Introduction
Myoepithelial cells display characteristics of
epithelial as well as smooth muscle cells, and are usually located
in the breast, throughout the mammary duct system, as an
interrupted layer of stellate cells between the continuous luminal
epithelial cell layer and the basement membrane (1,2).
Therefore, neoplasms that arise from myoepithelial cells exhibit
both epithelial and smooth muscle cell characteristics, but lack
ductal differentiation (3).
Despite the fact that myoepithelial cells are part
of the structure of the human breast, pure myoepithelial neoplasms
are extremely uncommon and the number of such reported case studies
is limited (3–5).
Tavassoli (6) proposed
that five types of lesions are derived from or are composed of a
dominant to pure population of myoepithelial cells: Adenoid cystic
carcinoma, a rare mixed tumor referred to as pleomorphic carcinoma,
multifocal myoepitheliosis, adenomyoepithelioma and malignant
myoepithelioma (myoepithelial carcinoma). The latter has a
phenotype similar with that of metaplastic carcinoma (6–8).
Myoepithelial carcinoma is generally a solitary
lesion, characterized by an infiltrating proliferation of plump
atypical spindle cells with easily identifiable mitotic figures and
without an epithelial component, dispersed in a collagenous stroma
(1,8–10).
Myoepithelial cells are usually prominent in ducts and ductules in
the periphery of the lesion.
The diagnosis of malignancy is based on the presence
of marked cellularity, high mitotic rate, ill-defined margins,
infiltrative growth pattern, necrosis and local recurrence of the
tumor (4,9,11).
Isolated cases of myoepithelial carcinoma have been
described arising from a preexisting adenomyoepithelioma (7).
Case report
A 74-year-old woman was admitted to our medical
center with a firm mass on her left breast, sized ~10×7 cm, which
was identified on routine physical examination. The entire breast
was erythematous and warm, with a widespread edema of the skin and
a widely ulcerated nipple, mimicking advanced inflammatory
cancer.
The patient had a medical history of endometrial
adenocarcinoma, endometrioid type (International Federation of
Gynecology and Obstetrics stage IA, World Health Organization stage
T1N0M0) treated with radical hysterectomy and pelvic radiotherapy
(25 sessions of radiotherapy) 4 years prior (08/2009). Menarche
occurred at the age of 13 years and menopause at 50 years. The
patient reported four pregnancies (two live births and two
abortions); she had never smoked or consumed alcohol on a regular
basis and had never received exogenous hormones, contraceptives or
any chronic drug treatment. There was no family history of breast
cancer.
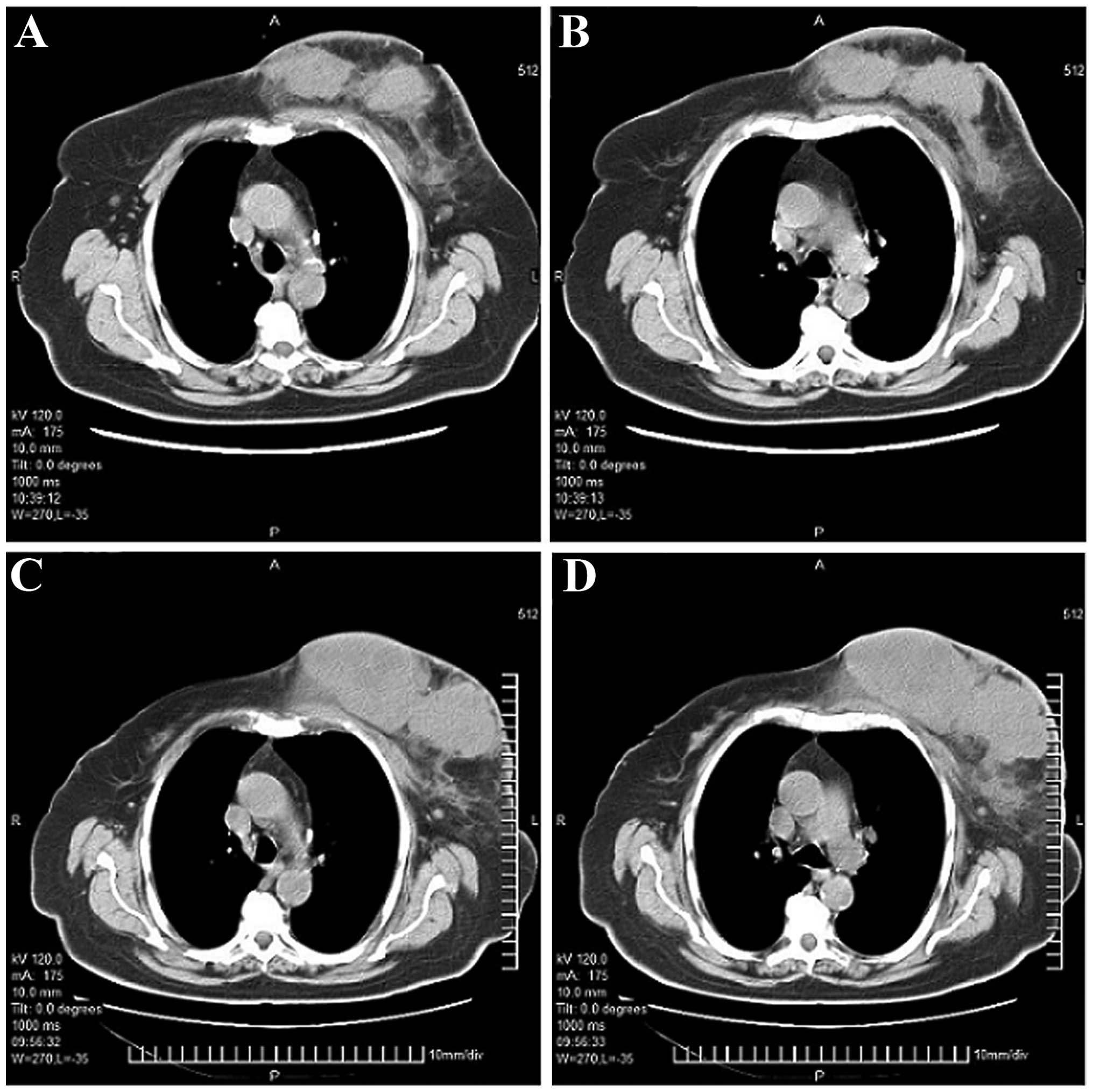
The laboratory tests and serum tumor marker levels
were within the normal range. A bone scan revealed no bone
metastasis. A computed tomography (CT) scan revealed multiple
diffuse lesions in the left breast (Fig.
1A and B), as well as abnormally enlarged unilateral axillary
lymph nodes, indicative of metastasis. No distant metastases were
detected. Aspiration biopsy cytology was performed, confirming the
diagnosis of breast cancer.
Due to the nature of the tumor (large size with
invasion of the skin and the chest wall, with additional
involvement of the axillary lymph nodes), the patient was staged as
IIIb and considered inoperable. Thus, neoadjuvant chemotherapy was
initiated, consisting of three cycles of docetaxel (75
mg/m2), doxorubicin (50 mg/m2) and
cyclophosphamide (500 mg/m2), repeated every 3
weeks.
Follow-up CT scans of the patient after completion
of therapy revealed disease progression, clearly indicating the
aggressiveness of the tumor and unresponsiveness to treatment
(Fig. 1C and D).
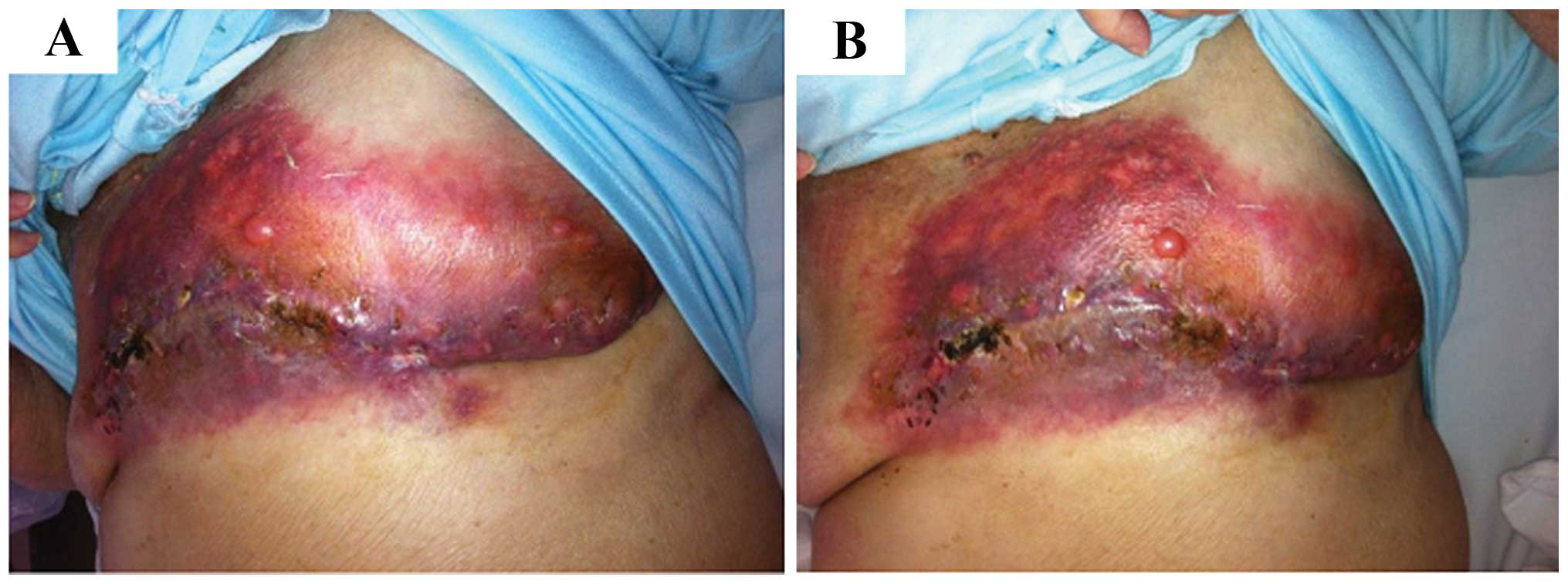
The surgical team performed drainage of an abscess
that had developed in the tumor area; however, due to excessive
bleeding, a palliative simple mastectomy was finally performed
(Fig. 2).
Postoperatively and prior to the administration of
further chemotherapy, the patient experienced early locoregional
recurrence (Fig. 2), also indicative
of the resistance of the tumor to treatment. First-line
chemotherapy with weekly doses of paclitaxel (70 mg/m2),
carboplatin (area under the curve 2) and bevacizumab (10 mg/kg)
every 3 weeks was scheduled.
Unfortunately, only two weekly doses of chemotherapy
were administered, as the patient developed a severe
disease-related infection, leading to fatal septic shock.
Consequently, the evaluation of the effectiveness of the
administered regimens could not be completed.
Gross findings
The dimensions of the surgical specimen were
23×15.5×8 cm, with skin attached to the exterior surface. On
dissection, almost the entire breast was occupied by firm,
multilobulated grayish-white areas measuring 16 cm in greater
diameter. The cut surface was partially solid, with areas of cystic
degeneration, hemorrhage and necrosis. The tumor infiltrated all
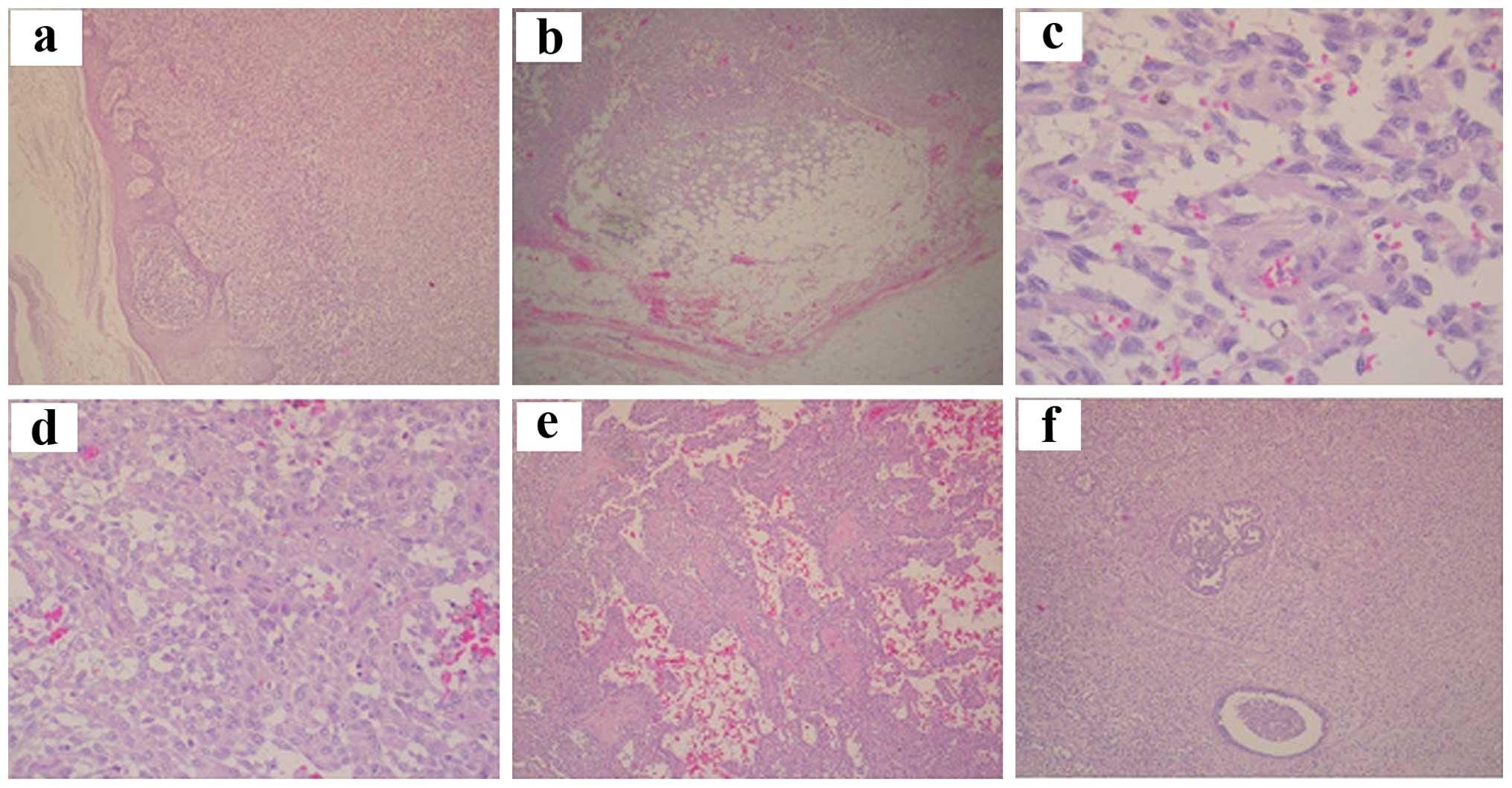
the surgical margins, as well as the nipple (Fig. 3a).
Histopathology
The microscopic examination revealed an invasive
proliferation (Fig. 3b) of
spindle-shaped/sarcomatoid cells (Fig.
3c), as well as epithelioid cells. The latter type exhibited
vesicular nuclei, prominent nucleoli, variable nuclear atypia and
eosinophilic cytoplasm (Fig. 3d). The
neoplastic cells were diffusely arranged in a reticular or
storiform pattern, with several cystically
dilated/pseudoangiomatous/alveolar spaces (Fig. 3e). The mitotic rate was up to 6
mitoses/10 high-power fields and the Ki-67 proliferation index was
~40%.
Extensive areas of necrosis and hemorrhage,
neoplastic infiltration of vessel walls, mild mixed inflammatory
infiltrate, as well as entrapment of normal breast tissue (ducts
and lobules) were detected within the tumor (Fig. 3f).
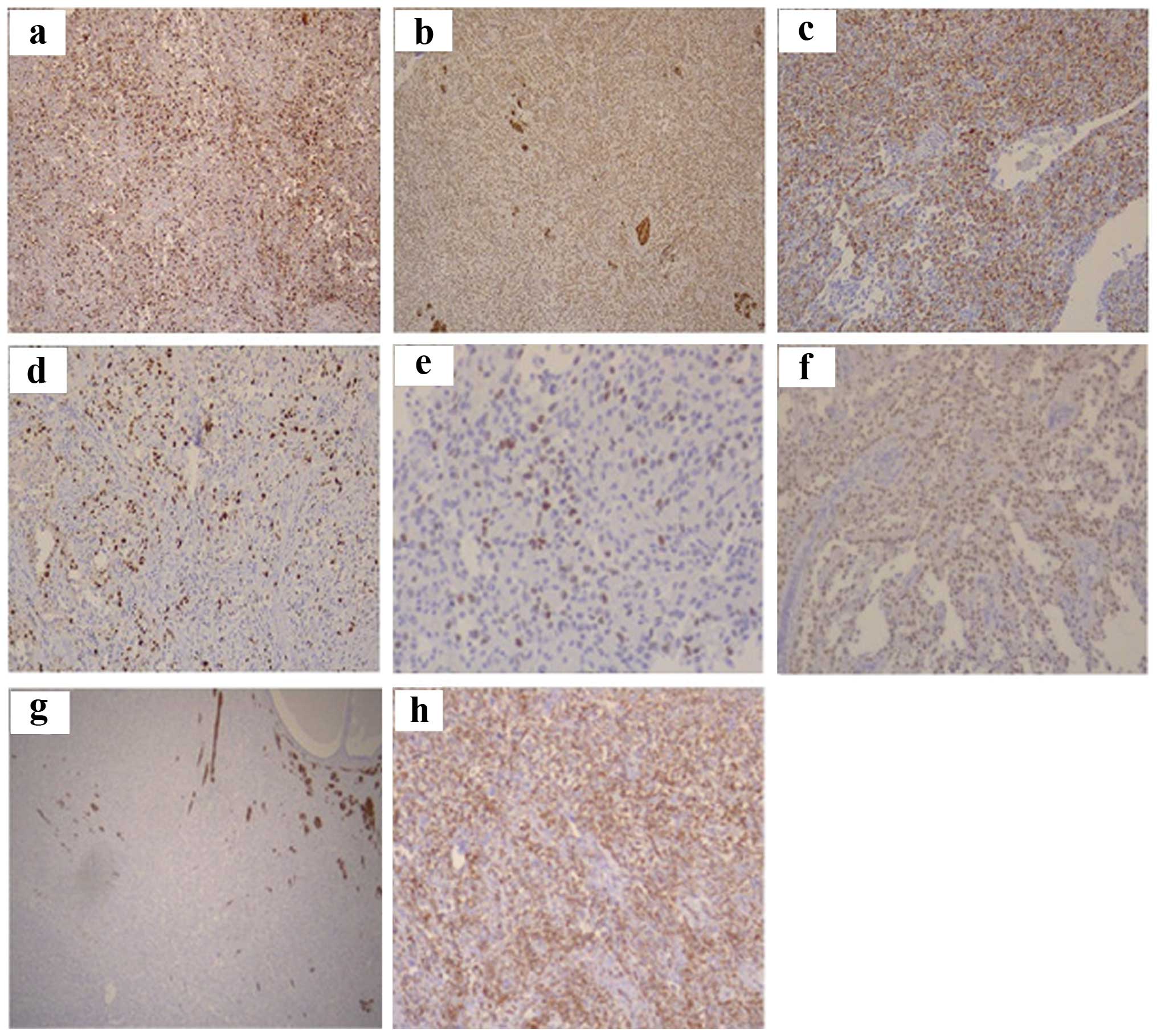
Immunohistochemistry (IHC)
IHC analysis for cytokeratin (CK)AE1-3, CK5/6, CK7,
CK14, CK8/18, CK20, epithelial membrane antigen, S-100, smooth
muscle actin (SMA), desmin, caldesmon, calponin, vimentin,
mammoglobulin, human gross cystic disease fluid protein-15,
estrogen receptor (ER), progesterone receptor (PR), MIB-1, p53,
p63, topoisomerase IIa, human epidermal growth factor receptor 2
(HER2), CD10, CD31, CD34 and CD99 was performed.
The tumor cells were immunoreactive for vimentin,
p63, p53, CD10, S-100, CK8/18 and CKAE1–3. Focal positivity for
caldesmon and desmin (focal myoid transformation) was also
observed. On the basis of the immunophenotype, the lesion was
finally diagnosed as malignant myoepithelioma (Fig. 4).
Discussion
Myoepithelial carcinomas of the breast are extremely
rare and represent a challenge in terms of diagnosis and treatment
(1,9,12). This
type of neoplasm occurs in women aged 25–81 years (mean, 54 years)
(9,11). The tumor size ranges between 1.4 and
17 cm (mean, 3.5 cm). The lesions are typically multinodular with
central necrosis. Cytologically, the tumors are composed of
epithelioid, plasmatocytoid and spindle cells (11–13).
In our case, the clinical manifestations (age 74
years and tumor size 16 cm), the macroscopic findings
(myltinodularity of the tumor with areas of central necrosis and
hemorrhage) and the microscopic examination (biphasic pattern of
growth with epithelioid and spindle cells entrapping normal breast
tissue) contributed to the diagnosis of malignant
myoepithelioma.
The contribution of the IHC results was key to
confirming the diagnosis. The neoplastic cells exhibited
immunoreactivity for markers indicative of myoepithelial
differentiation (p63, p53 and S-100) and focal positivity for
specific CKs (CK8/18, and CKAE1/AE3). The tumor cells also
exhibited focal myoid differentiation, particularly around terminal
ducts, which was highlighted by immunoreactivity for caldesmon and
desmin. The tumor was also triple-negative (negative staining for
ER, PR and HER2), with a Ki-67 proliferation index of ~40%.
Antibodies useful for detecting myoepithelial cells
are directed against CKs and myofilaments. Antibodies against
high-molecular weight CKs (CK5, CK5/6, CK14 and CK17) react in most
lesions (3). Strong nuclear p63 and
p53 immunostaining is observed, while S-100 is typically positive
(90%). There may be a positive reaction for muscle markers, such as
calponin (86%), muscle-specific actin, desmin (14%) and SMA (36%),
as well as for basement membrane proteins, type IV collagen and
laminin. Occasional cells exhibit immunostaining with glial
fibrillary acidic protein (GFAP) (5,7,9,11,14). All the tumors typically lack ER and PR
receptors and are mitotically active (14,15),
purely composed of myoepithelial cells. Myoid transformation is
most frequently encountered around terminal ducts and lobules, in
the absence of epithelial proliferation (7,8).
The differential diagnosis may be challenging,
particularly when it comes to spindle cell/metaplastic carcinomas
or the rare primary spindle cell sarcomas of the breast.
Occasionally, these tumors are almost impossible to differentiate
without IHC evaluation (7,14–16).
There remains controversy regarding whether
malignant myoepitheliomas and spindle cell carcinomas share the
same histogenesis, as both neoplasms exhibit a biphasic growth
pattern. It is hypothesized that both elements (mesenchymal and
epithelial) are derived from a common cell of origin or a
pluripotent stem cell, although this hypothesis has not yet been
confirmed (3,6,7). Despite
extensive sampling, concurrent presence of ordinary intraductal or
invasive ductal carcinoma or foci of other types of metaplastic
differentiation (e.g., squamoid, chondroid or osseous) were not
observed. These are common characteristics of metaplastic spindle
cell carcinomas. The diagnosis is further confirmed using
antibodies against CKs of variable molecular weight. Both types of
neoplasms express p63 and CK5, but the presence of smooth-muscle
markers and immunostaining for GFAP favors myoepithelial
differentiation. Metaplastic sarcomatoid carcinomas are usually
reactive for CK7, CK5/6, CK903 and CKAE1–3.
Primary spindle-cell sarcomas, such as fibrosarcomas
and dediferentiated liposarcomas, are generally not immunoreactive
for CKs. Leiomyosarcomas and rhabdomyosarcomas stain diffusely and
strongly positive with muscle markers, such as SMA, desmin and
caldesmon, or myoglobin, myogenin and myo-D1, respectively.
Fibromatosis should also be excluded prior to
confirming the diagnosis of myoepithelioma. Fibromatosis is a
well-recognized proliferation of myofibroblasts and fibroblasts
intermingled with abundant stromal collagen. Minimal pleomorphism
and the absence or minimal number of mitoses are indicative of the
benign nature of this lesion. Immunohistochemically, fibromatosis
often expresses actin, occasionally desmin and S-100, while CD34
and CKs are not expressed (6,7,14,15).
Other neoplasms that should be included in the
differential diagnosis are myofribroblastoma (usually negative for
CKs and S100 and positive for smooth muscle myosin-heavy chain and
CD34), solitary fibrous tumor, sclerosing adenosis with prominent
myoepithelial cells (usually in the elderly, associated with
atrophy of the epithelial component), melanoma, malignant fibrous
histiocytoma and malignant peripheral nerve sheath tumor (7,14,15).
Due to the rarity of myoepithelial carcinoma and the
limited data availability, very little is known on its biological
behavior and systemic treatment.
By the time the patient was admitted to our medical
center, she already had advanced-stage (IIIb) breast cancer with
inflammation/ulceration of the nipple and skin, involvement of the
chest wall and metastasis to axillary lymph nodes, but no distant
metastatic disease. Neoadjuvant chemotherapy with docetaxel,
doxorubicin and cyclophosphamide was administered for cytoreduction
in order to render the tumor operable. Chemotherapy not only proved
ineffective in that respect, but the CT scans also revealed
locoregional progression of the disease and the development of an
abscess in the tumor area. Therefore, a palliative simple
mastectomy was performed and further chemotherapy was scheduled to
treat the residual disease.
Taking into consideration the unresponsiveness of
the tumor to neoadjuvant therapy, there was an alteration of
regimens postoperatively. The patient was treated with paclitaxel,
carboplatin and bevacizumab. Despite the administration of
chemotherapy, a locoregional relapse occurred soon after surgery,
which emphasizes the agressiveness of the tumor and its resistance
to treatment.
Myoepithelial carcinoma has an aggressive course,
with locally invasive and widespread metastatic potential to
several organs, commonly the liver and lungs, and the tendency to
recur, even with clear resection margins. The treatment of choice
is surgical, namely wide tumor excision or mastectomy with regional
lymph node excision (5,10,17,18).
Adjuvant radiotherapy (1,19–21) or chemoradiation (22,23) are
often administered in order to minimize local recurrence.
The effectiveness of hormonal therapy is unknown
(4,9).
Since the tumor was triple-negative on IHC, which is characteristic
of malignant myoepitheliomas, we considered that hormonal therapy
would be of no benefit to the patient.
There are not sufficient data available to define
the role and effectiveness of first-line chemotherapy, although it
remains the only therapeutic choice in cases with distant
metastasis or recurrence disease. However, none of the regimens
used thus far have been proven effective (including carboplatin,
paclitaxel, doxorubicin, cyclophosphamide, gemcitabine and oral
capecitabine) (3). A
multidisciplinary treatment approach is recommended, taking into
account all the particularities of this rare type of cancer and its
ambiguous biological behavior.
Acknowledgements
The authors would like to thank Mr. Kostas P.
Karamoustos for his valuable support in connection with the
technical processing of all the photos which are included in this
project.
References
|
1
|
Liao KC, Lee WY and Chen MJ: Myoepithelial
carcinoma: A rare neoplasm of the breast. Breast Care (Basel).
5:246–249. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ahmed A: The myoepithelium in human breast
carcinoma. J Pathol. 113:129–135. 1974. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Endo Y, Sugiura H, Yamashita H, Takahashi
S, Yoshimoto N, Iwasa M, Asano T and Toyama T: Myoepithelial
carcinoma of the breast treated with surgery and chemotherapy. Case
Rep Oncol Med. 2013:1647612013.PubMed/NCBI
|
|
4
|
Lakhani SR, O'Hare MJ, Monaghan P,
Winehouse J, Gazet JC and Sloane JP: Malignant myoepithelioma
(myoepithelial carcinoma) of the breast: A detailed cytokeratin
study. J Clin Pathol. 48:164–167. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Liang YF, Zeng JC, Ruan JB, Kang DP, Wang
LM, Chen C, Xu JF and Wu QL: Malignant myoepithelioma of the
breast: A case report and review of literature. Int J Clin Exp
Pathol. 7:2654–2657. 2014.PubMed/NCBI
|
|
6
|
Tavassoli FA: Pathology of the Breast
(2nd). Appleton and Lange. Stamford, CT: 763–791. 1999.
|
|
7
|
Hoda SA, Brogi E, Koernen FC and Rosen PP:
Rosen's Breast Pathology (4th). Lippincott Williams & Wilkins.
Philadelphia, PA: 174–180. 2014.
|
|
8
|
Lakhani SR, Ellis IO, Schnitt SJ, Tan PH
and van de Vijrer MJ: WHO Classification of Tumours of the Breast.
IARC Press. Lyon, France: 120–123. 2012.
|
|
9
|
Suguna BV, Geethamani V, Niveditha SR and
Monika LS: Malignant myoepithelioma of the breast: Case report with
review of literature. Malaysian J Pathol. 33:125–128. 2011.
|
|
10
|
Poret H, Cormier B, Marret H, Body G and
Ouldamer L: Malignant myoepithelial breast carcinoma: Diagnosis and
therapeutic difficulties. Gynecol Obstet Fertil. 41:334–337. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Fayaz S, Samir S, Amanguno H, El-Sherify
M, Adesina A, Abozlouf S, George T, Attia G, Eissa H and Bedair A:
Myoepithelioma (myoepithelial carcinoma) of the breast: Case
reports. Austral-Asian Journal of Cancer. 12:7–12. 2013.
|
|
12
|
Enghardt MH and Hale JH: An epithelial and
spindle cell breast tumour of myoepithelial origin. An
immunohistochemical and ultrastructural study. Virchows Arch A
Pathol Anat Histopathol. 416:177–184. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Lingamfelter D, Chen Y, Kure K and
Lankachandra K: Infiltrating myoepithelial carcinoma of the breast,
a case report and cytologic-histologic correlation. Diagnostic
Pathology. 3:72008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Dabbs DJ: Breast Pathology (1st). Elsevier
Saunders. Philadelphia, PA: 307–318, 479–490. 2012.
|
|
15
|
Dabbs DJ: Diagnostic Immunohistochemistry:
Theranostic and Genomic Application (3rd). Saunders Elsevier.
Philadelphia, PA: 102–109, 783–785. 2010.
|
|
16
|
Gattuso P, Reddy VB and Odile D:
Differential Diagnosis in Surgical Pathology: Expert Consult-Online
and print. 2e. (2nd). Saunders. 2009.
|
|
17
|
Khattech R, Ben Othman M, Ben Romdhane K,
Gamoudi A and Ammar A: Breast myoepithelioma. Report of a case. Ann
Pathol. 15:138–141. 1995.(In French). PubMed/NCBI
|
|
18
|
Brasseur P, Hustin J and Collard M: Breast
tumor with myoepithelial cells. Apropos of a case report. J Belge
Radiol. 73:197–200. 1990.(In French). PubMed/NCBI
|
|
19
|
Scarpellini F, Usellini L and Foschini MP:
Malignant myoepithelioma associated with in situ and invasive
ductal carcinoma. Description of a case and review of the
literature. Pathologica. 89:420–424. 1997.(In Italian). PubMed/NCBI
|
|
20
|
Loose JH, Patchefsky AS, Hollander IJ,
Lavin LS, Cooper HS and Katz SM: Adenomyoepithelioma of the breast.
A spectrum of biologic behavior. Am J Surg Pathol. 16:168–876.
1992. View Article : Google Scholar
|
|
21
|
Fang ZM, Tse RV, Marjoniemi VM, Kozlov S,
Lavin MF, Chen H, Kearsley JH, Graham PH and Clarke RA:
Radioresistant malignant myoepithelioma of the breast with high
level of ataxia telangiectasia mutated protein. J Med Imaging
Radiat Oncol. 53:234–239. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Terada T: Malignant myoepithelioma of the
breast. Pathol Int. 61:99–103. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Trepp R, Padberg BC, Varga Z, Cathomas R,
Inauen R and Reinhart WH: Extensive extranodal metastases of
basal-like breast cancer with predominant myoepithelial spindle
cell differentiation. Pathol Res Pract. 206:334–337. 2010.
View Article : Google Scholar : PubMed/NCBI
|