Introduction
Follicular dendritic cells are, due to their
function of presenting and retaining antigens, important
contributors to memory B-Cell maturation during germinal centre
reaction (GCR) (1). They organise
B-Cell homeostasis and immune response in secondary lymphoid organs
and seem to be the connection between innate and adaptive (B cell)
response (2,3). B-Cell migration from follicles and
competent humoral immune response are dependent on Follicular
Dendritic Cells (4-6).
They secrete CXCL13 chemokine for B-Cell follicle homing and built
a scaffold for B-cell migration (7,8).
Cellular mechanisms of Follicular Dendritic Cells are subject to
research and lymph node FDC progenitor cells are still unknown.
Research is especially difficult considering the fact that FDCs
work in delicate 3D networks subsequent to pathogen exposition,
limiting vitro examination in particular (2,9,10). The
extremely rare neoplasm follicular dendritic cell sarcoma (FDCS)
was first characterised by Monda et al (11) in 1986. Until today about 120 cases
of FDCS of the head and neck region have been reported (12). The majority (60%) arises primarily
in cervical, abdominal or axillar lymph nodes, but also extra-nodal
origin from secondary lymphatic tissue like the tonsils, Waldeyer's
ring or MALT is not uncommon (40%) (13). Final diagnosis of FDCS can only be
established by immunohistochemical profiling. FDCS usually proves
positive for CD21, CD23, CD35, KI-M4p, clusterin, Claudin 4, CXCL
13 and Ki-FDC1p, and in some cases for vimentin, S-100 protein,
CD68, and specific muscle actin (SMA) (12,14,15).
Often further pathological, electron microscope and cytochemical
analyses are required. Clinically, FDCS shows low to intermediate
malignant potential and a local recurrence rate of 40%. Distant
metastasis occurs in 25% of cases, most often in the lungs, liver,
peritoneum, and lymph nodes resulting in a mortality rate of 16.7%
(14). Because the origin of
follicular dendritic cells is uncertain, therapy of the FDCS
varies. Krautler et al (16), found that FDCs are stromal in
origin. In contrast to other dendritic cells, which are
hematopoietic, they develop from mural cells (16) but opinions in literature vary
(5,17). Therapeutic approaches of FDCS vary
significantly and include total surgical removal with or without
adjuvant radio and/or chemotherapy or chemotherapy by itself.
Case report
A 66-year-old patient suffered from an otherwise
asymptomatic suddenly arisen right cervical mass in December of
2001. Upon clinical examination he presented with a rounded
well-relocatable submandibular tumour of about 2 cm in maximum
diameter and underwent surgical resection in early 2002 alio loco
(University Hospital Aachen, Germany). The tumour was completely
removed and the specimen was diagnosed as a metastasis of a medium
proliferative spindle-cell mesenchymal tumour to a cervical lymph
node, for instance a fibrosarcoma or a nerve sheath tumour. After
extensive subsequent screening of the patient for further
metastases and a primary tumour was negative, the specimens were
referred to the national reference centre for soft tissue tumours.
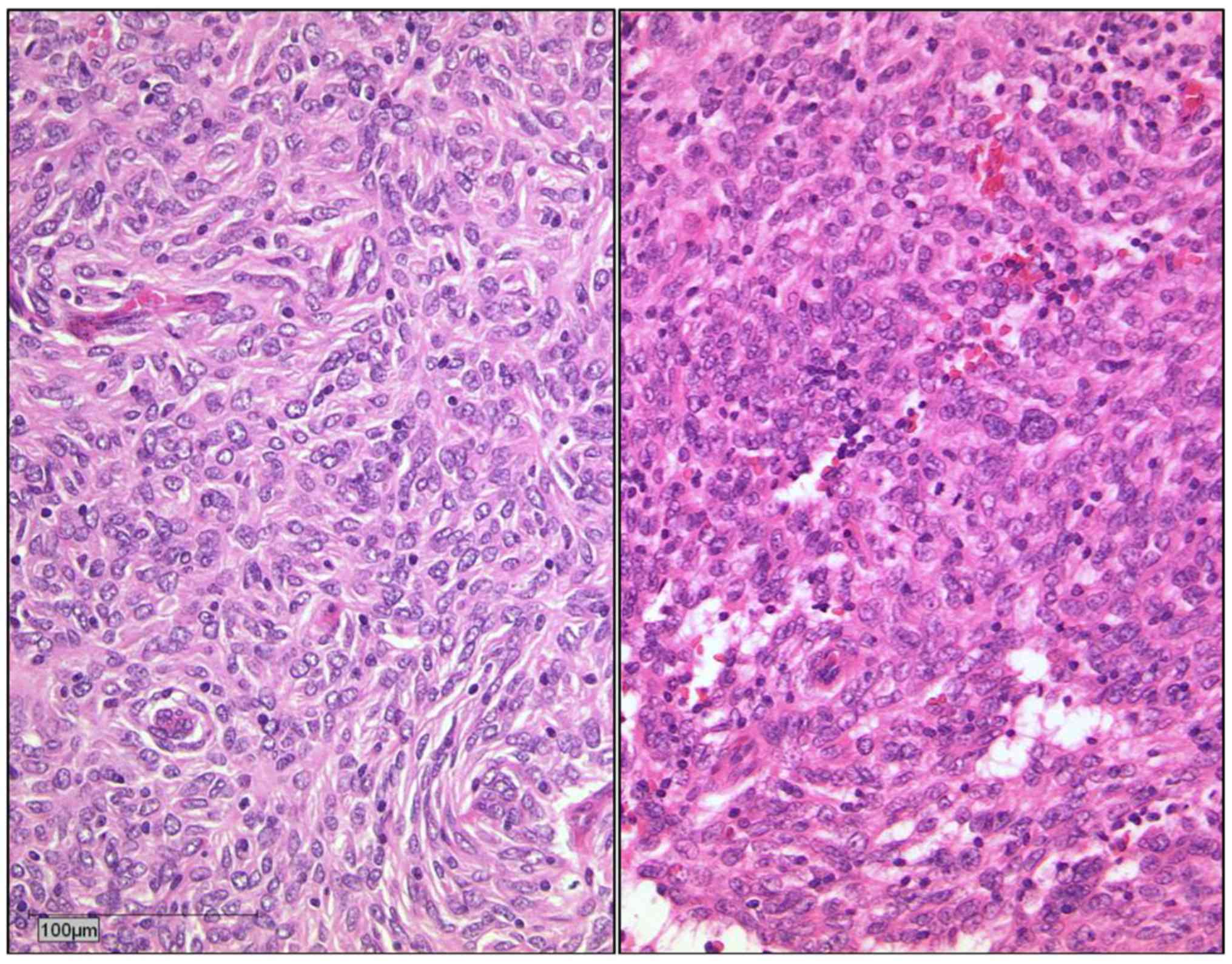
Histopathologic re-evaluation revealed a relatively uniform aspect
with balls and curls of tumour cells with a chromatin-rich, hardly
definable cytoplasm reminiscent of a nerve sheath tumour (Fig. 1; H&E micrographs).
Immunohistochemistry confirmed the suspected diagnosis of a FDCS
(Table I). In 2001 only few cases
of FDCS were reported, most of them treated FDSC with total, local
excision without adjuvant therapy (18-20).
In some cases of FDCS occurring in multiple locations chemotherapy
(alone or adjuvant) was performed (20,21).
Therefore, the patient was not subjected to any further
therapy.
 | Table IImmunohistochemical results. |
Table I
Immunohistochemical results.
| Marker | 2002 | 2005 | 2007 | 2008 |
|---|
| CD23 | +++ | +++ | +++ | +++ |
| CD21 | +++ | +++ | +++ | +++ |
| CD35 | - | - | + | - |
| PD-L1 | - | - | - | - |
| D2-40 | +++ | +++ | +++ | +++ |
| CD68 | + | + | + | + |
| EMA | - | + | + | - |
| Vimentin | +++ | +++ | +++ | +++ |
| S100 | \ | - | \ | \ |
| CK | \ | - | \ | \ |
| Mib-1 (in hot spot
areas), % | 30 | 45 | 30 | 40 |
In June 2005 the patient was referred to our
outpatient department (University Hospital Düsseldorf, Germany)
with a right-sided submandibular nontender cervical lump of 2.5x2.5
cm right beneath the scar of the former surgical approach. Again,
the lesion was asymptomatic otherwise, and clinically there were no
further pathologic findings. A contrast-enhanced CT scan
(SOMATOM® Sensation 6-System; Siemens) raised the
suspicion of a metastatic lymph node conglomerate in the right
neck-region I B without evidence of a primary tumour. MRI (1,5 T
Magnetom® Vision system; Siemens) demonstrated two
cervical masses almost isointense with skeletal muscles on
T1-weighted imaging, with a high signal intensity on T2-weighted
images and only weakly enhanced on fat-suppressed contrast-enhanced
T1-weigthed images obtained after administration of
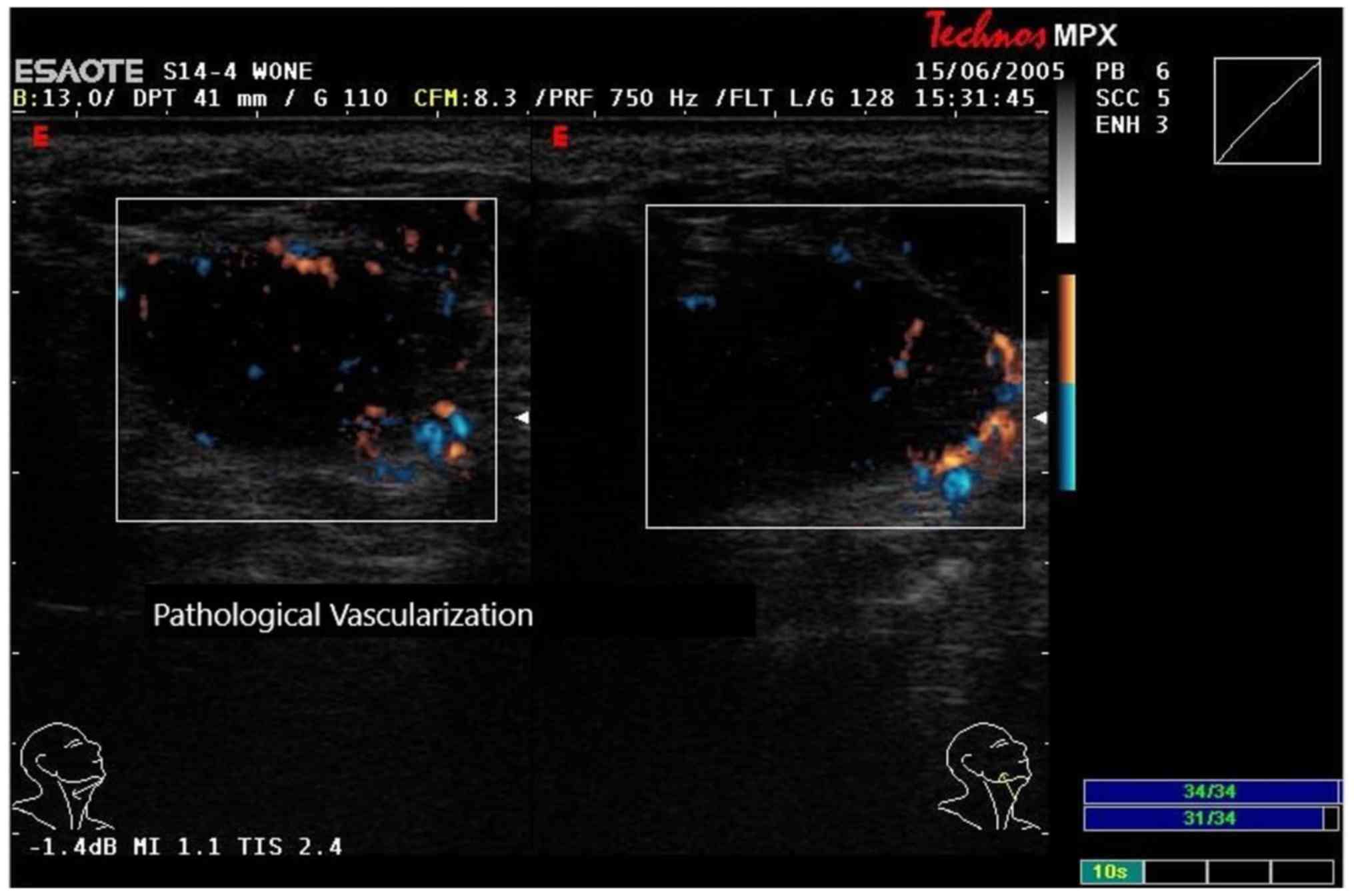
gadolinium-DTPA. Conventional B-scan-sonography of the region
(Technos MPX System by Esaote™) showed four homogenous round masses
of low echogenicity in the right submandibular region with a
pathologic diffuse vascularisation pattern [Fig. 2; sonography in 2005-B-Mode and color
doppler ultrasound using a linear (14-8 MHz)]. The size of the
masses ranged from 11.3 to 18.3 mm in maximum diameter.
Additionally, the lesions were investigated using power
doppler-analysis, tissue-enhanced imaging (TEI), and
contrast-enhanced phase inversion low MI (<0-1) real-time
ultrasound (CnTI) with the second-generation echo enhancer SonoVue™
(4.8 ml as a bolus i.v. followed by 5 ml NaCl i.v.; Bracco Corp.)
(Fig. 2; sonography in 2005).
Unfortunately, there were no PET images taken. A PET-CT could have
added further information.
Under the differential diagnosis of a recurrence of
the FDC-Tumour versus a CUP-syndrome (carcinoma of unknown
primary), the four masses were removed using the same submandibular
approach as used in 2002, and again they appeared to be
well-encapsulated and were removed macroscopically in toto.
Histopathologic evaluation now revealed four tumours well defined
by connective tissue consisting of spindle-shaped, less pleomorphic
cells with a light prominent nucleus and grained chromatin
(Fig. 1; H&E micrographs).
Upon confirmation of the suspected diagnosis by a
national reference centre the patient was submitted to a
restaging-program including CT-scans of the head and neck region,
the chest, and the abdomen as well as a contrast-enhanced
ultrasonographic examination of the abdominal organs. All
investigations were negative for any other primary or metastatic
disease. Again, the patient declined receiving any further therapy
and was closely monitored.
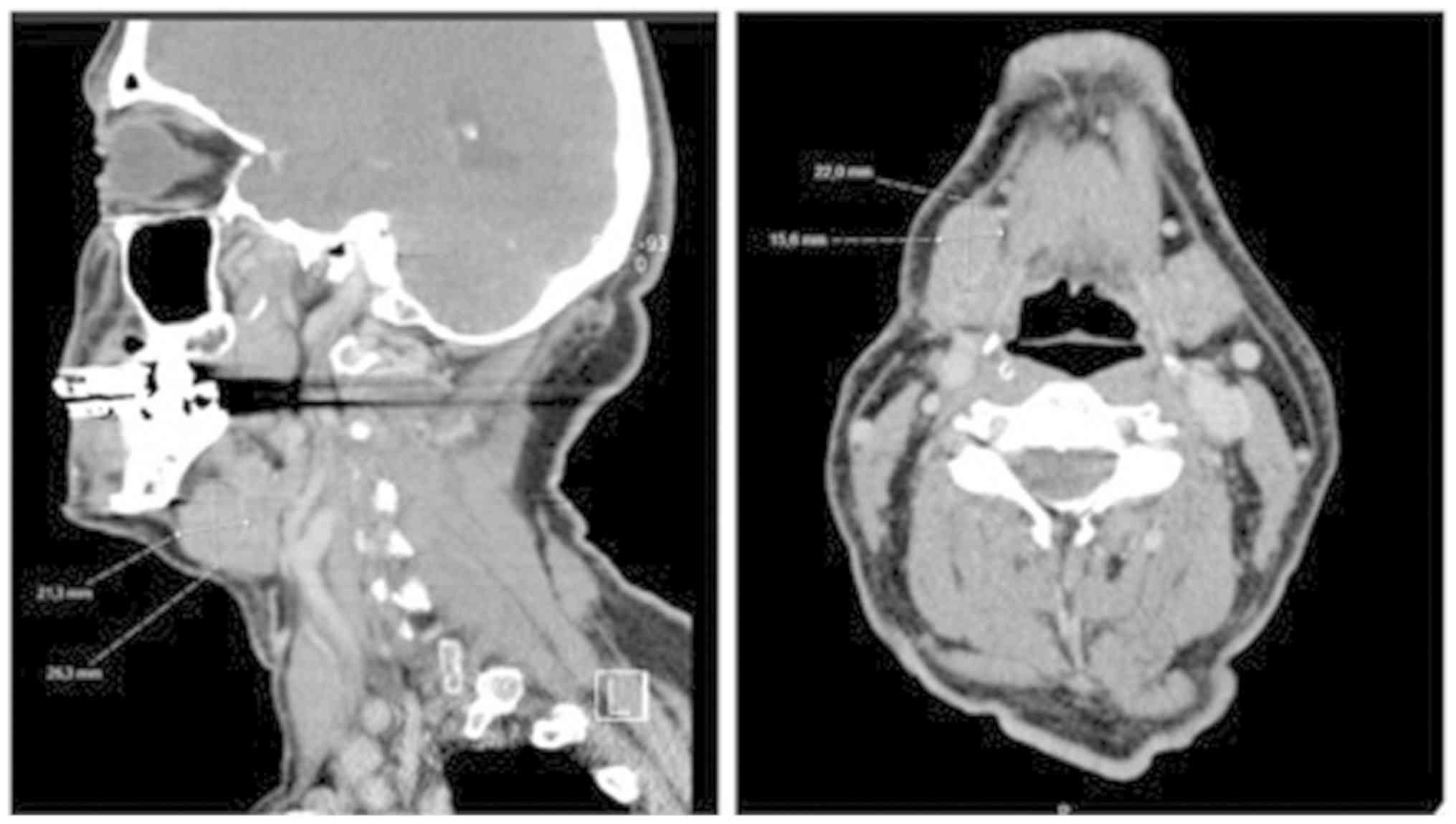
In 2007 the patient presented once more with two
enlarged lymph nodes both about 2.5x2.1x1.7 cm in size. One in the
right submandibular region (IB), the other in the anterior
submandibular region (IA) (Fig. 3;
CT scans in 2007-Somatom Emotion 6 by Siemens Healthcare GmbH). The
lymph nodes were surgically removed and histologically
investigated. Specimens showed cells matching the previously
identified follicular dendritic cell sarcoma. Adjuvant radiotherapy
and/or chemotherapy was offered but refused by the patient, because
of its indefinite success (22),
its side effects, and prolonged hospitalisation.
In 2008 the patient felt another submandibular mass
growing. In addition, several slightly enlarged lymph nodes were
found. Considering the quick recurrence and the involvement of
several lymph nodes the patient agreed to receive systemic
chemotherapy with a CHOP regimen. Nevertheless, to receive a second
opinion, he transferred to another hospital (University Hospital
Cologne, Germany), where a mass of 2x2x1.4 cm was identified
sonographically and a tumour resection in combination with a neck
dissection was performed in June of 2008. The pathohistological
examination of the excised specimens was congruous with the
previously described follicular dendritic cell sarcoma. No adjuvant
therapy was performed. After close monitoring the patient has been
recurrence-free for ten years.
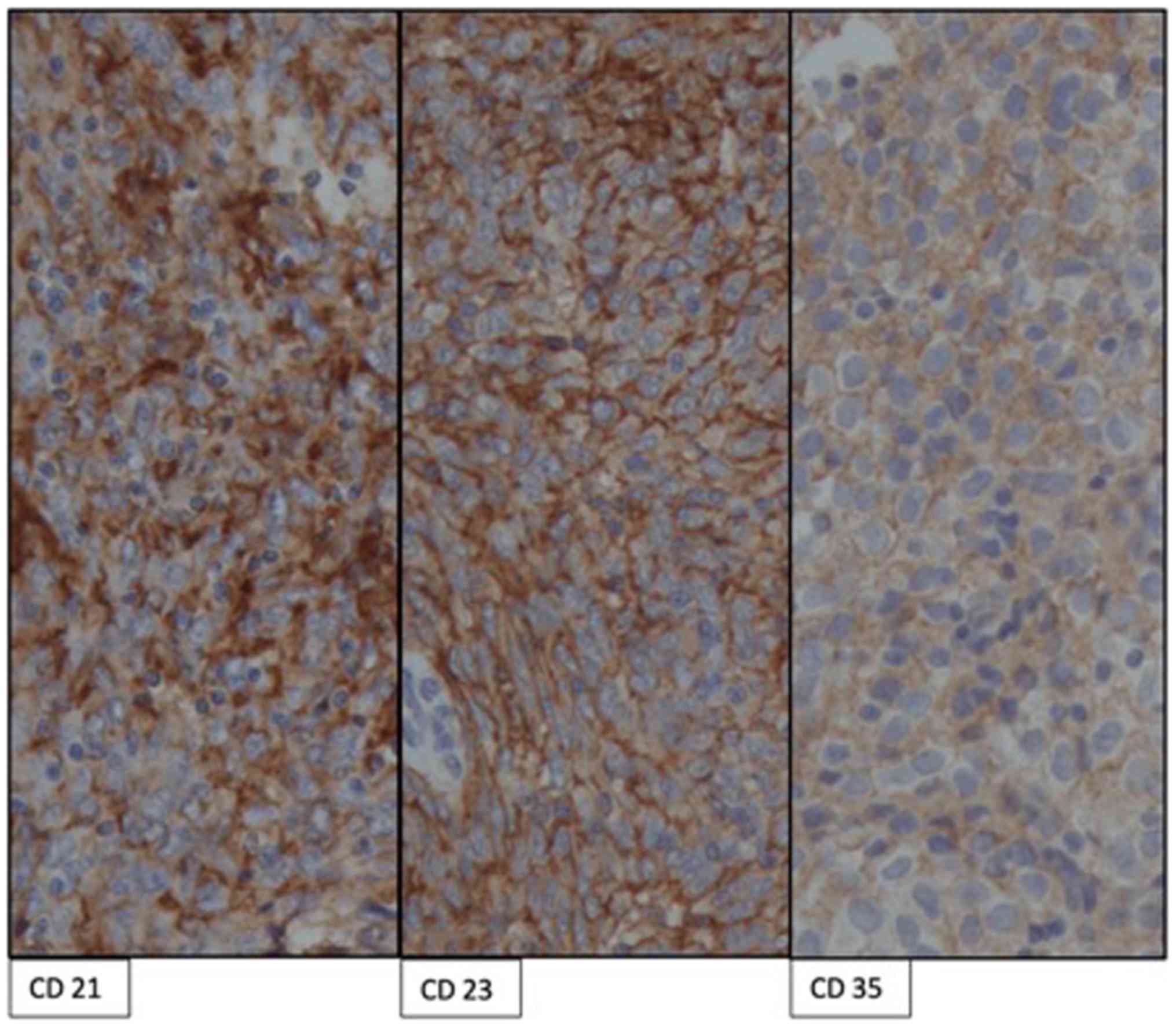
Retrospectively (in 2018) samples from all
operations (using formalin-fixed and paraffin-embedded archival
samples from 2002, 2005, 2007, and 2008) were reevaluated
immunohistochemically (Fig. 4;
immunochemical micrographs; Table
I; immunohistochemial results) and analysed by molecular
pathology using next-generation sequencing (NGS).
Immunohistochemical staining was performed according to standard
procedures on a Leica Bond system (Leica Microsystems) using
monoclonal antibodies directed against CD21 (clone 1F8, 1:50;
Dako), CD23 (clone SP23, 1: 100; Thermo Fischer Scientific, Inc.),
CD35 (clone LRB25, 1:25; Cell Marque), and PD-L1 (Clone 28-8,
1:100; Dako). For NGS six sections of 10 µm thickness were cut from
FFPE tissue blocks. Sections were deparaffinised and the tumour
areas were macrodissected from unstained slides using a marked
haematoxylin-eosin (H&E) stained slide as a reference. After
proteinase K digestion, the DNA was isolated with the
Maxwell® 16 FFPE Plus Tissue LEV DNA purification kit
(Promega) on the Maxwell® 16 (Promega) following
manufacturer's instructions. The DNA content was measured using
quantitative PCR (qPCR).
For multiplex PCR-based target enrichment, the
isolated DNA (10 ng each) was amplified with a customised GeneRead
DNAseq Targeted Panel V2 (Qiagen) and the GeneRead DNAseq Panel PCR
kit V2 (Qiagen) according to the GeneRead DNASeq Gene Panel
handbook (Qiagen). The custom panel comprised a subset of cancer
relevant genes including: BRAF, CDK4, CDKN2A, GNA11, GNAQ, HRAS,
IDH1, KIT, KNSTRN, KRAS, NRAS, OXA1L, PDGFRA, PIK3CA, PTEN, RAC1
and TP53.
Libraries were constructed using the Gene Read DNA
Library I Core kit and the Gene Read DNA I Amp kit (Qiagen). After
end-repair and adenylation, NEXTflex DNA Barcodes were ligated (Bio
Scientific). Barcoded libraries were amplified and then the final
library product was quantified with QuantiFluor dsDNA System
(Promega) on the Quantus Fluorometer (Promega), diluted and pooled
in equal amounts. Finally, 12 pM of the constructed libraries were
sequenced on the MiSeq (Illumina) with a MiSeq reagent kit V2
(300-cycles; Illumina) following the manufacturer's
recommendations.
Data were exported as FASTQ files. Alignment and
annotation was done using a modified version of a previously
described method (23). BAM files
were visualised in the Integrative Genomics viewer (http://www.broadinstitute.org/igv/). A 5% cut-off
for variant calls was used and results were only interpreted if the
coverage was >200x.
Discussion
Because of the rarity of FDCS, there is no
standardized or even guideline-based treatment of the tumour.
Therefore, treatment modalities can differ significantly. Depending
on its supposed origin (stromal or lymphoid) the tumour is treated
differently.
On the one hand FDCS is treated similar to sarcoma
by surgery. Surgical excision has proven successful in unilocular
FDCS (18-20)
Amin at al. for example reported a case of FDCS of the head and
neck which was treated by surgical excision. No neck dissection was
performed. Their patient showed no recurrence after two years
(12). Surgery in combination with
adjuvant chemo- or radiotherapy has also been attempted in cases of
multilocular FDCS (20,21). Pisani et al (24), treated FDCS of the head and neck by
surgical excision and five courses of adjuvant chemotherapy with
COP plus (PEG)-liposomal doxorubicin. Nevertheless, in localised
FDCS adjuvant treatment showed no significant effect on overall
survival (22).
On the other hand FDCS is treated like lymphoid
tumours by chemotherapy with cyclophosphamide, doxorubicin,
vincristine, and prednisone (CHOP) or CHOP-like regimens. As
immunotherapeutial and chemotherapeutical options increase due to
advances in research and technology, there are more therapeutic
attempts coming from this field. Choi et al (13), reported a case of FDCS in which the
patient was treated with a CHOP regimen. The outcome was a partial
response after two cycles. High recurrence rates could be a result
of not yet elaborated regimens. Roesch et al (25), for example hypothesized in 2014 that
intensive chemotherapies lead to a depletion of immune cells
allowing an early regrowth of the tumour.
Our patient tested positive for CD21, CD23, D2-40
and Vimentin, partially positive for CD68, and negative for CD35
(except in 2007) in every sample taken (Table I). This indicates an apparently low
evolution of the tumour over a long period of time. In NGS no
somatic mutation was detected, all genes were wild type. This
combination could be specific for a locally less aggressive and
only slowly progressive tumour with a low malignant potential.
Furthermore, it might indicate a high recurrence rate. Our case is
unique because although there were many recurrences (indeed, this
many recurrences in one patient haven't been described before) in
different locations of the neck, the patient refused to obtain any
treatment other than surgery. This case raises the question whether
the excisions left behind vital tumour tissue giving raise to the
recurrences or if there is some kind of local (micro-) metastasis
in lymph nodes occurring in FDCS causing further spread. After the
4th recurrence a comprehensive neck dissection was performed.
Following that, the patient has been recurrence-free for over ten
years. A more extensive surgical approach might therefore, in the
individual case, prevent regrowth and can lead to a full recovery
even in multiple recurrences.
Molecular technologies like whole transcriptome
sequencing (WTS) have not only revealed new markers for FDC, such
as FDCSP or serglycin (26), but
they also might open the door to definitively clear the
histogenesis of FDCs and to study the immunological
microenvironment (27). Those
techniques are expected to lead to new targeted drug therapies for
FDCS in the future. Even though it might be challenging, research
has to be continued in order to fully understand the function and
progenitors of follicular dendritic cells. Only if FDCs are fully
understood, a way for adequate therapy for FDC Sarcoma can be
developed.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analysed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
LS wrote the manuscript. JL, NK, MR and RD revised
the manuscript critically. CH and PL performed and interpreted the
histopathological and immunohistochemical staining in 2018. PK was
involved in the earlier histopathological and immunohistochemical
staining. CS collected samples, performed sonographies, was the
leading surgeon and had the idea to publish this case. All authors
read and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
van Nierop K and de Groot C: Human
follicular dendritic cells: Function, origin and development. Semin
Immunol. 14:251–257. 2002.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Jarjour M, Jorquera A, Mondor I, Wienert
S, Narang P, Coles MC, Klauschen F and Bajénoff M: Fate mapping
reveals origin and dynamics of lymph node follicular dendritic
cells. J Exp Med. 211:1109–1122. 2014.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Aguzzi A, Kranich J and Krautler NJ:
Follicular dendritic cells: Origin, phenotype, and function in
health and disease. Trends Immunol. 35:105–113. 2014.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Cyster JG, Ansel KM, Reif K, Ekland EH,
Hyman PL, Tang HL, Luther SA and Ngo VN: Follicular stromal cells
and lymphocyte homing to follicles. Immunol Rev. 176:181–193.
2000.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Allen CD and Cyster JG: Follicular
dendritic cell networks of primary follicles and germinal centers:
Phenotype and function. Semin Immunol. 20:14–25. 2008.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Wang X, Cho B, Suzuki K, Xu Y, Green JA,
An J and Cyster JG: Follicular dendritic cells help establish
follicle identity and promote B cell retention in germinal centers.
J Exp Med. 208:2497–2510. 2011.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Bajénoff M, Egen JG, Koo LY, Laugier JP,
Brau F, Glaichenhaus N and Germain RN: Stromal cell networks
regulate lymphocyte entry, migration, and territoriality in lymph
nodes. Immunity. 25:989–1001. 2006.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Ansel KM, Ngo VN, Hyman PL, Luther SA,
Förster R, Sedgwick JD, Browning JL, Lipp M and Cyster JG: A
chemokine-driven positive feedback loop organizes lymphoid
follicles. Nature. 406:309–314. 2000.PubMed/NCBI View
Article : Google Scholar
|
|
9
|
Usui K, Honda S, Yoshizawa Y,
Nakahashi-Oda C, Tahara-Hanaoka S, Shibuya K and Shibuya A:
Isolation and characterization of naïve follicular dendritic cells.
Mol Immunol. 50:172–176. 2012.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Muñoz-Fernández R, Blanco FJ, Frecha C,
Martín F, Kimatrai M, Abadía-Molina AC, García-Pacheco JM and
Olivares EG: Follicular dendritic cells are related to bone marrow
stromal cell progenitors and to myofibroblasts. J Immunol.
177:280–289. 2006.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Monda L, Warnke R and Rosai J: A primary
lymph node malignancy with features suggestive of dendritic
reticulum cell differentiation. A report of 4 cases. Am J Pathol.
122:562–572. 1986.PubMed/NCBI
|
|
12
|
Amin Z, Suhaimi Y and Ahmad R: Head and
neck follicular dendritic cell sarcoma: Disease associations and
treatment review. Med J Malaysia. 65:77–79. 2010.PubMed/NCBI
|
|
13
|
Choi BS, Baek JH, Shin YM, Kim JH, Kim HW,
Lee SJ and Cha HJ: Follicular dendritic cell sarcoma: A case report
and review of the literature. Cancer Res Treat. 42:121–124.
2010.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Chan JK, Fletcher CD, Nayler SJ and Cooper
K: Follicular dendritic cell sarcoma. Clinicopathologic analysis of
17 cases suggesting a malignant potential higher than currently
recognized. Cancer. 79:294–313. 1997.PubMed/NCBI
|
|
15
|
Vermi W, Lonardi S, Bosisio D, Uguccioni
M, Danelon G, Pileri S, Fletcher C, Sozzani S, Zorzi F, Arrigoni G,
et al: Identification of CXCL13 as a new marker for follicular
dendritic cell sarcoma. J Pathol. 216:356–364. 2008.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Krautler NJ, Kana V, Kranich J, Tian Y,
Perera D, Lemm D, Schwarz P, Armulik A, Browning JL, Tallquist M,
et al: Follicular dendritic cells emerge from ubiquitous
perivascular precursors. Cell. 150:194–206. 2012.PubMed/NCBI View Article : Google Scholar
|
|
17
|
El Shikh ME, El Sayed RM, Sukumar S,
Szakal AK and Tew JG: Activation of B cells by antigens on
follicular dendritic cells. Trends Immunol. 31:205–211.
2010.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Han JH, Kim SH, Noh SH, Lee YC, Kim HG and
Yang WI: Follicular dendritic cell sarcoma presenting as a
submucosal tumor of the stomach. Arch Pathol Lab Med.
124:1693–1696. 2000.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Katano H, Kaneko K, Shimizu S, Saito T,
Irié T and Mori S: Follicular dendritic cell sarcoma complicated by
hyaline-vascular type Castleman's disease in a schizophrenic
patient. Pathol Int. 47:703–706. 1997.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Perez-Ordonez B, Erlandson RA and Rosai J:
Follicular dendritic cell tumor: Report of 13 additional cases of a
distinctive entity. Am J Surg Pathol. 20:944–955. 1996.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Toyoda K, Taniguchi J, Kikawa K, Uike N,
Haraoka S, Ooshima K, Kikuchi M and Kawanishi H: Follicular
dendritic cell sarcoma: Ultrastructural and immunohistochemical
studies. Intern Med. 39:950–955. 2000.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Chow SC, Yeung EC, Ng CS, Wong RH, Fai To
K and Wan IY: Mediastinal follicular dendritic cell sarcoma with
paraneoplastic pemphigus. Asian Cardiovasc Thorac Ann. 23:732–734.
2015.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Peifer M, Fernández-Cuesta L, Sos ML,
George J, Seidel D, Kasper LH, Plenker D, Leenders F, Sun R, Zander
T, et al: Integrative genome analyses identify key somatic driver
mutations of small-cell lung cancer. Nat Genet. 44:1104–1110.
2012.PubMed/NCBI View
Article : Google Scholar
|
|
24
|
Pisani F, Marino M, Sentinelli S and Petti
MC: Follicular dendritic cell sarcoma of the neck: Report of a case
treated by surgical excision and COP plus (PEG)-liposomal
doxorubicin. J Exp Clin Cancer Res. 27(33)2008.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Roesch K, Hasenclever D and Scholz M:
Modelling lymphoma therapy and outcome. Bull Math Biol. 76:401–430.
2014.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Lorenzi L, Döring C, Rausch T, Benes V,
Lonardi S, Bugatti M, Campo E, Cabeçadas J, Simonitsch-Klupp I,
Borges A, et al: Identification of novel follicular dendritic cell
sarcoma markers, FDCSP and SRGN, by whole transcriptome sequencing.
Oncotarget. 8:16463–16472. 2017.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Laginestra MA, Tripodo C, Agostinelli C,
Motta G, Hartmann S, Döring C, Rossi M, Melle F, Sapienza MR,
Tabanelli V, et al: Distinctive histogenesis and immunological
microenvironment based on transcriptional profiles of follicular
dendritic cell sarcomas. Mol Cancer Res. 15:541–552.
2017.PubMed/NCBI View Article : Google Scholar
|