Introduction
Chordoma is a rare malignancy with an incidence rate
of 0.8-5/100,000 per year (1-4).
Chordomas account for 1-4% of all bone malignancies and are
predominant in men and in the 50-70 years age group (1,5). Based
on histological characteristics, chordomas may be subclassified
into the typical, chondroid and dedifferentiated types. Chordomas
arise from undifferentiated remnant cells of the embryonal
notochord that reside within the axial skeleton (1). Although the mechanism underlying their
malignant transformation is largely unclear, mutations in the
brachyury gene have been frequently detected in chordoma patients
(6). Furthermore, 50-60% of the
tumors occur in the sacrococcygeal region, 25-35% at the skull base
and 10-15% in the mobile spine (7).
The clinical manifestations of chordoma depend on tumor location
and invasion, and typically include radiculopathy, deeply localized
pain and neurological deficits. Computed tomography (CT) and
magnetic resonance imaging (MRI) are the preferred methods for
determining chordoma extension into the bone and adjacent soft
tissues. The tumor masses appear as lytic lesions and may contain
areas of calcification on CT scans, and as iso- to hypointense on
T1-weighted MRI and hyperintense on T2-weighted MRI (1,5). The
most effective treatment is surgical excision, although it is
technically challenging due to the complex anatomical structure of
the affected sites. Therefore, postoperative complications and
recurrence are common, and the local recurrence rate is as high as
43-85% (8), whereas only 5% of the
tumors metastasize, typically to the lung, bone or brain. Pulmonary
metastasis of primary sacral and thoracic chordomas is rare. The
aim of the present study was to describe a rare case of sacral and
thoracic vertebral chordoma with pulmonary metastasis, and to
review the available literature on chordomas of the thoracolumbar
spine.
Case report
A 73-year-old man presented at the Department of
Orthopedic Surgery of the Second Affiliated Hospital of Inner
Mongolia Medical University in June 2018 with intermittent
lumbosacral pain and root pain of the lower limbs, which severely
affected his gait and gradually led to difficulty in defecating and
urinating. On inspection and palpation, a large soft tissue mass
was identified in the lumbosacral area. The patient had been
manifesting the symptoms for 8 years, and the lower back pain had
progressed in the preceding 2 years. The patient had also undergone
rectostomy and indwelling catheterization for incontinence 2 years
prior. The preoperative Nurick grade and McCormick score were 3 and
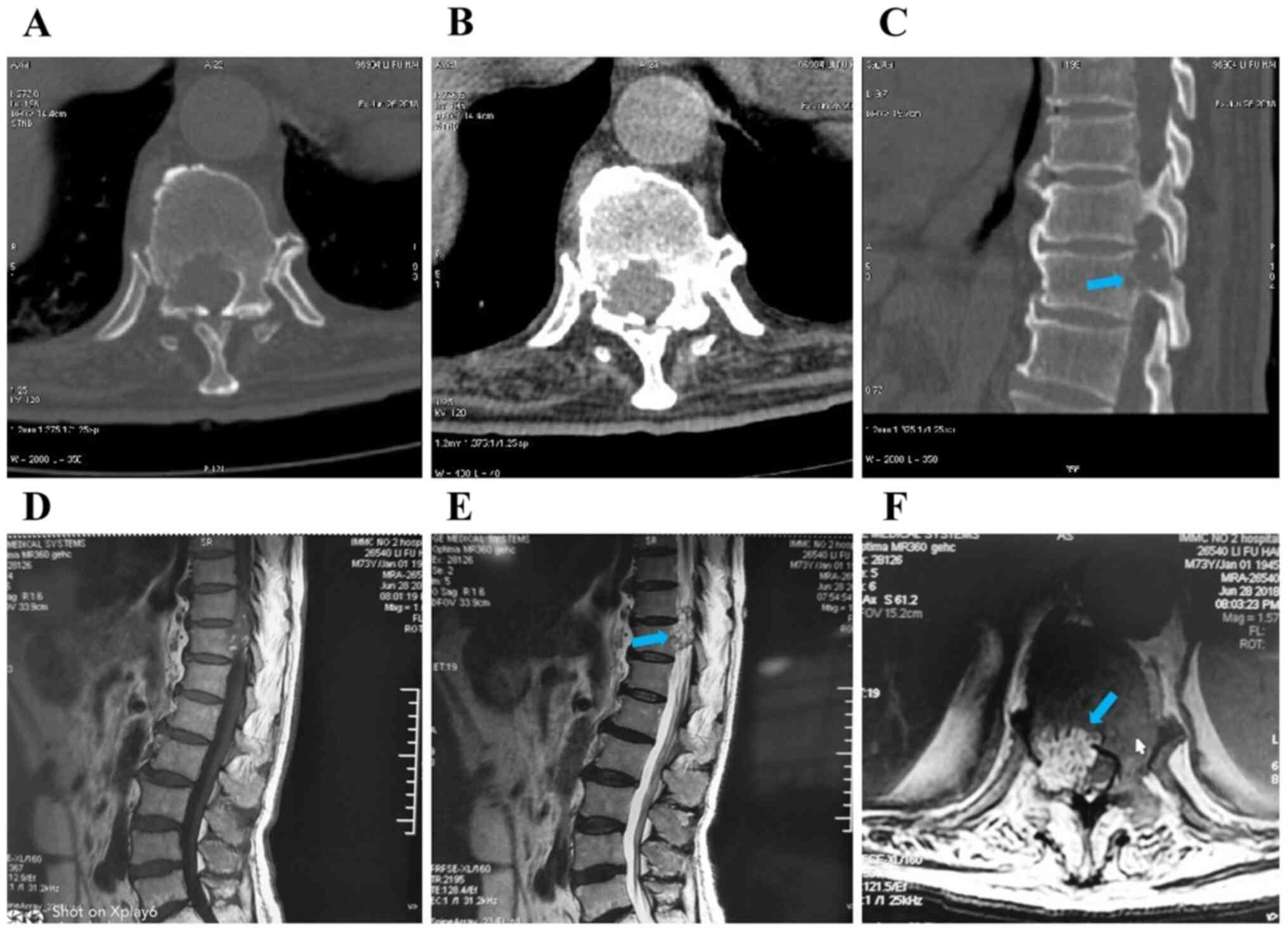
II, respectively. Thoracolumbar CT and MRI examinations revealed
bone destruction of the right medial wall of the spinal canal and
right pedicle of the T11 vertebra, protrusion of the soft tissue
mass into the spinal canal, with dural sac compression and shift to
the left (Fig. 1). In addition,
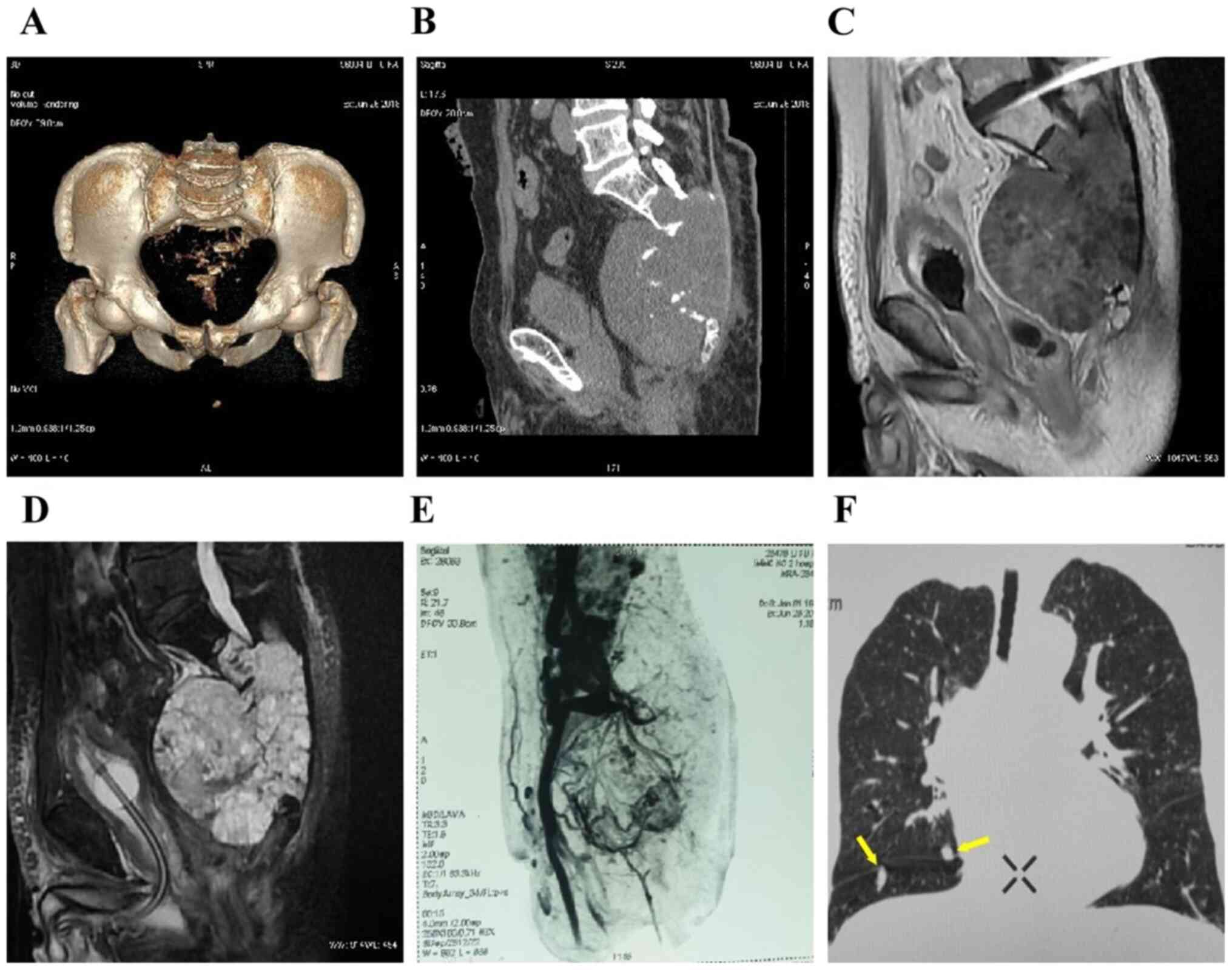
bone dissolution was observed below the S2 level, along with a
14x13x12.6-cm round soft tissue mass with a clear boundary, and an
irregular calcified spot (Fig.
2A-D). Pelvic angiography revealed abundant blood supply to the
tumor (Fig. 2E). Furthermore,
pulmonary CT scan revealed multiple dense nodules with a smooth
border, with a maximum diameter of ~0.95 cm, in both lungs
(Fig. 2F). The patient also
presented with hypertension, first-degree atrioventricular block
and cerebral infarction sequelae. Based on these findings, a
diagnostic biopsy was recommended.
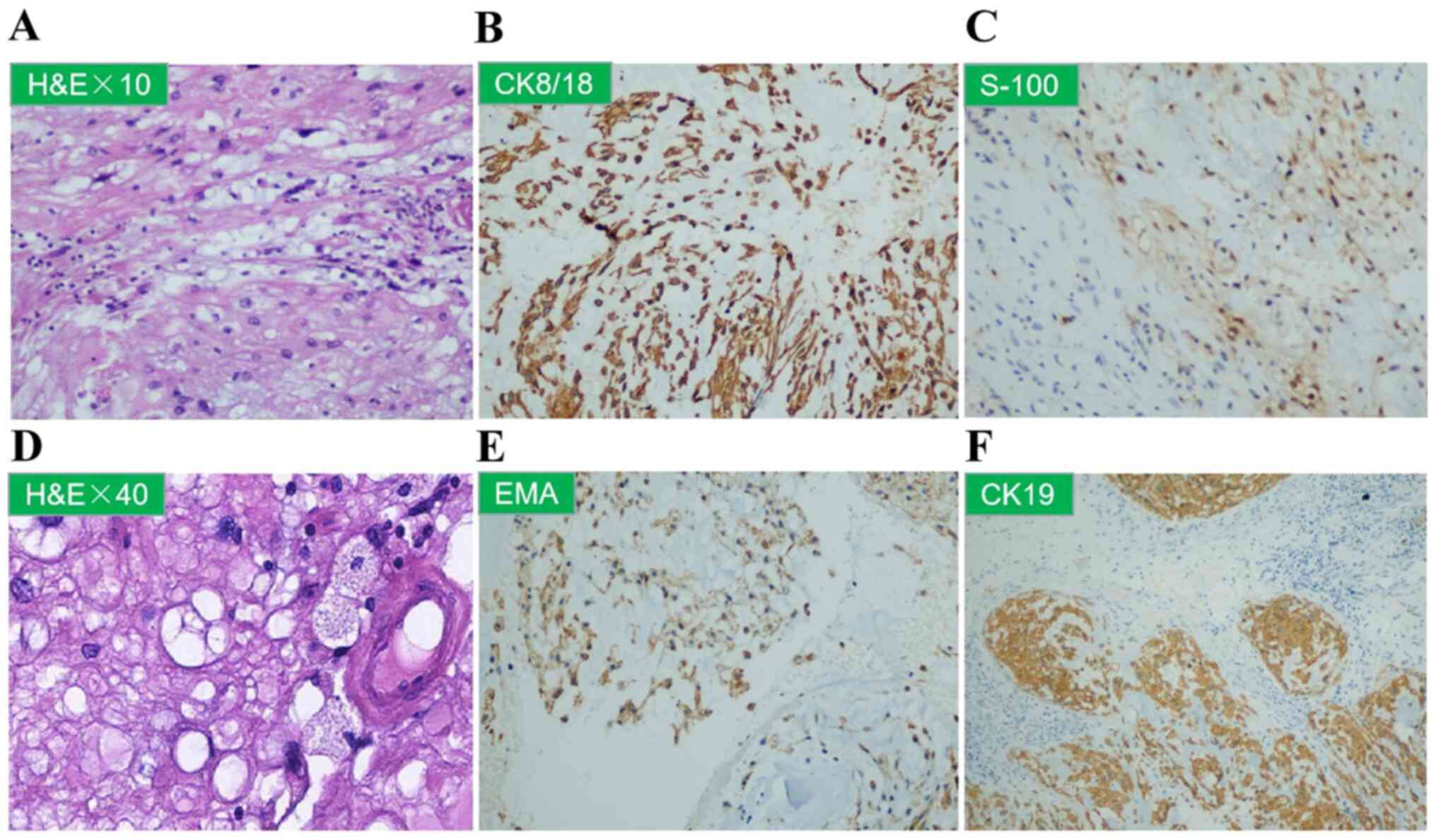
Sacral needle biopsy, hematoxylin-eosin and
immunohistochemical staining confirmed the diagnosis of chordoma
positive for AE1/AE3, S100 and cytokeratin (CK)8/18 expression
(Fig. 3A-C). Accordingly, the tumor
mass in the thoracic vertebrae was considered to be metastatic
chordoma. However, due to the risk of spinal cord injury, puncture
biopsies of the thoracic vertebral tumor were not performed.
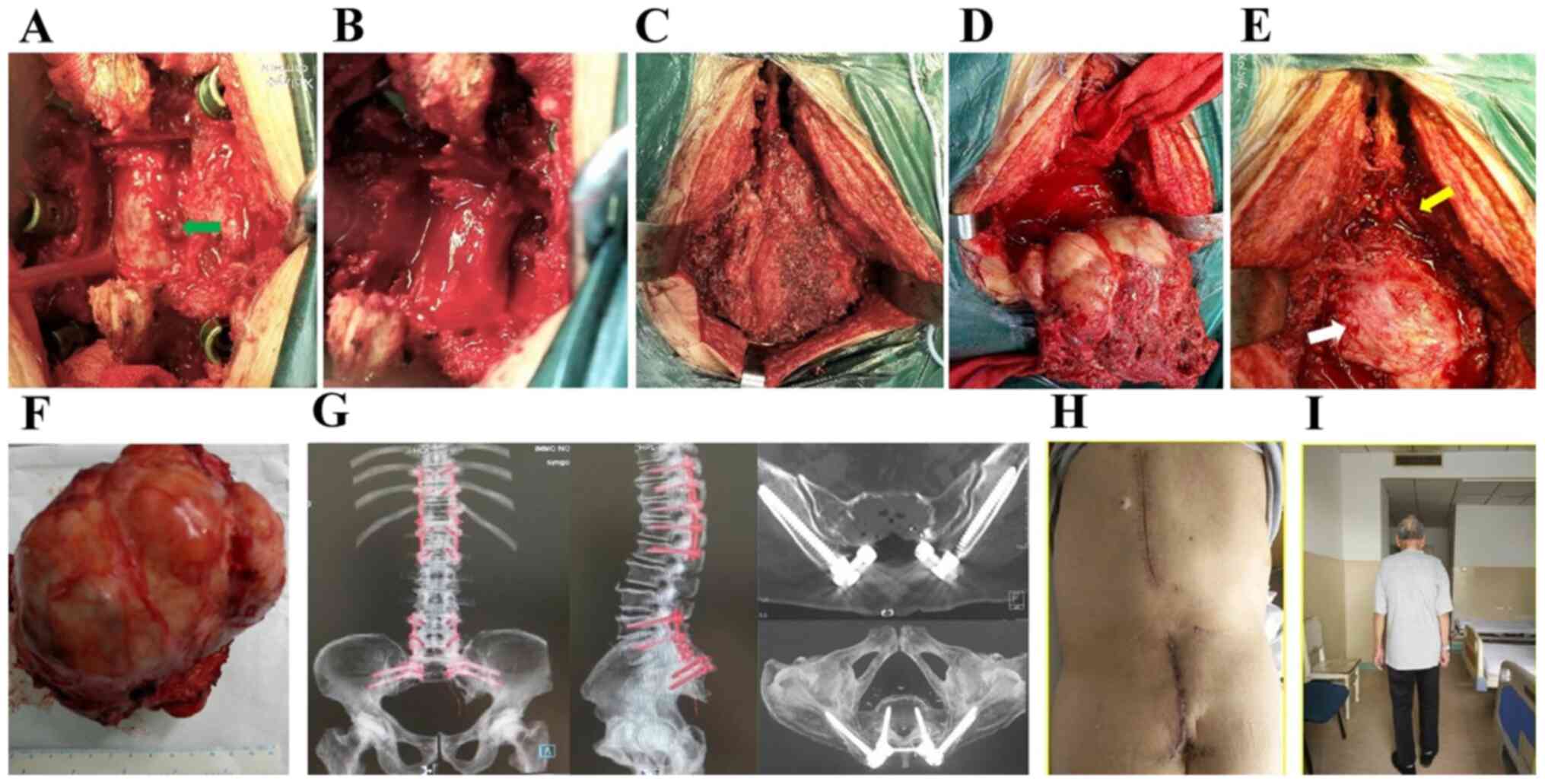
Posterior laminectomy and tumor curettage were used on the thoracic
vertebrae (Fig. 4A and B). On histopathological examination, the
T11 vertebral specimen exhibited cytoplasmic vacuolation (Fig. 3D), and was positive for epithelial
membrane antigen and CK19 (Fig. 3E
and F), and negative for CK7 and
chromogranin A expression, findings that were indicative of
chordoma.
The posterior median spinous process of the
lumbosacral spine (L3-S1, ~20 cm) were removed, and the L4-S1
bilateral lamina, superior and inferior articular processes,
bilateral iliac wings and positioning needle were exposed. Four
pedicle screws were fastened into both sides of L4 and L5. An
inverted ‘Y’ incision was extended to the distal end to reveal the
posterior sacrococcyx and sacroiliac joint, and the sacral mass was
extensively resected. Two iliac screws were fastened downwards on
both sides at the S1 level, and the connecting rods were installed
on the left and right sides, followed by locking and fixing the
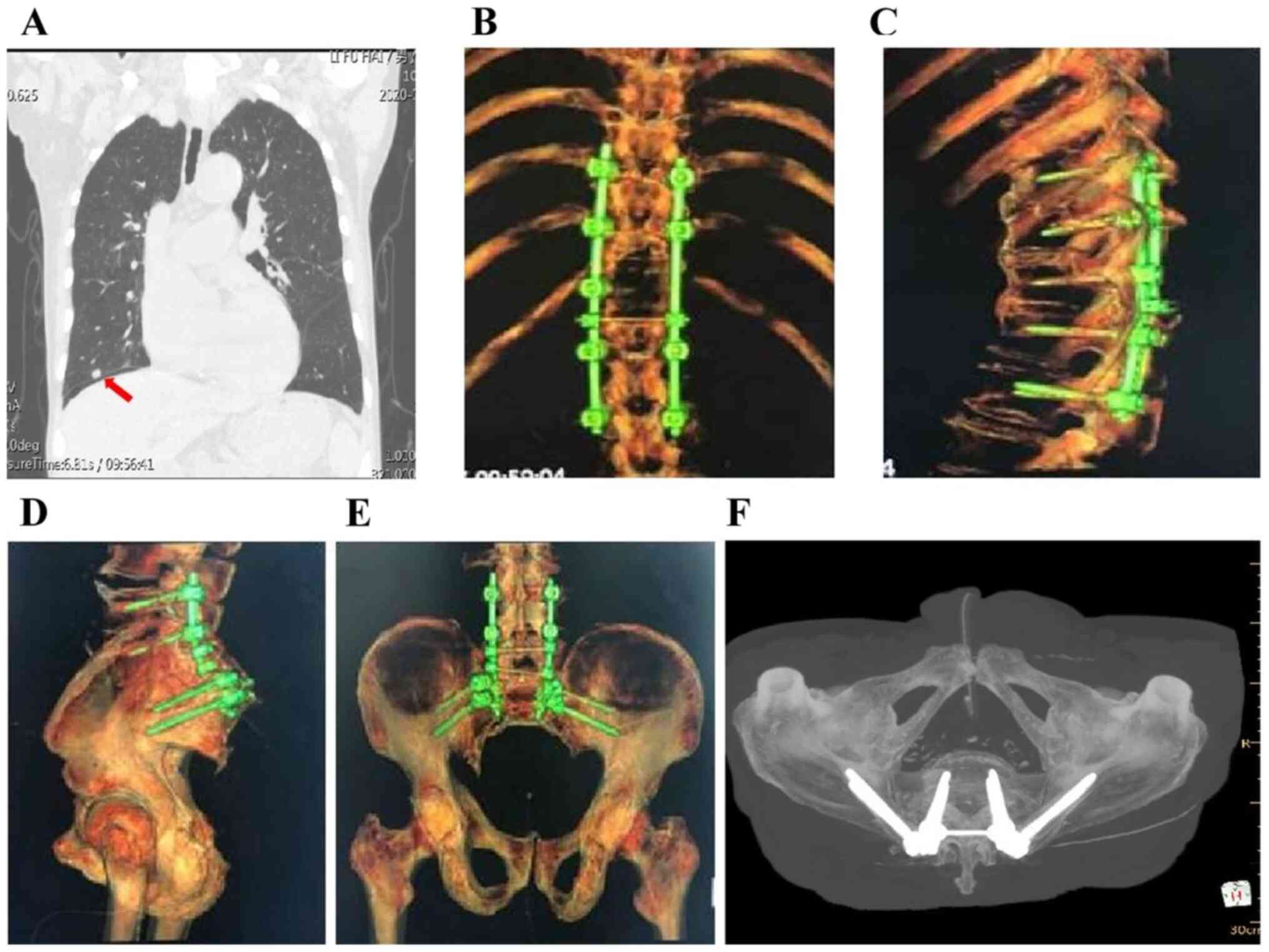
nuts (Fig. 4C-G). The volume of
intraoperative blood loss was ~3,000 ml. The patient did not
receive any chemotherapy or radiotherapy after surgery, and the
pulmonary X-ray at the 24-month follow-up revealed stable disease
(Fig. 5A). In addition, X-ray and
CT examination revealed stable internal fixation of the spine, and
there was no clinical or radiological evidence of local recurrence
or metastasis (Fig. 5B-F). The
patient achieved good spine stabilization and was able to walk and
perform daily activities without assistance. The postoperative
Nurick score decreased from grade 3 to grade 2, and the
postoperative McCormick grade was I. On the last follow-up (June
2020) the patient was in good overall condition with good mobility,
and the lung lesions were stable. Computed tomography
reconstruction of the thoracic vertebra and pelvis revealed no
loosening or fracture in the internal fixation, and no local tumor
recurrence.
Discussion
Chordomas are slow-growing,
low-to-intermediate-grade tumors that are often diagnosed at an
advanced stage with significant bony destruction and soft tissue
invasion (1,5). Chordomas may be falsely diagnosed as
relatively benign tumors, and their resection may be challenging
due to their high invasiveness. Therefore, chordoma resection is
associated with a high risk of morbidity and mortality. In
addition, the epidemiology of chordoma is unclear (9), particularly as regards its incidence
rates and the most frequently affected parts of the axial skeleton
(10,11). This is clinically significant, since
the symptoms and treatment strategies of chordoma largely depend on
its anatomical location (12,13).
Pain is the most common symptom of chordoma.
Furthermore, spinal cord or nerve root compression may result in
neurological symptoms, whereas nerve root involvement in the sacrum
leads to bowel and bladder dysfunction, including incontinence
(14). Although CT and MRI may be
used to determine the extent of chordoma lesions and facilitate
surgical planning, pathological examination following puncture
biopsy is the gold standard for diagnosing chordoma. Complete
surgical resection with negative margins may effectively reduce the
risk of local recurrence and distant metastasis (15,16).
Our patient had been experiencing intermittent lumbosacral pain and
root pain of the lower limbs over the previous 2 years, and
eventually developed incontinence. CT and MRI examination revealed
bone destruction of the right medial wall of the spinal canal and
right pedicle of the T11 vertebra, and a soft tissue mass with
well-defined boundaries protruding into the spinal canal, resulting
in dural sac compression. Therefore, posterior decompression of the
thoracic tumor was performed to reduce compression symptoms, and
the spine was stabilized by intravertebral fixation, followed by
extensive sacral tumor resection.
The 2020 NCCN guidelines (17) for the diagnosis and treatment of
sacrococcygeal or spinal chordomas recommend extensive resection of
operable lesions. Postoperative radiotherapy may be considered if
the resection margin is positive or if the soft tissue mass is
large (>7 cm in largest diameter). Surgical resection, whether
curative or subtotal, remains the gold standard for the treatment
of chordoma. It has been reported that the recurrence rate of
chordomas located in the sacrum and spine was 33% following
extensive resection and 67% after intracapsular or marginal
resection (18). Sacral chordomas
may be classified into proximal and distal types, depending on the
affected segments; the former involves the first and second
segments of the sacrum, and the latter originates from other
segments. A combined anteroposterior approach is considered as
appropriate for proximal sacrum chordoma and the posterior approach
for distal sacrum chordoma (19).
For S1 or S2 level tumors, resection via the posterior approach is
considered as adequate and is associated with an acceptable risk of
surgical complications. However, curative or complete resection is
difficult to achieve due to invasion of the tumor mass into the
vertebral body, spinal cord, nerve roots, peripheral nerves, or
other tissues. Therefore, only 10-20% of chordomas are curable by
surgery, and the postoperative recurrence rate is high (20).
Radiotherapy is often combined with surgery to
improve local control. A recent retrospective study reported that
the 5-year local control and survival rates were 85.4 and 81.9%,
respectively, in patients without surgical resection of chordoma
who were treated by photon or proton radiotherapy (21). A chordoma recurrence rate of >90%
has been reported following subtotal intratumoral resection and
radiotherapy, which may be attributed to incomplete tumor removal
(22). By contrast, Park et
al demonstrated that local radiotherapy after complete
resection improved the 5- and 10-year survival rates to 93 and 91%,
respectively (23). For patients
who are not candidates for surgical intervention due to underlying
conditions (e.g., compromised renal/cardiac function), radiation
therapy alone may be warranted. Chen et al (24) reported a 5-year survival rate of 78%
with high-dose radiation in a study on patients with chordoma who
were not deemed fit for surgery. Therefore, an initial tumor
debulking surgery followed by radiotherapy and chemotherapy, may be
a viable strategy. In addition, radiotherapy may also be used for
inoperable patients.
There is currently no clearly effective drug
recommended for the systemic treatment of chordoma. Imatinib and
sorafenib may delay disease progression or partially alleviate
symptoms in some cases (25-29).
Erlotinib and apatinib may also be administered (30,31).
However, conventional chemotherapy is not considered as a suitable
option for advanced chordomas, apart from cases with
well-differentiated tumors (32-34).
Despite the low risk (5%) of metastasis, the
prognosis of chordoma remains poor, with 5- and 10-year survival
rates of 50-68 and 28-40%, respectively (5). A retrospective analysis of 115
patients with sacral chordoma who underwent surgery revealed a
5-year overall survival rate of 81% over a mean follow-up duration
of 4.9 years (range, 1.3-10.8 years). The survival rates declined
in the initial 3 years and improved in the 4th year. The effect of
surgical margin and prior surgery were not correlated linearly with
conditional survival (35). Another
retrospective study on 171 patients with sacral chordoma recurrence
indicated metastasis in 17 cases (10.8%), including 5 with primary
pulmonary metastasis, 3 with bone metastasis (ribs and sternum) and
9 with postoperative pulmonary metastasis. Of the 14 patients with
pulmonary metastases, 9 succumbed to the disease, whereas 2
patients with rib metastases underwent rib resection and did not
develop any new lesions. A patient with spinal metastasis underwent
tumor removal and decompression, followed by a second surgery upon
recurred in the spine. Furthermore, local recurrence was identified
as the only significant risk factor for metastasis (36).
Based on the findings of the present case and those
of previous studies, it may be inferred that local progression and
recurrence are the most crucial prognostic factors of chordoma. In
addition, the extent of the initial surgical resection is also
prognostically significant. It was previously reported that age,
sex, treatment history, tumor location, pathological grade,
surgical margin, radiotherapy and chemotherapy affect the long-term
prognosis of chordoma patients (37). In the same cohort, younger age
(pediatric group), sacral location, dedifferentiated tumors and
chemotherapy were identified as independent risk factors of shorter
progression-free survival, whereas larger tumor size and tumor
necrosis have also been implicated as negative prognostic factors
(7).
Lumbosacral chordoma with pulmonary metastasis is
difficult to treat due to its anatomical location and high risk of
local recurrence. The case presented herein demonstrated that
radical surgery may effectively control the local recurrence or
distant metastasis of chordoma, whereas the combination of surgery
and postoperative adjuvant therapy may further improve patient
outcomes.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed in the present study
are included in this published article.
Authors' contributions
SBG and RB conceived and designed the study. SBG,
RB, ZQZ, YXW, WZ and CLL participated in the design of the study
and drafting of the manuscript. LSW and SXC performed anesthesia
and monitoring for surgery. SBG, RB, ZQZ, CLL, YXW and WZ reviewed
and edited the manuscript. All the authors have read and approved
the final version of the manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
the Second Affiliated Hospital of Inner Mongolia Medical
University.
Patient consent for publication
Written informed consent was obtained from the
patient for the publication of the case details and associated
images. A copy of the consent form is available for review.
Competing interests
All the authors declare that they have no competing
interests.
References
|
1
|
Walcott BP, Nahed BV, Mohyeldin A, Coumans
JV, Kahle KT and Ferreira MJ: Chordoma: Current concepts,
management, and future directions. Lancet Oncol. 13:e69–e76.
2012.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Ropper AE, Cahill KS, Hanna JW, McCarthy
EF, Gokaslan ZL and Chi JH: Primary vertebral tumors: A review of
epidemiologic, histological and imaging findings, part II: Locally
aggressive and malignant tumors. Neurosurgery. 70:211–219.
2012.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Chambers KJ, Lin DT, Meier J,
Remenschneider A, Herr M and Gray ST: Incidence and survival
patterns of cranial chordoma in the United States. Laryngoscope.
124:1097–1102. 2014.PubMed/NCBI View Article : Google Scholar
|
|
4
|
McMaster ML, Goldstein AM, Bromley CM,
Ishibe N and Parry DM: Chordoma: Incidence and survival patterns in
the United States, 1973-1995. Cancer Causes Control. 12:1–11.
2001.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Sciubba DM, Chi JH, Rhines LD and Gokaslan
ZL: Chordoma of the spinal column. Neurosurg Clin N Am. 19:5–15.
2008.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Jahangiri A, Jian B, Miller L, El-Sayed IH
and Aghi MK: Skull base chordomas: Clinical features, prognostic
factors, and therapeutics. Neurosurg Clin N Am. 24:79–88.
2013.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Chugh R, Tawbi H, Lucas DR, Biermann JS,
Schuetze SM and Baker LH: Chordoma: The non sarcoma primary bone
tumor. Oncologist. 12:1344–1350. 2007.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Fuchs B, Dickey ID, Yaszemski MJ, Inwards
CY and Sim FH: Operative management of sacral chordoma. J Bone
Joint Surg Am. 87:2211–2216. 2005.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Bongers MER, Dea N, Ames CP and Schwab JH:
Surgical strategies for chordoma. Neurosurg Clin N Am. 31:251–261.
2020.PubMed/NCBI View Article : Google Scholar
|
|
10
|
D'Amore T, Boyce B and Mesfin A: Chordoma
of the mobile spine and sacrum: Clinical management and prognosis.
J Spine Surg. 4:546–552. 2018.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Alan O, Akin Telli T, Ercelep O, Tanrikulu
Simsek E, Basoglu Tuylu T, Mutis A, Hasanov R, Kaya S, Akgül
Babacan N, Dane F and Yumuk PF: Chordoma: A case series and review
of the literature. J Med Case Rep. 12(239)2018.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Vellutini EAS, Brock RS, Martins HO,
Taricco MA and de Oliveira MF: Diffuse spinal spreading following
previous intracranial intradural chordoma resection: A rare case
report. J Clin Neurosci. 64:44–46. 2019.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Akmansu M, Kurt G, Demircan V and Senturk
E: Results of chordoma patients treated by different approaches in
a single institution. Turk Neurosurg. 30:366–370. 2020.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Ahmed R, Sheybani A, Menezes AH, Buatti JM
and Hitchon PW: Disease outcomes for skull base and spinal
chordomas: A single center experience. Clin Neurol Neurosurg.
130:67–73. 2015.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Pu F, Wang B, Liu J, Chen F and Shao Z:
Giant chordoma in the thoracolumbar spine: A case report and
literature review. Eur Spine J. 26 (Suppl 1):S95–S99.
2017.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Colangeli S, Muratori F, Bettini L, Frenos
F, Totti F, D'Arienzo A, Campo FR, Scoccianti G, Beltrami G,
Campanacci DA and Capanna R: Surgical treatment of sacral chordoma:
En bloc resection with negative margins is a determinant of the
long-term outcome. Surg Technol Int. 33:343–348. 2018.PubMed/NCBI
|
|
17
|
Niu XH: Interpretation of 2020 NCCN
clinical practice guidelines in oncology-bone cancer. Zhonghua Wai
Ke Za Zhi. 58:430–434. 2020.PubMed/NCBI View Article : Google Scholar : (In Chinese).
|
|
18
|
Ruggieri P, Angelini A, Ussia G, Montalti
M and Mercuri M: Surgical margins and local control in resection of
sacral chordomas. Clin Orthop Relat Res. 468:2939–2947.
2010.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Mohanty S, Pai Kanhangad M and Kundangar
R: The extended posterior approach for resection of sacral tumours.
Eur Spine J. 28:1461–1467. 2019.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Yang Y, Li Y, Liu W, Xu H and Niu X: The
clinical outcome of recurrent sacral chordoma with further surgical
treatment. Medicine (Baltimore). 97(e13730)2018.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Kabolizadeh P, Chen YL, Liebsch N,
Hornicek FJ, Schwab JH, Choy E, Rosenthal DI, Niemierko A and
DeLaney TF: Updated outcome and analysis of tumor response in
mobile spine and sacral chordoma treated with definitive high-dose
photon/proton radiation therapy. Int J Radiat Oncol Biol Phys.
97:254–262. 2017.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Imai R, Kamada T, Tsuji H, Sugawara S,
Serizawa I, Tsujii H and Tatezaki S: Working Group for Bone and
Soft Tissue Sarcomas. Effect of carbon ion radiotherapy for sacral
chordoma: Results of Phase I-II and Phase II clinical trials. Int J
Radiat Oncol Biol Phys. 77:1470–1476. 2010.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Park L, Delaney TF, Liebsch NJ, Hornicek
FJ, Goldberg S, Mankin H, Rosenberg AE, Rosenthal DI and Suit HD:
Sacral chordomas: Impact of high-dose proton/photon-beam radiation
therapy combined with or without surgery for primary versus
recurrent tumor. Int J Radiat Oncol Biol Phys. 65:1514–1521.
2006.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Chen YL, Liebsch N, Kobayashi W, Goldberg
S, Kirsch D, Calkins G, Childs S, Schwab J, Hornicek F and DeLaney
T: Definitive high-dose photon/proton radiotherapy for unresected
mobile spine and sacral chordomas. Spine (Phila Pa 1976).
38:E930–E936. 2013.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Bompas E, Le Cesne A, Tresch-Bruneel E,
Lebellec L, Laurence V, Collard O, Saada-Bouzid E, Isambert N, Blay
JY, Amela EY, et al: Sorafenib in patients with locally advanced
and metastatic chordomas: a phase II trial of the French Sarcoma
Group (GSF/GETO). Ann Oncol. 26:2168–2173. 2015.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Lebellec L, Bertucci F, Tresch-Bruneel E,
Bompas E, Toiron Y, Camoin L, Mir O, Laurence V, Clisant S,
Decoupigny E, et al: Circulating vascular endothelial growth factor
(VEGF) as predictive factor of progression-free survival in
patients with advanced chordoma receiving sorafenib: An analysis
from a phase II trial of the French sarcoma group (GSF/GETO).
Oncotarget. 7:73984–73994. 2016.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Stacchiotti S, Longhi A, Ferraresi V,
Grignani G, Comandone A, Stupp R, Bertuzzi A, Tamborini E, Pilotti
S, Messina A, et al: Phase II study of imatinib in advanced
chordoma. J Clin Oncol. 30:914–920. 2012.PubMed/NCBI View Article : Google Scholar
|
|
28
|
George S, Merriam P, Maki RG, Van den
Abbeele AD, Yap JT, Akhurst T, Harmon DC, Bhuchar G, O'Mara MM,
D'Adamo DR, et al: Multicenter phase II trial of sunitinib in the
treatment of nongastrointestinal stromal tumor sarcomas. J Clin
Oncol. 27:3154–3160. 2009.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Stacchiotti S, Marrari A, Tamborini E,
Palassini E, Virdis E, Messina A, Crippa F, Morosi C, Gronchi A,
Pilotti S and Casali PG: Response to imatinib plus sirolimus in
advanced chordoma. Ann Oncol. 20:1886–1894. 2009.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Meng T, Jin J, Jiang C, Huang R, Yin H,
Song D and Cheng L: Molecular targeted therapy in the treatment of
chordoma: A systematic review. Front Oncol. 9(30)2019.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Liu C, Jia Q, Wei H, Yang X, Liu T, Zhao
J, Ling Y, Wang C, Yu H, Li Z, et al: Apatinib in patients with
advanced chordoma: A single-arm, single-centre, phase 2 study.
Lancet Oncol. 21:1244–1252. 2020.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Stacchiotti S and Sommer J: Chordoma
Global Consensus Group. Building a global consensus approach to
chordoma: A position paper from the medical and patient community.
Lancet Oncol. 16:e71–e83. 2015.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Stacchiotti S, Gronchi A, Fossati P,
Akiyama T, Alapetite C, Baumann M, Blay JY, Bolle S, Boriani S,
Bruzzi P, et al: Best practices for the management of
local-regional recurrent chordoma: A position paper by the chordoma
global consensus group. Ann Oncol. 28:1230–1242. 2017.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Colia V and Stacchiotti S: Medical
treatment of advanced chordomas. Eur J Cancer. 83:220–228.
2017.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Ji T, Guo W, Yang R, Tang X, Wang Y and
Huang L: What are the conditional survival and functional outcomes
after surgical treatment of 115 patients with sacral chordoma? Clin
Orthop Relat Res. 475:620–630. 2017.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Yang Y, Niu X, Li Y, Liu W and Xu H:
Recurrence and survival factors analysis of 171 cases of sacral
chordoma in a single institute. Eur Spine J. 26:1910–1916.
2017.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Zhou J, Sun J, Bai HX, Huang X, Zou Y, Tan
X, Zhang Z, Tang X, Tao Y, Xiao B, et al: Prognostic factors in
patients with spinal chordoma: An integrative analysis of 682
patients. Neurosurgery. 81:812–823. 2017.PubMed/NCBI View Article : Google Scholar
|