Introduction
Lenvatinib is a multireceptor tyrosine kinase
inhibitor with versatile application approved by the Food and Drug
Administration (FDA), at different dose, for the treatment of
locally recurrent or metastatic progressive radioactive
iodine-refractory (RAIR) differentiated thyroid cancer (TC)
(1), as well as renal cell carcinoma
(in combination with everolimus) and hepatocellular carcinoma
(2,3). Lenvatinib inhibits several tyrosine
kinase receptors implicated in pathogenic angiogenesis, tumor
growth, and cancer progression, in addition to their normal
cellular functions including the vascular endothelial growth factor
(VEGF) receptors VEGFR1 (FLT1), VEGFR2 (KDR), and VEGFR3 (FLT4),
the fibroblast growth factor receptors (FGFR) 1, 2, 3, and 4, the
platelet-derived growth factor receptor alpha, KIT, and RET
(4). In TC, the starting dose is 24
mg daily (5). However, it is
possible, in clinical practice, consider starting at other dose
(20, 14, 10 mg/day and escalate or de-escalate as tolerated), based
on clinical consideration (age, concomitant diseases, performance
status and risk of adverse events) (6).
In recent years, antiangiogenic drugs, including
monoclonal antibodies like bevacizumab and multikinase inhibitors
like lenvatinib, have represented an enormous improvement in the
treatment of several types of cancer and a shift towards
personalized and precision therapy. However, they present some side
effects that have never been observed with conventional
chemotherapy. In clinical practice, the most frequent adverse
events related to antiangiogenic drugs are cardiovascular and
gastrointestinal problems, thromboembolic events, and dermatologic
alterations including wound healing complications (7,8).
We present the case of an 80-year-old man with stage
IV TC diagnosed with Fournier's gangrene (FG) that was most likely
related to the antiangiogenic effect of lenvatinib. Written
informed consent was provided by the patient for the publication of
his clinical information and images.
Case report
In January 2018, an 80-year-old man was admitted to
the Department of Emergency due to an anorectal abscess. His past
medical history was significant for hypertension, prostatic
hyperplasia, and stage IV RAIR TC, with metastases to the lungs,
mediastinum, and liver. He was not a smoker nor a drinker. He
underwent total thyroidectomy in 2000. Surgical pathology showed a
multifocal papillary TC with poorly differentiated component. He
received a first RAI treatment two months after the surgery. Post
treatment whole body scan showed uptake in the thyroid bed and
upper mediastinum. A second cycle of RAI was given in 2001
(cumulative activity 370 mCi). Posttreatment scan was negative. In
2001 and in 2016 he had central compartment and bilateral neck
dissection for recurrent disease. The first evidence of lung
metastasis was in 2005. His metastatic disease had been observed
for several years but in 2017, due to lung and liver progression,
he was started on lenvatinib at a dose of 20 mg daily. After 4
months with stable disease, lenvatinib was reduced to 20 mg daily
(5 days on, 2 off) because of toxicity (uncontrolled hypertension,
mucositis, fatigue).
This unconventional treatment scheme was offered in
accordance with patient preference and pharmacokinetic data
(half-life of lenvatinib: 28 h) (9).
It resulted in a better tolerability, less toxicity and increased
adherence to therapy.
After 14 months of treatment with lenvatinib, he was
admitted to the emergency room. He was hypotensive (90/55 mmHg),
tachycardic (150 beats per min), and afebrile. His hemoglobin level
was 14.4 g/dl, with a hematocrit level of 42.5%; white blood cell
count was 24.9x103 cells/µl (with 87% neutrophils), and
platelet count was 328x103 cells/µl. C-reactive protein
was 26.33 mg/dl, creatinine was 1.9 ng/dl, serum sodium was 131
mmol/l, serum potassium was 5.5 mmol/l, and lactate level to venous
blood gas was 1.79 mmol/l. Fournier's gangrene severity index was
8(10). Unfortunately, there was
hemolysis in the sample.
At that time, other medications included
levothyroxine, calcium, vitamin D3, silodosin, olmesartan,
amlodipine, and sotalol. He was overweight (BMI: 28
kg/m2) and the metabolic panel performed one month
before the event showed dyslipidemia (triglycerides: 299 mg/dl; LDL
cholesterol: 107 mg/dl; and HDL: 36 mg/dl) with a fasting blood
sugar of 88 mg/dl.
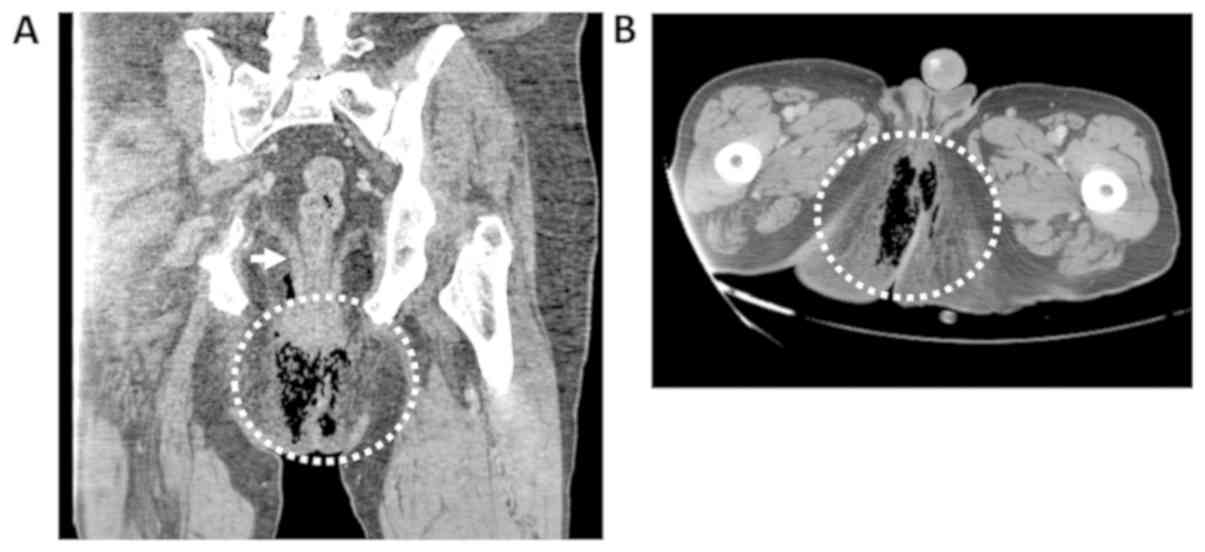
An abdominal CT scan performed in the emergency room
showed an abscess in the perianal area with thickening of the
levator ani muscle. Abscess tissue surrounded the anus and deepened
caudally and posteriorly between the buttocks, and there was
evidence of gaseous nuclei which were also involved in the anal,
perineal, and gluteus region and extended anteriorly to the penile
region, a presentation compatible with FG (Fig. 1). No signs of progressive disease
were found. Surgery was performed with an incision at the root of
the scrotum, which was then washed and packed with iodoform gauze.
As limitation of this report, blood and tissue culture data were
not available. Empirical treatment with meropenem 1 g,
metronidazole 0.5 g, and amoxicilline 2 g was started.
Clinical evolution was satisfactory and the patient
was discharged after 7 days. Lenvatinib treatment was discontinued
after the diagnosis of Fournier's gangrene. The patient experienced
brain progression 6 months after lenvatinib was stopped. Because of
the oligoprogression, stereotactic radiation therapy was
administered without adding systemic treatment. Multiorgan
progression occurred 8 months later. At that point the patient
moved to another city. He was still alive 16 months after the
event.
Discussion
FG is a type of necrotizing fasciitis that involves
the perineal, perianal, and genital areas and most frequently
affects elderly men. Traditional risk factors are diabetes,
immunosuppression, recent surgery, and trauma to the genital and
perianal area. Clinical manifestations usually present with acute
and rapidly progressive edema, erythema, and tenderness. Advanced
cases are defined by toxic symptoms including fever, tachycardia,
hypotension, and septic shock. Clinical suspicion should be
confirmed with surgical exploration. A CT scan can also help
identify an infectious origin and delineate the extent of disease.
Surgical debridement of the necrotic areas, along with parenteral
broad-spectrum antibiotics, represents the gold standard of
treatment. Early diagnosis and treatment are crucial for a better
outcome, as the mortality of this condition is high (11).
Our patient developed FG with the only known risk
factor being advanced age. No symptoms were reported in our chart
that might have been suggestive of this condition. None of the
available blood parameters measured prior to development of FG
provided any indication about the development of FG.
To the best of our knowledge, this is the first
reported case of FG in relation to lenvatinib treatment. According
to the Naranjo Adverse Drug Reaction Probability Scale (12) and Jones algorithm (13), lenvatinib was determined to be the
probable cause of FG (Tables SI and
SII; http://www.pmidcalc.org/?sid=7249508&newtest=Y).
In 2012, the FDA reported 22 cases of necrotizing
fasciitis that developed during treatment of colorectal cancer with
bevacizumab, with death resulting in 13.6% of patients (14). A safety alert regarding some cases
related to bevacizumab has also been described in literature
(15-17).
Other cases have been reported in association with aflibercept for
the treatment of colorectal cancer (18) and sunitinib in a patient treated for
renal cell carcinoma (19). In all
these cases, the condition developed in the absence of major risk
factors other than antiangiogenic treatment. We assume that the
condition is likely due to a perturbation of vascular endothelial
cells of the skin due to the inhibition of VEGF/VEGFR signaling,
since these drugs don't have other targets in common. It has been
found that VEGF/VEGFR inhibition leads to a perturbation in the
coagulation cascade, resulting in a prothrombotic state (20). Thrombosis in small skin vessels could
lead to ischemia and necrosis of the tissue with secondary
bacterial colonization, causing the development of the
infection.
As regards the temporal relationship between the
treatment and side effects, in our patient FG appeared 14 months
after lenvatinib was started and was a late serious side effect. In
previous reports (15,16,18,19), the
median time until the occurrence of this event was 6.5 months
(range 4-12) and appeared during treatment with the antiangiogenic
agent. In clinical practice, physicians worry about acute side
effects, but late side effects could be serious as well and few
data are available on this topic (14). Delayed or late onset adverse events
are common with VEGF/VEGFR. For instance, proteinuria and nephrotic
syndrome develop over time (21).
FG, in previous reports as well as in our case, has been described
after several months of therapy. So far, most studies have not been
able to address late-onset toxicity incidence because treatment
times in clinical trials are shorter. Post-marketing analyses help
in identifying late and/or severe adverse events (14). Since TC is commonly a slow-growing
cancer compared to other solid tumors and since the median
progression-free survival associated with lenvatinib in this
setting has been shown to be long (18 months) (5), it would not be surprising if other
late-onset toxicities come to light in post-marketing studies or
anecdotal cases.
The worldwide growing use of lenvatinib for the
treatment of RAI refractory thyroid cancer and other tumors will
lead the clinicians to deal with adverse events not reported in the
SELECT study (5) or in the reports
of real-life experience (22).
Combining knowledge of the risk factors-signs of FG and our
findings reported in this case, should push clinicians, during
periodic evaluation of patients on lenvatinib, to ask questions
about symptoms of discomfort of perineal area and consider
anorectal abscess/FG in differential diagnosis. In particular, in
patients with risk factors for FG and under treatment with
antiangiogenic drugs, the choice of a more specific follow-up based
on periodic and symptoms-based inspection of the genitalia,
perineum and digital rectal examination should be considered.
Moreover, a clinical evaluation of this body area may be
appropriate prior to prescribing antiangiogenics.
In conclusion, this is the first case reported in
literature of Fournier's gangrene likely related to lenvatinib
treatment in a patient with advanced thyroid cancer. In our
opinion, Fournier's gangrene is a class effect of antiangiogenic
treatment. Clinicians who deal with these drugs in clinical
practice should be aware of the possibility, even though remote,
that this condition may develop given the fact that it has a high
mortality rate and prompt diagnosis and management are needed.
Supplementary Material
Naranjo adverse drug reaction
probability scale.
Naranjo adverse drug reaction
probability scale: Interpretation of scores.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
CD, GG, VR and RF evaluated the patient and
participated in treatment planning. TG evaluated radiological
images and generated Fig. 1. MB and
RF wrote the manuscript. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Informed consent was provided by the patient for the
publication of his clinical information and images.
Competing interests
CD declares receiving an Advisory Board fee from
EISAI. MB, GG, VR, TG and RF declare that they have no competing
interests.
References
|
1
|
Lamartina L, Grani G, Durante C and
Filetti S: Recent advances in managing differentiated thyroid
cancer. F1000Res. 7(86)2018.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Kudo M, Finn RS, Qin S, Han KH, Ikeda K,
Piscaglia F, Baron A, Park JW, Han G, Jassem J, et al: Lenvatinib
versus sorafenib in first-line treatment of patients with
unresectable hepatocellular carcinoma: A randomised phase 3
non-inferiority trial. Lancet. 391:1163–1173. 2018.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Motzer RJ, Hutson TE, Glen H, Michaelson
MD, Molina A, Eisen T, Jassem J, Zolnierek J, Maroto JP, Mellado B,
et al: Lenvatinib, everolimus, and the combination in patients with
metastatic renal cell carcinoma: A randomised, phase 2, open-label,
multicentre trial. Lancet Oncol. 16:1473–1482. 2015.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Fala L: Lenvima (Lenvatinib), a
multireceptor tyrosine kinase inhibitor, approved by the FDA for
the treatment of patients with differentiated thyroid cancer. Am
Health Drug Benefits. 8 (Spec Feature):176–179. 2015.PubMed/NCBI
|
|
5
|
Schlumberger M, Tahara M, Wirth LJ,
Robinson B, Brose MS, Elisei R, Habra MA, Newbold K, Shah MH, Hoff
AO, et al: Lenvatinib versus placebo in radioiodine-refractory
thyroid cancer. N Engl J Med. 372:621–630. 2015.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Kim SY, Kim SM, Chang H, Kim BW, Lee YS,
Chang HS and Park CS: Safety of tyrosine kinase inhibitors in
patients with differentiated thyroid cancer: Real-world use of
lenvatinib and sorafenib in Korea. Front Endocrinol (Lausanne).
10(384)2019.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Krajewska J, Kukulska A and Jarzab B: Drug
safety evaluation of lenvatinib for thyroid cancer. Expert Opin
Drug Saf. 14:1935–1943. 2015.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Schmidinger M: Understanding and managing
toxicities of vascular endothelial growth factor (VEGF) inhibitors.
EJC. (Suppl 11):172–191. 2013.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Capozzi M, De Divitiis C, Ottaiano A, von
Arx C, Scala S, Tatangelo F, Delrio P and Tafuto S: Lenvatinib, a
molecule with versatile application: From preclinical evidence to
future development in anti-cancer treatment. Cancer Manag Res.
11:3847–3860. 2019.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Laor E, Palmer LS, Tolia BM, Reid RE and
Winter HI: Outcome prediction in patients with Fournier's gangrene.
J Urol. 154:89–92. 1995.PubMed/NCBI
|
|
11
|
Singh A, Ahmed K, Aydin A, Khan MS and
Dasgupta P: Fournier's gangrene. A clinical review. Arch Ital Urol
Androl. 88:157–164. 2016.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Naranjo CA, Busto U, Sellers EM, Sandor P,
Ruiz I, Roberts EA, Janecek E, Domecq C and Greenblatt DJ: A method
for estimating the probability of adverse drug reactions. Clin
Pharmacol Ther. 30:239–245. 1981.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Jones JK: Adverse drug reactions in the
community health setting: Approaches to recognizing, counseling,
and reporting. Fam Community Health. 5:58–67. 1982.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Shamloo BK, Chhabra P, Freedman AN,
Potosky A, Malin J and Weiss Smith S: Novel adverse events of
bevacizumab in the US FDA adverse event reporting system database:
A disproportionality analysis. Drug Saf. 35:507–518.
2012.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Gamboa EO, Rehmus EH and Haller N:
Fournier's gangrene as a possible side effect of bevacizumab
therapy for resected colorectal cancer. Clin Colorectal Cancer.
9:55–58. 2010.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Sendur MA, Aksoy S, Özdemir NY and Zengin
N: Necrotizing fasciitis secondary to bevacizumab treatment for
metastatic rectal adenocarcinoma. Indian J Pharmacol. 46:125–126.
2014.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Ugai T, Norizuki M, Mikawa T, Ohji G and
Yaegashi M: Necrotizing fasciitis caused by Haemophilus influenzae
type b in a patient with rectal cancer treated with combined
bevacizumab and chemotherapy: A case report. BMC Infect Dis.
14(198)2014.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Gonzaga-López A, Muñoz-Rodriguez J and
Ruiz-Casado A: Necrotising fasciitis in a patient treated with
FOLFIRI-aflibercept for colorectal cancer: A case report. Ann R
Coll Surg Engl. 99:e225–e226. 2017.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Piszczek J, Dalton B, Peters T, Ruether D
and Urbanski S: Extensive necrotizing fasciitis associated with
sunitinib therapy. Clin Genitourin Cancer. 12:e47–e49.
2014.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Kuenen BC: Analysis of prothrombotic
mechanisms and endothelial perturbation during treatment with
angiogenesis inhibitors. Pathophysiol Haemost Thromb. 33 (Suppl
1):S13–S14. 2003.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Moriconi D, Cappagli V, Viola D, Molinaro
E, Agate L, Lorusso L, Egidi MF and Elisei R: Proteinuria is a late
onset adverse event in patients treated with cabozantinib: A single
center experience. Nephrol Dial Transpl. 33:i388–i38918. 2018.
|
|
22
|
Locati LD, Piovesan A, Durante C, Bregni
M, Castagna MG, Zovato S, Giusti M, Ibrahim T, Puxeddu E, Fedele G,
et al: Real-world efficacy and safety of lenvatinib: Data from a
compassionate use in the treatment of radioactive iodine-refractory
differentiated thyroid cancer patients in Italy. Eur J Cancer.
118:35–40. 2019.PubMed/NCBI View Article : Google Scholar
|