Introduction
Gastrointestinal stromal tumours (GISTs) are
mesenchymal cell-derived neoplasms of the gut that have assumed
oncological importance out of proportion to their relatively rare
incidence due to having provided important insight into cancer
biology. They originate from the interstitial cells of Cajal, the
pacemaker cells that regulate peristalsis in the digestive tract
(1). The pathogenesis of GISTs is
based on the oncogenic, mutational activation of KIT tyrosine
kinase in >95% of cases, or less frequently, on that of
platelet-derived growth factor receptor alpha (2,3).
Pre-clinical studies revealed that the drug imatinib
mesylate inhibits the activity of the protein products of these two
GIST-associated oncogenes, which led to the development of one of
the first identified pathway-driven, highly effective treatments
for a solid tumour. While the majority of GISTs are
chemotherapy-resistant, >50% of affected patients responded to
imatinib mesylate, increasing the average survival of patients with
advanced disease to 5 years (4).
GISTs are rare with an age-adjusted yearly incidence
rate of 0.68/100,000 individuals; they mostly affect individuals
aged >50 years with a male-to-female ratio of 1.5 (5). GISTs occur throughout the
gastrointestinal tract from the lower esophagus to the anus with
the most common sites being the stomach (60%), jejunum and ileum
(30%), duodenum (5%) and colorectum (<5%) (6).
Small bowel GISTs have a wide clinicopathological
spectrum at presentation, ranging from minute incidental nodules to
large tumours. Clinical signs and symptoms are usually
non-specific, and acute abdomen prompting emergency surgery is rare
and commonly arises from bleeding, intestinal obstruction, tumour
rupture with intra-abdominal haemorrhage, pelvic mass and
appendicitis-like acute pain (6,7).
The present study reported on a case of a primary
small bowel GIST, which was initially diagnosed as an abdominal
abscess. While this complication has been reported in the
literature (6–9), abscess formation inside a GIST tumour
mass is a rare occurrence.
Case report
A male patient (age, 51 years) was admitted to
Maggiore Hospital (Parma, Italy), who had been presenting with
fever, dysuria and lower abdominal pain for four days. On
admission, the patient's axillary temperature was 39,4°C, the heart
rate was 104 beats per minute and the blood pressure was 145/90
mmHg. The patient did not have neurofibromatosis type I or any
other relevant family history, was taking no medications and his
past medical history was unremarkable. On physical examination, the
upper abdomen was soft with normal sensitivity, while in the lower
abdomen, a moderate tenderness in the hypogastrium without
peritoneal signs was present. General physical examination was
unremarkable.
Routine laboratory data on admission revealed a
white blood cell count of 18,200/mm3 (normal range,
3500–11,000/mm3), C-reactive protein levels of 130 mg/l
(normal range, 0–10 mg/l) and an erythrocyte sedimentation rate of
65 mm/h (normal range, 0–22 mm/h). Other biochemical parameters and
liver function tests were normal. Plain abdominal radiography
showed an extraintestinal air-fluid level in the hypogastric region
without any free intraperitoneal air. Ultrasonography and computed
tomography (CT) of the abdomen revealed the presence of a 7,5×5,5
cm pelvic mass containing air and liquid, which was located behind
the bladder and close to a normal appendix, and was indicated to be
an intraperitoneal abscess. Gastrografin enema examination excluded
colon pathologies.
Diagnostic laparoscopy showed a huge, soft cystic
mass adherent to the small bowel. The procedure was then converted
to an open exploration through a midline incision. At laparotomy,
the cyst-like mass arising from the ileal wall, with a prevalent
extramural growth and mostly protruding into the mesentery, was
located ~40 cm from the ileo-cecal valve. A normal Meckel's
diverticulum was observed at ~20 cm from the mass. No other
visceral abnormalities or intraperitoneal fluids were detected.
Ileal resection, including the Meckel's diverticulum, and
end-to-end ileal anastomosis were performed without tumour
rupture.
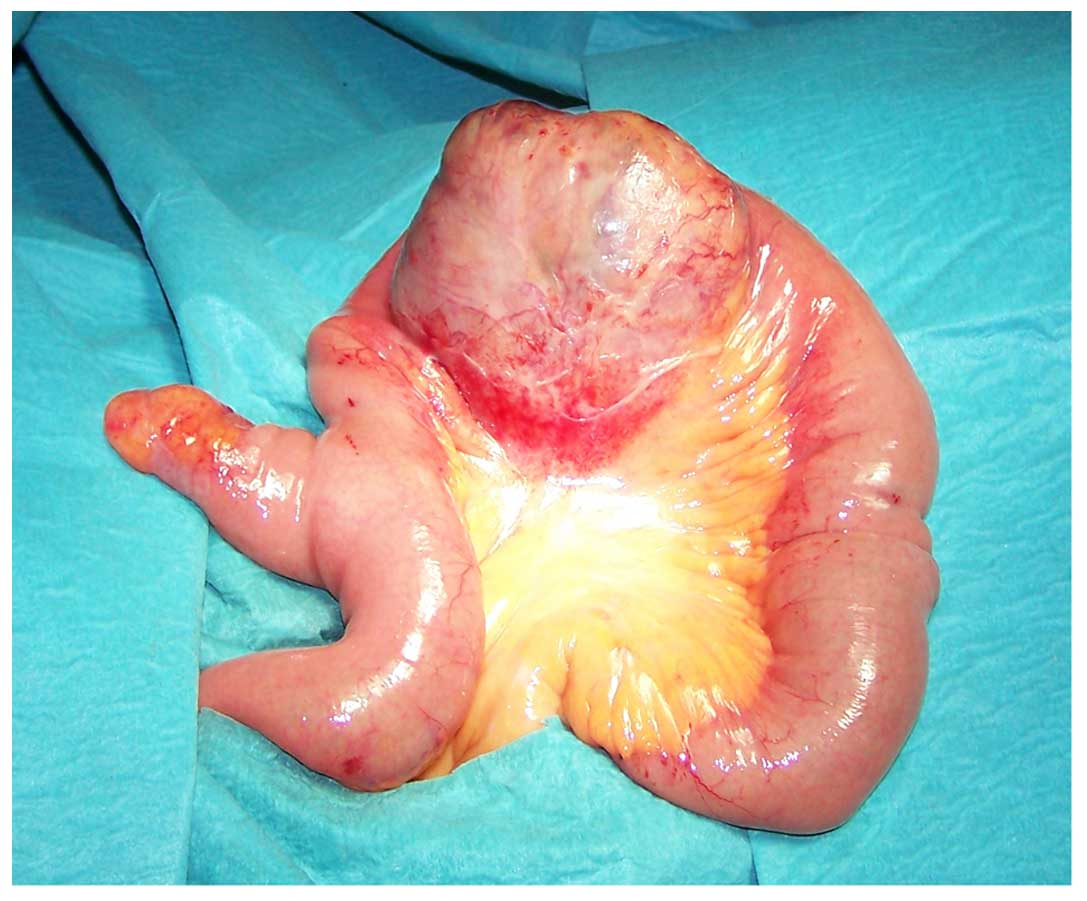
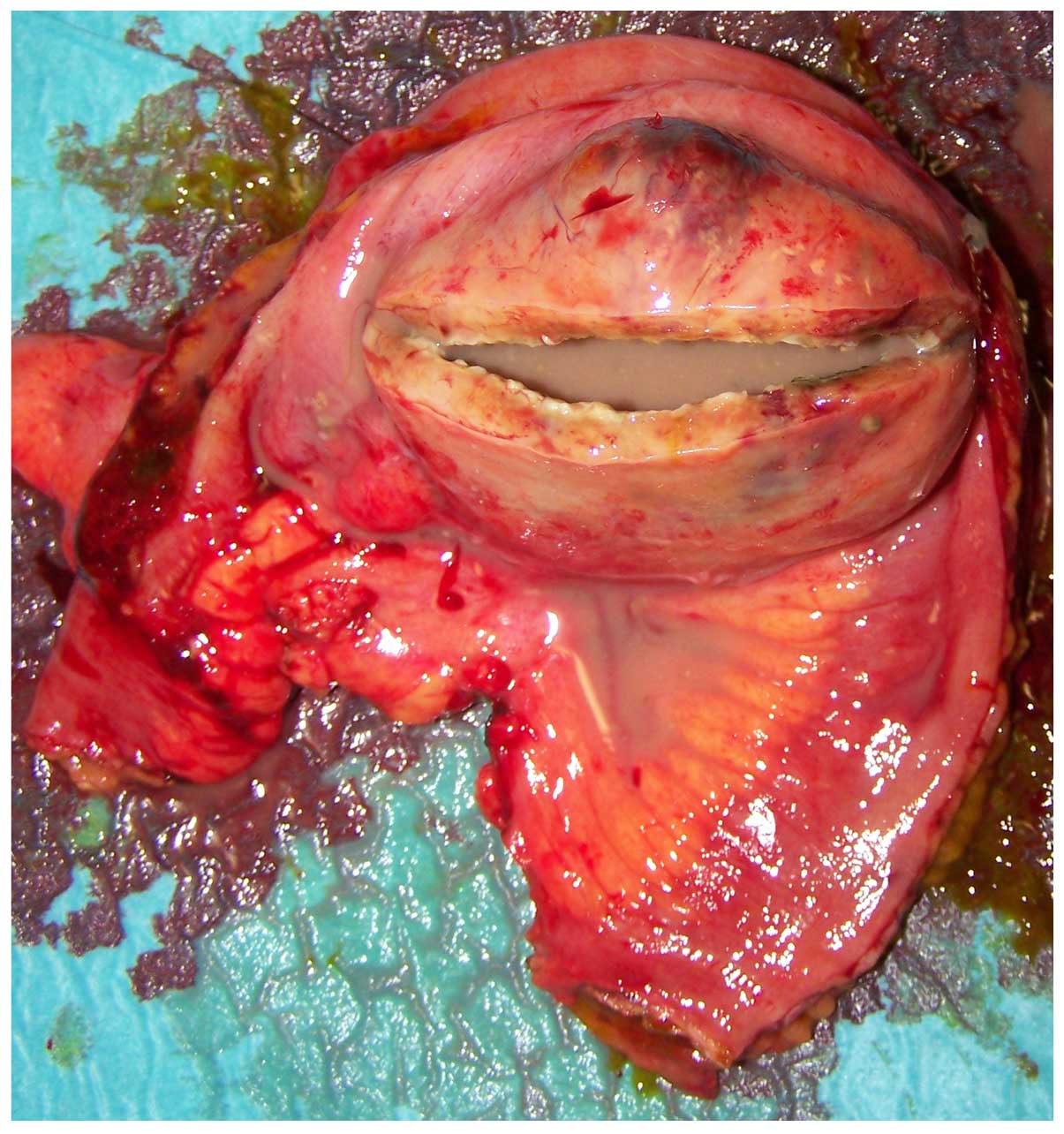
At macroscopic examination, the excised mass,
measuring 7 cm in diameter (Fig. 1),
showed a cystic aspect with a central cavity containing a large
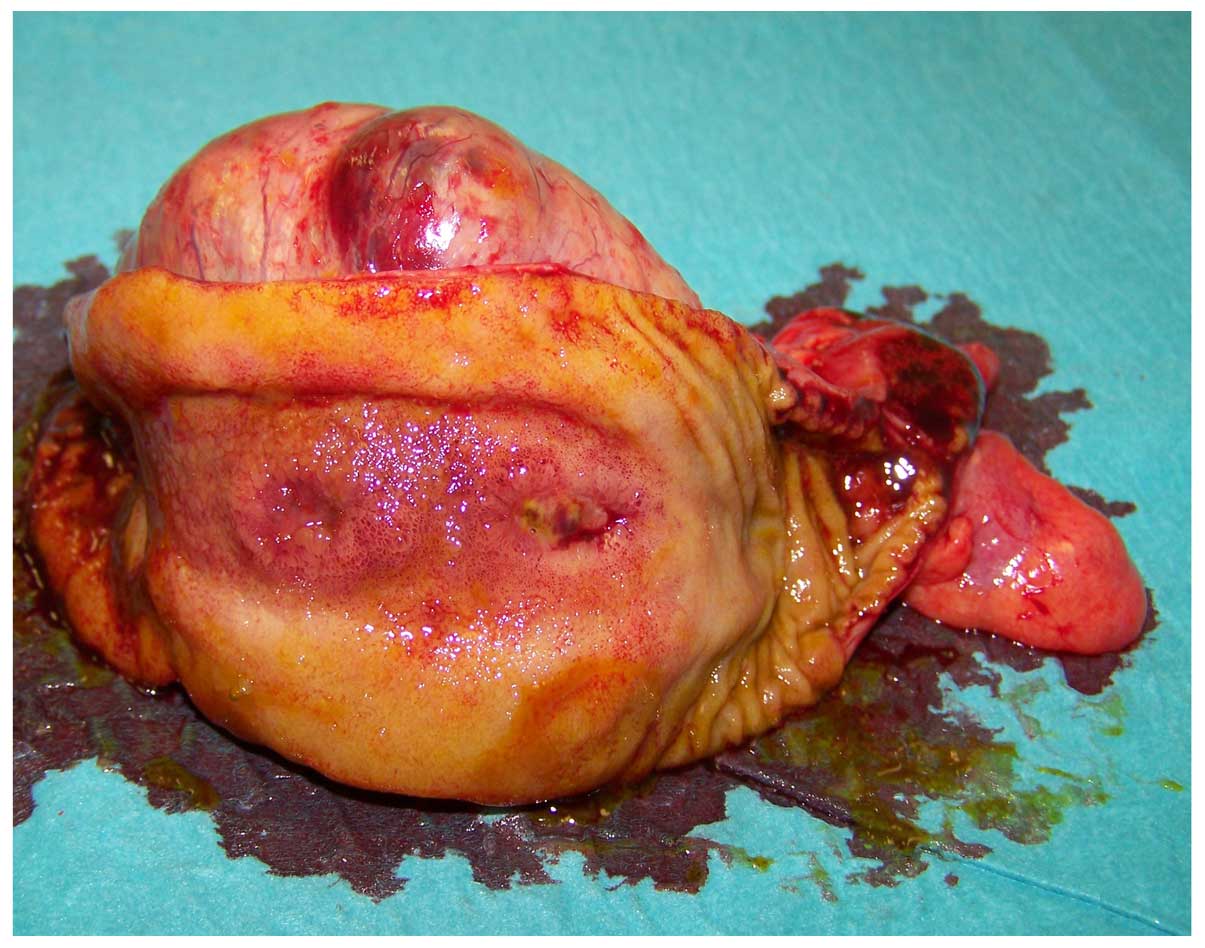
amount of pus (Fig. 2); closer
examination revealed a communication with the small bowel lumen via
a mucosal ulceration and enteric leakage through the central part
of the mass (Fig. 3).
Histopathology showed a spindle-cell
mesenchymal-type neoplasm with erosion of the small bowel mucosal
layer. Immunohistochemistry revealed that tumour cells were
c-KIT-positive, CD34-negative, α-smooth muscle actin-negative and
S-100-negative. The mitotic rate was <5/50 high-power fields.
The resection margins and mesenteric lymph nodes were disease free.
Pathological examination of the Meckel's diverticulum was
unremarkable. Of note, histopathology of the abscess wall showed
that tumour cells had replaced the full thickness of the ileal
wall. The final diagnosis was intermediate-risk GIST.
The post-operative course was uneventful and the
patient was discharged home on the seventh post-operative day.
Adjuvant imatinib mesylate (400 mg daily for 1 year) was
administered. Yearly follow-up by CT scan was performed and at 72
months after surgery, no tumour recurrence had been detected.
Discussion
Among the acute clinical presentations of primary
small bowel GIST, tumour mass perforation with peritonitis has been
infrequently reported in the literature, while abscess formation
inside the GIST mass represents an exceptional occurrence (6–9). In
fact, a literature search of the PubMed database on sporadic
primary small bowel GISTs including studies published from January
1976 to December 2015 in English language using the search terms
‘gastrointestinal stromal tumour’ (7,595 studies) and
‘gastrointestinal stromal tumour complications’ (1,545 studies)
retrieved only two cases of abscess formation inside a small bowel
GIST (10,11).
The first case study by Bardell et al
(10) reported on a large GIST of
the ileum in a male patient (age, 41 years), presenting as an
infected mesenteric cystic mass. The patient was subjected to ileal
resection including the mass. Pathological examination of the
resected specimen showed a large GIST with a central cystic area
communicating with the intestinal lumen via a fistula tract. The
second case was a male patient (age, 22 years) with abdominal pain
and fever as well as a pelvic mass detected by CT, who was
subjected to CT-guided drainage of the abscess and subsequently to
segmental resection of the jejunum with subsequent pathological
examination revealing a GIST (11).
In these two cases as well as in the case of the present study, it
is likely that a wide coagulative necrosis inside the tumour mass
caused ulceration of the intestinal mucosa with enteric leakage and
abscess development; in fact in the present study,
histopathological analysis of the abscess wall showed that tumour
growth had replaced the full thickness of the gut wall. By
contrast, in the few reported cases of GIST complicated by an
abscess, the abscess wall was constituted by omentum and
surrounding intestinal loops wrapping a GIST tumour mass
perforation (8,12).
The macroscopic presentation of GIST in the present
study represents an exceptional finding and differential diagnoses
included abdominal cystic masses such as infected mesenteric cysts
of neoplastic or lymphatic origin, enteric duplication cysts and
cystic teratomas (13,14). However, histopathology revealed
positive staining for c-KIT, which excluded the diagnosis of other
types of mesenchymal neoplasm.
The prognosis for patients with GISTs is difficult
to predict. The most powerful and most widely examined criteria for
evaluating the biological properties of GIST are tumour size and
mitotic activity (15). The impact
of the anatomical location is controversial, while the majority of
studies indicate that primary small bowel GISTs have a more
aggressive behaviour than gastric GISTs with similar size and
mitosis parameters (6,7,16).
Moreover, tumour rupture, either occurring spontaneously or at
surgery, is considered an additional negative prognostic factor due
to increasing the risk of intra-abdominal implant tumours (17).
In conclusion, the present study reported on a
patient who appeared to have an abdominal abscess, which, after
surgical resection, was revealed to be a GIST including an abscess.
While this pathology is rare, resection of a preliminarily
diagnosed abdominal abscesses should be performed with caution to
avoid the rupture of a possible tumour and peritoneal seeding. In
the present case, conversion from laparotomy to open surgery was
mainly performed due to tumour mass size and tumour wall weakness.
The laparoscopic approach should be considered, taking into account
the result of the intraoperative assessment, the diameter of the
mass, the type of tumour wall and the feasibility of successful
oncologic clearance.
Glossary
Abbreviation
Abbreviations:
|
GIST
|
gastrointestinal stromal tumour
|
References
|
1
|
Kindblom LG, Remotti HE, Aldenborg F and
Meis-Kindblom JM: Gastrointestinal pacemaker cell tumor (GIPACT):
Gastrointestinal stromal tumors show phenotypic characteristics of
the interstitial cells of Cajal. Am J Pathol. 152:1259–1269.
1998.PubMed/NCBI
|
|
2
|
Hirota S, Isozaki K, Moriyama Y, Hashimoto
K, Nishida T, Ishiguro S, Kawano K, Hanada M, Kurata A, Takeda M,
et al: Gain-of-function mutations of c-kit in human
gastrointestinal stromal tumors. Science. 279:577–580. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Heinrich MC, Corless CL, Duensing A,
McGreevey L, Chen CJ, Joseph N, Singer S, Griffith DJ, Haley A,
Town A, et al: PDGFRA activating mutations in gastrointestinal
stromal tumors. Science. 299:708–710. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Demetri GD, von Mehren M, Blanke CD, Van
den Abbeele AD, Eisenberg B, Roberts PJ, Heinrich MC, Tuveson DA,
Singer S, Janicek M, et al: Efficacy and safety of imatinib
mesylate in advanced gastrointestinal stromal tumors. N Engl J Med.
347:472–480. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Tran T, Devila JA and El-Serag HB: The
epidemiology of malignant gastrointestinal stromal tumors: An
analysis of 1,458 cases from 1992 to 2000. Am J Gastroenterol.
100:162–168. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Miettinen M and Lasota J: Gastrointestinal
stromal tumors: Review on morphology, molecular pathology,
prognosis, and differential diagnosis. Arch Pathol Lab Med.
130:1466–1478. 2006.PubMed/NCBI
|
|
7
|
Miettinen M, Makhlouf H, Sobin LH and
Lasota J: Gastrointestinal stromal tumors of the jejunum and ileum:
A clinicopathologic, immunohistochemical, and molecular genetic
study of 906 cases before imatinib with long-term follow-up. Am J
Surg Pathol. 30:477–489. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Lord C, Ozgediz D and Cohen MJ: Image of
the month. Gastrointestinal stromal tumor. Arch Surg. 144:87–88.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Efremidou EI, Liratzopoulos N,
Papageorgiou MS and Romanidis K: Perforated GIST of the small
intestine as a rare cause of acute abdomen: Surgical treatment and
adjuvant therapy. Case report. J Gastrointestin Liver Dis.
15:297–299. 2006.PubMed/NCBI
|
|
10
|
Bardell T, Jalink DW, Hurlbut DJ and
Mercer CD: Gastrointestinal stromal tumour: Varied presentation of
a rare disease. Can J Surg. 49:286–289. 2006.PubMed/NCBI
|
|
11
|
Chen HW and Lin TY: Tumor abscess
formation caused by Morganella morganii complicated with bacteremia
in a patient with gastrointestinal stromal tumor. Clin Res Hepatol
Gastroenterol. 36:e29–e31. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Karagülle E, Türk E, Yildirim E, Gõktürk
HS, KiYici H and Moray G: Multifocal intestinal stromal tumors with
jejunal perforation and intra-abdominal abscess: Report of a case.
Turk J Gastroenterol. 19:264–267. 2008.PubMed/NCBI
|
|
13
|
Dow N, Giblen G, Sobin LH and Miettinen M:
Gastrointestinal stromal tumors: Differential diagnosis. Semin
Diagn Pathol. 23:111–119. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Rubin BP: Gastrointestinal stromal
tumours: An update. Histopathology. 48:83–96. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Fletcher CD, Berman JJ, Corless C,
Gorstein F, Lasota J, Longley BJ, Miettinen M, O'Leary TJ, Remotti
H, Rubin BP, et al: Diagnosis of gastrointestinal stromal tumors: A
consensus approach. Hum Pathol. 33:459–465. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Miettinen M and Lasota J: Gastrointestinal
stromal tumors: Pathology and prognosis at different sites. Semin
Diagn Pathol. 23:70–83. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Takahashi T, Nakajima K, Nishitani A,
Souma Y, Hirota S, Sawa Y and Nishida T: An enhanced risk-group
stratification system for more practical prognostication of
clinically malignant gastrointestinal stromal tumors. Int J Clin
Oncol. 12:369–374. 2007. View Article : Google Scholar : PubMed/NCBI
|