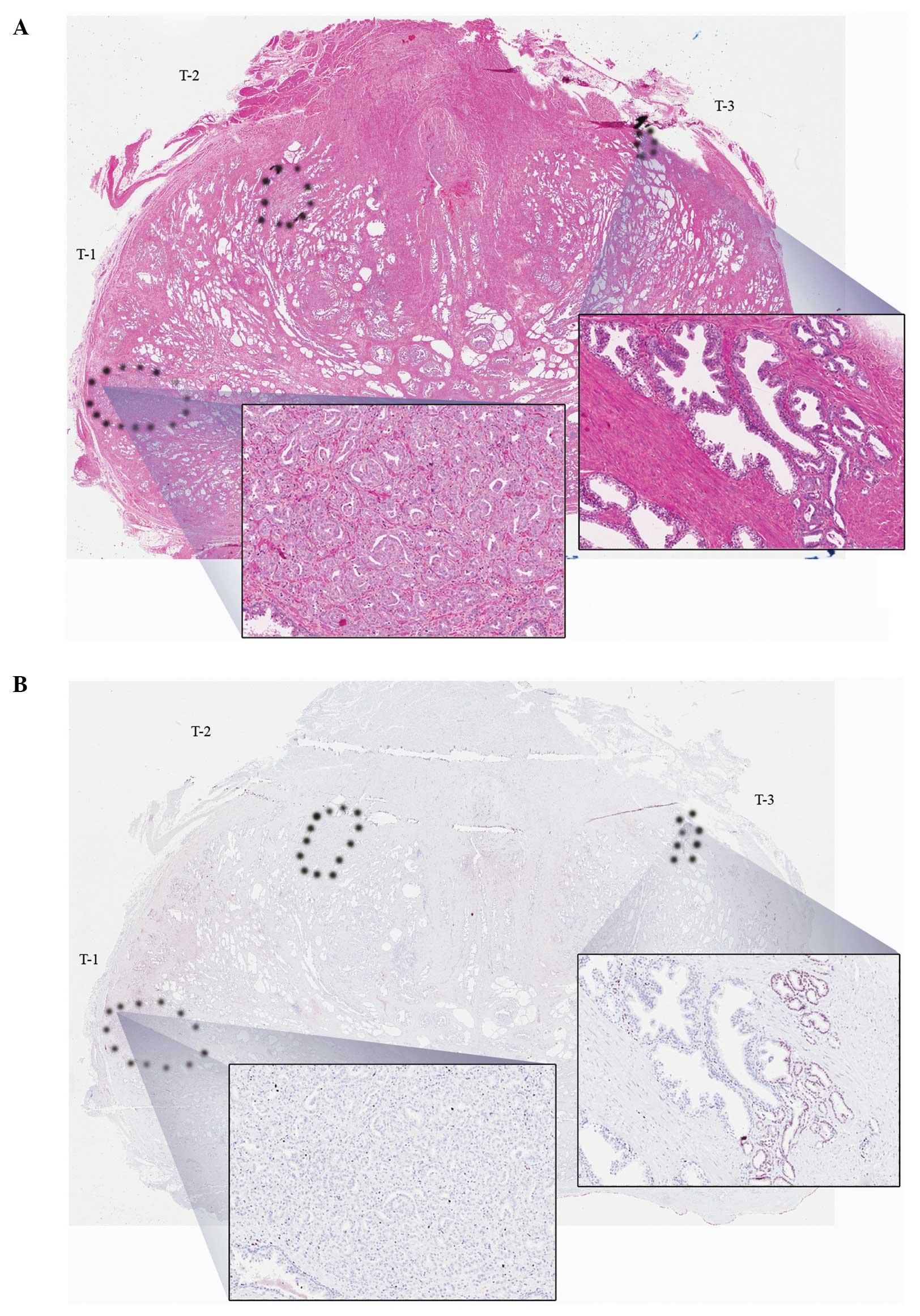
The index tumor and all other tumors were classified as
ERG-positive (any number of tumor cells positive) or negative (all
tumor cells negative). Fig. 1
provides representative examples.
Sample size and statistical analysis
Categorical patient clinicopathological data were
described across race using frequencies and percentages.
Continuously measured variables were compared using measures of
central tendency, namely mean, median and standard deviation. The
Chi-square test was used to compare the distribution of the
clinicopathological characteristics between the CA and AA cohorts,
as well as IHC status (positive vs. negative) for the AA vs. CA
cohorts. Biochemical recurrence (BCR), was defined as 2 consecutive
prostate-specific antigen (PSA) measurements of ≥0.2 ng/ml at least
8 weeks post-RP. Unadjusted Kaplan-Meier estimate curves and
multivariable Cox proportion hazards analysis were used to evaluate
the prognostic significance of ERG oncoprotein on BCR-free
survival. The log-rank test was used to test for differences in the
Kaplan-Meier curves by ERG status. P<0.05 was considered to
indicate a statistically significant difference. All data analyses
were conducted using SAS software, version 9.3 (SAS Institute,
Cary, NC, USA).
Results
Clinicopathological characteristics
The study cohort of 126 patients (63 CA and 63 AA)
did not exhibit significant differences in clinicopathological
variables across race (Table I).
The majority of the tumors had Gleason scores of 8–10 and pT3
disease (Table I). This patient
cohort provided an 80% power to detect a 25–30% absolute difference
across race for ERG positivity (two-sided P-value=0.05).
 | Table IClinicopathological characteristics of
all patients and breakdown across racial cohorts. |
Table I
Clinicopathological characteristics of
all patients and breakdown across racial cohorts.
| Variables | All (n=126) | AA (n=63) | CA (n=63) | P-value |
|---|
| Age at RP, years | | | | 0.5887 |
| Mean (SD) | 60.4 (7.1) | 60.1 (7.2) | 60.8 (7.1) | |
| PSA at diagnosis,
ng/ml | | | | 0.2718 |
| Median (range) | 6.7 (0.9–5,065) | 6.9 (1–5,065) | 6.5 (0.9–23.4) | |
| Pathological T
stage | | | | 0.2008 |
| pT2 | 49 (38.9) | 28 (44.4) | 21 (33.3) | |
| pT3 or higher | 77 (61.1) | 35 (55.6) | 42 (66.7) | |
| Gleason sum | | | | 0.8538 |
| 4+3 | 47 (37.3) | 24 (38.1) | 23 (36.5) | |
| 8–10 | 79 (62.7) | 39 (61.9) | 40 (63.5) | |
| ECE | | | | 0.6855 |
| Negative | 49 (43.0) | 26 (44.8) | 23 (41.1) | |
| Positive | 65 (57.0) | 32 (55.2) | 33 (58.9) | |
| SV | | | | 0.2496 |
| Negative | 91 (72.8) | 48 (77.4) | 43 (68.2) | |
| Positive | 34 (27.2) | 14 (22.6) | 20 (31.8) | |
| Margin status | | | | 0.3230 |
| Negative | 83 (69.2) | 44 (73.3) | 39 (65.0) | |
| Positive | 37 (30.8) | 16 (26.7) | 21 (35.0) | |
ERG status by race and grade
Overall, 46% of the patients had ≥1 ERG-positive
tumor foci. The index tumor was ERG-positive in 41 of the 126
patients. In CA men, the index tumor was ERG-positive in 31 of 63
patients (49%), which was significantly higher compared to 10 of 63
patients (16%) in AA men (P<0.0001) (Table II). CA men were also significantly
more likely to have any tumor focus positive for ERG compared to AA
men (59 vs. 41%, P=0.0042, data not shown). ERG-positive status was
significantly lower in higher-grade (16%) compared to lower-grade
(34%) index tumors of AA men (P=0.04), which was not the case in CA
men (Table II).
| Table IIPrevalence of ERG positivity across
race in high-grade (Gleason score, 8–10 and 4+3) index tumors
(upper lane, present study) and in low-grade (Gleason score, 6)
index tumors (lower lane). |
Table II
Prevalence of ERG positivity across
race in high-grade (Gleason score, 8–10 and 4+3) index tumors
(upper lane, present study) and in low-grade (Gleason score, 6)
index tumors (lower lane).
| ERG status/grade | Total | CA | AA | P-value |
|---|
| ERG+/high-grade | 33% (41/126) | 49% (31/63) | 16% (10/63) | <0.0001 |
|
ERG+/low-gradea | 52% (35/67) | 69% (24/35) | 34% (11/32) | 0.0051 |
| P-value | | 0.0642 | 0.0400 | |
ERG as a predictor of recurrence
ERG was not found to be an independent predictor of
BCR in this cohort (Table III).
Pathological stage was an independent predictor of BCR [hazard
ratio (HR)=5.749, P=0.0043] and there was a trend towards higher
serum PSA levels at diagnosis (HR=1.289, P=0.0564) (Table III).
| Table IIIUnivariable and multivariable Cox
proportional hazard models for the prediction of biochemical
recurrence by using ERG IHC status and clinicopathological
variables. |
Table III
Univariable and multivariable Cox
proportional hazard models for the prediction of biochemical
recurrence by using ERG IHC status and clinicopathological
variables.
| Univariable Cox
models | Multivariable Cox
model |
|---|
|
|
|
|---|
| Variables | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age at RP | 1.011
(0.965–1.059) | 0.6481 | | |
| Log PSA | 1.352
(1.062–1.723) | 0.0145 | 1.289
(0.993–1.674) | 0.0564 |
| Race/ethnicity |
| CA | 1 | | | |
| AA | 0.705
(0.371–1.340) | 0.2866 | | |
| Pathological T
stage |
| pT2 | 1 | | 1 | |
| pT3 or higher | 4.737
(1.972–11.379) | 0.0005 | 5.749
(1.729–19.115) | 0.0043 |
| Gleason sum |
| 4+3 | 1 | | 1 | |
| 8–10 | 1.858
(0.879–3.928) | 0.1048 | 1.272
(0.545–2.968) | 0.5777 |
| SV |
| Negative | 1 | | 1 | |
| Positive | 2.240
(1.183–4.241) | 0.0133 | 1.159
(0.571–2.354) | 0.6827 |
| Margin status |
| Negative | 1 | | 1 | |
| Positive | 2.276
(1.193–4.342) | 0.0126 | 0.890
(0.427–1.855) | 0.7562 |
| ERG IHC status |
| ERG− | 1 | | | |
| ERG+ | 1.366
(0.704–2.652) | 0.3564 | | |
Discussion
CaP is a multifocal, heterogeneous disease with a
variable clinical course. Two cancers of the same grade and stage
do not necessarily exhibit similar progression characteristics and
CaP does not behave equally across age groups or ethnicities
(1–5,18).
Molecular alterations are likely involved in the ethnic differences
of CaP and we sought to describe the prevalence of ERG in
higher-grade disease in AA and CA men with a focus on index tumors.
High Gleason scores are recognized as surrogates of aggressive
disease and are independently predictive of BCR (19).
Studies from our and other groups have demonstrated
significantly lower frequencies of ERG in CaP of AA men in
comparison to that of CA men (5,12,13).
Our previous preliminary observation indicated more significant
differences in ERG in high-grade tumors of AA compared to those of
CA men. This adequately powered study addressed this issue by using
matched cohorts of CA and AA CaP specimens. A striking finding of
this study was that ERG was significantly (3 times) more likely to
be present in the higher-grade index tumors of CA men compared to
those of AA men (31 of 63 vs. 10 of 63 patients, respectively;
P<0.0001). Thus, although ERG may be the most common oncogenic
alteration in CA men, it does not appear to be the case in AA men,
particularly not in those with higher-grade CaP. The biological
basis underlying this observation remains to be elucidated; these
results nonetheless support the association of an ERG-negative
status with more aggressive disease in AA men. These data also
suggest that ERG may not be the primary driver of higher-grade CaP
in AA men.
While there is a general agreement that ERG
is a highly prevalent and early oncogenic alteration in CaP and it
defines a large subtype of prostate tumors, it is also important to
recognize that there are significant proportions of ERG-negative
prostate tumors for which a common driver gene alteration is not
known. Emerging data from the present and other studies underscore
the higher prevalence of the ERG-negative subtype of CaP in AA and
Asian men (4,5). The higher frequency of high-grade
ERG-negative tumors in AA men likely reflects the presence of
distinct genomic alterations associated with the initiation and
progression of this subtype of CaP.
The utility of ERG detection in CaP is apparent in
the diagnostic setting and ERG typing of tumors may also be of
significant value for biological classification and future targeted
therapy. However, the utility of ERG in assessing CaP progression
remains controversial, which may be attributed to multifactorial
causes, including specific patient cohort, disease stage and assay
type (8,17). In this high-grade cohort, the ERG
protein status was not found to be correlated with disease
progression.
In summary, this study provides important
observations on the predominance of ERG-negative high-grade CaP in
AA men. The biological implications of these observations are
far-reaching, particularly in delineating biological typing and
future treatment of CaP tumors in men of different ethnicities.
Acknowledgements
The views expressed in this review do not reflect
any official policy of the Department of the Army, Department of
Defense, or the US Government. We wish to thank Mr. Stephen Doyle
for the artwork.
References
|
1
|
Siegel R, Naishadham D and Jemal A: Cancer
statistics, 2013. CA Cancer J Clin. 63:11–30. 2013. View Article : Google Scholar
|
|
2
|
Schwartz K, Powell IJ, Underwood W III, et
al: Interplay of race, socioeconomic status and treatment on
survival of patients with prostate cancer. Urology. 74:1296–1302.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Williams H and Powell IJ: Epidemiology,
pathology and genetics of prostate cancer among African Americans
compared with other ethnicities. Methods Mol Biol. 472:439–453.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Martin DN, Starks AM and Ambs S:
Biological determinants of health disparities in prostate cancer.
Curr Opin Oncol. 25:235–241. 2013.PubMed/NCBI
|
|
5
|
Farrell J, Petrovics G, McLeod DG and
Srivastava S: Genetic and molecular differences in prostate
carcinogenesis between African American and Caucasian American men.
Int J Mol Sci. 14:15510–15531. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tomlins SA, Rhodes DR, Perner S, et al:
Recurrent fusion of TMPRSS2 and ETS transcription factor genes in
prostate cancer. Science. 310:644–648. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Petrovics G, Liu A, Shaheduzzaman S, et
al: Frequent overexpression of ETS-related gene-1 (ERG1) in
prostate cancer transcriptome. Oncogene. 24:3847–3852. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Rubin MA, Maher CA and Chinnaiyan AM:
Common gene rearrangements in prostate cancer. J Clin Oncol.
29:3659–3668. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Barbieri CE, Bangma CH, Bjartell A, et al:
The mutational landscape of prostate cancer. Eur Urol. 64:567–576.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hu Y, Dobi A, Sreenath T, et al:
Delineation of TMPRSS2-ERG splice variants in prostate cancer. Clin
Cancer Res. 14:4719–4725. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Rice KR, Chen Y, Ali A, et al: Evaluation
of the ETS-related gene mRNA in urine for the detection of prostate
cancer. Clin Cancer Res. 16:1572–1576. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Magi-Galluzzi C, Tsusuki T, Elson P, et
al: TMPRSS2-ERG gene fusion prevalence and class are significantly
different in prostate cancer of Caucasian, African-American and
Japanese patients. Prostate. 71:489–497. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Rosen P, Pfister D, Young D, et al:
Differences in frequency of ERG oncoprotein expression between
index tumors of Caucasian and African American patients with
prostate cancer. Urology. 80:749–753. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Furusato B, Tan SH, Young D, et al: ERG
oncoprotein expression in prostate cancer: clonal progression of
ERG-positive tumor cells and potential for ERG-based
stratification. Prostate Cancer Prostatic Dis. 13:228–237. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Park K, Tomlins SA, Mudaliar KM, et al:
Antibody-based detection of ERG rearrangement-positive prostate
cancer. Neoplasia. 12:590–598. 2010.PubMed/NCBI
|
|
16
|
Braun M, Goltz D, Shaikhibrahim Z, et al:
ERG protein expression and genomic rearrangement status in primary
and metastatic prostate cancer - a comparative study of two
monoclonal antibodies. Prostate Cancer Prostatic Dis. 15:165–169.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Rosen P, Sesterhenn IA, Brassell SA, et
al: Clinical potential of the ERG oncoprotein in prostate cancer.
Nat Rev Urol. 9:131–137. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Brassell SA, Rice KR, Parker PM, et al:
Prostate cancer in men 70 years old or older, indolent or
aggressive: clinicopathological analysis and outcomes. J Urol.
185:132–137. 2011.PubMed/NCBI
|
|
19
|
Brimo F, Montironi R, Egevad L, et al:
Contemporary grading for prostate cancer: implications for patient
care. Eur Urol. 63:892–901. 2013. View Article : Google Scholar : PubMed/NCBI
|