Introduction
Multiple primary malignancies (MPMs) are defined as
more than two primary cancers detected in an individual patient.
The classic criteria for the diagnosis of a second primary
malignancy were proposed by Warren and Gates in 1932 and include
(i) histologic confirmation of malignancy in both the index and
secondary tumor; (ii) the two malignancies must be anatomically
separated by normal mucosa; and (iii) the possibility of the second
primary malignancy being a metastasis from the index tumor must be
excluded. MPMs can be classified as either synchronous or
metachronous based on their timing of diagnosis (1). According to the Surveillance,
Epidemiology, and End Results Program Coding and Staging Manual
2004, synchronous tumors are defined as multiple tumors diagnosed
within 2 months of the original/initial diagnosis, and metachronous
tumors are multiple tumors or lesions that occur more than 2 months
after the original/initial diagnosis (2).
Recent progress in diagnostic techniques and
treatment modalities has improved the outcomes of each organ
malignancy and resulted in an increase in the number of patients
diagnosed with multiple primary malignancies during long-term
follow-up (3). Consequently, the
risk of developing MPMs is a common problem for cancer survivors.
We report a rare case involving a patient with malignancies of
three histological types in six different organs, namely
adenocarcinoma (AC) of the stomach, prostate, colon, pancreas; a
urothelial carcinoma (UC) of the urinary bladder; and a squamous
cell carcinoma (SCC) of the facial skin.
Case report
A 79-year-old male was referred to our hospital for
further evaluation of a pancreatic mass on January 2014. He drank a
glass of shochu (20 grams of alcohol) a day for 50 years and smoked
20 cigarettes a day for 30 years until he stopped smoking in 2004.
His father was diagnosed with lung cancer and his mother was
diagnosed with pancreatic cancer.
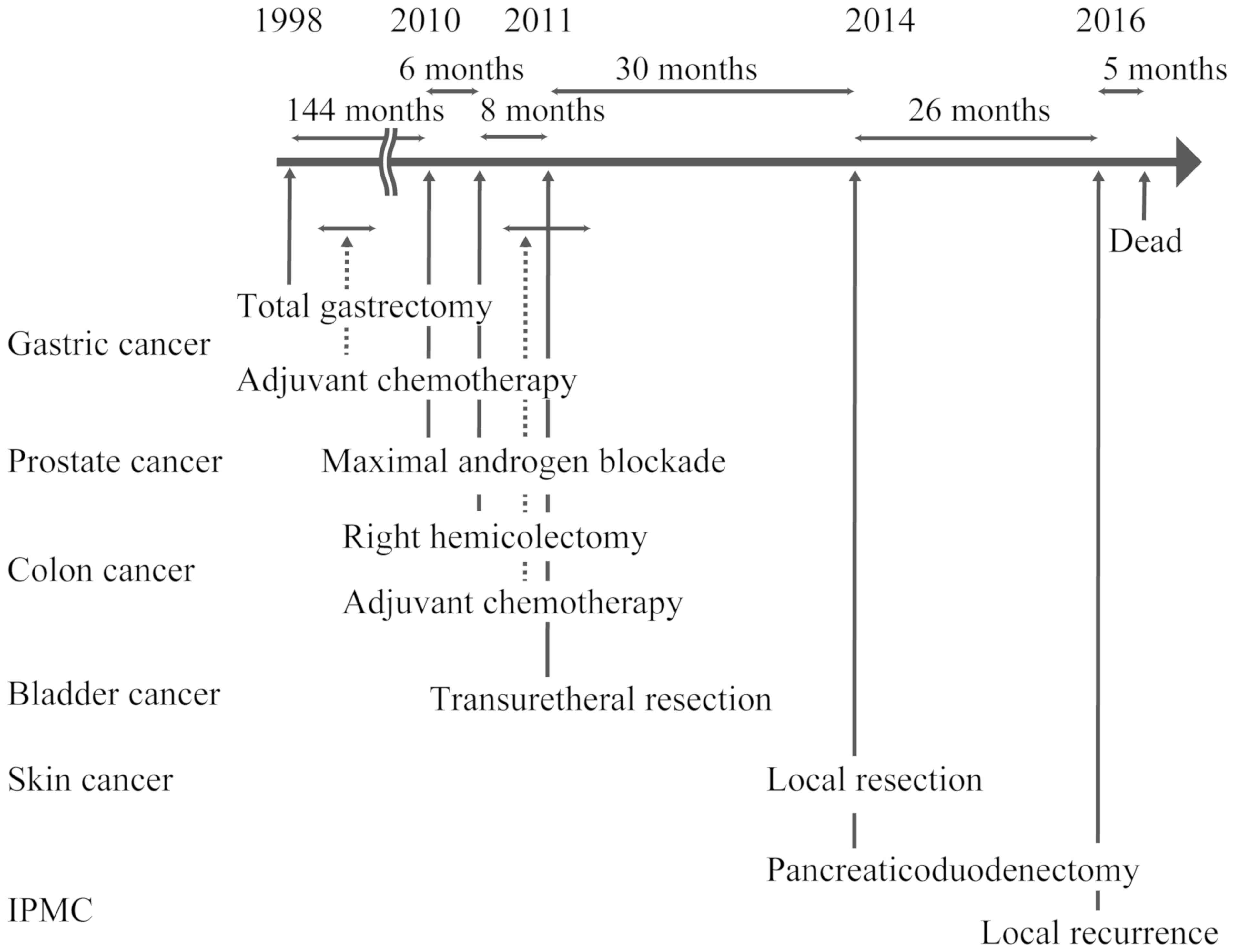
In March 1998 he was diagnosed with upper gastric
cancer and underwent a total gastrectomy and splenectomy with D2
lymph node dissection at a nearby hospital at the age of 63. The
pathological diagnosis was moderately differentiated AC, pT3N0M0
(stage IIA), according to the UICC TNM classification, 7th edition.
Adjuvant chemotherapy was performed with mitomycin C and oral
uracil/tegafur for 18 months. In March 2010 he underwent prostate
cancer screening and was diagnosed with adenocarcinoma of the
prostate with Gleason score 5+5, according to the Gleason grading
system. He was treated with maximum androgen blockade therapy. In
November 2010, stenotic ascending colon cancer was detected by
colonoscopy performed at the previous hospital. He underwent right
hemicolectomy with D3 lymph node dissection. The pathological
finding was well differentiated AC, pT3N0M0, stage IIA, according
to the UICC TNM classification, 7th edition. As the tumor was large
(40 mm) and stenotic, he was administered adjuvant chemotherapy
with oral uracil/tegafur and oral leucovorin for 1 year. In July
2011, cystoscopy revealed a bladder tumor and the patient underwent
transurethral resection of bladder tumor in August 2011. The
pathological finding was UC of the urinary bladder, high-grade,
pTisN0M0 (stage 0), according to the UICC TNM classification, 7th
edition. In January 2014 he noticed a mass on his right cheek.
Dermatologists resected that mass completely. The pathological
finding was a squamous cell skin cancer of right cheek, pT1N0M0
(stage I), according to the UICC TNM classification, 7th edition.
An abdominal CT scan in January 2014 for follow-up after colon
cancer treatment revealed dilatation of the tortuous pancreatic
duct and a 10-mm tumor at the pancreatic head. Although he had no
symptoms, the tumor was suspected to be intraductal papillary
mucinous neoplasm (IPMN). He was referred to our hospital for
further investigation and treatment. Endoscopic retrograde
cholangiopancreatography and cytology were performed and he was
diagnosed with intraductal papillary mucinous carcinoma (IPMC). We
performed pancreaticoduodenectomy with D1 lymph node dissection.
The pathological finding was IPMC of the main pancreatic duct in
pancreas head, well differentiated, pT1, N0, M0 (stage IA),
according to the UICC TNM classification, 7th edition. After the
surgery follow-up was conducted by an abdominal CT scan performed
every 6 months and local recurrence of IPMC appeared in March 2016.
After receiving best supportive care, he died of cancer in August
2016.
The six primary malignancies are listed in
chronological order in Table I, and
the schema of this patient time course is described on Fig. 1.
 | Table I.List of malignancies in the present
patient. |
Table I.
List of malignancies in the present
patient.
|
|
|
| TNM Staging |
|
|
|---|
|
|
|
|
|
|
|
|---|
| Month and year | Organ | Histology | T | N | M | UICC stage | Treatment |
|---|
| March 1998 | Stomach | Tubular
adenocarcinoma | 3 | 0 | 0 | IIA | Total gastrectomy
Adjuvant chemotherapy |
| March 2010 | Prostate | Poorly differentiated
adenocarcinoma | 1c | 0 | 0 | I | MAB |
| November 2010 | Colon | Tubular
adenocarcinoma | 3 | 0 | 0 | IIA | Right hemicolectomy
Adjuvant chemotherapy |
| July 2011 | Bladder | UC | Tis | 0 | 0 | 0 | TURBT |
| January 2014 | Skin | SCC | 1 | 0 | 0 | I | Resection |
| January 2014 | Pancreas | IPMC | 1 | 0 | 0 | IA |
Pancreaticoduodenectomy |
Discussion
The case presented here is exceedingly rare in view
of the number of primary malignancies and their combination. We
found only 13 papers that reported multiple malignancies of five or
six different organs from a search of PubMed and the Japan Medical
Abstracts Society databases (Table
II) (4–10). Besides, we could not find any reports
of this particular combination of MPMs to date. Nine cases were
reported from Japan and 4 cases were from other countries. There is
no difference between Japanese and worldwide MPMs cases, e.g. age,
sex, organs.
| Table II.Previous studies of multiple primary
malignancies occurring in five or six different organs. |
Table II.
Previous studies of multiple primary
malignancies occurring in five or six different organs.
| Author, year | Country | Age | Sex | Organs, listed
chronologically | Family history | Prognosis | Refs. |
|---|
| Jones, 1976 | UK | 37 | M | Duo, Sma, Kid, Col,
Pan | Unknown | Unknown | (4) |
| Uchida et
al, 1987 | Japan | 62 | F | Eso, Lym, Ute, Sto,
Ora, Pha | No | Unknown | – |
| Sommers et
al, 1988 | USA | 57 | F | Skin, Col, Kid,
Ova, Ute | Unknown | Unknown | (5) |
| Hashimoto et
al, 1997 | Japan | 59 | M | Rec, Bla, Sto, Col,
Liv, Lung | Unknown | Unknown | – |
| Martin-Granizo
et al, 1997 | Spain | 61 | F | Lar, Bla, Pro, Ora,
Ton | Unknown | Alive | (6) |
| Yakushiji et
al, 1999 | Japan | 71 | M | Rec, Bla, Sto, Col,
Liv, Lung | Yes | Alive | (7) |
| Moriyama et
al, 2008 | Japan | 76 | F | Sto, Kid, Bla, Rec,
Col, Sma | Yes | Alive | – |
| Watanabe et
al, 2008 | Japan | 80 | F | Col, Ute, Duo, Sto,
Mam, Sma | Yes | Unknown | – |
| Cercato et
al, 2008 | Italy | 75 | F | Ute, Thy, Rec, Col,
Bro | Unknown | Alive | (8) |
| Komiyama et
al, 2012 | Japan | 46 | F | Ova, Ute, Col, Rec,
Lung | Yes | Alive | (9) |
| Mukaiyama et
al, 2014 | Japan | 58 | M | Glo, Kid, Bla, Ora,
Pro, Eso | No | Dead | (10) |
| Murakami et
al, 2014 | Japan | 73 | M | Lar, Eso, Sto, Pro,
Pha, Lung | Unknown | Alive | – |
| Hashimoto et
al, 2014 | Japan | 60 | M | Eso, Sto, Glo, Sma,
Col, Lung | No | Alive | – |
| Present case,
2018 | Japan | 79 | M | Sto, Pro, Col, Bla,
Skin, Pan | No | Dead |
|
Demandante et al (11) reviewed 1,104,269 cancer patients in
the literature and reported that the prevalence of multiple primary
malignant neoplasms ranges between 0.734 and 11.7%. They stated
that multiple primary malignant neoplasms might occur more
frequently than expected by random chance. They also noted that the
incidence of developing MPMs increased with increasing age
(11). The precise risk of MPMs in
Japan is unknown. Tabuchi et al reported that metachronous
second primary cancers developed in 3.8% of cancer patients after a
median follow-up of 2.5 years and the 10-year cumulative risk was
estimated as 13.0% for those who first developed cancer at 60–69
years of age (12).
It is difficult to estimate the risk of sextuple
cancers. However, several investigators have reported patients with
MPMs for each type of cancer. We previously reported that MPMs at
extracolonic sites were identified in 117 of 1,111 patients (10.5%)
with colorectal cancer (CRC) and that gastric cancer had the
highest incidence (44.4%, 52 of 117) among all MPMs. The rarest
combination was that of CRC and skin cancer, which was found in
only 1 of 117 patients with MPMs (3). For patients with gastric cancer,
Takeuchi et al (13) reported
that MPMs were observed in 109 patients (25.1%): 40 (9.2%) with
synchronous and 76 (18.2%) with metachronous MPMs. The most common
malignancy was colorectal cancer (22.8%). These data seem to
suggest that CRC and gastric cancer share common risk factors. In a
previous study, microsatellite instability (14), translocation of TP53 (15,16), and
ageing (17,18) were identified as shared risk factors
between CRC and gastric cancer. Cercato et al reported that
most MPMs arise in the respiratory, gastrointestinal, and
genitourinary systems and one of the most common malignancies is
prostate cancer (33–64% of all MPMs in a male patient series)
(8). Regarding IPMN, it has been
generally accepted that patients with IPMN have an increased risk
for MPMs (19,20). We previously reported the
relationship between IPMN and MPMs, showing that MPMs were more
frequent in patients with malignant (50.0%) IPMNs than in those
with benign disease (21.6%). We suggested that IPMNs, especially
malignant IPMNs, have an increased risk for the development of
neoplastic disease (21).
Powell et al (22) studied the prognosis of patients with
synchronous MPMs and metachronous MPMs. The median survival time
was 49 months in the synchronous group compared with 115 months in
the metachronous group (adjusted hazard ratio 0.50, p<0.001).
This is somewhat expected, as incidental malignancies found on
imaging studies such as those used for staging are often in an
earlier stage (22). In the present
case, the patient unfortunately had a recurrence of IPMC despite
metachronous malignancies.
Several factors affect the etiology of MPMs,
including lifestyle (e.g., tobacco, alcohol, diet), environment
(e.g., contaminants, occupation), and host factors (e.g., genetics,
immune function, hormonal interactions) (23). Tobacco smoking is one of the major
causes of multiple primary malignancies, with strong
well-established associations with tumors of the lung, oral cavity,
pharynx, nasal cavity, larynx, esophagus, stomach, pancreas,
colorectum, liver, kidney, ureter, urinary bladder, uterine cervix,
and ovary, and myeloid leukemia (24). Patients who continue to smoke after
development of a first smoking-related primary cancer have a
substantially increased risk of developing smoking-related
secondary primary cancers (25).
Alcohol intake has been implicated as one of the causes of upper
aerodigestive tract cancers such as tumors of liver, breast, and
colorectum (26). Moreover,
synergistic effects of tobacco and alcohol exist for upper
aerodigestive tract cancers (23,27). In
the present case, smoking might be associated with the incidence of
colon cancer, bladder cancer and IPMN. Similarly, alcohol
consumption may have contributed to increase the risk of acquiring
colon cancer.
We also should take into account genetic factors
that contribute to diseases, such as Lynch syndrome. The incidence
of MPMs has been reported to be high in patients with Lynch
syndrome. However, previous studies have suggested that the
frequency of Lynch syndrome in Japan is low, ranging from 0.15 to
0.2% compared with up to 5% in Western countries (28). Among the cases of MPMs listed in
Table II, four had family histories
of cancer and three did not; family history was unknown for the
remaining cases. In the present case, the patient did not meet the
Amsterdam II Criteria or the Revised Bethesda Guidelines. Other
major hereditary gastrointestinal cancer syndromes are familial
adenomatous polyposis (FAP), Li-Fraumeni syndrome, Hereditary
diffuse gastric cancer (29). FAP is
an autosomal dominant disease that is classically characterized by
the development of hundreds to thousands of adenomas in the rectum
and colon during the second decade of life (30). The patient did not have the typical
FAP phenotype of polyposis. The diagnosis of FAP was unlikely.
Li-Fraumeni syndrome is a cancer predisposition syndrome caused by
a germline mutation of the TP53 gene (31), and hereditary diffuse gastric cancer
is characterized by an accumulation of diffuse type gastric cancer
in the family pedigree (32). These
syndromes were unlikely in the present case, since the patients was
elder male and the combination of MPMs was not typical of these
hereditary cancer syndromes. Although we could not exclude
completely the possibility of hereditary cancer syndromes as we did
not perform germline exome sequencing, the MPMs of the present
patient might have been sporadic in nature, rather than
hereditary.
In conclusion, patients with cancers typically
undergo far more testing than the general population, accounting
for the high detection rate of additional malignancies. As a result
of increased detection of early cancers and development of new
therapeutic strategies, the prognosis for cancer patients has
steadily improved. This improvement in prognosis has led to an
increased incidence of MPMs. In the near future, molecular biologic
techniques might help to diagnose MPMs earlier. It is important to
understand the characteristics of MPMs in order to administer
suitable treatment and determine relevant follow-up plans for
cancer patients.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
YM and KS conceived the study. YM was involved in
the acquisition of clinical documents and drafting the manuscript.
KS and TK supervised the writing of the manuscript. FW, YK, HN and
TR performed the surgery. TK, KI, YT, TF, NK, FW, YK, HN and TR
treated the patient. All authors read and approved the final
version of the manuscript.
Ethics approval and consent to
participate
Written informed consent for surgery, chemotherapy
and publication was obtained from the patient.
Patient consent for publication
Written informed consent was obtained from the
patient for publication of this case report.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
IPMC
|
intraductal papillary mucinous
carcinoma
|
|
MPM
|
multiple primary malignancy
|
|
AC
|
adenocarcinoma
|
|
UC
|
urothelial carcinoma
|
|
SCC
|
squamous cell carcinoma
|
|
IPMN
|
intraductal papillary mucinous
neoplasm
|
|
CRC
|
colorectal cancer
|
References
|
1
|
Warren S and Gates O: Multiple primary
malignant tumors: A survey of the literature and a statistic study.
Am J Cancer. 16:1358–1414. 1932.
|
|
2
|
Johnson CH: SEER Program Coding and
Staging Manual 2004, Revision 1. National Cancer Institute, NIH
Publication. (Bethesda, MD). 2004.
|
|
3
|
Kato T, Suzuki K, Muto Y, Sasaki J,
Tsujinaka S, Kawamura YJ, Noda H, Horie H, Konishi F and Rikiyama
T: Multiple primary malignancies involving primary sporadic
colorectal cancer in Japan: Incidence of gastric cancer with
colorectal cancer patients may be higher than previously
recognized. World J Surg Oncol. 13:232015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Jones P: Letter: Five separate
malignancies in one patient. BMJ. 1:15331976. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sommers GM, Logan S and Camel HM: Six
independent neoplasms in one woman. A case report. J Reprod Med.
33:82–83. 1988.PubMed/NCBI
|
|
6
|
Martin-Granizo R, Naval L, Castro P,
Goizueta C and Muñoz M: Quintuple cancers: Report of a case with
triple cancers in the head and neck. J Craniomaxillofac Surg.
25:153–157. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Yakushiji H, Mukai S, Matsukura S, Sato S,
Ogawa A, Sasatomi E and Miyazaki K: DNA mismatch repair deficiency
in curatively resected sextuple primary cancers in different
organs: A molecular case report. Cancer Lett. 142:17–22. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Cercato MC, Colella E, Ferraresi V,
Diodoro MG and Tonachella R: Report of two cases of quintuple
primary malignancies and review of the literature. Anticancer Res.
28:2953–2958. 2008.PubMed/NCBI
|
|
9
|
Komiyama S, Nishio E, Ichikawa R, Miyamura
H, Kawamura K, Komiyama M, Nishio Y and Udagawa Y: Asymptomatic
synchronous quintuple primary cancers. Gynecol Obstet Invest.
74:324–328. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Mukaiyama Y, Suzuki M, Morikawa T, Mori Y,
Takeshima Y, Fujimura T, Fukuhara H, Nakagawa T, Nishimatsu H, Kume
H, et al: Multiple primary malignant neoplasms of the glottis,
renal pelvis, urinary bladder, oral floor, prostate, and esophagus
in a Japanese male patient: A case report. World J Surg Oncol.
12:2942014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Demandante CG, Troyer DA and Miles TP:
Multiple primary malignant neoplasms: Case report and a
comprehensive review of the literature. Am J Clin Oncol. 26:79–83.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Tabuchi T, Ito Y, Ioka A, Miyashiro I and
Tsukuma H: Incidence of metachronous second primary cancers in
Osaka, Japan: Update of analyses using population-based cancer
registry data. Cancer Sci. 103:1111–1120. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Takeuchi D, Koide N, Komatsu D, Okumura M,
Suzuki A and Miyagawa S: Relationships of obesity and diabetes
mellitus to other primary cancers in surgically treated gastric
cancer patients. Int J Surg. 12:587–593. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Yun HR, Yi LJ, Cho YK, Park JH, Cho YB,
Yun SH, Kim HC, Chun HK and Lee WY: Double primary malignancy in
colorectal cancer patients--MSI is the useful marker for predicting
double primary tumors. Int J Colorectal Dis. 24:369–375. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Uchino S, Noguchi M, Ochiai A, Saito T,
Kobayashi M and Hirohashi S: p53 mutation in gastric cancer: A
genetic model for carcinogenesis is common to gastric and
colorectal cancer. Int J Cancer. 54:759–764. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Sawai T, Nanashima A, Tsuji T, Yamaguchi
H, Yasutake T, Nakagoe T, Ayabe H and Tagawa Y: Instability of
chromosome 17 and the p53 locus in non-familial colorectal cancer
with multiple primary malignancies. J Exp Clin Cancer Res.
20:401–405. 2001.PubMed/NCBI
|
|
17
|
Schatzkin A, Baranovsky A and Kessler LG:
Diet and cancer. Evidence from associations of multiple primary
cancers in the SEER program. Cancer. 62:1451–1457. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Saito S, Hosoya Y, Togashi K, Kurashina K,
Haruta H, Hyodo M, Koinuma K, Horie H, Yasuda Y and Nagai H:
Prevalence of synchronous colorectal neoplasms detected by
colonoscopy in patients with gastric cancer. Surg Today. 38:20–25.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Sugiyama M and Atomi Y: Extrapancreatic
neoplasms occur with unusual frequency in patients with intraductal
papillary mucinous tumors of the pancreas. Am J Gastroenterol.
94:470–473. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Larghi A, Panic N, Capurso G, Leoncini E,
Arzani D, Salvia R, Del Chiaro M, Frulloni L, Arcidiacono PG, Zerbi
A, et al: Prevalence and risk factors of extrapancreatic
malignancies in a large cohort of patients with intraductal
papillary mucinous neoplasm (IPMN) of the pancreas. Ann Oncol.
24:1907–1911. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kato T, Alonso S, Noda H, Miyakura Y,
Tsujinaka S, Saito M, Muto Y, Fukui T, Ichida K, Takayama Y, et al:
Malignant, but not benign, intraductal papillary mucinous neoplasm
preferentially associates with prior extrapancreatic malignancies.
Oncol Rep. 35:3236–3240. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Powell S, Tarchand G, Rector T and Klein
M: Synchronous and metachronous malignancies: Analysis of the
Minneapolis Veterans Affairs (VA) tumor registry. Cancer Causes
Control. 24:1565–1573. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Travis LB, Rabkin CS, Brown LM, Allan JM,
Alter BP, Ambrosone CB, Begg CB, Caporaso N, Chanock S, DeMichele
A, et al: Cancer survivorship--genetic susceptibility and second
primary cancers: Research strategies and recommendations. J Natl
Cancer Inst. 98:15–25. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Begg CB, Zhang ZF, Sun M, Herr HW and
Schantz SP: Methodology for evaluating the incidence of second
primary cancers with application to smoking-related cancers from
the Surveillance, Epidemiology, and End Results (SEER) program. Am
J Epidemiol. 142:653–665. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Do KA, Johnson MM, Lee JJ, Wu XF, Dong Q,
Hong WK, Khuri FR and Spitz MR: Longitudinal study of smoking
patterns in relation to the development of smoking-related
secondary primary tumors in patients with upper aerodigestive tract
malignancies. Cancer. 101:2837–2842. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Pöschl G and Seitz HK: Alcohol and cancer.
Alcohol Alcohol. 39:155–165. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Schottenfeld D: Alcohol as a co-factor in
the etiology of cancer. Cancer. 43 (Suppl 5):1962–1966. 1979.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Yamamoto S, Yoshimura K, Ri S, Fujita S,
Akasu T and Moriya Y: The risk of multiple primary malignancies
with colorectal carcinoma. Dis Colon Rectum. 49 (Suppl 10):S30–S36.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Hata K, Yamamoto Y, Kiyomatsu T, Tanaka T,
Kazama S, Nozawa H, Kawai K, Tanaka J, Nishikawa T, Otani K, et al:
Hereditary gastrointestinal cancer. Surg Today. 46:1115–1122. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Half E, Bercovich D and Rozen P: Familial
adenomatous polyposis. Orphanet J Rare Dis. 4:222009. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Correa H: Li-Fraumeni Syndrome. J Pediatr
Genet. 5:84–88. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Fitzgerald RC, Hardwick R, Huntsman D,
Carneiro F, Guilford P, Blair V, Chung DC, Norton J, Ragunath K,
Van Krieken JH, et al International Gastric Cancer Linkage
Consortium, : Hereditary diffuse gastric cancer: Updated consensus
guidelines for clinical management and directions for future
research. J Med Genet. 47:436–444. 2010. View Article : Google Scholar : PubMed/NCBI
|