Introduction
Glioblastoma (GBM) is the most common adult
malignant brain tumor and has a uniquely poor prognosis. Median
survival is 14-16 months, and overall survival (OS) at 2 years is
27.2 and 9.8% at 5 years (1-3).
Standard of care treatment consists of maximal safe resection of
the enhancing portion of the tumor followed by 30 times 2 Gray
daily fractionated intensity-modulated radiation therapy (IMRT)
with concomitant temozolomide (TMZ) dosed at 75
mg/m2/day. This is followed by at least six cycles of
five daily doses of TMZ (150 mg/m2 for the first month
and 200 mg/m2 for subsequent treatments) with each cycle
being 28 days long (3).
Temozolomide is an oral alkylating agent that leads
to the formation of specific DNA adducts almost exclusively
repaired by O6-methylguanine-DNA methyltransferase
(MGMT) (4). In rapidly dividing
cells, there is less time for the repair to take place, allowing
for selective damage or killing of GBM cells (5). GBM tumor cells and somatic cells,
including bone marrow progenitors, largely share MGMT polymorphisms
and promoter methylation status. The limiting toxicity of TMZ is
myelosuppression (particularly thrombocytopenia) and is thought to
be due to low MGMT activity in hematopoietic progenitors (6). If severe myelosuppression occurs, the
current practice is to stop or reduce the dose of TMZ to limit the
risk of complications and allow for marrow recovery. For efficient
treatment, however, the dose of TMZ should be adjusted according to
individual MGMT activities (7).
MGMT activity assays are available for research but not for routine
clinical use. A surrogate marker of somatic MGMT repair activity
during TMZ treatment may be myelosuppression.
Studies using various chemotherapies other than TMZ
have suggested that greater toxicity to certain organ systems may
reflect increased potency of the drug and is therefore associated
with better treatment effect, including longer progression-free
survival (PFS) (8-10).
Recent reports suggest that decreases in platelet count and white
blood cell count in the setting of TMZ use is associated with
increased OS in GBM patients (11-13).
Our objective is to reproduce this finding and verify whether
leukopenia in the setting of TMZ use is associated with increased
OS in GBM patients at our institution.
Materials and methods
Patients
To be included in the study, patients must have
histologically confirmed GBM and exposure to TMZ. Baseline and
follow-up complete blood counts (CBC) were stored in the Beth
Israel Deaconess Medical Center's electronic medical record system
as part of routine clinical care. Patients were not excluded for
any other reason such as demographics, clinical or radiologic
outcomes. One hundred and forty-one patients met inclusion
criteria. Age, sex, extent of surgical resection (categorized as
biopsy, partial resection, and complete resection), radiation dose,
and chemotherapy treatments were recorded. CBCs were recorded at
baseline (defined as the most recent set of laboratory results
prior to TMZ exposure) and at various time points available
throughout the patient's course of TMZ up to six cycles of adjuvant
TMZ. The primary endpoint was OS, and the secondary end point was
PFS. This study was reviewed and approved by the Institutional
Review Board of Beth Israel Deaconess Medical Center (Boston, MA).
Patients were retrospectively identified using a database of GBM
patients seen at Beth Israel Deaconess Medical Center between
January 2012 and December 2017.
Data collection and statistical
analysis
The severity of leukopenia was classified based on
the National Cancer Institute's Common Terminology Criteria for
Adverse Events (CTCAE version 5.0). OS was measured from the date
of tissue diagnosis to the date of death due to any cause. Patients
who were still alive by July 2020 were censored. Kaplan-Meier
analysis with log rank and Cox multivariate proportional hazards
analysis were performed using statistical computing language and
survival analysis libraries (R version 4.0.2, R Foundation, Vienna,
Austria; ‘survival’ library version 3.2-3; ‘survminer’ library
version 0.4.8). Individual de-identified participant data used in
this publication, including patient age, sex, extent of surgery,
length of TMZ treatment, radiation dose, time to progression, time
to death, baseline WBC and nadir WBC is available as supplementary
material for download (Table
SI).
Results
Patient characteristics
Between January 2012 and December 2017, 141
biopsy-proven GBM patients exposed to TMZ were retrospectively
identified. Patient characteristics were comparable with respect to
sex, extent of surgical resection, and fraction of patients
completed six weeks of IMRT/TMZ followed by six cycles of adjuvant
TMZ (Table I). The BIDMC cohort was
older than the reference cohort (3) with a median age of
64 compared to 56, respectively. There were 26 patients younger
than 50 years and 115 patients 50 years of age or older. The median
age was 64 (range 18-90). 88 of 141 patients completed the planned
course of IMRT and concomitant TMZ with at least six cycles of
adjuvant TMZ. Reasons for stopping or decreasing the dose of TMZ
are listed in Table II. 53
patients stopped TMZ treatment (37.6%). Of these, hematologic
toxicity (n=20, 14.2%) and progression of disease (n=29, 20.6%)
were the two main reasons. Seventy five patients developed
leukopenia, and 95 patients developed thrombocytopenia. IDH1 R132H
mutation was identified in five patients, absent in 89 patients,
and data was not available in 47 patients. The median OS for all
141 patients was 19 months, and the median PFS was 8 months. There
were no treatment-associated deaths.
 | Table IComparison of patient demographics at
time of study between the BIDMC cohort and the reference
cohort. |
Table I
Comparison of patient demographics at
time of study between the BIDMC cohort and the reference
cohort.
| Characteristic | BIDMC cohort
(n=141) | Reference
cohorta (n=287) |
|---|
| Age, years |
|
Median | 64 | 56 |
|
Range | 18-90 | 19-70 |
| Age, years, n
(%) |
|
<50
years | 26(18) | 90(31) |
|
≥50
years | 115(82) | 197(69) |
| Sex, n (%) |
|
Male | 76(54) | 185(64) |
|
Female | 65(46) | 102(36) |
| Surgery, n (%) |
|
Biopsy | 40(28) | 48(17) |
|
Partial
resection | 30(21) | 126(44) |
|
Complete
resection | 71(50) | 113(39) |
| IMRT/TMZ + cTMZ, n
(%) |
|
Completed | 88(62) | 105(37)a |
|
Did not
complete | 53(38) | 182(63) |
| Median OS,
months | 19 | 14.6 |
| Median PFS,
months | 8 | 6.9 |
| Table IIReasons for discontinuation of
intensity-modulated radiation therapy/TMZ and 6 cycles of adjuvant
TMZ. |
Table II
Reasons for discontinuation of
intensity-modulated radiation therapy/TMZ and 6 cycles of adjuvant
TMZ.
| Complication | Number affected
(%) |
|---|
| Disease
progression | 29 (20.6) |
| Bone marrow
toxicity | 20 (14.2) |
| Dysphagia | 1 (0.7) |
| Cerebral
hemorrhage | 1 (0.7) |
| Cardiac arrest
(unrelated) | 1 (0.7) |
| Heart failure
(unrelated) | 1 (0.7) |
| Total | 53 (37.6) |
Correlation of leukopenia with
survival
Younger patient age (<50 years old) and
development of leukopenia correlated with increased OS. Median OS
for patients younger than 50 years old was 22 months compared to 16
months in patients 50 years of age and older (P=0.006). There is a
significant increase in OS in patients who develop leukopenia
(P=0.008). In patients with leukopenia, median OS was 21 months
compared to 14 months in those without leukopenia (P=0.008;
Table III). Subgroup analysis
showed that leukopenia in patients with IDH1 R132H mutation does
not correlate with increased OS, although the numbers are low.
While sex was not a significant determinant of outcomes, completion
of IMRT/TMZ with cyclic TMZ was associated with longer OS. Patients
who had total resections had a median OS of 21 months compared to
14 months in patients with partial resections or biopsies
(P=0.063). Those who completed the full course of IMRT/TMZ with six
cycles of adjuvant TMZ had a median OS of 20 months compared to
patients unable to complete the regimen (OS 14 months; P=0.030;
Table III). There was no
significant difference in median PFS in patients who developed
leukopenia (P=0.088). There was no significant difference in median
OS or PFS in patients who developed thrombocytopenia (P=0.082 and
P=0.928, respectively).
| Table IIIUnivariate survival analysis using
Kaplan Meier analysis and the log-rank test. |
Table III
Univariate survival analysis using
Kaplan Meier analysis and the log-rank test.
| Characteristic | Median PFS,
months | P-value | Median OS,
months | P-value |
|---|
| Age, years |
|
<50 | 7 | 0.262 | 22 | 0.006a |
|
≥50 | 8 | | 16 | |
| Sex |
|
Male | 8 | 0.324 | 20 | 0.742 |
|
Female | 8 | | 18 | |
| Extent of
resection |
|
Total | 9 | 0.707 | 21 | 0.063 |
|
Partial,
biopsy | 6 | | 14 | |
| IMRT/TMZ + cTMZ |
|
Completed | 9 | 0.108 | 20 | 0.030a |
|
Did not
complete | 6 | | 14 | |
| Platelet count |
|
No
thrombocytopenia | 6 | 0.082 | 20 | 0.928 |
|
Thrombocytopenia | 9 | | 17 | |
| WBC count |
|
No
leukopenia | 6 | 0.088 | 14 | 0.008a |
|
Leukopenia | 9 | | 21 | |
| IDH1 status |
|
IDH1 wild
type (89) | 8 | 0.697 | 16 | 0.287 |
|
IDH1
mutation (5) | 13 | | 23 | |
| WBC, absent IDH1
R132H |
|
No
leukopenia (46) | 6 | 0.116 | 13 | 0.053 |
|
Leukopenia
(43) | 9 | | 20 | |
| WBC, present IDH1
R132H |
|
No
leukopenia (2) | 12 | 0.432 | 30 | 0.586 |
|
Leukopenia
(3) | 13 | | 23 | |
| WBC, incomplete
IMRT/TMZ + cTMZ |
|
No
leukopenia (23) | 5 | 0.035 | 10 | 0.055 |
|
Leukopenia
(30) | 8 | | 17 | |
| WBC, IMRT/TMZ +
cTMZ |
|
No
Leukopenia (43) | 7 | 0.532 | 16 | 0.048 |
|
Leukopenia
(45) | 9 | | 24 | |
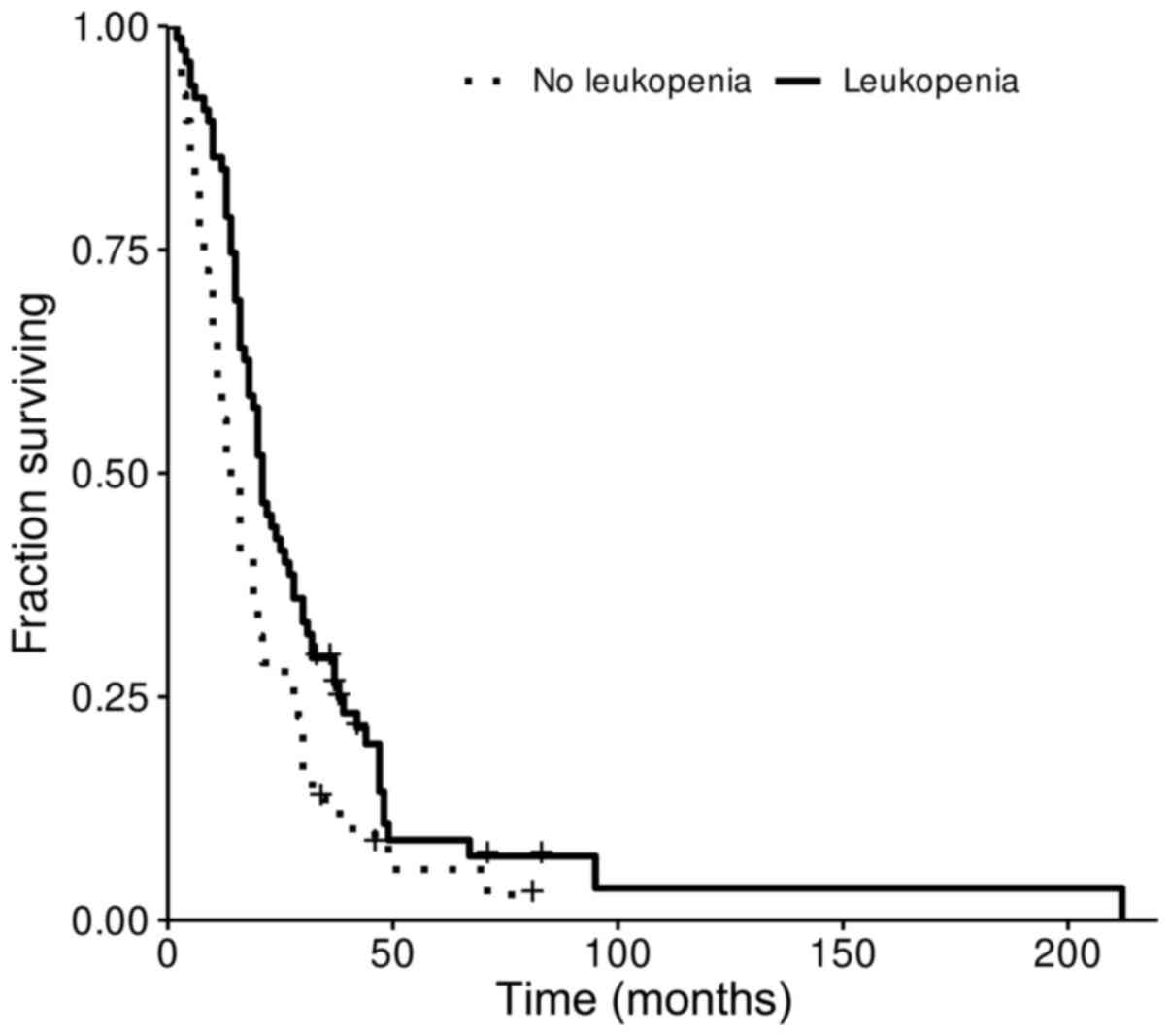
Correlation of leukopenia grade with
survival
Kaplan-Meier survival representation of the
correlation of leukopenia with OS is shown in Fig. 1. Of the patients who developed
leukopenia, those who developed grade 2 leukopenia had a median OS
of 28.5 months compared to 14 months in patients who maintained a
normal white blood cell count (P=0.024). When assessing OS in
patients with grades 1, 3, and 4 leukopenia compared to patients
who did not develop leukopenia, there was no significant difference
(P>0.05; Table IV).
Multivariate analysis using Cox proportional hazards model revealed
that leukopenia grade was associated with longer OS after taking
into account other known predictors of survival such as age, extent
of surgery, and completed standard TMZ (P=0.00205, likelihood ratio
test P=4.41e-09*; Table
V). In this analysis, age, extent of surgery and completion of
standard TMZ therapy were also highly associated with longer
OS.
| Table IVSurvival analysis of leukopenia grade
using Kaplan Meier analysis and log-rank test. |
Table IV
Survival analysis of leukopenia grade
using Kaplan Meier analysis and log-rank test.
| Grade | Patients, n
(%) | Median PFS,
months | P-value | Median OS,
months | P-value |
|---|
| 0 | 66(47) | 6 | | 14 | |
| 1 | 41(29) | 8 | 0.918 | 20 | 0.069 |
| 2 | 18(13) | 11 | 0.033a | 29 | 0.024a |
| 3 | 9(6) | 10 | 0.047a | 15 | 0.278 |
| 4 | 7(5) | 11 | 0.544 | 25 | 0.417 |
| Table VMultivariate analysis using Cox
proportional hazards model. |
Table V
Multivariate analysis using Cox
proportional hazards model.
| Variable | P-value | Hazard ratio (95%
CI) |
|---|
| Age |
5.92x10-6a | 1.03
(1.02-1.05) |
| Sex | 0.94627 | 0.99
(0.68-1.43) |
| Extent of
surgery |
0.00106a | 0.71
(0.57-0.87) |
| Leukopenia
grade |
0.00205a | 0.77
(0.65-0.91) |
| TMZ completed |
0.00252a | 1.80
(1.23-2.64) |
Discussion
In this study, we demonstrate that leukopenia in the
setting of TMZ exposure is an apparent predictor of improved OS in
GBM patients. Compared to a landmark reference study (3), our cohort was older (median age 56
compared to 64, respectively). The percentage of patients able to
complete six weeks of IMRT/TMZ followed by six cycles of TMZ was
similar, though the reasons for discontinuation differed. Whereas
14.2% of our patients stopped treatment or had treatment held for
hematologic toxicity, 17% of patients in the reference cohort
stopped treatment for bone marrow suppression. Thirty-nine percent
of patients in the reference cohort discontinued treatment due to
disease progression compared to 20.6% of our patients. The
reference cohort had a median OS of 14.6 months and a median PFS of
6.9 months while our cohort had a median OS of 19 months and a
median PFS of 8 months. Our data is limited in that we are unable
to determine the precise dose of corticosteroid exposure at the
time of TMZ treatment. A follow-up study to the landmark reference
study showed that corticosteroids can compromise survival in GBM
patients, and 67% of patients who were part of the reference cohort
were on corticosteroid therapy at the time of the study (14).
There have been three prior publications suggesting
that myelosuppression in the form of thrombocytopenia or
neutropenia is associated with better OS in patients who have had
surgery, radiation, and TMZ. The initial study found that during
six weeks of radiation with concomitant TMZ in 84 patients, a
decrease in platelet count compared to baseline correlated with
prolonged OS whereas changes in lymphocyte count showed no such
correlation (13). Lymphocyte count
was chosen as a general marker for myelosuppression as this was
more common than neutropenia. Neutrophil count and general
leukopenia were not evaluated. The second study reviewed changes in
neutrophil count during the course of standard treatment for
correlation with survival (12). It
was reported that MGMT promoter methylation, wild type EGFR status,
younger age at diagnosis, and treatment-induced decreases in white
blood cell (WBC) count in 86 patients who completed the full
six-week course of IMRT/TMZ followed by six cycles of adjuvant TMZ
had increased median OS. IDH1 R132H mutation and MGMT promoter
methylation did not correlate with changes in WBC counts. In our
study, patients who were unable to complete the standard treatment
of six weeks IMRT/TMZ with six cycles of adjuvant TMZ were not
excluded. Instead, all patients who were exposed to TMZ were
included to assess bone marrow suppression and survival.
The third study assessed the change in neutrophil
count in 50 patients with absent IDH1 R132H mutation during the
initial six weeks of IMRT/TMZ only (11). They found that patients with greater
than or equal to a 40% decrease in neutrophils showed significantly
longer OS than those with less than a 40% decrease. They also
report that extent of resection, MGMT status, decreased rate of WBC
count, and decreased rate of platelet count were associated with
increased median OS by univariate analysis. After adjusting for
various factors, however, only the decrease in neutrophils remained
significant. In our subset of IDH1 R132H negative patients, OS
between patients who developed leukopenia and those who did not
with any TMZ exposure approached statistical significance (P=0.05).
Our patients with IDH1 R132H mutation did not have increased OS,
probably the result of the small sample size (n=5). Another prior
study evaluated platelet count as a marker of outcomes in this
setting and found that an increase in platelet count during
chemoradiation was associated with poor outcome (15). Platelet count, however, is unlikely
to be useful as biomarker of bone marrow suppression owing to
multiple factors that are unrelated to megakaryocyte activity such
as consumption rate and acute-phase induction.
The association of leukopenia with OS is not fully
understood. We hypothesize that TMZ causes marrow suppression
depending on MGMT repair activity, which in turn depends on factors
like TMZ clearance, MGMT promoter methylation, MGMT protein
expression, and polymorphisms and mutations affecting MGMT enzyme
stability and activity. Current dosing practices do not take into
account such individual differences, resulting in a large
proportion of patients experiencing dose-limiting toxicity due to
slow clearance and low MGMT repair activity. It can be assumed that
some patients are relatively under-dosed with TMZ due to fast TMZ
clearance or high MGMT repair activity (16). This raises the possibility that
there are patients who are relatively under-dosed with current
standard-of-care treatment and would do better with higher doses of
TMZ, perhaps on a protocol targeting brief nadirs of grade 2
leukopenia.
The limitations of this study include its
observational design and performance in a single-institution
involving a relatively small number of patients. Important clinical
data such as corticosteroid use and MGMT methylation status were
not available. This study does however confirm earlier reports of
the association between bone marrow suppression and improved OS in
GBM. For better understanding of this phenomenon, further studies
such as a randomized controlled TMZ dose escalation trial or a
two-tier dose stratification trial based on MGMT promoter
methylation is needed.
In conclusion, a possible interpretation of these
results is that grade 2 leukopenia is a biomarker of adequate TMZ
dosing in a population with diverse DNA repair function, which in
turn may be the consequence of variable MGMT activity. A
prospective dose escalation trial is necessary to determine if
treatment-induced leukopenia is beneficial for all patients
receiving TMZ.
Supplementary Material
Individual participant outcome
data.
Acknowledgements
The authors would like to thank Mrs. Julianne Bloom,
RN and Ms. Loretta Barron, NP (Brain Tumor Clinic, Department of
Neurology, Beth Israel Deaconess Hospital, Boston, USA) for
coordinating the care of our patients.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
KGH, EJU and ETW conceived and designed the study.
KGH drafted the article. ENU and KGH performed statistical
analysis. KGH, EJU and ETW critically revised the article. KGH,
EJU, ETW and ENU reviewed the submitted version of the manuscript.
All authors read and approved the final manuscript.
Ethics approval and consent to
participate
Ethical approval was obtained from the institutional
review board of the Dana Farber Harvard Cancer Center. The
Institutional Review Board waived the requirement for informed
consent due to retrospective design. Once the clinical data was
collected, all identifiers were removed.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Gilbert MR, Wang M, Aldape KD, Stupp R,
Hegi ME, Jaeckle KA, Armstrong TS, Wefel JS, Won M, Blumenthal DT,
et al: Dose-dense temozolomide for newly diagnosed glioblastoma: A
randomized phase III clinical trial. J Clin Oncol. 31:4085–4091.
2013.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Stupp R, Hegi ME, Mason WP, van den Bent
MJ, Taphoorn MJ, Janzer RC, Ludwin SK, Allgeier A, Fisher B,
Belanger K, et al: Effects of radiotherapy with concomitant and
adjuvant temozolomide versus radiotherapy alone on survival in
glioblastoma in a randomised phase III study: 5-year analysis of
the EORTC-NCIC trial. Lancet Oncol. 10:459–466. 2009.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Stupp R, Mason WP, van den Bent MJ, Weller
M, Fisher B, Taphoorn MJ, Belanger K, Brandes AA, Marosi C, Bogdahn
U, et al: Radiotherapy plus concomitant and adjuvant temozolomide
for glioblastoma. N Engl J Med. 352:987–996. 2005.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Tolcher AW, Gerson SL, Denis L, Geyer C,
Hammond LA, Patnaik A, Goetz AD, Schwartz G, Edwards T, Reyderman
L, et al: Marked inactivation of O6-alkylguanine-DNA
alkyltransferase activity with protracted temozolomide schedules.
Br J Cancer. 88:1004–1011. 2003.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Knizhnik AV, Roos WP, Nikolova T, Quiors
S, Tomaszowski K, Christmann M and Kaina B: Survival and death
strategies in glioma cells: Autophagy, senescence and apoptosis
triggered by a single type of temozolomide-induced DNA damage. PLoS
One. 8(e55665)2013.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Gerson SL, Phillips W, Kastan M, Dumenco
LL and Donovan C: Human CD34+ hematopoietic progenitors
have low, cytokine-unresponsive O6-alkylguanine-DNA
alkyltransferase and are sensitive to O6-benzylguanine plus BCNU.
Blood. 88:1649–1655. 1996.PubMed/NCBI
|
|
7
|
Newlands ES, Stevens MF, Wedge SR,
Wheelhouse RT and Brock C: Temozolomide: A review of its discovery,
chemical properties, pre-clinical development and clinical trials.
Cancer Treat Rev. 23:35–61. 1997.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Abola MV, Prasad V and Jena AB:
Association between treatment toxicity and outcomes in oncology
clinical trials. Ann Oncol. 25:2284–2289. 2014.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Di Maio M, Gridelli C, Gallo C, Shepherd
F, Piantedosi FV, Cigolari S, Manzione L, Illiano A, Barbera S,
Robbiati SF, et al: Chemotherapy-induced neutropenia and treatment
efficacy in advanced non-small-cell lung cancer: A pooled analysis
of three randomised trials. Lancel Oncol. 6:669–677.
2005.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Fontein DB, Seynaeve C, Hadji P, Hille ET,
van de Water W, Putter H, Kranenbarg EM, Hasenburg A, Paridaens RJ,
Vannetzel JM, et al: Specific adverse events predict survival
benefit in patients treated with tamoxifen or aromatase inhibitors:
An international tamoxifen exemestane adjuvant multinational trial
analysis. J Clin Oncol. 31:2257–2264. 2013.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Saito T, Sugiyama K, Hama S, Yamasaki F,
Takayasu T, Nosaka R, Muragaki Y, Kawamata T and Kurisu K:
Prognostic importance of temozolomide-induced neutropenia in
glioblastoma, IDH-wildtype patients. Neurosurg Rev. 41:621–628.
2018.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Vaios EJ, Nahed BV, Muzikansky A, Fathi AT
and Dietrich J: Bone marrow response as a potential biomarker of
outcomes in glioblastoma patient. J Neurosurg. 127:132–138.
2017.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Williams M, Liu ZW, Woolf D, Hargreaves S,
Michalarea V, Menashy R, Kooner I and Wilson E: Change in platelet
levels during radiotherapy with concurrent and adjuvant
temozolomide for the treatment of glioblastoma: A novel prognostic
factor for survival. J Cancer Res Clin Oncol. 138:1683–1688.
2012.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Pitter K, Tamagno I, Alikhanyan K,
Hosni-Ahmen A, Pattwell SS, Donnola S, Dai C, Ozawa T, Chang M,
Chan TA, et al: Corticosteroids compromise survival in
glioblastoma. Brain. 139:1458–1471. 2016.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Boonyawan K, Hess KR, Yang J, Long L, Wang
Q, Ezhilarasan R, Auia A, Alfaro-Munoz KD, de Groot JF, Bhat KP and
Sulman EP: A relative increase in circulating platelets following
chemoradiation predicts for poor survival of patients with
glioblastoma. Oncotarget. 8:90488–90495. 2017.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Armstrong TS, Cao Y, Scheurer ME,
Vera-Bolaños E, Manning R, Okcu MF, Bondy M, Zhou R and Gilbert MR:
Risk analysis of severe myelotoxicity with temozolomide: The
effects of clinical and genetic factors. Neuro Oncol. 11:825–832.
2009.PubMed/NCBI View Article : Google Scholar
|