Introduction
Hepatocellular carcinoma (HCC) is the sixth most
prevalent cancer, the third most frequent cause of cancer-related
mortality and the leading cause of mortality among patients with
cirrhosis (1). Chronic hepatitis B
virus (HBV) and hepatitis C virus (HCV) infection are the most
significant causes of HCC. HCCs spread via the hematogenous route,
the lymphatic route, or by direct invasion into adjacent organs
(2). Metastasis is not rare among
patients with HCC and has increased in prevalence over the last
decade (3). HCCs may exhibit
multiple intrahepatic occurrences and intrahepatic metastasis,
whereas extrahepatic metastasis occurs in 30–50% of the patients
(4). The most common site of
extrahepatic metastasis of HCC is the lungs, followed by lymph
nodes and bones (3, 4). Although HCC may metastasize to
various extrahepatic organs, metastases with cardiac involvement
are rare (5–19). The majority of the cardiac
metastases are direct and contiguous extensions of the intrahepatic
HCC via the inferior vena cava into the right atrium (16), whereas isolated metastases in the
left atrium that are discontinuous with an intrahepatic HCC are
extremely rare (5, 6, 9,
12). This is the case report of a
46-year-old Japanese man with isolated left atrial metastases from
HCC and a review of published reports, treatments and prognoses in
similar cases. Written informed consent was obtained from the
patient's relatives.
Case report
A 46-year-old Japanese man was referred to our
institution for the treatment of progressive breathlessness and
persistent cough over the past 3 months. Two years prior to this
visit, the patient had undergone a curative operation for HCC
secondary to chronic HBV infection. The patient's blood biochemical
values demonstrated elevated levels of serum α -fetoprotein (AFP)
and protein induced by vitamin K absence or antagonist-II
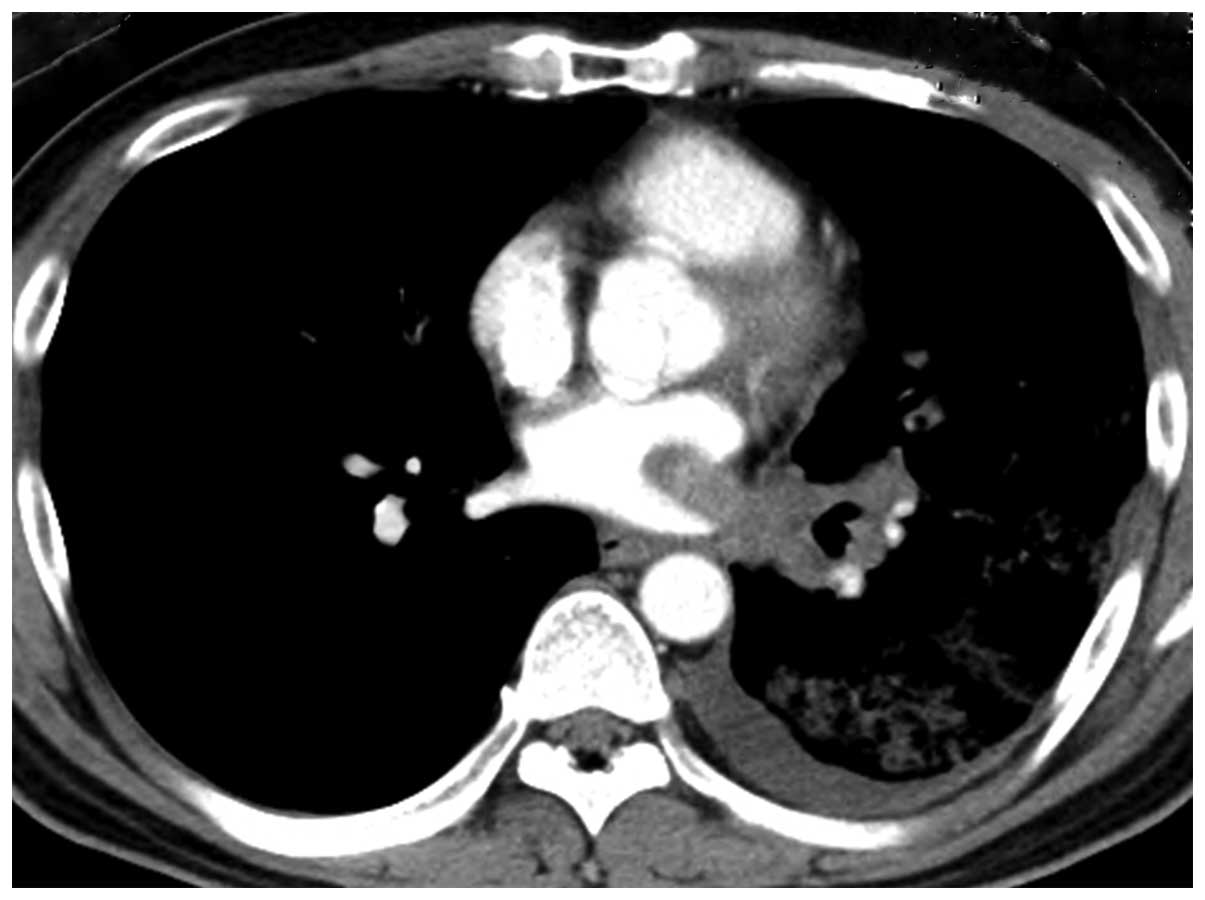
(PIVKA-II). A contrast-enhanced computed tomography (CT) scan of
the patient's chest revealed a tumor extending from the left lower
lobe bronchus into the left atrium via the pulmonary vein (Fig. 1). A positron emission tomography
scan with18F-fluorodeoxyglucose (18F-FDG)
showed increased FDG uptake, with a maximum standardized uptake
value of 5.1 in the tumor. There was no abnormal accumulation of
FDG in the liver.
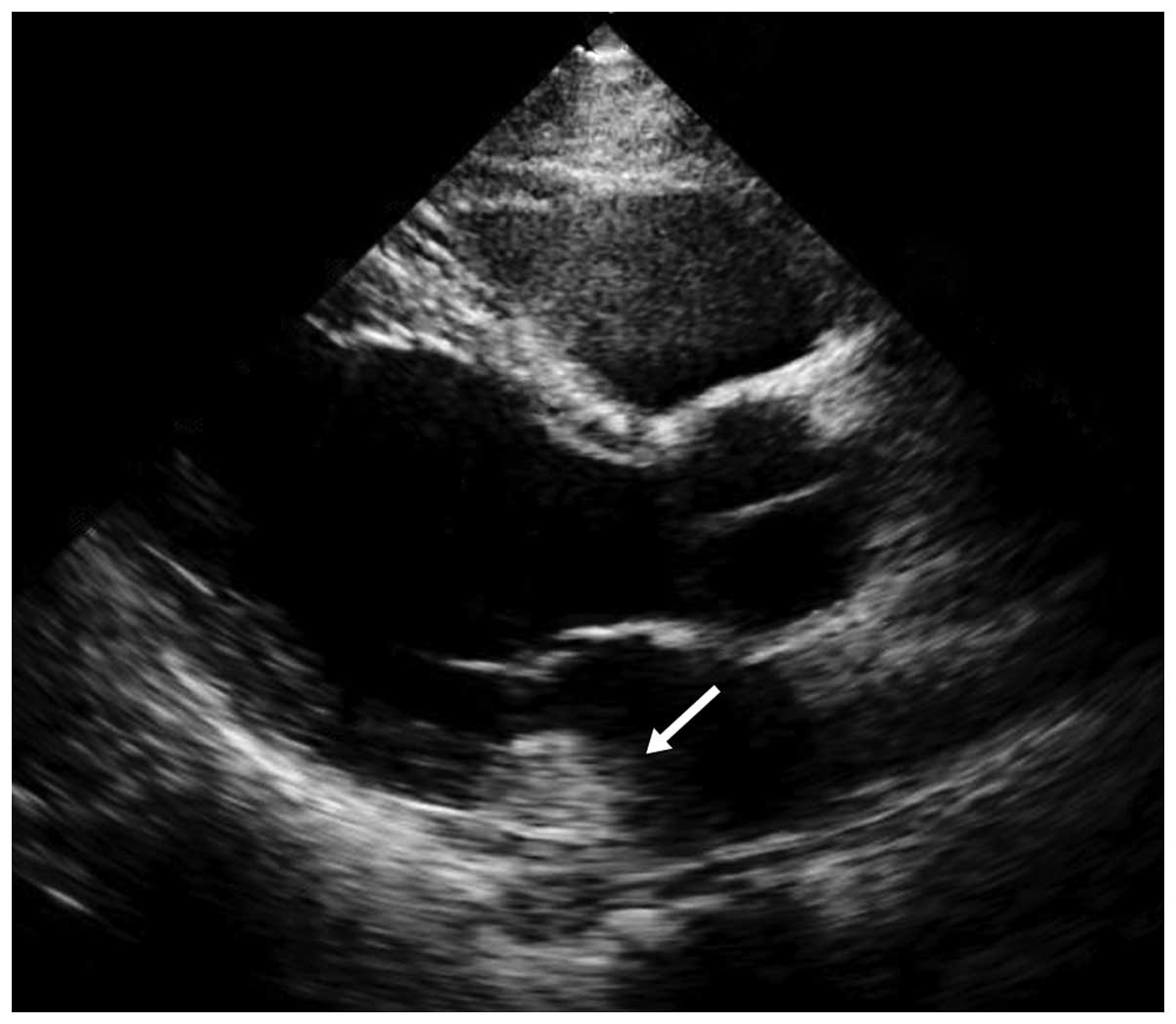
A transthoracic echocardiography image revealed a
round mass-like lesion in the left atrium (Fig. 2). An endobronchial
ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) was
performed, targeting the submucosal lesion in the left lower lobe
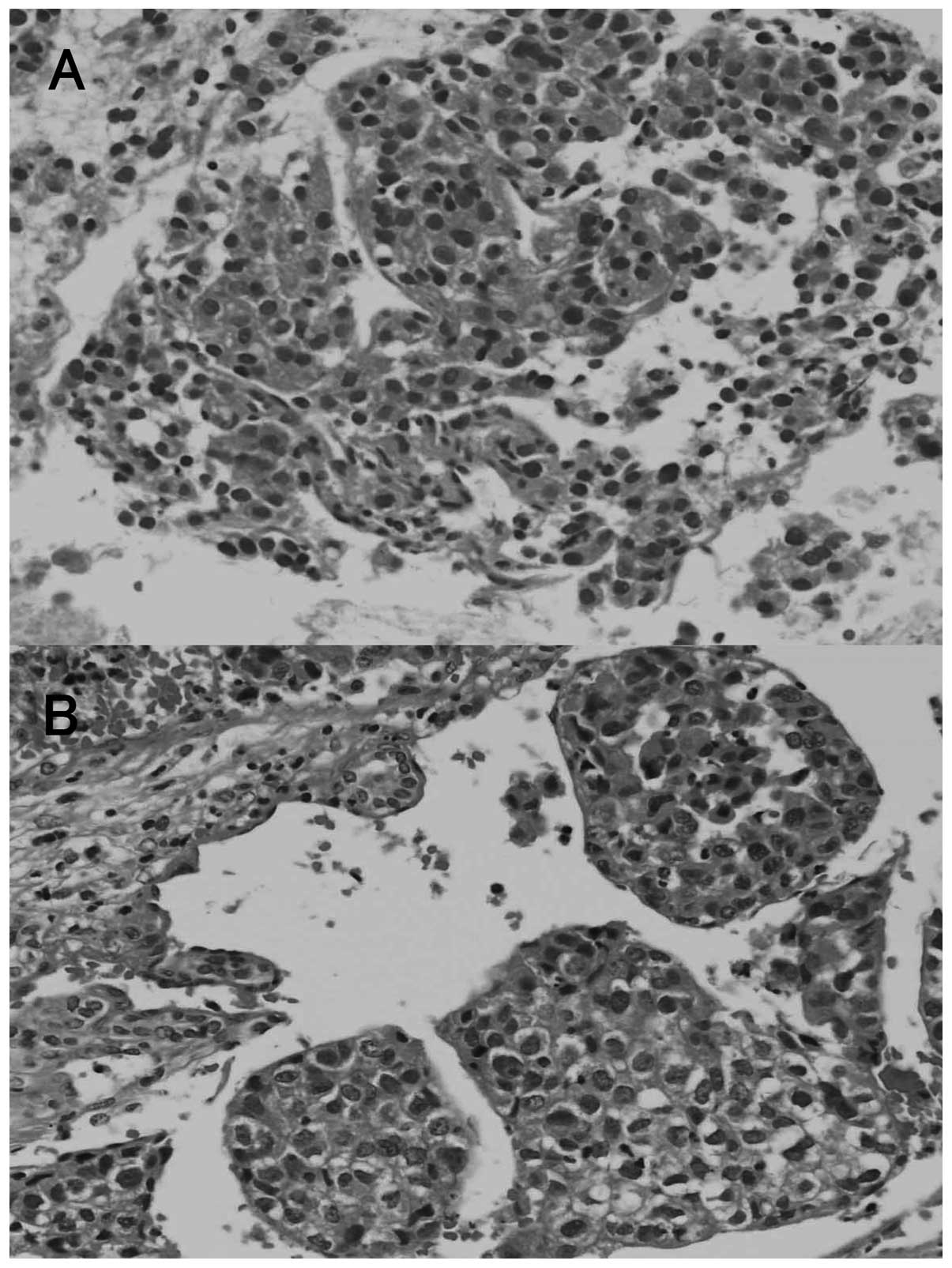
bronchus. The microscopic findings of the specimens obtained by
EBUS-TBNA demonstrated polygonal tumor cells with centrally located
round nuclei arranged in a predominantly trabecular pattern
(Fig. 3A). The tumor was
compatible with metastatic HCC, as the cytopathological
characteristics of the tumor cells were identical to those of the
previously resected HCC, with moderate differentiation (Fig. 3B). Subsequently, oral sorafenib
therapy was initiated at the dose of 400 mg/day in the outpatient
setting. Two weeks after the initiation of sorafenib treatment, the
patient was admitted to our institution with nausea, vomiting and
weakness of the right upper limb. A contrast CT scan of the brain
revealed a metastatic brain tumor in the left parietal cerebral
lobe with an intracranial hemorrhage. The patient underwent gamma
knife radiosurgery for the metastatic brain tumor, following
control of the intracranial hemorrhage by conservative treatment
and discontinuation of sorafenib. However, the patient's condition
gradually deteriorated and he succumbed to multiple organ failure 4
months later.
Discussion
To the best of our knowledge, this is the first
reported case of isolated metastases of HCC to the left atrium
treated with sorafenib. Metastases of HCC tend to spread through
the intrahepatic vessels, the lymphatic system, or by direct
invasion. HCC has a marked propensity for vascular invasion and
extension. Hematogenous spread may result from the involvement of
the portal vein, hepatic veins, or inferior vena cava (18). Although HCC may metastasize to
various extrahepatic organs, metastases with cardiac involvement
are rare (12). The majority of
cardiac metastases are direct and contiguous extensions of the
intrahepatic HCC via the inferior vena cava into the right atrium
(16).
In an antemortem series, the incidence of metastatic
HCC to the right heart cavity with extension via the inferior vena
cava was reported to be <6% (5). Isolated cardiac metastases that are
discontinuous with an intrahepatic HCC are extremely rare; to the
best of our knowledge, a total of 18 cases with isolated cardiac
metastases from HCC have been reported to date (14, 16). In those cases, the majority of
metastases were located in the right side of the heart, while
metastases in the left atrium were observed in only 2 patients. The
involvement of the left atrium is possibly associated with tumor
growth from the pulmonary veins following metastasis to the lung,
direct invasion of the atrial septum, or tumor implantation via a
subclinical right-to-left shunt through a patent foramen ovale.
In the present case, the lung metastases of HCC may
be considered to be the origin of the patient's metastatic tumor in
the left atrium. It is hypothesized that the tumor cells
hematogenously spread from the tumor located in the lung via the
pulmonary veins directly into the left atrium, as the
echocardiography and CT scan did not reveal a patent foramen ovale
or other cardiac defect.
The risk of cardiopulmonary collapse is high in
patients with cardiac involvement. Possible cardiopulmonary
complications include heart failure, tricuspid stenosis or
insufficiency, ventricular outflow tract obstruction, sudden
cardiac death, secondary Budd-Chiari syndrome, pulmonary embolism
and pulmonary metastasis (19).
Acute severe complications, including cerebral infarction,
peripheral arterial occlusion and syncopal attack have also been
reported, as left atrial masses may give rise to widespread emboli
(20). In the present case, the
tumor cells in the left atrium may have spread hematogenously to
the brain via the systemic circulation, resulting in tumor emboli
and a cerebral hemorrhage. Brain metastases from HCC are extremely
rare, with a reported frequency ranging from 0.2 to 2.2% at
autopsy, and they are frequently associated with hemorrhage
(21). In general, the
hypervascularity of HCCs and the underlying coagulopathy due to
liver cirrhosis may account for cerebral hemorrhage (21).
Multidisciplinary treatments to control the growth
of HCC offer patients with cardiac involvement a potentially
curative option. Surgical and non-surgical approaches, including
transcatheter arterial embolization and transcatheter arterial
infusion chemotherapy, have been undertaken to treat patients with
isolated cardiac metastases from HCC (14, 16). However, such therapeutic modalities
may not be feasible, particularly if the patient has a poor general
status, metastatic disease, or underlying hepatic dysfunction
(17). Until recently, no
effective treatment was available for HCC patients diagnosed at an
advanced stage, or who progressed to an advanced stage following
failure of other treatments (1).
Several molecular-targeted agents are currently
under development, but the only one with proven survival benefit is
sorafenib (1). This agent, which
may be administered orally, is a multikinase inhibitor that blocks
Raf signaling and vascular endothelial growth factor (VEGF),
platelet-derived growth factor (PDGF) and c-Kit (1). Recent studies have established
sorafenib as the standard of care for advanced HCC (1). Since an aggressive surgical resection
of the tumor was not feasible for our patient due to the advanced
stage of the HCC, treatment with sorafenib was initiated to prolong
his survival. However, sorafenib was ineffective and provided no
survival benefit in this case. It is possible that the growth
mechanisms of this tumor do not depend on Raf, VEGF, PDGF or c-Kit
signaling, but rather on an alternative signal transduction
pathway, resulting in failure of sorafenib treatment.
The prognosis of HCC with cardiac involvement is
poor (14, 16, 17). The reported median survival time
from the time of diagnosis of cardiac metastasis was 102 days
(17). The most common cause of
death is usually associated with the HCC per se or the
underlying liver disease; only a few patients reportedly succumb to
cardiac metastases (17).
In conclusion, we treated a patient with HCC and
isolated metastases in the left atrium. Isolated metastases in the
left atrium that are discontinuous with an intrahepatic HCC are
extremely rare. Given the severe complications that have been
reported in patients with this type of metastasis, immediate
multidisciplinary treatment, including surgical resection, should
be considered.
References
|
1
|
Forner A, Llovet JM and Bruix J:
Hepatocellular carcinoma. Lancet. 379:1245–1255. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Becker AK, Tso DK, Harris AC, Malfair D
and Chang SD: Extrahepatic metastases of hepatocellular carcinoma:
a spectrum of imaging findings. Can Assoc Radiol J. 65:60–66. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Abbas A, Medvedev S, Shores N, et al:
Epidemiology of metastatic hepatocellular carcinoma, A Nationwide
Perspective. Dig Dis Sci. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Terada T and Maruo H: Unusual extrahepatic
metastatic sites from hepatocellular carcinoma. Int J Clin Exp
Pathol. 6:816–820. 2013.PubMed/NCBI
|
|
5
|
Lei MH, Ko YL, Kuan P, Lien WP and Chen
DS: Metastasis of hepatocellular carcinoma to the heart: unusual
patterns in three cases with antemortem diagnosis. J Formos Med
Assoc. 91:457–461. 1992.PubMed/NCBI
|
|
6
|
Barasch E, Frazier OH, Silberman H,
Shannon RL and Wilansky S: Left atrial metastasis from
hepatocellular carcinoma: a case report. J Am Soc Echocardiogr.
7:547–549. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Masci G, Magagnoli M, Grimaldi A, et al:
Metastasis of hepatocellular carcinoma to the heart: a case report
and review of the literature. Tumori. 90:345–347. 2004.PubMed/NCBI
|
|
8
|
Longo R, Mocini D, Santini M, et al:
Unusual sites of metastatic malignancy: case 1. Cardiac metastasis
in hepatocellular carcinoma. J Clin Oncol. 22:5012–5014. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Nam SW, Baek JT, Kang SB, et al: A case of
the hepatocellular carcinoma during the pregnancy and metastasis to
the left atrium. Korean J Hepatol. 11:381–385. 2005.PubMed/NCBI
|
|
10
|
Agelopoulou P, Kapatais A, Varounis C, et
al: Hepatocellular carcinoma with invasion into the right atrium.
Report of two cases and review of the literature.
Hepatogastroenterology. 54:2106–2108. 2007.PubMed/NCBI
|
|
11
|
Leo F, Rapisarda F, Stefano PL and
Batignani G: Cavo-atrial thrombectomy combined with left
hemi-hepatectomy for vascular invasion from hepatocellular
carcinoma on diseased liver under hypothermic cardio-circulatory
arrest. Interact Cardiovasc Thorac Surg. 10:473–475. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Jeong DS, Kim JS, Kim KH and Ahn H: Left
atrial metastasis from hepatocellular carcinoma with liver
cirrhosis. Interact Cardiovasc Thorac Surg. 11:703–705. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Inoue Y, Hayashi M, Katsumata T, Shibayama
Y and Tanigawa N: Hepatocellular carcinoma with right atrial tumor
thrombus: report of a case. Surg Today. 41:1122–1129. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Tastekin E, Usta U, Ege T, Kazindir G and
Kutlu AK: Cardiac metastasis of hepatocellular carcinoma in a young
non-cirrhotic patient, to the left ventricle. Ann Hepatol.
11:392–394. 2012.PubMed/NCBI
|
|
15
|
Li SS, Jian LL, Gang PB, Ando KM and Ming
LD: Removal of hepatocellular carcinoma extending into the right
atrium with extracorporeal circulation. Hepatogastroenterology.
59:1591–1593. 2012.PubMed/NCBI
|
|
16
|
Kawakami M, Koda M, Mandai M, et al:
Isolated metastases of hepatocellular carcinoma in the right
atrium: case report and review of the literature. Oncol Lett.
5:1505–1508. 2013.PubMed/NCBI
|
|
17
|
Albackr HB: A large right atrial mass in a
patient with hepatocellular carcinoma: case report and literature
review. J Saudi Heart Assoc. 26:174–178. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Liu YC, Ho YL, Huang GT, Chen DS, Sheu JC
and Chen CH: Clinical manifestations and survival of patients with
hepatocellular carcinoma and cardiac metastasis. J Gastroenterol
Hepatol. 25:150–155. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Sung AD, Cheng S, Moslehi J, Scully EP,
Prior JM and Loscalzo J: Hepatocellular carcinoma with
intracavitary cardiac involvement: a case report and review of the
literature. Am J Cardiol. 102:643–645. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Funakoshi Y, Mukohara T, Kataoka T, et al:
Left atrial extension of metastatic lung tumor via pulmonary vein:
report on the first case of Ewing sarcoma. Rare Tumors. 2:e532010.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Jiang XB, Ke C, Zhang GH, et al: Brain
metastases from hepatocellular carcinoma: clinical features and
prognostic factors. BMC Cancer. 12:492012. View Article : Google Scholar : PubMed/NCBI
|