Introduction
Hilar cholangiocarcinoma (HCCA), which comprises
~50% of all malignant bile duct tumors, is a type of cancer that is
difficult to treat (1). Surgical
resection is the only potentially curative treatment for HCCA,
although it fails to reduce the recurrence rate. A previous report
has revealed that the HCCA recurrence rate following primary
curative resection was up to 50–75% (2). The locoregional areas that are usually
regarded as the main recurrent sites have also been documented in
the literature (3), and contrary to
the locoregional recurrence following radical resection, very few
reports regarding isolated brain metastases prior to locoregional
recurrence are available. The present case study describes a
patient with HCCA who underwent curative resection, and experienced
isolated brain metastases prior to locoregional recurrence.
Case report
A 63-year-old female patient with a 2 weeks' history
of intermittent epigastric pain was admitted to the Sun Yat-sen
Memorial Hospital, Sun Yat-sen University, Guangzhou, China. A
physical examination did not reveal any neurological symptoms, and
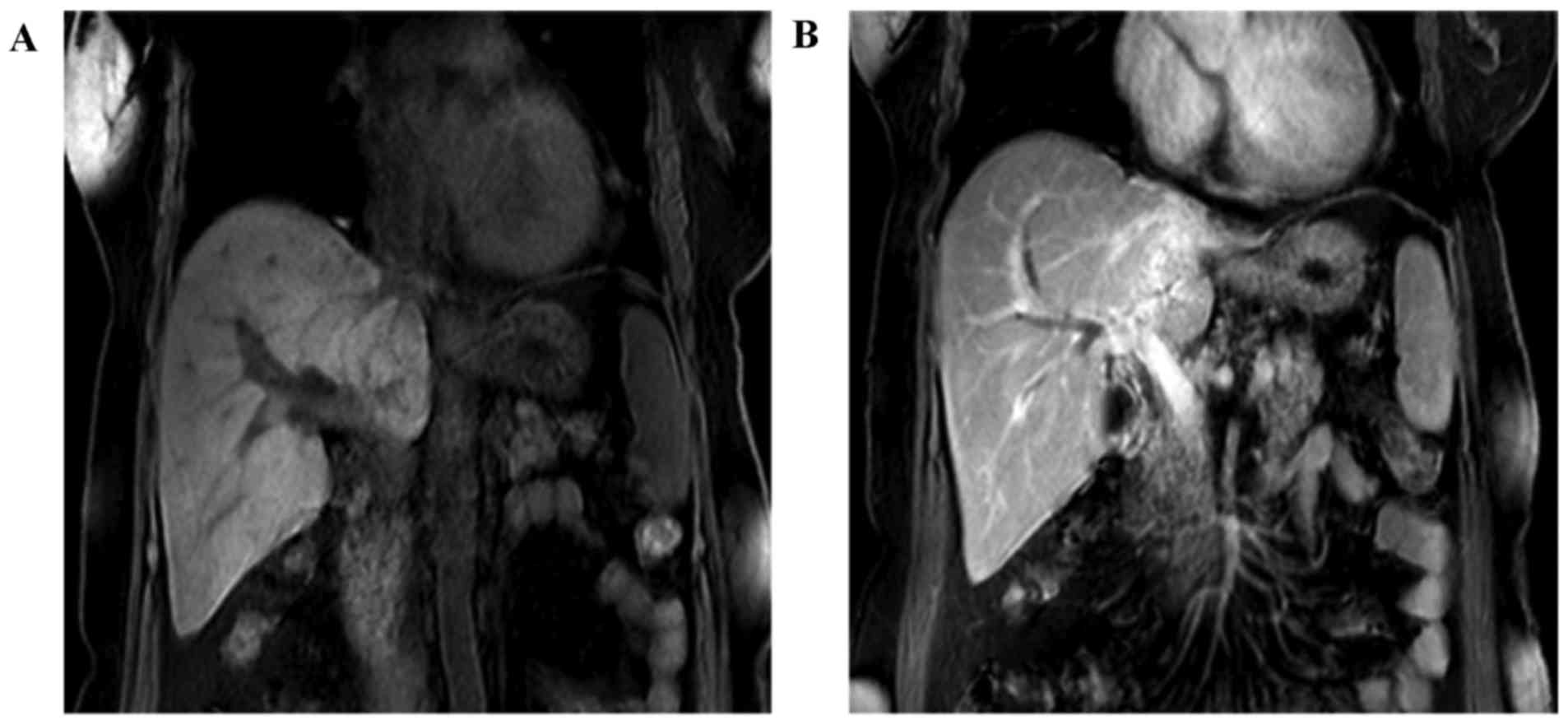
the patient denied having any associated medical history. An
magnetic resonance imaging (MRI) scan of the abdomen revealed that
the left bile duct was replaced with a mass, and the intrahepatic
biliary duct was dilated; furthermore, the left branch of the
portal vein had been invaded (Fig.
1). Simultaneously, a laboratory examination revealed a level
of the tumor marker, carcinoembryonic antigen (CEA), of 6.3 ng/ml
(normal value, ≤5 ng/ml), and a cancer antigen 19-9 (CA19-9)
concentration of 316 U/ml, as well as a moderately increased
concentration of serum total bilirubin.
A curative resection procedure of left hepatectomy
with caudate lobectomy and Roux-en-Y bilioenteric anastomosis to
re-establish biliary continuity were performed for this patient,
with a clinical diagnosis of HCCA being made 7 days later. The
patient was intraoperatively diagnosed with type IIIB HCCA,
according to the Bismuth-Corlette classification system (4). Ultimately, R0 resection was achieved
with negative hepatic margin and bile duct margin, confirmed by
pathological examination postoperatively. None of 15 harvested
lymph nodes were identified as positive. Finally, the pathological
diagnosis of HCCA for this patient [according to the
tumor-nodes-metastasis (TNM) system] was stage II, T2bN0M0, with
well-differentiated adenocarcinoma. According to the National
Comprehensive Cancer Network® (NCCN®)
guidelines (5), patients with HCCA
following curative resection may be free from adjuvant chemotherapy
or radiotherapy. Therefore, the patient did not receive any
postoperative adjuvant chemotherapy or radiation, although the
present authors conformed with the appropriate follow-up schedules.
The patient was released from hospital 2 weeks postoperatively.
During the following-up, the level of the biomarker,
CEA, was determined to be 3.2 ng/ml and the CA19-9 concentration
was 32.6 U/ml 3 months after the initial radical surgery, which
suggested that the patient was disease-free and that no tumor
recurrence activity had been identified. The patient remained alive
for 14 months without any tumors, and neither abdominal computed
tomography (CT) nor a laboratory examination revealed any sign of
tumor recurrence. Subsequently, the patient felt weakness of the
right upper extremity and presented with mildly epigastric
distention, as well as nausea, 15 months after the initial surgery.
Therefore, the patient was readmitted to the Sun Yat-sen Memorial
Hospital, Sun Yat-sen University, Guangzhou, China. A physical
examination was unremarkable. Laboratory tests revealed that the
level of aminotransferase was moderately increased, the level of
CEA was 9.2 ng/ml, and the concentration of CA 19-9 was 207 U/ml.
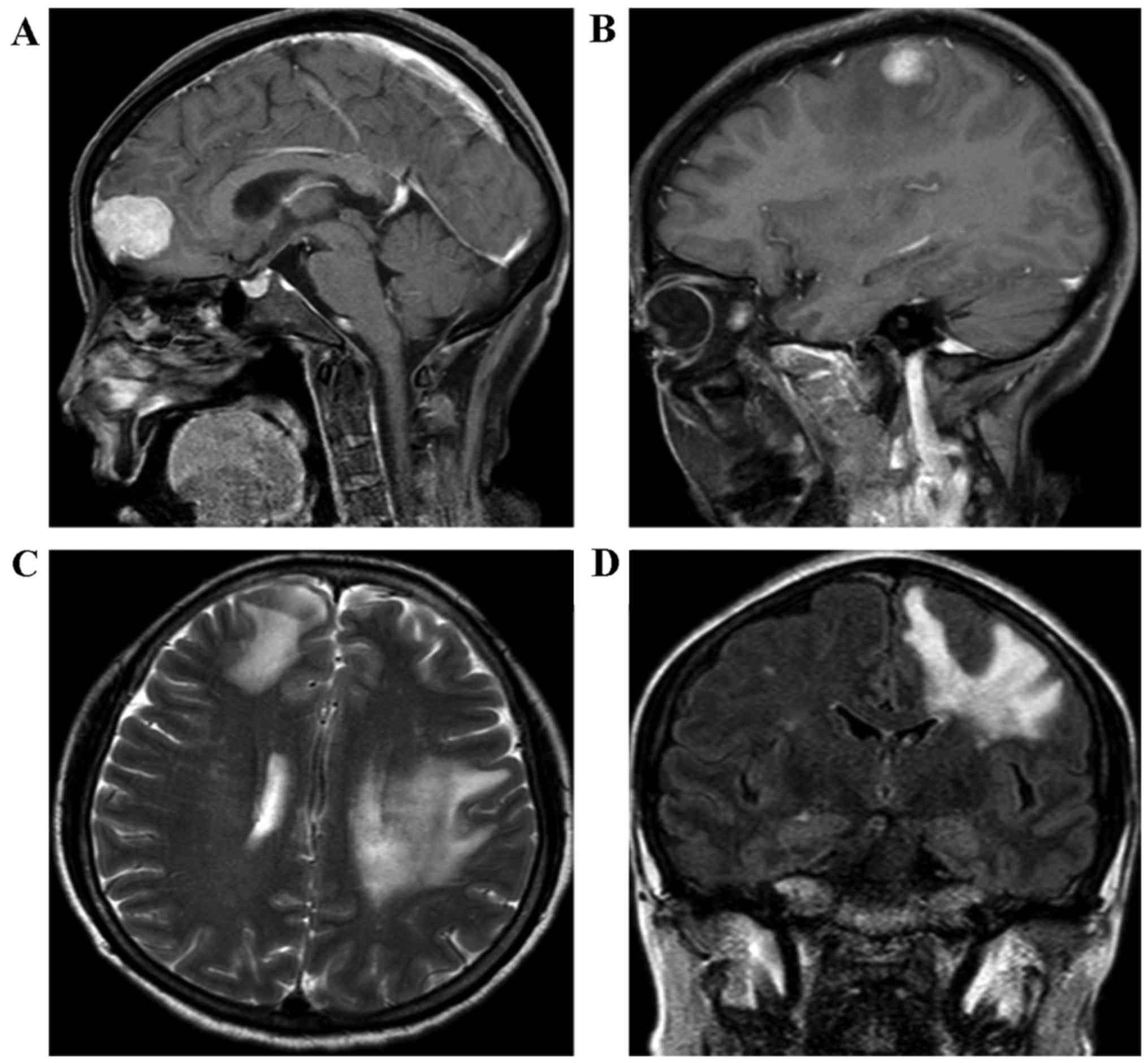
Furthermore, the cerebral MRI displayed enhancing lesions of the
right subcortical frontal lobe and the left subcortical parietal
cortex lobe (Fig. 2). It was clearly
indicated that these small tumor entities were surrounded with
flaky edema (Fig. 2B-D), which is a
feature of metastatic encephaloma. Our multidisciplinary team
discussed the presentation of the cerebral MRI images, and the
radiologist and neurosurgeon considered that they were consistent
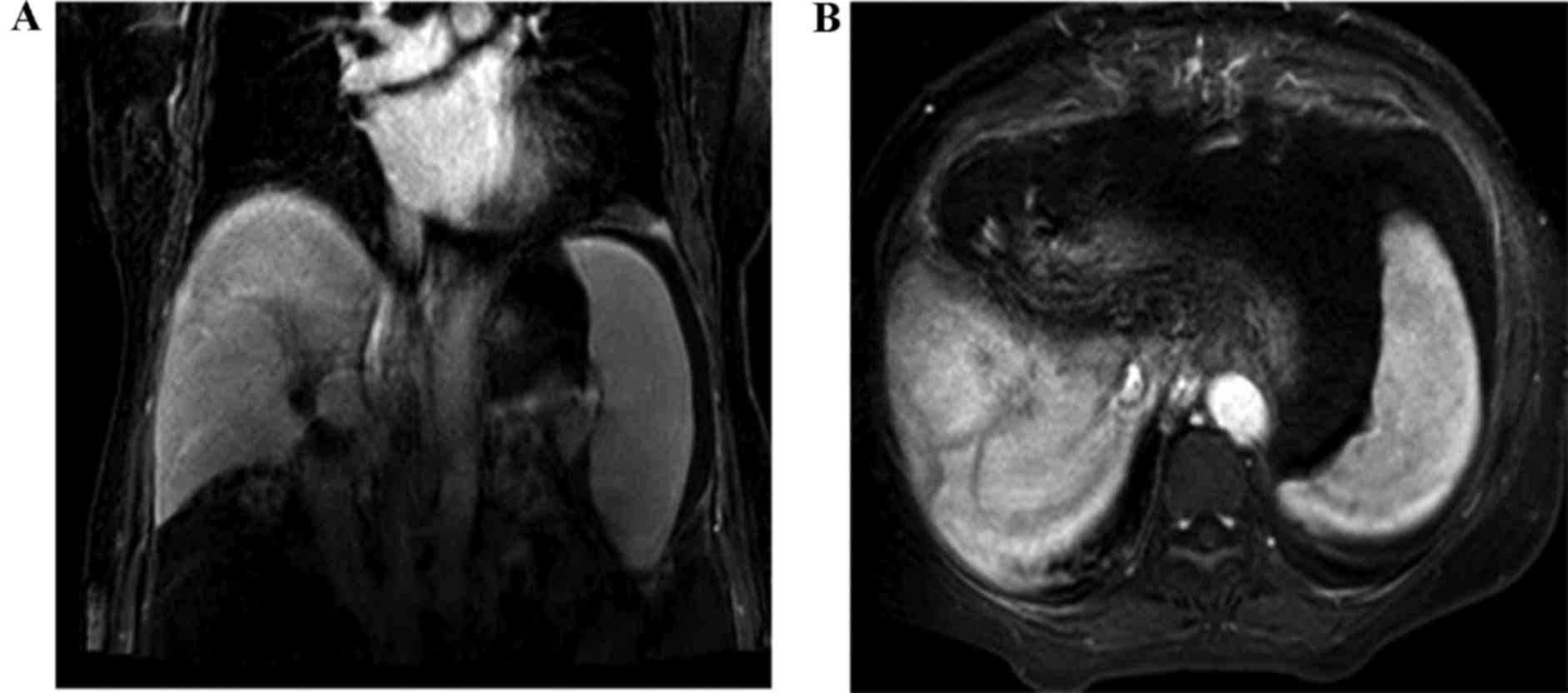
with metastatic tumors, rather than a primary tumor of brain. At
the same time, neither tumor recurrence nor locoregional lymph
nodes metastasis was detected in the abdomen using contrasted CT
(Fig. 3). A neurosurgeon was
consulted for possible biopsy prior to chemotherapy or
radiotherapy, but the patient refused to accept any further medical
therapy. She died suddenly from a brain hernia due to progression
of brain metastasis 2 months after the isolated brain
metastasis.
Discussion
Brain metastases, with an incidence of ~5%, usually
occurs in patients with primary carcinoma, including breast cancer,
lung cancer, and melanoma (6,7).
Regarding the brain metastases from HCCA, only a few cases with
brain metastases can be located in the previous literature, which
is predominantly associated with intrahepatic cholangiocarcinoma
(ICC) rather than HCCA (6,8,9).
Surgical resection is the only potential curative
option for HCCA. However, the recurrence rate following primary
curative resection is currently at the level of 50–75% (2). At the same time, the main recurrent
sites are predominantly located in locoregional areas, such as the
hepatic resection margin, bilioenteric anastomosis, and porta
hepatis (3). Non-hematogenous spread
to distant organs is a rare phenomenon, particularly in the brain.
In a recent study from Thailand, brain metastases occurred in 0.15%
(8 out of 5,164) of patients with cholangiocarcinoma, but only 2
were patients with HCCA (10).
Additionally, cholangiocarcinoma is known to be a poorly
vascularized carcinoma that originates from the biliary tree, which
may account for the rare occurrence of brain metastases in
HCCA.
Although, in the present case study, the diagnosis
of isolated brain metastases was a clinical diagnosis made without
biopsy due to the refusal of the patient, it was observed that the
CEA concentration of 9.2 ng/ml (normal concentration, ≤5 ng/ml) and
the CA19-9 concentration of 207 U/ml (normal, ≤34 U/ml) were
markedly abnormal. Comparing these values with the CEA level of 3.2
ng/ml and the CA19-9 level of 32.6 U/ml recorded 3 months after
radical surgery, this suggested that HCCA recurrence had occurred
to a large extent. Furthermore, the additional primary tumor of the
alimentary tract was excluded on the basis of past history and
abdominal image workup. Importantly, multiple lesions, but not only
one tumor entity, were detected by the brain MRI scan. In addition,
these small tumor entities were surrounded with clearly flaky edema
(Fig. 2B-D), which is a feature of
metastatic encephaloma.
To differentiate brain metastasis from the
recurrence of HCCA is challenging, particularly in the early
stages, since neurological findings of brain metastasis were occult
and subtle. Indeed, in this case, no remarkable sign was observed
until 15 months postoperatively, when the patient developed
weakness of the upper extremity. Although MRI scans may help in
detection of the cerebral lesion, it is not a routine workup for
HCCA during postoperative follow-up. Furthermore,
hepatopancreatobiliary practitioners tend to focus on examinations
of the abdominal CT and laboratory tests to detect regular
recurrence sites of HCCA postoperatively, which may miss other
potential solitary recurrence sites. Furthermore, to the best of
our knowledge, the median survival time of brain metastasis from
ICC is dismal, even after having performed whole-brain radiotherapy
or chemotherapy (6,9,10).
However, a similar outcome of isolated brain metastasis in HCCA
following curative resection is not available. It must be admitted
that our case presented a poor prognosis. Hence, early diagnosis
and an associated aggressive treatment might be necessary in order
to prevent irreversible neurological deficits, and to stabilize the
neurological status to a certain extent.
In conclusion, isolated brain metastases prior to
locoregional recurrence in HCCA following curative surgery is a
fatal complication that occurs extremely rarely. Clinicians are
supposed to keep their minds open and focus on the neurological
symptoms, such as motor weakness, or alteration of consciousness.
It is indispensable that any patient with HCCA who has undergone
radical resection surgery, and subsequently presented with a
further onset of neurological symptoms, should be evaluated for
brain involvement (11).
Acknowledgements
The present study was supported by the ‘Young Stuff’
foundation of Sun Yat-Sen University (grant no. 15ykpy20) the Key
Laboratory of Malignant Tumor Mechanism and Translational Medicine
of Guangzhou Bureau of Science and Information Technology (grant
no. [2013] 163), and the Key Laboratory of Malignant Tumor Gene
Regulation and Target Therapy of Guangdong Higher Education
Institutes (grant no. KLB 09001).
References
|
1
|
Khan SA, Davidson BR, Goldin RD, Heaton N,
Karani J, Pereira SP, Rosenberg WM, Tait P, Taylor-Robinson SD,
Thillainayagam AV, et al: Guidelines for the diagnosis and
treatment of cholangiocarcinoma: An update. Gut. 61:1657–1669.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Jang JY, Kim SW, Park DJ, Ahn YJ, Yoon YS,
Choi MG, Suh KS, Lee KU and Park YH: Actual long-term outcome of
extrahepatic bile duct cancer after surgical resection. Ann Surg.
241:77–84. 2005.PubMed/NCBI
|
|
3
|
Jarnagin WR, Ruo L, Little SA, Klimstra D,
D'Angelica M, DeMatteo RP, Wagman R, Blumgart LH and Fong Y:
Patterns of initial disease recurrence after resection of
gallbladder carcinoma and hilar cholangiocarcinoma: Implications
for adjuvant therapeutic strategies. Cancer. 98:1689–1700. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Bismuth H and Corlette MB: Intrahepatic
cholangioenteric anastomosis in carcinoma of the hilus of the
liver. Surg Gynecol Obstet. 140:170–178. 1975.PubMed/NCBI
|
|
5
|
National Comprehensive Cancer Network.
(NCCN), . Clinical Practice Guidelines in Oncology. Hepatobiliary
Cancer. (Version 2. 2016). https://www.nccn.org/professionals/physician_gls/f_guidelines.aspJune
27–2016
|
|
6
|
William BM and Grem JL: Brain metastasis
and leptomeningeal carcinomatosis in a patient with
cholangiocarcinoma. Gastrointest Cancer Res. 4:144–145.
2011.PubMed/NCBI
|
|
7
|
Pan Z, Yang G, Yuan T, Pang X, Wang Y, Qu
L and Dong L: Leptomeningeal metastasis from hepatocellular
carcinoma with other unusual metastases: A case report. BMC Cancer.
14:3992014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Huffman JL, Yeatman TJ and Smith JB:
Leptomeningial Carcinomatosis: A sequela of Cholangiocarcinoma. Am
Surg. 63:310–313. 1997.PubMed/NCBI
|
|
9
|
Jacobs RE, McNeill K, Volpicelli FM,
Warltier K, Iturrate E, Okamura C, Adler N, Smith J, Sigmund A,
Mednick A, et al: Treatment of leptomeningeal carcinomatosis in a
patient with metastatic cholangiocarcinoma. ACG Case Rep J.
2:39–41. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Chindaprasirt J, Sookprasert A,
Sawanyawisuth K, Limpawattana P and Tiamkao S: Brain metastases
from cholangiocarcinoma: A first case series in Thailand. Asian Pac
J Cancer Prev. 13:1995–1997. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Mirrakhimov AE, Nwankwo N, Zdunek T and
Bucher N: Cholangiocarcinoma and brain lesions: An extremely rare
finding. BMJ Case Rep: bcr2013009235. 2013. View Article : Google Scholar
|