Introduction
Hepatocellular carcinoma (HCC) is one of the most
prevalent tumor types worldwide (1).
In Asia, resection of HCC remains the predominant treatment for
potentially curable diseases. Even in patients with huge HCC, it is
possible to obtain long-term survival for the well-selected subsets
of patients following surgical resection (2). However, prognosis of patients with HCC
who undergo resection differs substantially and large variation is
predominantly unexplained. Therefore, the risk factors for
postoperative survival prediction in patients with HCC have been
intensively studied (3,4). Nevertheless, the clinical outcomes for
patients with HCC with identical clinicopathological
characteristics are heterogeneous (5). Owing to the limitations of current
staging systems and advances in the understanding of the biology of
HCC, molecular alterations can complement clinical variables in
staging systems and guide therapeutic decision-making (6). Unfortunately, evaluating molecular
markers requires extra time and effort, as well as increased cost.
Therefore, routine laboratory assessments, including γ-glutamyl
transpeptidase (GGT) (7), monocyte
count (8), platelet count (9) and neutrophil-to-lymphocyte ratio
(10) have been developed to be
predictive factors for survival in HCC.
Hypoxia appears to be an influencing factor for
numerous cancer types, and anemia has been suggested to be
associated with tumor hypoxia (11).
Previously, evidence has indicated that anemia is correlated with
poor clinical prognosis in several cancer types (12–15). In
addition, in HCC, a previous report demonstrated the prognostic
impact of hemoglobin (HGB) levels prior to treatment (16). The mean corpuscular hemoglobin (MCH),
which refers to a measurement of the average HGB content of each
red blood cell, is another anemia associated factor, which reflects
iron metabolism. Abnormalities in iron metabolism are known to be
crucial in cancer progression (17,18).
Despite this evidence, the added value of these two markers in
predicting long-term overall survival (OS) for HCC remains to be
elucidated. On the basis of these considerations, the present study
assessed the ability of using the levels of HGB and MCH for
long-term prognosis prediction of patients with HCC resection.
Patients and methods
Study population
All patients (n=445) with HCC between January 1987
and December 1994 underwent hepatic resection of HCC by the
identical surgical team at the Department of Hepatobiliary
Oncology, Sun Yat-Sen University Cancer Center (Guangdong, China).
The diagnosis of HCC and underlying liver disease was confirmed in
all patients by histological examination. Of these 445 cases, 399
had complete clinicopathological and follow-up data, however, had
not received any preoperative treatments, including trans-hepatic
arterial chemoembolization, radiotherapy or chemotherapy. The
clinicopathological variables are shown in Table I. All blood samples were obtained 3
days prior to the operation. Tumor size was based on gross
examination, as documented in the operation records, hepatitis B
history was defined as a history with positive serum hepatitis B
surface antigen (HBsAg), tumor encapsulation was defined that
presence of a clear fibrous sheath around the tumor at gross
inspection, tumor differentiation was based on the
Edmondson-Steiner classification, and tumor number and macroscopic
venous invasion were determined by the surgeon at the time of
resection. The tumors were pathologically staged using the
7th edition of the American Joint Committee on Cancer
staging system (19). All recruited
patients provided written informed consent prior to examination and
treatment. The study protocol was approved by the Ethics Committee
of Sun Yat-Sen University Cancer Center and conformed to the
ethical guidelines of the Helsinki Declaration.
 | Table I.HGB and MCH levels in relation to the
clinicopathalogical variables in 399 patients with HCC. |
Table I.
HGB and MCH levels in relation to the
clinicopathalogical variables in 399 patients with HCC.
|
|
| HGB | MCH |
|---|
|
|
|
|
|
|---|
| Variable | No. cases | ≤110 g/l n (%)
(n=51) | >110 g/l n (%)
(n=348) | P-value | ≤27 pg n (%)
(n=88) | >27 pg n (%)
(n=311) | P-value |
|---|
| Age, years |
|
|
|
|
|
|
|
|
≤48 | 207 | 30
(14.5) | 177 (85.5) | 0.288 | 48 (23.2) | 159 (76.8) | 0.571 |
|
>48 | 192 | 21
(10.9) | 171 (89.1) |
| 40 (20.8) | 152 (79.2) |
|
| Gender |
|
|
|
|
|
|
|
|
Female | 43 | 10 (23.3) | 33 (76.7) | 0.029 | 16 (37.2) | 27 (62.8) | 0.011 |
|
Male | 356 | 41 (11.5) | 315 (88.5) |
| 72 (20.2) | 284 (79.8) |
|
| HBsAg |
|
|
|
|
|
|
|
|
Negative | 80 | 13
(16.3) | 67 (83.7) | 0.299 | 24 (30.0) | 56 (70.0) | 0.055 |
|
Positive | 319 | 38
(11.4) | 281 (88.6) |
| 64 (20.1) | 255 (79.9) |
|
| Cirrhosis |
|
|
|
|
|
|
|
| No | 86 | 10
(11.6) | 76 (88.4) | 0.717 | 23 (26.7) | 63 (73.3) | 0.236 |
|
Yes | 313 | 41
(13.1) | 272 (86.9) |
| 65 (20.8) | 248 (79.2) |
|
| Tumor size |
|
|
|
|
|
|
|
|
<10 | 272 | 34
(12.5) | 238 (87.5) | 0.805 | 61 (22.4) | 211 (77.6) | 0.793 |
|
≥10 | 127 | 17
(13.4) | 110 (86.6) |
| 27 (21.3) | 100 (78.7) |
|
| Tumor
encapsulation |
|
|
|
|
|
|
Complete | 193 | 22
(11.4) | 171 (88.6) | 0.423 | 33 (17.1) | 160 (82.9) | 0.021 |
|
None | 206 | 29
(14.1) | 177 (85.9) |
| 55 (26.7) | 151(73.3) |
|
| Tumor number |
|
|
|
|
|
|
|
|
Solitary | 259 | 34
(13.1) | 225 (86.9) | 0.779 | 57 (22.0) | 202 (78.0) | 0.975 |
|
Multiple | 140 | 17
(12.1) | 123 (87.9) |
| 31 (22.1) | 109 (77.9) |
|
| Vascular
invasion |
|
|
|
|
|
|
|
|
Absent | 326 | 42
(12.9) | 284 (87.1) | 0.898 | 75 (23.0) | 251 (77.0) | 0.333 |
|
Present | 73 | 9
(12.3) | 64 (87.7) |
| 13 (17.8) | 60 (82.2) |
|
|
Differentiation |
|
|
|
|
|
|
|
|
I–II | 285 | 34
(11.9) | 251 (88.1) | 0.420 | 65 (22.8) | 220 (77.2) | 0.567 |
|
III–IV | 114 | 17
(14.9) | 97 (85.1) |
| 23 (20.2) | 91 (79.8) |
|
| TNM stage |
|
|
|
|
|
|
|
| I | 225 | 32
(14.2) | 193 (85.8) | 0.327 | 49 (21.8) | 176 (78.2) | 0.879 |
|
II–III | 174 | 19
(10.9) | 155 (89.1) |
| 39 (22.4) | 135 (77.6) |
|
| AFP, µg/l |
|
|
|
|
|
|
|
|
≤25 | 127 | 21
(16.5) | 106 (83.5) | 0.125 | 30 (23.6) | 97 (76.4) | 0.606 |
|
>25 | 272 | 30
(11.0) | 242 (89.0) |
| 58 (21.3) | 214 (78.7) |
|
Tumor-associated anemia was defined as a HGB ≤110
g/l without acute blood loss (20).
MCH ≤27 pg (normal range, 27–32 pg) was used, since the decreased
preoperative MCH level reflected low quantities of HGB per red
blood cell.
Follow-up
Postoperative mortality was defined as all
mortalities within 30 days of surgery or during the same hospital
stay following liver resection. Following discharge, all patients
were followed up regularly at the outpatient clinic, more that once
every 3 months in the first year and every 3–6 months thereafter.
The follow-up included a clinical examination, liver function
tests, serum α-fetoprotein (AFP) level, chest X-ray and abdomen
ultrasonography. Computed tomography and/or magnetic resonance
imaging were performed when intrahepatic recurrence or distant
metastasis were suspected. The present study was censored on July
30th 2011. The median follow-up was 26 months (range,
1–269 months).
Statistical analysis
Descriptive statistics are expressed as the mean ±
standard deviation. The Chi-square test or Fisher's exact test,
where appropriate, were used for univariate comparisons. The
postoperative mortality was included when calculating the OS, using
the Kaplan-Meier method. Cox's proportional hazard model was used
for univariate and multivariate analyses of prognostic factors.
P<0.05 was considered to indicate a statistically significant
difference. All statistical analyses were performed using SPSS
statistical software package version 16.0 (SPSS, Inc., Chicago, IL,
USA).
Results
Correlations of clinicopathological
variables with HGB and MCH
The mean serum levels of HGB and MCH were
137.40±20.53 g/l and 30.31±5.30 pg, respectively. These two
continuous variables were positively associated with each other
(r=0.296, P<0.001; Data not shown). However, when they were
dichotomized, according to the corresponding cut-off points,
certain patients possessed high HGB and contrarily low MCH (n=49).
As shown in Table I, 51 (12.8%)
patients had preoperative HGB ≤110 g/l. Low HGB level was only
associated with female patients (P=0.029) and low MCH level was
associated with female patients (P=0.011) and incomplete
encapsulation (P=0.021).
Long-term outcome for patients with
HCC following hepatic resection
A total of 327 mortalities were recorded until the
final follow-up, of which six were hospital mortalities within 30
days of surgery. The majority of the remaining mortalities were due
to tumor recurrence. A total of 74 patients in the cohort survived
>10 years. The OS rates following hepatectomy at 5, 10 and 15
years were 32.5, 21.9 and 16.3% in the whole group, respectively.
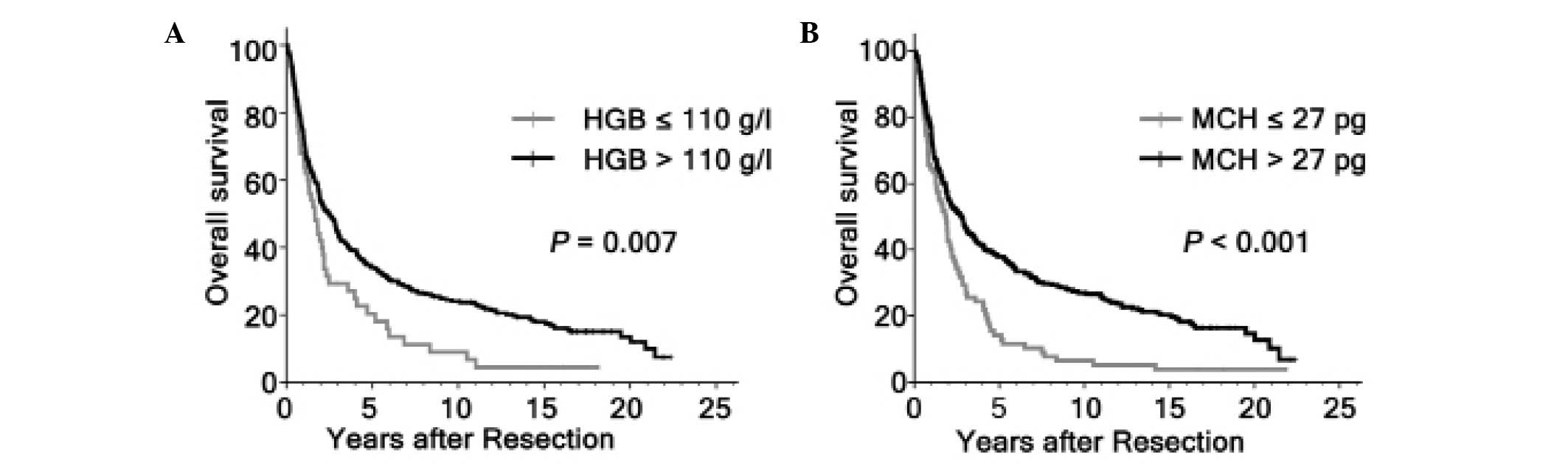
Variables, which may affect the OS of patients with HCC in this
study were subjected to univariable and multivariable Cox
regression analysis. Univariate analysis revealed that HBsAg
(P=0.024), tumor size (P<0.001), tumor encapsulation (P=0.002),
tumor number (P<0.001), vascular invasion (P<0.001), tumor
differentiation (P=0.031), tumor node metastasis (TNM) stage
(P<0.001), GGT (P<0.001), AFP (P=0.036), HGB (P=0.007) and
MCH (P<0.001) levels were all significantly associated with the
OS (Fig. 1; Table II). As the TNM stage was associated
with several clinical indexes, including tumor size, tumor number
and vascular invasion, the TNM stage was not entered into the
multivariate Cox proportional hazards analysis with these indexes
to avoid potential bias. In multivariate models, tumor size
(P<0.001), vascular invasion (P<0.001), GGT (P=0.001), HBsAg
(P=0.035) and MCH level (P<0.001) were revealed to be
independently significant factors of OS (Table II).
| Table II.Prognostic factors of OS in 399
patients with HCC. |
Table II.
Prognostic factors of OS in 399
patients with HCC.
|
| Univariate | Multivariate |
|---|
|
|
|
|
|---|
| Variable | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Age, years |
|
|
|
|
|
|
| >48
vs. ≤48 | 0.932 | 0.750–1.758 | 0.525 |
|
|
|
| Gender |
|
|
|
|
|
|
| Male
vs. female | 1.273 | 0.874–1.853 | 0.208 |
|
|
|
| HBsAg |
|
|
|
|
|
|
|
Positive vs. negative | 1.382 | 1.043–1.830 | 0.024 | 1.369 | 1.023–1.832 | 0.035 |
| Cirrhosis |
|
|
|
|
|
|
| Yes vs.
no | 1.100 | 0.843–1.435 | 0.484 |
|
|
|
| Tumor size, cm |
|
|
|
|
|
|
| ≥10 vs.
<10 | 1.699 | 1.347–2.143 | <0.001 | 1.679 | 1.310–2.152 | <0.001 |
| Tumor
encapsulation |
|
|
|
|
|
|
| None
vs. complete | 1.412 | 1.136–1.756 | 0.002 | 1.138 | 0.899–1.441 | 0.283 |
| Tumor no. |
|
|
|
|
|
|
|
Multiple vs. solitary | 1.599 | 1.275–2.006 | <0.001 | 1.123 | 0.872–1.448 | 0.369 |
| Vascular
invasion |
|
|
|
|
|
|
| Present
vs. absent | 2.051 | 1.548–2.718 | <0.001 | 1.758 | 1.305–2.367 | <0.001 |
|
Differentiation |
|
|
|
|
|
|
| III–IV
vs. I–II | 1.298 | 1.024–1.645 | 0.031 | 1.245 | 0.973–1.594 | 0.082 |
| TNM stage |
|
|
|
|
|
|
| II–III
vs. I | 1.678 | 1.346–2.091 | <0.001 |
|
|
|
| AFP, µg/l |
|
|
|
|
|
|
| >25
vs. ≤25 | 1.284 | 1.107–1.622 | 0.036 | 1.191 | 0.935–1.516 | 0.157 |
| GGT, U/l |
|
|
|
|
|
|
| >50
vs. ≤50 | 1.631 | 1.312–2.028 | <0.001 | 1.486 | 1.184–1.866 | 0.001 |
| HGB, g/l |
|
|
|
|
|
|
| ≤110
vs. >110 | 1.183 | 0.905–1.546 | 0.007 | 1.205 | 0.861–1.686 | 0.278 |
| MCH, pg |
|
|
|
|
|
|
| ≤27 vs.
>27 | 1.737 | 1.346–2.242 | <0.001 | 1.845 | 1.393–2.445 | <0.001 |
Subanalysis of patients with large
tumor size
Although previous studies have shown that hepatic
resection is a safe modality for HCC >10 cm, the efficacy of
surgical resection for large HCC remained controversial for high
risk of recurrence. In the present study, the patients with large
HCC were associated with non-cirrhotic (P=0.012), absence of tumor
encapsulation (P=0.025), multiple tumor number (P=0.001), presence
of vascular invasion (P=0.003) and high TNM stage (P<0.001;
Table III). In addition, tumors ≥10
cm had a tendency of higher postoperative mortality compared with
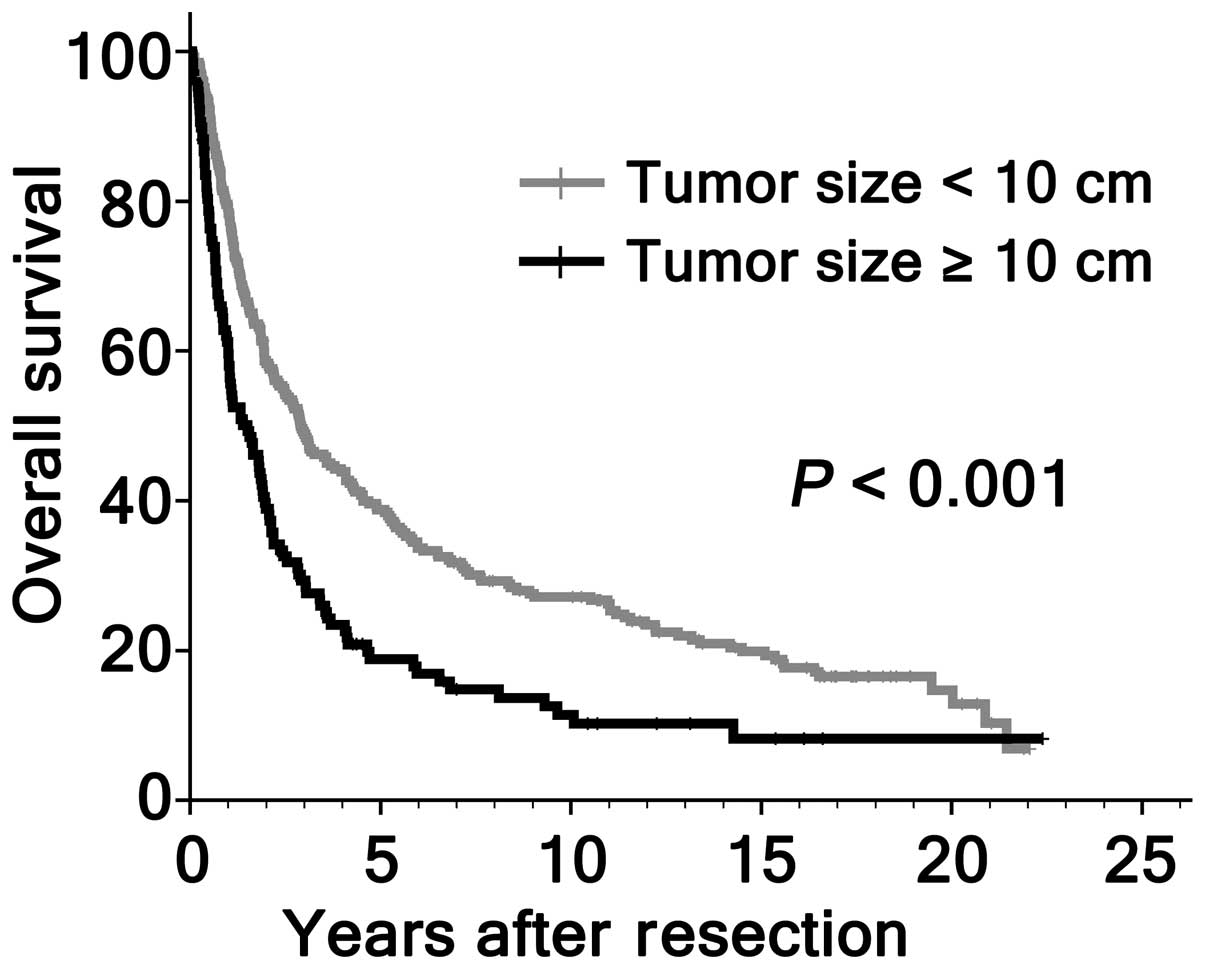
patients with smaller HCC (3.1, vs. 0.7%; P=0.084; Table III). The OS rates at 5, 10 and 15
years for patients with large HCC were significantly lower compared
with those with smaller HCC (18.3, vs. 38.9, 9.4, vs. 27.4 and 7.1,
vs. 20.1%, respectively; P<0.001; Fig.
2). However, 18/127 (14.2%) patients with large HCC survived
>5 years following hepatic resection. A natural question arose
as to whether selected cases with larger HCC had favorable
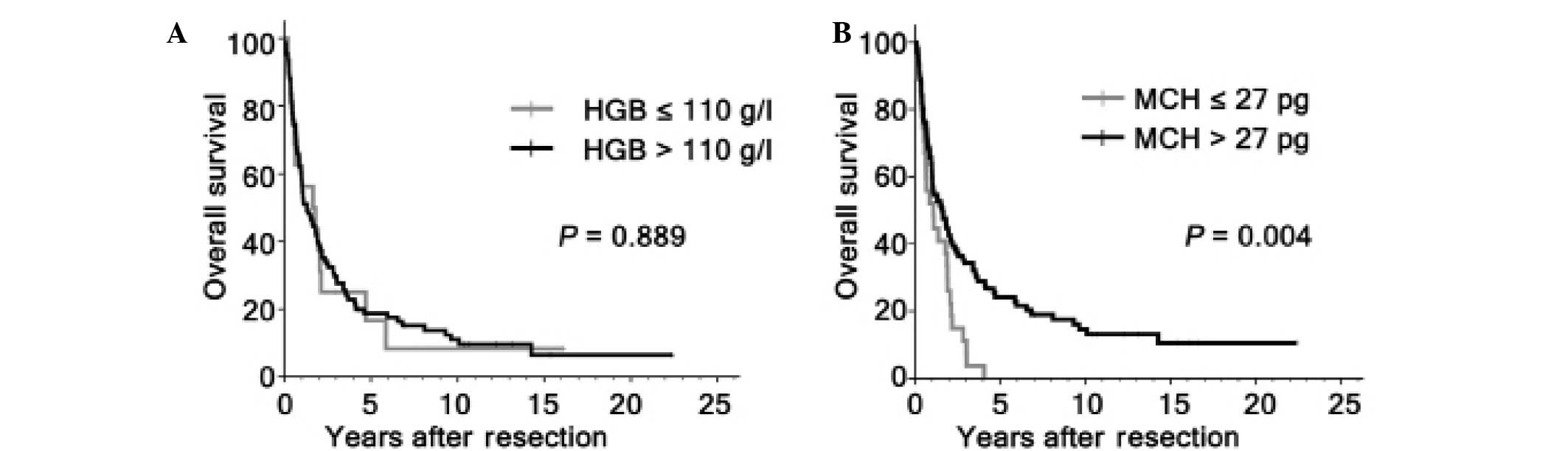
survival. Therefore, the present study further investigated the
prognostic significance of HGB, MCH and other clinicopathological
variables on OS among the 127 patients with large HCC. By
univariate analysis, HGB level was not associated with OS
(P=0.889), while tumor encapsulation (P=0.001), vascular invasion
(P<0.001), tumor differentiation (P<0.001) and MCH level
(P=0.004) were significant prognostic factors for OS (Fig. 3; Table
IV). On multivariate analysis, vascular invasion (P<0.001),
tumor differentiation (P<0.001) and MCH level (P=0.001) were
identified as independent prognostic indicators for OS (Table IV).
| Table III.Cinicopathalogical variables in
patients with HCC >10 cm and in patients with smaller
tumors. |
Table III.
Cinicopathalogical variables in
patients with HCC >10 cm and in patients with smaller
tumors.
| Variable | No. cases | HCC <10 cm n (%)
(n= 272) | HCC ≥10 cm n (%)
(n= 127) | P-value |
|---|
| Age, years |
|
|
|
|
|
≤48 | 207 | 237 (50.4) | 70
(55.1) | 0.376 |
|
>48 | 192 | 135 (49.6) | 57 (44.9) |
|
| Gender |
|
|
|
|
|
Female | 43 | 30 (11.0) | 13 (10.2) | 0.812 |
|
Male | 356 | 242
(89.0) | 114 (89.8) |
|
| HBsAg |
|
|
|
|
|
Negative | 80 | 55 (20.2) | 25
(19.7) | 0.901 |
|
Positive | 319 | 217 (79.8) | 102 (80.3) |
|
| Cirrhosis |
|
|
|
|
| No | 86 | 49 (18.0) | 37
(29.1) | 0.012 |
|
Yes | 313 | 223
(82.0) | 90 (70.9) |
|
| Tumor
encapsulation |
|
|
|
|
|
Complete | 193 | 142 (52.2) | 51
(40.2) | 0.025 |
| None | 206 | 130
(47.8) | 76 (59.8) |
|
| Tumor no. |
|
|
|
|
|
Solitary | 259 | 191 (70.2) | 68
(53.5) | 0.001 |
|
Multiple | 140 | 81
(29.8) | 59 (46.5) |
|
| Vascular
invasion |
|
|
|
|
|
Absent | 326 | 233 (85.7) | 93 (73.2) | 0.003 |
|
Present | 73 | 39 (14.3) | 34 (26.8) |
|
|
Differentiation |
|
|
|
|
|
I–II | 285 | 194 (71.3) | 91
(71.7) | 0.946 |
|
III–IV | 114 | 78
(28.7) | 36 (28.3) |
|
| TNM stage |
|
|
|
|
| I | 225 | 170 (62.5) | 55
(43.3) | <0.001 |
|
II–III | 174 | 102
(37.5) | 72 (56.7) |
|
| AFP, µg/l |
|
|
|
|
| ≤25 | 127 | 88 (32.4) | 39 (30.7) | 0.743 |
| >25 | 272 | 184 (67.6) | 38 (69.3) |
|
| Hospital
mortality | 6 | 2 (0.7) | 4 (3.1) | 0.084 |
| Table IV.Prognostic factors of OS in patients
with HCC >10 cm. |
Table IV.
Prognostic factors of OS in patients
with HCC >10 cm.
|
| Univariate | Multivariate |
|---|
|
|
|
|
|---|
| Variable | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Age, years |
|
|
|
|
|
|
| >48
vs. ≤48 | 0.770 | 0.527–1.125 | 0.175 |
|
|
|
| Gender |
|
|
|
|
|
|
| Male
vs. female | 1.829 | 0.889–3.761 | 0.096 |
|
|
|
| HBsAg |
|
|
|
|
|
|
|
Positive vs. negative | 1.530 | 0.932–2.513 | 0.090 |
|
|
|
| Cirrhosis |
|
|
|
|
|
|
| Yes vs.
no | 1.349 | 0.887–2.052 | 0.161 |
|
|
|
| Tumor
encapsulation |
|
|
|
|
|
|
| None
vs. complete | 1.887 | 1.274–2.795 | 0.001 | 1.276 | 0.824–1.976 | 0.274 |
| Tumor no. |
|
|
|
|
|
|
|
Multiple vs. solitary | 1.374 | 0.939–2.011 | 0.100 |
|
|
|
| Vascular
invasion |
|
|
|
|
|
|
| Present
vs. absent | 2.768 | 1.777–4.310 | <0.001 | 2.363 | 1.486–3.759 | <0.001 |
|
Differentiation |
|
|
|
|
|
|
| III–IV
vs. I–II | 2.194 | 1.453–3.312 | <0.001 | 2.179 | 1.406–3.375 | <0.001 |
| TNM stage |
|
|
|
|
|
|
| II–III
vs. I | 1.579 | 1.074–2.323 | 0.019 |
|
|
|
| AFP, µg/l |
|
|
|
|
|
|
| >25
vs. ≤25 | 1.493 | 0.989–2.255 | 0.055 |
|
|
|
| GGT, U/l |
|
|
|
|
|
|
| >50
vs. ≤50 | 1.469 | 0.987–2.186 | 0.056 |
|
|
|
| HGB, g/l |
|
|
|
|
|
|
| ≤110
vs. >110 | 0.961 | 0.548–1.686 | 0.889 |
|
|
|
| MCH, pg |
|
|
|
|
|
|
| ≤27 vs.
>27 | 1.931 | 1.224–3.049 | 0.004 | 2.222 | 1.361–3.636 | 0.001 |
Discussion
It has been previously reported that anemia was
prevalent in certain patients with malignant disease (12), however, few studies reported the
prevalence of anemia in HCC. Qiu et al (16) revealed that the percentage of
pretreatment anemia in the HCC group was 7.0%, which was <12.8%
of the present study. This difference may be due to study
population selection bias.
The prevalence of anemia among patients with HCC may
be associated with a number of reasons. The pathogenesis of
cancer-associated anemia, including nutritional deficiency,
hemolysis, blood loss and infiltration of the bone marrow by tumor
cells was postulated to be one of the common causes (21). Similarly, chronic liver injury can
result in anemia in patients with HCC (22). A previous study showed that
downregulation of iron-regulatory genes, including hepcidin,
ceruloplasmin, transferrin and transferrin receptor, disturbed
systemic iron balance and contributed to anemia in patients with
HCC (23). Disordered iron
homeostasis is considered to be a co-factor in the onset and
progression of almost all liver diseases, including the development
of HCC (24). In the present study,
it was revealed that one of the iron status markers, MCH, was
reduced in 12.8% of the patients with HCC in the entire cohort. The
positive correlation of MCH and HGB indicated that anemia was
partially caused by iron deficiency.
In numerous previous studies, HGB levels, either
prior to or during anticancer treatment, have been shown to have an
impact on survival (15,25). Cordella et al (26) demonstrated that a low level of HGB was
an indicator for lymph node metastasis and poor survival of oral
squamous cell carcinoma. Two independent studies demonstrated that
low HGB was a significant risk factor for patients with non-small
cell lung cancer TNM stage I (27,28). Qiu
et al (16) previously showed
that anemia was an independent prognostic factor in patients with
HCC. However, no previous study focused on the correlation of MCH
with survival in patients with cancer. In the present study, it was
revealed that both preoperative HGB and MCH were correlated with
gender. Furthermore, patients with low levels of MCH were more
prone to have absence of tumor encapsulation. Although HGB and MCH
were not observed to be widely associated with tumor-associated
factors, the outcome in patients with low levels of HGB or MCH was
poor overall on univariate analysis. Therefore, HGB and MCH
appeared to be reliable prognostic biomarkers. However,
multivariate analysis using the Cox proportional hazard model
demonstrated that MCH, however, not HGB was associated with poor
survival following consideration of other prognostic factors.
Multivariate analysis excluding HGB level is probably due to the
correlation between the presence of anemia and iron deficiency. In
general, MCH is one of the hematological indicators of iron
deficiency (29,30). Several previous studies have shown
that microcytic hypochromic anemia is associated with iron
overload, particularly in the liver (31,32). In
fact, iron overload is considered to be a co-factor in the onset
and progression of HCC (24). Taken
together, iron overload may explain, at least in part, poorer
prognosis of HCC patients with low levels of MCH.
In the entire cohort, 127 (31.8%) patients with HCC
met the tumor size ≥10 cm. As previously reported (33), the present study revealed that large
HCCs were more aggressive compared with smaller HCCs. Additionally,
extremely poor outcome following resection for large HCC was clear.
It appeared that resection for large HCC was not a good selection
for treatment. However, increasing evidence indicated that hepatic
resection performed on carefully selected patients was safe and
effective for HCC patients with large tumor size (2). Similarly, hospital mortality between the
two groups was comparable in the present study, which suggested
that hepatic resection for large HCC was safe. With the
improvements in surgical techniques and peri-operative care,
hepatic resection for large HCC provided an improved long-term
survival compared with transcatheter arterial chemoembolization or
other therapies (34). However,
surgical resection had excellent outcomes only in carefully
selected patients with large tumor size. In trying to select those
patients with large HCCs, which may be best served by resection,
several previous studies had defined the prognostic factors for HCC
with large tumor types (35). A
previous review summed up the risk factors influencing the survival
of large HCC under resection (2), and
the risk factor with the highest prevalence was vascular invasion.
Two previous reports revealed that poor tumor differentiation
indicates inferior OS of large HCC (36,37). In
the present study, vascular invasion and poor tumor differentiation
was able to predict poor OS in HCC patients with large tumors.
Similarly, when we observed HCC patients with large tumors, MCH
significantly predicted OS. Together, the present data indicated
that MCH, which are easily obtained, may be an important
consideration when selecting HCC with large tumors for
hepatectomy.
One of the major limitations of the present study
was that the quantity of iron deposition in the liver was not
determined. Whether low MCH level was associated with iron overload
in the liver remains to be elucidated. Therefore, the present study
hypothesized that the underlying pathophysiology in HCC patients
with low MCH level warrants further investigation. Retrospective
design, which has the associated issues of potential selection
bias, was another limitation. In this case, consecutive patient
sampling was used to reduce patient selection bias. Notably, the
present results require further confirmation by prospective
investigations in multicenter clinical trials.
In conclusion, the present study demonstrated that
MCH level effectively classified patients with HCC under liver
resection into groups of poor and improved outcomes, thereby adding
novel prognostic value to traditional clinicopathological risk
factors. Additionally, selection based on MCH level may be modified
to identify patients with large HCC who are most likely benefit
from resection.
Acknowledgements
The present study was supported by grants from the
National Natural Science Foundation of China (no. 81372571) and the
Guangdong Department of Science and Technology Translational
Medicine Center (no. 2011A080300002).
Glossary
Abbreviations
Abbreviations:
|
AFP
|
α-fetoprotein
|
|
HGB
|
hemoglobin
|
|
MCH
|
mean corpuscular hemoglobin
|
|
HBsAg
|
hepatitis B surface antigen
|
|
TNM
|
tumor-node-metastasis
|
|
HCC
|
hepatocellular carcinoma
|
|
OS
|
overall survival
|
References
|
1
|
Jemal A, Bray F, Center MM, Ferlay J, Ward
E and Forman D: Global cancer statistics. CA Cancer J Clin.
61:69–90. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Tsoulfas G, Mekras A, Agorastou P and
Kiskinis D: Surgical treatment for large hepatocellular carcinoma,
Does size matter? ANZ J Surg. 82:510–517. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Poon Tung-Ping R, Fan ST and Wong J: Risk
factors, prevention and management of postoperative recurrence
after resection of hepatocellular carcinoma. Ann Surg. 232:10–24.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Forner A, Llovet JM and Bruix J:
Hepatocellular carcinoma. Lancet. 379:1245–1255. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Villanueva A, Minguez B, Forner A, Reig M
and Llovet JM: Hepatocellular carcinoma, Novel molecular approaches
for diagnosis, prognosis and therapy. Annu Rev Med. 61:317–328.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Villanueva A, Hoshida Y, Toffanin S, et
al: New strategies in hepatocellular carcinoma: Genomic prognostic
markers. Clin Cancer Res. 16:4688–4694. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ju MJ, Qiu SJ, Fan J, et al: Preoperative
serum gamma-glutamyl transferase to alanine aminotransferase ratio
is a convenient prognostic marker for Child-Pugh A hepatocellular
carcinoma after operation. J Gastroenterol. 44:635–642. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sasaki A, Iwashita Y, Shibata K, et al:
Prognostic value of preoperative peripheral blood monocyte count in
patients with hepatocellular carcinoma. Surgery. 139:755–764. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Amano H, Tashiro H, Oshita A, et al:
Significance of platelet count in the outcomes of hepatectomized
patients with hepatocellular carcinoma exceeding the Milan
criteria. J Gastrointest Surg. 15:1173–1181. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Mano Y, Shirabe K, Yamashita Y, et al:
Preoperative neutrophil-to-lymphocyte ratio is a predictor of
survival after hepatectomy for hepatocellular carcinoma: A
retrospective analysis. Ann Surg. 258:301–305. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Boogaerts M, Mittelman M and Vaupel P:
Beyond anaemia management, Evolving role of erythropoietin therapy
in neurological disorders, multiple myeloma and tumour hypoxia
models. Oncology. 69((Suppl 2)): S22–S30. 2005. View Article : Google Scholar
|
|
12
|
Caro JJ, Salas M, Ward A and Goss G:
Anemia as an independent prognostic factor for survival in patients
with cancer, A systemic, quantitative review. Cancer. 91:2214–2221.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Holzner B, Kemmler G, Greil R, et al: The
impact of hemoglobin levels on fatigue and quality of life in
cancer patients. Ann Oncol. 13:965–973. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Van Belle: SJ andC ocquyt V: Impact of
haemoglobin levels on the outcome of cancers treated with
chemotherapy. Crit Rev Oncol Hematol. 47:1–11. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kim JH, Lee JM, Ryu KS, et al: The
prognostic impact of duration of anemia during chemotherapy in
advanced epithelial ovarian cancer. Oncologist. 16:1154–1161. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Qiu MZ, Xu RH, Ruan DY, et al: Incidence
of anemia, leukocytosis and thrombocytosis in patients with solid
tumors in China. Tumour Biol. 31:633–641. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wu XN, Su D, Wang L and Yu FL: Roles of
the hepcidin-ferroportin axis and iron in cancer. Eur J Cancer
Prev. 23:122–133. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Heath JL, Weiss JM, Lavau CP and Wechsler
DS: Iron deprivation in cancer-potential therapeutic implications.
Nutrients. 5:2836–2859. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Chun YH, Kim SU, Park JY, do Kim Y, Han
KH, Chon CY, Kim BK, Choi GH, Kim KS, Choi JS and Ahn SH:
Prognostic value of the 7th edition of the AJCC staging system as a
clinical staging system in patients with hepatocellular carcinoma.
Eur J Cancer. 47:2568–2575. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Chen MH, Chang PM, Chen PM, et al:
Prognostic significance of a pretreatment hematologic profile in
patients with head and neck cancer. J Cancer Res Clin Oncol.
135:1783–1790. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Aapro M, Österborg A, Gascón P, Ludwig H
and Beguin Y: Prevalence and management of cancer-related anaemia,
iron deficiency and the specific role of i.v. Histopathology. Ann
Oncol. 23:1954–1962. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Intragumtornchai T, Rojnukkarin P,
Swasdikul D, et al: Anemias in Thai patients with cirrhosis. Int J
Hematol. 65:365–373. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Tseng HH, Chang JG, Hwang YH, et al:
Expression of hepcidin and other iron-regulatory genes in human
hepatocellular carcinoma and its clinical implications. J Cancer
Res Clin Oncol. 135:1413–1420. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Deugnier Y and Turlin B: Pathology of
hepatic iron overload. Semin Liver Dis. 31:260–271. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Reichel O, Panzer M, Wimmer C, et al:
Prognostic implications of hemoglobin levels before and after
surgery as well as before and after radiochemotherapy for head and
neck tumors. Eur Arch Otorhinolaryngol. 260:248–253.
2003.PubMed/NCBI
|
|
26
|
Cordella C, Luebbers HT, Rivelli V, Grätz
KW and Kruse AL: An evaluation of the preoperative hemoglobin level
as a prognostic factor for oral squamous cell carcinoma. Head Neck
Oncol. 3:352011. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Tomita M, Shimizu T, Hara M, Ayabe T and
Onitsuka T: Impact of preoperative hemoglobin level on survival of
non-small cell lung cancer patients. Anticancer Res 28 (3B).
1947–1950. 2008.
|
|
28
|
Yovino S, Kwok Y, Krasna M, et al: An
association between preoperative anemia and decreased survival in
early-stage non-small-cell lung cancer patients treated with
surgery alone. Int J Radiat Oncol Biol Phys. 62:1438–1443. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Juncà J, Fernández-Avilés F, Oriol A, et
al: The usefulness of the serum transferrin receptor in detecting
iron deficiency in the anemia of chronic disorders. Haematologica.
83:676–680. 1998.PubMed/NCBI
|
|
30
|
Alquaiz JM, Abdulghani HM, Khawaja RA and
Shaffi-Ahamed S: Accuracy of various iron parameters in the
prediction of iron deficiency anemia among healthy women of child
bearing age, Saudi Arabia. Iran Red Crescent Med J. 14:397–401.
2012.PubMed/NCBI
|
|
31
|
Iolascon A: DeF alco L and Beaumont C:
Molecular basis of inherited microcytic anemia due to defects in
iron acquisition or heme synthesis. Haematologica. 94:395–408.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Batts KP: Iron overload syndromes and the
liver. Mod Pathol. 20((Suppl 1)): S31–S39. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Truant S, Boleslawski E, Duhamel A, et al:
Tumor size of hepatocellular carcinoma in noncirrhotic liver: A
controversial predictive factor for outcome after resection. Eur J
Surg Oncol. 38:1189–1196. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Zhong JH, Ke Y, Gong WF, et al: Hepatic
resection associated with good survival for selected patients with
intermediate and advanced-stage hepatocellular carcinoma. Ann Surg.
260:329–340. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Shah SA, Wei AC, Cleary SP, Yang I,
McGilvray ID, Gallinger S, Grant DR and Greig PD: Prognosis and
results after resection of very large (>or=10 cm) hepatocellular
carcinoma. J Gastrointest Surg. 11:589–595. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Mok KT, Wang BW, Lo GH, et al:
Multimodality management of hepatocellular carcinoma larger than 10
cm. J Am Coll Surg. 197:730–738. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Shrager B, Jibara GA, Tabrizian P, et al:
Resection of large hepatocellular carcinoma (≥10 cm): A unique
western perspective. J Surg Oncol. 107:111–117. 2013. View Article : Google Scholar : PubMed/NCBI
|