Introduction
Neutrophilic dermatoses include a group of
inflammatory conditions of the skin, characterised by
polymorphonuclear infiltration. Sweet's syndrome is a neutrophilic
dermatosis with dermal involvement that may be associated with
hematological malignancies (1,2). Sweet's
syndrome is characterised by sudden onset of fever, neutrophilia,
erythematous skin lesions and neutrophilic infiltration of the
dermis on skin biopsy (3,4). Malignancy-associated Sweet's syndrome is
often associated with the discovery or recurrence of the underlying
malignancy and it is more common in myelogenous leukemia compared
with lymphoproliferative disorders (5,6).
Subcutaneous Sweet's syndrome (Sweet's panniculitis)
is a variant with certain different clinical and pathological
characteristics, which distinguish it from the classic syndrome. In
particular, the subcutaneous fat rather than the dermis is the main
site of neutrophilic infiltration. The number of cases with this
variant reported to date is limited (7). However, to the best of our knowledge, no
association between lymphoproliferative disorders and subcutaneous
Sweet's syndrome has been reported to date.
Rituximab is a monoclonal antibody (anti-CD20) that
has been shown to be effective in certain dermatological disorders,
particularly when standard systemic therapies are ineffective or
contraindicated (8).
In this report, we present a patient with chronic
lymphocytic leukemia (CLL) with refractory subcutaneous Sweet's
syndrome, and report the patient's clinical response to treatment
with rituximab. To the best of our knowledge, this is one of the
first reports on rituximab as a novel biological therapy for
Sweet's syndrome.
Case report
A 48-year-old man with a 2-year history of CLL
developed fever and skin lesions in December, 2013. Following the
diagnosis of CLL (Rai stage IV), the patient received several
chemotherapeutic regimens, including cyclophosphamide, vincristine
and prednisolone (CVP; 4 cycles), chlorambucil-prednisolone (1
cycle) and rituximab, fludarabine and cyclophosphamide (RFC; 4
cycles). Furthermore, during his last course of chemotherapy, he
received multiple doses of granulocyte colony-stimulating factor
(G-CSF). Complete remission had been achieved 3 months prior to
admission and the patient was under surveillance.
Four days prior to the onset of fever and skin rash,
thrombocytopenia without any other symptoms was detected on the
last surveillance visit. Peripheral blood smear and bone marrow
examination revealed no evidence of relapse and dexamethasone pulse
therapy (40 mg/day/for 4 days) was administered with the diagnosis
of autoimmune thrombocytopenia. Following the fourth dose of
dexamethasone, the patient developed fever, chills, malaise,
dyspnea, headache and myalgia. After 2 days, painful skin rashes
appeared at the back of the legs, anterior surface of the left
thigh, mons pubis, lower abdomen and anterior chest, followed by
additional similar lesions within the next 2 days. The rash was not
associated with pruritus. Celecoxib, indomethacin and prednisolone
were administered and the pain in some lesions was diminished;
however, enlargement of the skin lesions and edema persisted,
despite treatment. The patient reported red urine colour and edema
of the lower extremities within the next few days. Given the
progression of the symptoms, colchicine was added to the
treatment.
On the 10th day after the onset of symptoms, the
patient was admitted to the emergency department of our center. The
patient had no history of any other underlying disease. A history
of war injuries and exposure to a blast wave were reported.
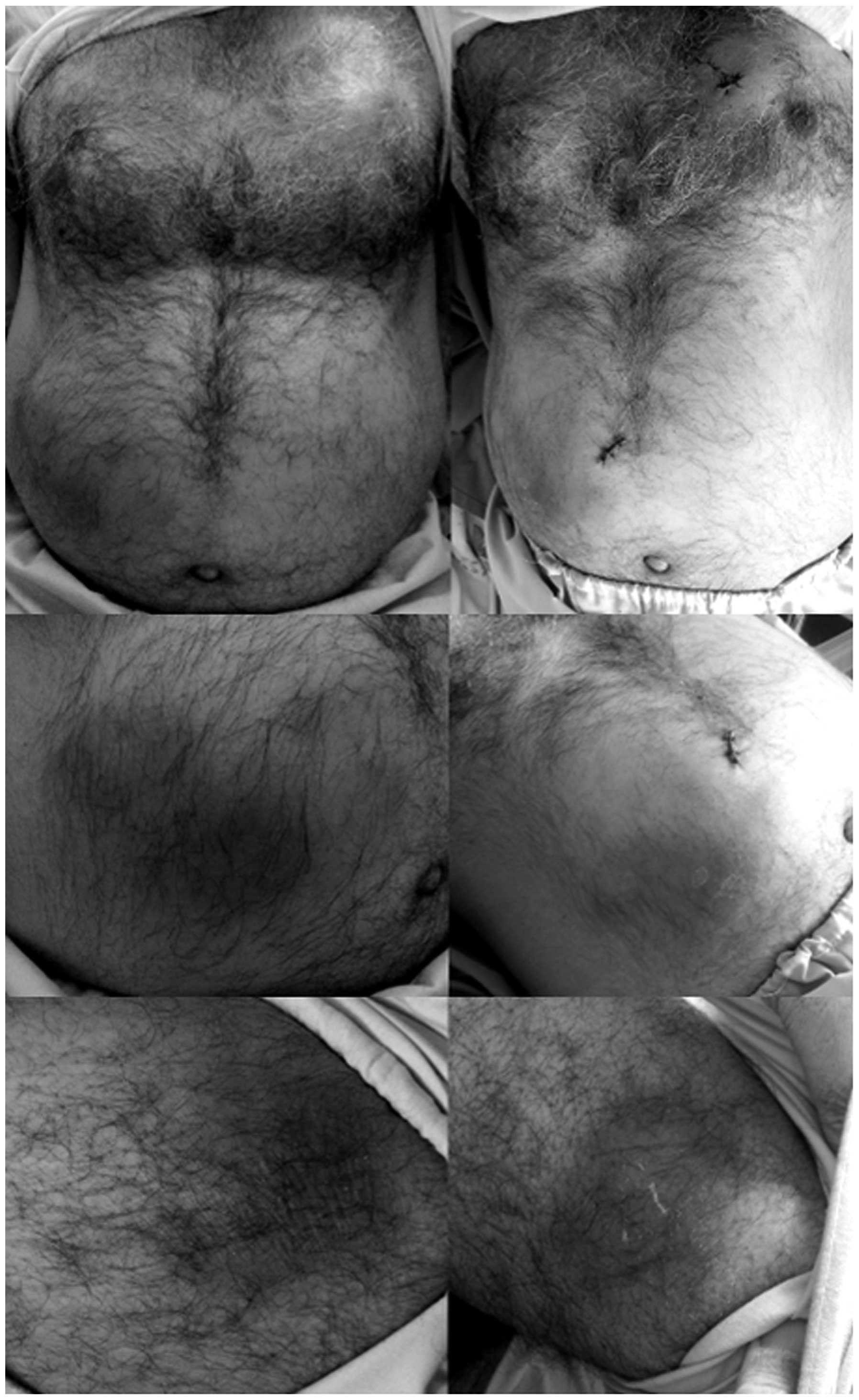
On admission, the patient's vital signs were as
follows: blood pressure, 80/60 mmHg; pulse rate, 100 beats/min;
respiratory rate, 14 breaths/min; and temperature, 36.7°C. A
dermatological examination revealed 5 mobile, well-defined,
erythematous, subcutaneous, painful periareolar masses on the
chest, varying in size from 2 to 8 cm. There were also firm,
indurated, well-defined, erythematous, painful lesions in the right
lower abdomen and mons pubis (5×5 cm). Similar lesions, sized 4×4
cm were identified in the left lower abdomen. Indurated,
well-defined, erythematous, painful plaques were observed in the
left middle thigh and posterolateral part of the left lower limb,
with a size varying from 1 to 4 cm. There was also pitting edema of
the lower extremities (Fig. 1).
Other physical findings included diffuse wheezing
and coarse crackles in the lungs, and mild abdominal distention. No
lymphadenopathy, organomegaly or arthritis were present.
The laboratory examination results were as follows:
white blood cell count, 7.6×109/l, with 96.6%
neutrophils and 2.4% lymphocytes (Table
I); hemoglobin concentration, 9.3 g/dl (mean corpuscular
volume, 89 fl/cell); platelet count, 38×109/l;
erythrocyte sedimentation rate, 34 mm/h (normal, 0–15 mm/h); and
C-reactive protein level, 113 mg/l (normal, <6 mg/l). In the
biochemical tests, the blood urea nitrogen was 65 mg/dl; the
creatinine level was 2.1 mg/dl; the lactate dehydrogenase level was
257 IU/l; and the albumin level was 2.5 g/dl.
 | Table I.Changes in the patient's blood cells
counts following onset of symptoms. |
Table I.
Changes in the patient's blood cells
counts following onset of symptoms.
|
|
Days |
|---|
|
|
|
|---|
| Variables | 10th | 11th | 12th | 13th | 14th | 17th | 18th | 21st | 22nd | 25th |
|---|
| WBC (/µl) | 7,600 | 11,200 | 7,000 | 5,700 | 8,100 | 5,500 | 2,600 | 1,900 | 2,200 | 3,500 |
| Seg (%) | 96.6 | 97.5 | 96 | 88.4 | 93.4 | 95.1 | 83.2 | 67.6 | 71.0 | 70.7 |
| Lymph (%) | 2.4 | 0.6 | 2.7 | 4.7 | 3.3 | 3.8 | 7.0 | 14.5 | 14.7 | 15.2 |
| Hb (g/dl) | 9.3 | 10.7 | 10.8 | 11.9 | 10.3 | 8.5 | 8.4 | 8.7 | 8.1 | 8.6 |
| MCV (fl) | 89.0 | 88.6 | 83.9 | 83.9 | 87.2 | 81.6 | 81.1 | 81.3 | 83.2 | 85.1 |
| Plt (/ml) | 38000 | 44000 | 56000 | 59000 | 64000 | 36000 | 64000 | 69000 | 78000 | 80000 |
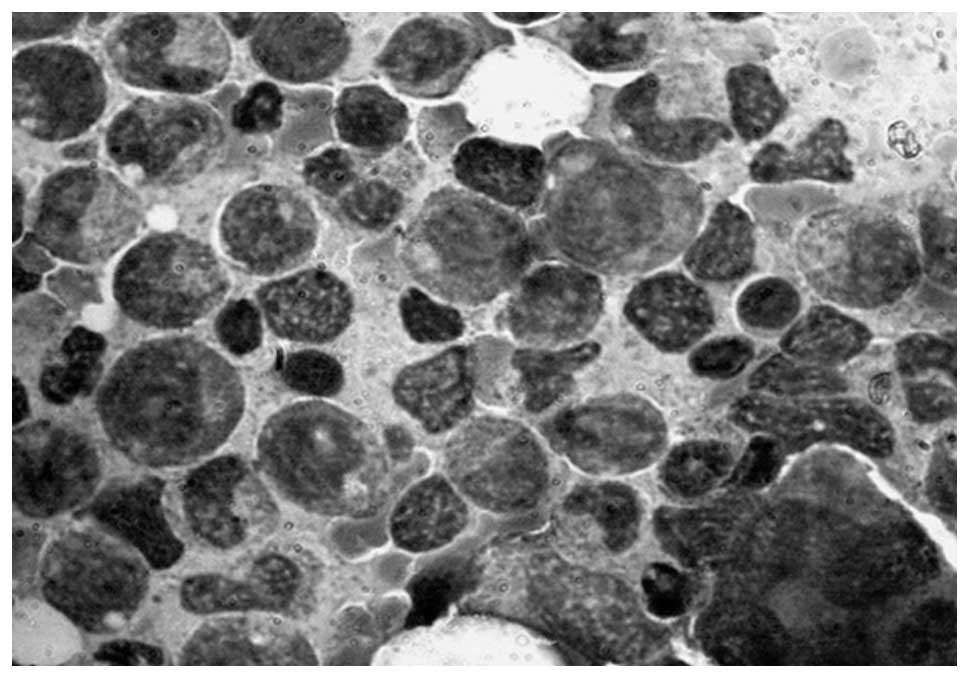
The bone marrow biopsy revealed a reactive and
hypercellular marrow. The myeloid:erythroid ratio was 4–5:1 and the
lymphocytes were <10%, with an increased proportion of
promyelocytes to myelocytes (Fig. 2).
There was no evidence of relapse.
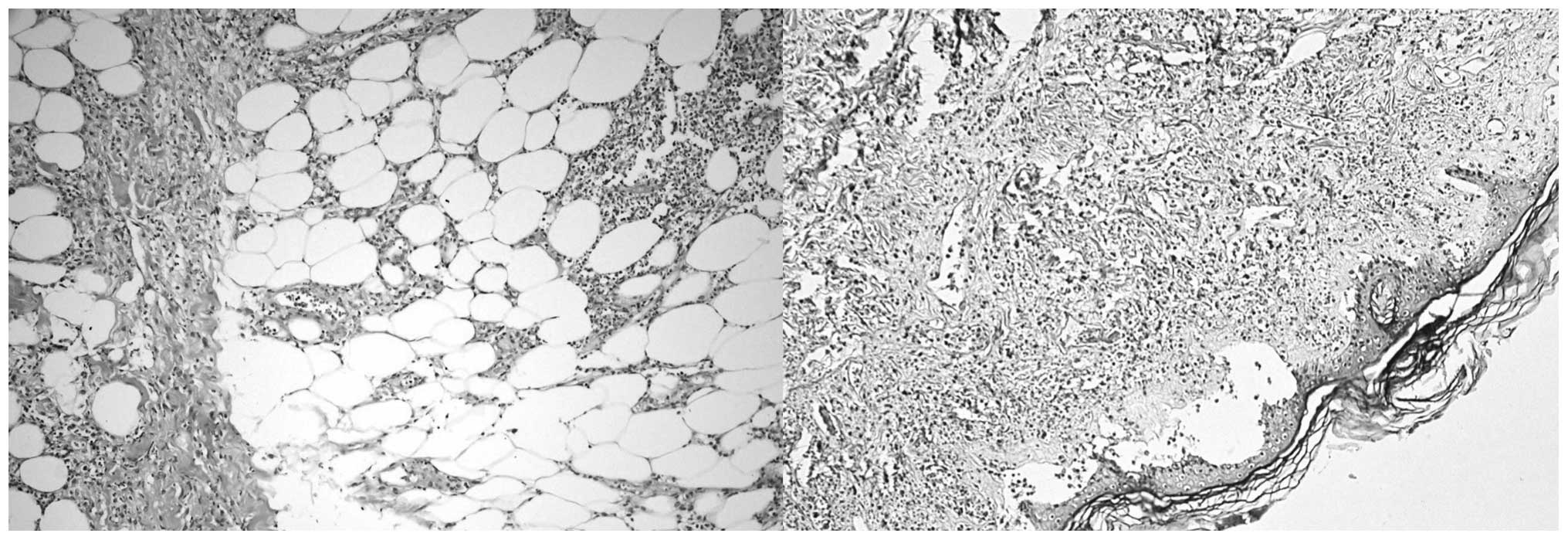
The skin biopsy revealed an unremarkable epidermis
and a thick dermis, with multilayered collagenous bundles. The
hypodermis was infiltrated by mature polymorphonuclear cells into
and between the subcutaneous adipocytes. Few foci of lymphocyte and
polymorphonuclear lymphocyte (PMN) infiltration into the vessels
wall were observed. The pathological examination was compatible
with mixed septal and lobular neutrophilic panniculitis (Fig. 3). Urine culture was positive for
Pseudomonas, which was treated with suitable antibiotics.
The blood culture was negative.
Following hospital admission, prednisolone,
indomethacin and colchicine were discontinued. Hydrocortisone and
ceftriaxone were introduced and celecoxib was continued. The first
dose of rituximab (375 mg/m2 body surface) was
administered. On the 18th day, a second rituximab dose was
administered and, given the patient's wheezing, indomethacin was
discontinued (Table II).
| Table II.Summary of the clinical course and
therapeutic measures. |
Table II.
Summary of the clinical course and
therapeutic measures.
| Time point | Clinical
event(s) | Therapeutic
measure(s) |
|---|
| Last surveillance
visit | Diagnosis of
autoimmune thrombocytopenia | Dexamethasone pulse
therapy |
| 1st day (onset of
symptoms) | Onset of skin rash
(last dose of dexamethasone) | Celecoxib (100 mg
t.d.s.); indomethacin (75 mg b.i.d.); prednisolone (5 mg
daily) |
| 9th day | Progression of
symptoms | Addition of
colchicine (0.5 mg q 2 h up to 8 times) |
| 10th day (day of
admission) |
| Discontinuation of
prednisolone, indomethacin and colchicine |
|
|
| Initiation of:
Rituximab (1st dose) 375 mg/m2 body surface;
hydrocortisone (200 mg i.v. stat before rituximab, then 100 mg i.v.
t.d.s.); celecoxib (100 mg p.o. b.i.d.); ceftriaxone (2 gr i.v.
stat, then 1 gr i.v. b.i.d.); cimetidine (400 mg i.v. stat before
rituximab) |
| 13th day | No improvement in
symptoms | Reinstitution of:
Indomethacin (75 mg p.o. b.i.d.); colchicine (1 mg p.o. daily) |
| 15th day | Progression of limb
and scrotal edema | Triamterene H (1 tab
p.o. daily); hydrocortisone (100 mg i.v. b.i.d.) |
| 18th day | Continuous limb and
scrotal edema | Rituximab (2nd dose);
furosemide (40 mg i.v. daily) |
|
| Continued
wheezing | Discontinuation of
indomethacin; colchicine (1 mg p.o. b.i.d.); hydrocortisone (100 mg
i.v. t.d.s.) |
|
| Positive urine
culture and antibiogram result | Discontinuation of
ceftriaxone; imipenem (250 mg t.d.s.) |
| 19th day | Decreased upper limb
edema and patient's weight; no dyspnea |
|
| 21st day | Disappearance of
fever |
|
| 22nd day | Reduced pain and
tenderness in skin lesions Improved superficial features of the
rash |
|
| 28th day | Discharge with good
general condition |
|
From the 19th day onwards, the patient's condition
started to improve. Upper limb edema and the patient's weight
decreased and there was no complaint of dyspnea. The fever had
disappeared since the 21st day. On the 22nd day, the patient
observed a reduction in the pain and tenderness of the skin lesions
and the examination revealed minor alterations in the superficial
characteristics of the rash (Fig.
1).
Our patient was discharged in a good general
condition, 28 days aftert the onset of fever and skin rash. A
follow-up skin biopsy revealed a very thin epidermis and an
edematous fibrotic dermis, with a diffuse dermal infiltrate of
mature PMNs, as well as moderate red blood cell extravasation.
There was previous evidence of septal and lobular panniculitis
(Fig. 3). Approximately 2 months
later, the patient succumbed to septic shock.
Discussion
We herein report the case of a CLL patient with
refractory neutrophilic dermatosis not responding to conventional
therapeutic regimens. However, after receiving two doses of
rituximab, the patient's symptoms and general condition
improved.
On the primary skin biopsy, unlike the classic
Sweet's syndrome, which is characterised by dermal infiltration by
PMNs (7), the neutrophilic
infiltration was seen in hypodermis. Accordingly, the terms
‘subcutaneous Sweet's syndrome’ (7)
or ‘Sweet's panniculitis’ (9) may be
used. The pathological examination revealed mixed lobular and
septal panniculitis. The most common reported pattern for
subcutaneous Sweet's syndrome is lobular panniculitis. However,
there are some reports of a mixed pattern in the literature
(7).
The follow-up skin biopsy revealed a neutrophilic
infiltration of the dermis in conjunction with prior mixed lobular
and septal neutrophilic panniculitis. These findings indicate that
subcutaneous Sweet's syndrome may evolve to a classic Sweet's
syndrome, despite systemic treatment.
We described a lymphoproliferative disorder as the
underlying hematological malignancy in our patient; however,
myeloid leukemia appears to be more commonly associated with this
syndrome in the literature (5,6). Sweet's
syndrome is usually accompanied with evidence suggesting the onset,
relapse or recurrence of the underlying malignancy in similar
reports (3,5,10–12). However, in our patient, the leukemia
was in remission. To the best of our knowledge, the association of
subcutaneous Sweet's syndrome and lymphoproliferative disorders has
not been priorly reported.
The head, neck, upper and lower limbs, are the
predominant regions affected in Sweet's syndrome (6). In our patient, the lesions were located
on the anterior wall of abdomen and chest, as well as in the lower
extremities, with an ascending pattern of development. This pattern
of involvement is unusual in classic Sweet's syndrome; however, the
majority of the cases of subcutaneous Sweet's syndrome have been
associated with lower extremity involvement (7).
Given the positive urine culture, infectious
panniculitis was considered as a differential diagnosis. However,
the disease course and relief of the lesions following rituximab
treatment, but not with antibiotic therapy, excluded this
possibility.
Our patient received G-CSF as part of his
chemotherapeutic regimen for up to 4 months prior to the
development of the skin lesions. A review of the literature
indicated a similar association between treatment with G-CSF and
development of Sweet's syndrome (13). The patient's rash had appeared
following a high-dose pulse of dexamethasone. The literature search
yielded no report on neutrophilic dermatosis following
dexamethasone administration.
Various treatments have been proposed for Sweet's
syndrome to date and, although it is a self-limiting disease,
timely recognition and appropriate treatment may reduce its
morbidity (6). The first-line
systemic drugs are corticosteroids, potassium iodide and
colchicine, with second-line drugs including indomethacin,
clofazimine, cyclosporine and dapsone (14). Other successful methods, such as
biological treatments with tumor necrosis factor antagonists, have
been reported (14). There are
several reports on the beneficial effects of the interleukin-1
receptor antagonist anakinra on neutrophilic dermatoses (15–17). In
addition, limited reports have investigated other biological agents
for the treatment of Sweet's syndrome, such as adalimumab (18), immunoglobulin (19,20) and
infliximab (18,21).
Rituximab affects the progression of the cell cycle
and is used as an adjunctive to chemotherapy in the treatment of
neoplasms. The volume of evidence on the benefits of rituximab in
the treatment of autoimmune diseases is currently growing and it is
suggested that rituximab may also be helpful in certain
dermatological conditions (22).
To the best of our knowledge, this is one of the
first reports the role of rituximab for the treatment of Sweet's
syndrome has been documented. In our patient, an improvement in the
general condition and skin lesions, as well as a reduction in the
neutrophil count following administration of rituximab, suggest
that this biological agent may be a novel treatment for refractory
Sweet's syndrome. However, future randomized trials are required to
study its efficacy and side effects.
References
|
1
|
Assari R, Ziaee V, Parvaneh N and
Moradinejad MH: Periodic fever and neutrophilic dermatosis, Is it
Sweet's syndrome? Case Reports Immunol. 2014:3209202014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Prat L, Bouaziz JD, Wallach D,
Vignon-Pennamen MD and Bagot M: Neutrophilic dermatoses as systemic
diseases. Clin Dermatol. 32:376–388. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Thompson MA, Dyson SW and Faderl S:
Sweet's syndrome in chronic lymphocytic leukemia associated with
neutropenic fever and granulocyte colony-stimulation factor. Am J
Hematol. 81:703–705. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Sweet RD: An acute febrile neutrophilic
dermatosis. Br J Dermatol. 76:349–356. 1964. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Cohen PR: Sweet's syndrome - a
comprehensive review of an acute febrile neutrophilic dermatosis.
Orphanet J Rare Dis. 2:342007. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Dabade TS and Davis MD: Diagnosis and
treatment of the neutrophilic dermatoses (pyoderma gangrenosum
Sweet's syndrome). Dermatol Ther. 24:273–284. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Guhl G and Garcia-Diez A: Subcutaneous
Sweet syndrome. Dermatol Clin. 26:541–551. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Bhandari PR and Pai VV: Novel applications
of rituximab in dermatological disorders. Indian Dermatol Online J.
5:250–259. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Cullity J, Maguire B and Gebauer K:
Sweet's panniculitis. Australas J Dermatol. 32:61–64. 1991.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Usul Afşar C, Paydaş S, Günaldi M, Bozkurt
Duman B, Erçolak V, Zorludemir S and Açikalin A: Sweet syndrome in
a patient with chronic lymphocytic leukemia/small lymphocytic
lymphoma: Curious lymphocyte/neutrophil fluctuations. Turk J
Haematol. 30:413–415. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Cholongitas E, Pipili C, Dasenaki M and
Kaklamanis L: Piperacillin/tazobactam-induced Sweet syndrome in a
patient with chronic lymphocytic leukemia and autoimmune
cholangitis. Am J Dermatopathol. 30:203–204. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Tageja N, Giorgadze T and Zonder J:
Dermatological complications following initiation of lenalidomide
in a patient with chronic lymphocytic leukaemia. Intern Med J.
41:286–288. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Reuss-Borst MA, Müller CA and Waller HD:
The possible role of G-CSF in the pathogenesis of Sweet's syndrome.
Leuk Lymphoma. 15:261–264. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Cohen PR: Neutrophilic dermatoses: A
review of current treatment options. Am J Clin Dermatol.
10:301–312. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lipsker D, Perrigouard C, Foubert A and
Cribier B: Anakinra for difficult-to-treat neutrophilic
panniculitis, IL-1 blockade as a promising treatment option for
neutrophil-mediated inflammatory skin disease. Dermatology.
220:264–267. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kluger N, Gil-Bistes D, Guillot B and
Bessis D: Efficacy of anti-interleukin-1 receptor antagonist
anakinra (Kineret®) in a case of refractory Sweet's syndrome.
Dermatology. 222:123–127. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Delluc A, Limal N, Puéchal X, Francès C,
Piette JC and Cacoub P: Efficacy of anakinra, an IL1 receptor
antagonist, in refractory Sweet syndrome. Anne Rheum Dis.
67:278–279. 2008. View Article : Google Scholar
|
|
18
|
Karamlou K and Gorn AH: Refractory Sweet
syndrome with autoimmune organizing pneumonia treated with
monoclonal antibodies to tumor necrosis factor. J Clin Rheumatol.
10:331–335. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Gill HH, Leung AY, Trendell-Smith NJ,
Yeung CK and Liang R: Sweet syndrome due to myelodysplastic
syndrome, Possible therapeutic role of intravenous immunoglobulin
in addition to standard treatment. Adv Hematol. 2010:3283162010.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Haliasos E, Soder B, Rubenstein DS,
Henderson W and Morrell DS: Pediatric Sweet syndrome and
immunodeficiency successfully treated with intravenous
immunoglobulin. Pediatr Dermatol. 22:530–535. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Lobo AM, Stacy R, Cestari D, Stone JH,
Jakobiec FA and Sobrin L: Optic nerve involvement with panuveitis
in Sweet syndrome. Ocul Immunol Inflamm. 19:167–170. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Schafranski MD, Merlini AB, Hungaro AC,
Luciano JJ and Schumacher MS: Rituximab: Update on pharmacology and
clinical applications.
|