Introduction
Sarcoidosis is a multisystemic granulomatous disease
characterized by a chronic inflammatory process of an unidentified
etiology. The most frequently affected organ is the lung, which
accounts for 90% of all cases of sarcoidosis, followed by eyes,
heart and lymphatic system (1).
Splenic sarcoidosis is rare and has been reported sporadically
(2-12).
Therefore, how to treat, diagnose, and manage isolated splenic
sarcoidosis is not established.
Malignant lymphomas, lymphangiomas, or hemangiomas
are the most frequently encountered splenic tumors. There are no
specific radiological findings for sarcoidosis. So, differentiation
between these tumors using radiological images alone is difficult;
histological examination is usually required.
This report presents a case of isolated splenic
sarcoidosis that was diagnosed histologically following
laparoscopic splenectomy, because it was difficult to diagnose
sarcoidosis using radiological images and laboratory tests. We also
attempted to determine whether there are distinctive
characteristics that could be associated with the diagnosis of
splenic sarcoidosis.
Case report
A 76-year-old woman with a past medical history of
left radical nephroureterectomy for left renal pelvic cancer 7
years previously and breast mastectomy for left breast cancer 6
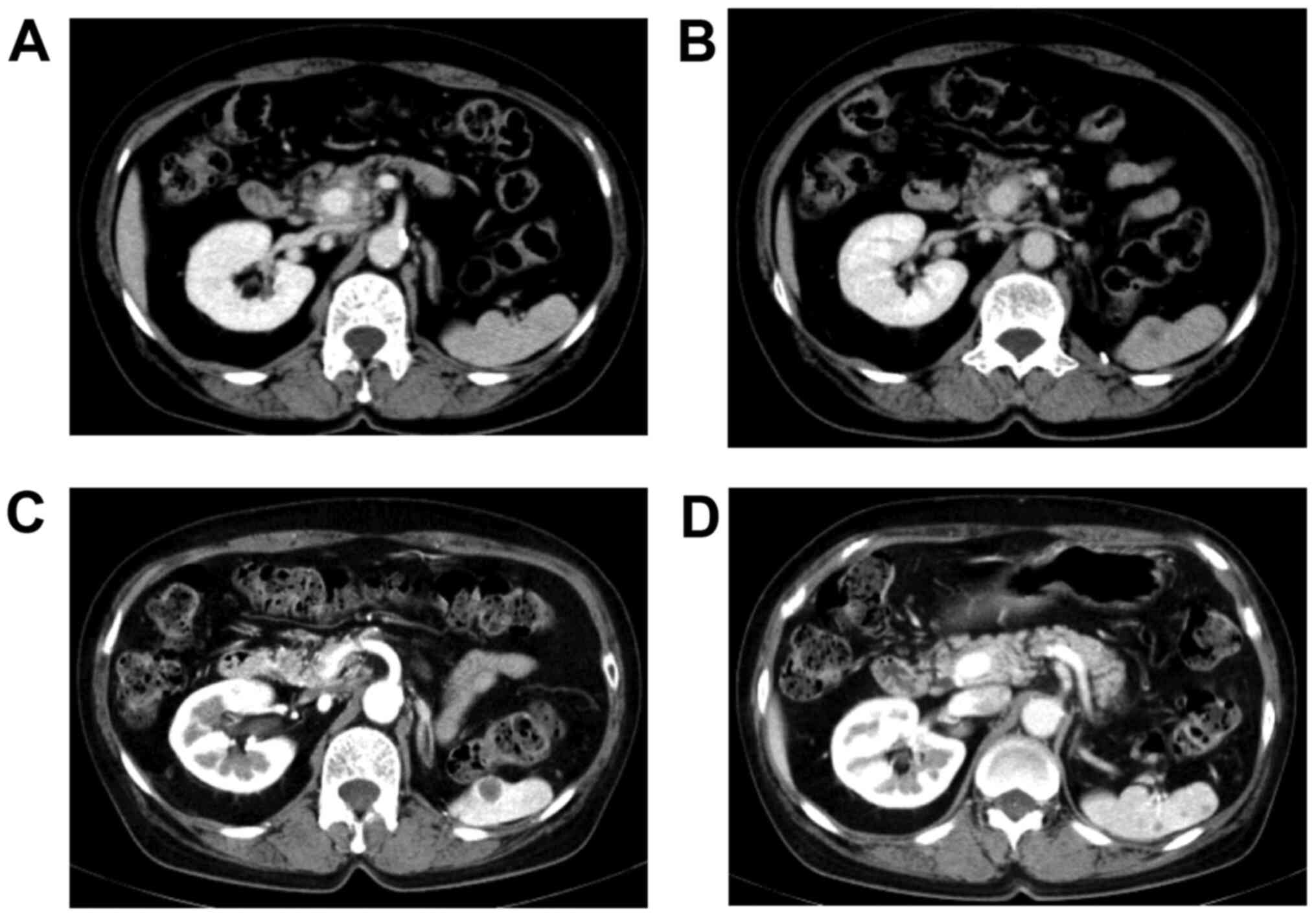
years previously had been undergoing follow-up. Contrast-enhanced
computed tomography (CT) revealed multiple poorly enhanced splenic
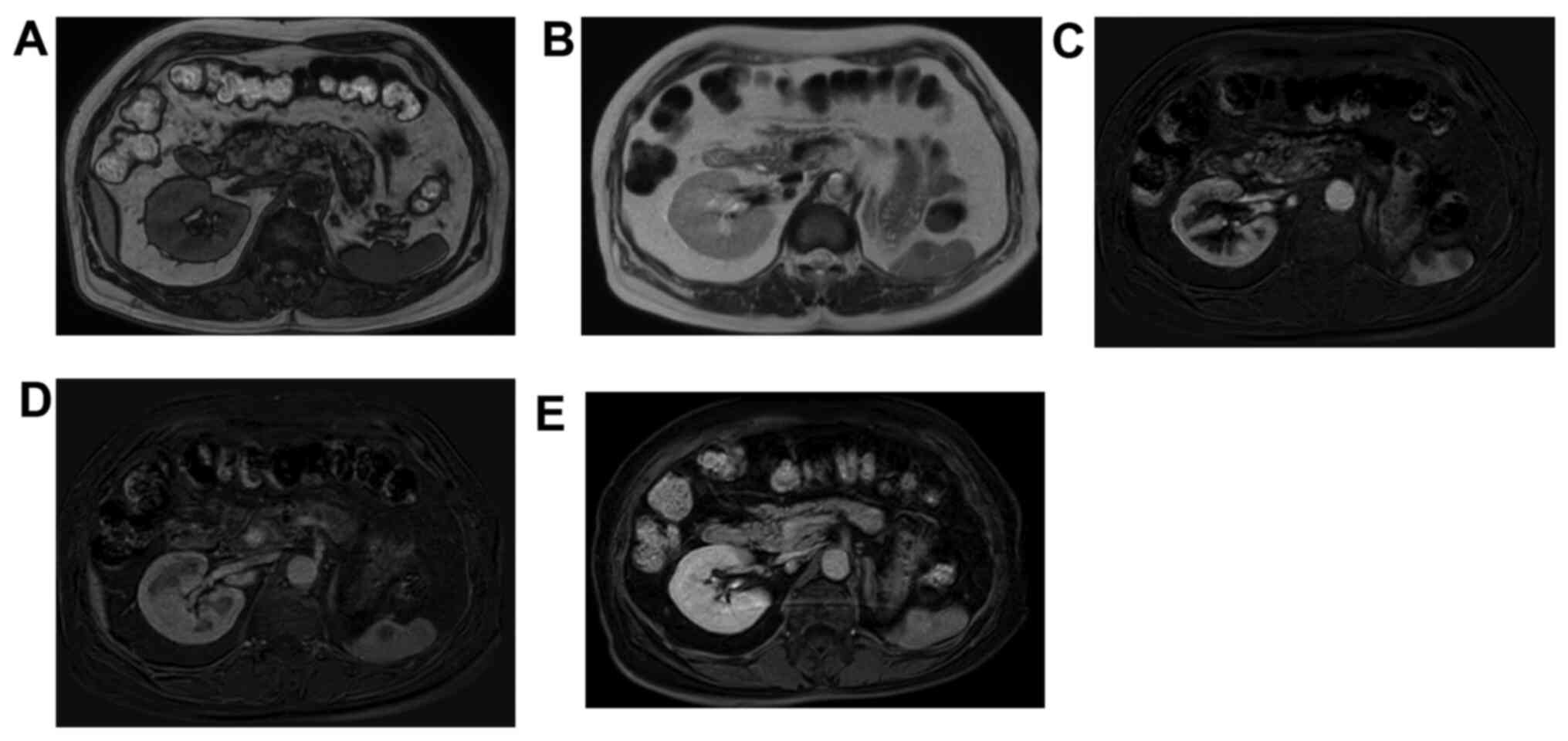
tumors, with the largest one measuring 1.2 cm in diameter (Fig. 1). Using magnetic resonance imaging
(MRI), the lesions showed equivalent intensity with the spleen on
T1 weighted images and low intensity on T2-weighted images
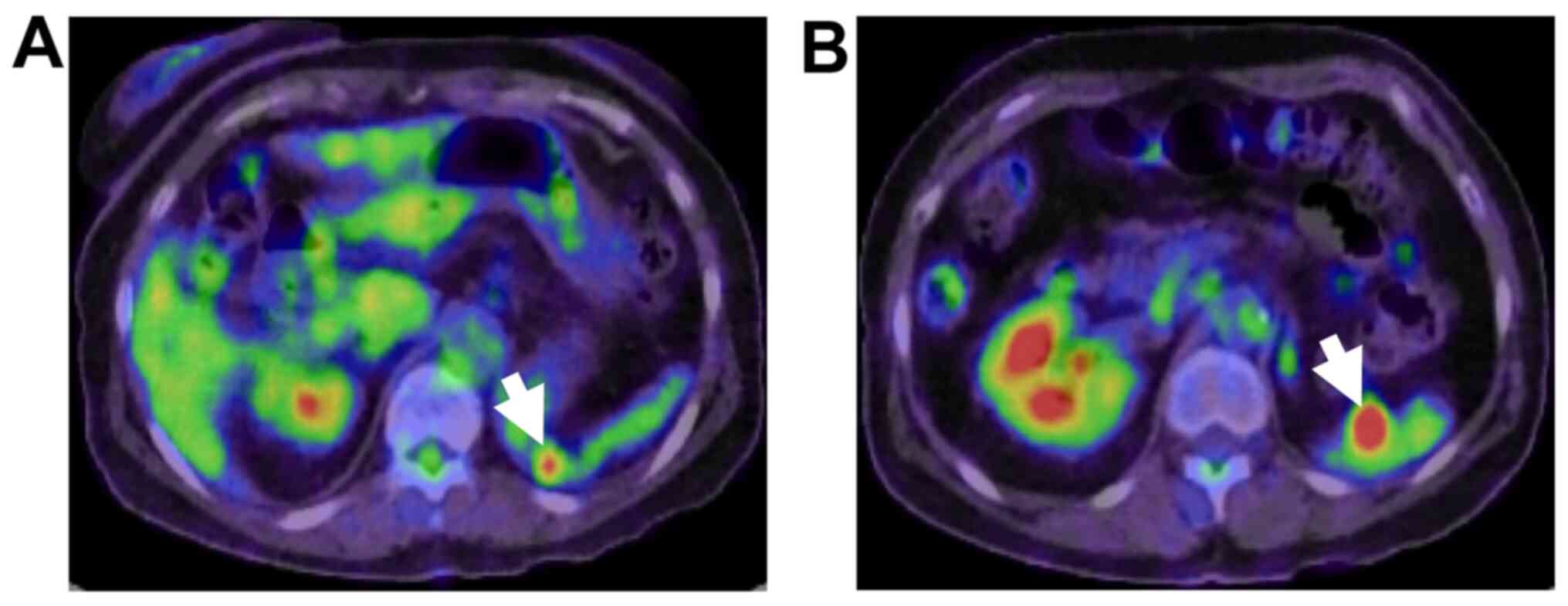
(Fig. 2). The lesions had increased
in size over the previous 2 years. Positron emission tomography
(PET)-CT revealed [18F]-fluorodeoxyglucose (FDG) accumulation at
the upper and lower poles of the spleen (Fig. 3).
Because laboratory data showed slightly elevated
lactate dehydrogenase (LDH; 275U/l) and soluble interleukin-2
receptor (sIL-2R; 588 U/ml), we suspected that the lesions were
malignant lymphoma. To confirm the diagnosis, we performed
laparoscopic splenectomy. The operative time was 264 minutes, and
the amount of bleeding was 291 ml. The patient recovered
uneventfully and was discharged on the 8th postoperative day.
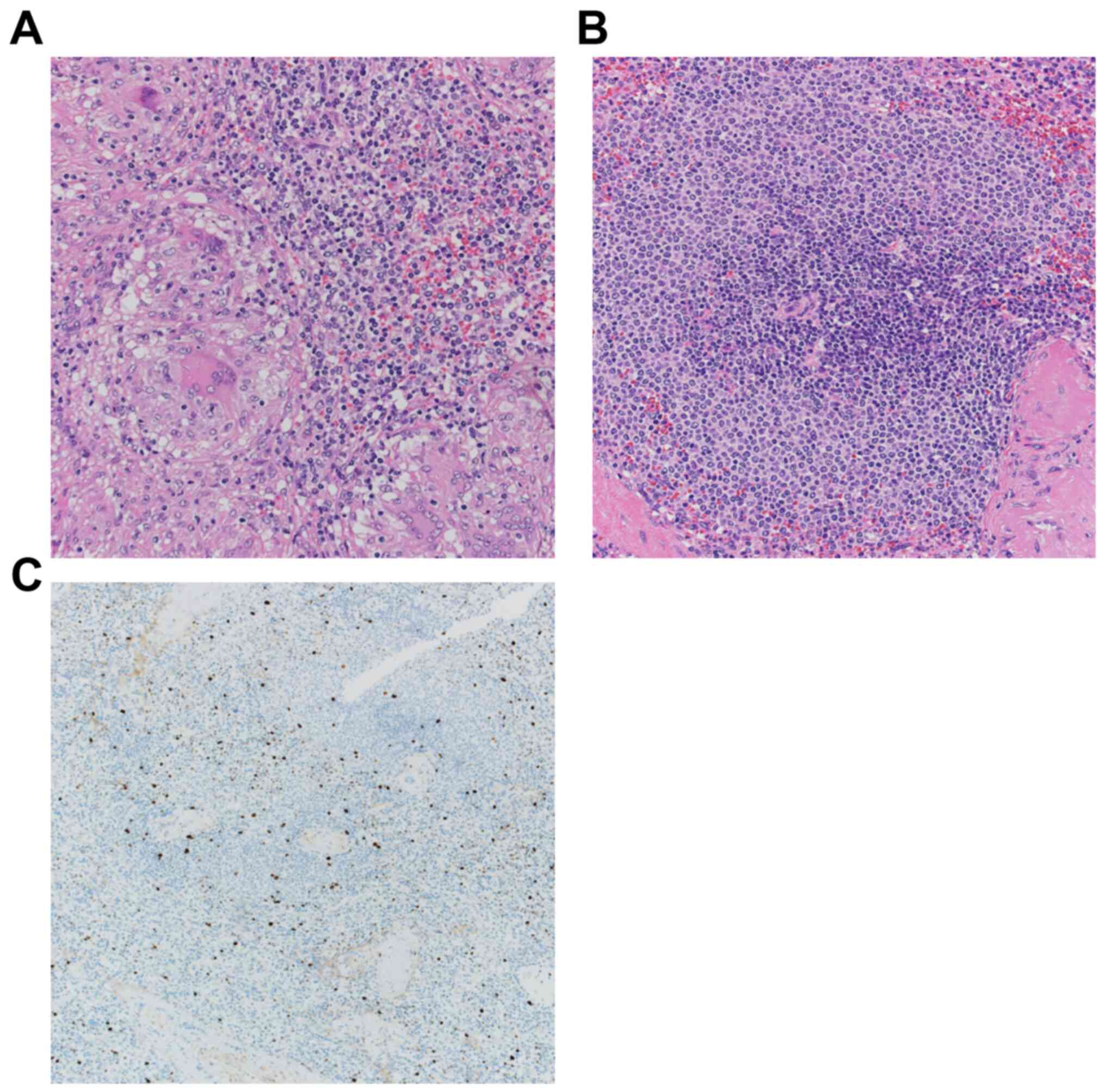
Histological examination of the splenic specimen revealed small and
dense epithelioid non-caseating granulomas (Fig. 4A). There was a marginal zone around
the lymphoid follicles (Fig. 4B),
but the targetoid pattern was negative for Ki-67 staining (Fig. 4C). Therefore, the diagnosis of
marginal zone lymphoma was not supported. Furthermore,
microorganisms were not identified via Gram staining or
Ziehl-Neelsen staining. Flow cytometry also did not confirm the
diagnosis of malignant lymphoma. Postoperative laboratory test
results demonstrated no remarkable change in LDH (235 U/l) or
sIL-2R (565 U/ml). Based on these tests, isolated sarcoidosis of
the spleen was confirmed, although sarcoidosis was not detected in
the patient's eyes, lungs, or heart. The patient remained alive
after the 7th month follow-up without signs of
exacerbation of the sarcoidosis or recurrence of renal or breast
cancer.
Discussion
We experienced a case of isolated splenic
sarcoidosis. Regarding the affected organs of sarcoidosis, the
spleen reportedly accounted for only 6.7% of occurrences and in
most cases, other organs were involved (1). Isolated splenic sarcoidosis is rare
and is reported sporadically (13).
So diagnosis, treatment, and management of isolated splenic
sarcoidosis was not established.
Sarcoidosis is an inflammatory disease characterized
by the presence of non-caseating granulomas. Its diagnosis is based
on clinical and radiological findings, in addition to
histologically confirmed epithelioid granulomas. Laboratory tests
are not usually helpful. Because there are no specific radiological
findings for splenic sarcoidosis, histopathological examination is
mandatory for its definitive diagnosis.
If there is a lesion of the spleen, methods for
obtaining tissues for histopathology include biopsy and
splenectomy. Because biopsy has the risk of bleeding and
dissemination, especially where the tumor is malignant, splenectomy
is commonly considered.
Granulomas are not a specific finding of
sarcoidosis. The differential diagnoses of splenic granulomatous
lesions include infection, foreign material exposure with talc or
beryllium, benign vascular tumor, metastatic tumor, lymphoma, and
Langerhans cell histiocytosis (14). According to an international
consensus statement (15), even if
the histopathological findings are indicative of sarcoidosis, a
local sarcoid reaction, which develops in different neoplastic and
non-neoplastic diseases, at the site of the main lesion and/or in
regional lymph nodes, must be excluded. The present case fulfilled
the criteria of Statement on sarcoidosis; therefore, the diagnosis
of isolated splenic sarcoidosis was confirmed.
To the best of our knowledge, there are only 11
cases of isolated splenic sarcoidosis in the literature (2-12).
Table I shows these 11 cases and
the present case. It was suggested that splenic sarcoidosis was
more common in women, and that sweating, and weight loss were
frequently identified as subjective symptoms (5 among 11 cases;
45%).
 | Table ISummary of 13 reported cases of
isolated splenic sarcoidosis. |
Table I
Summary of 13 reported cases of
isolated splenic sarcoidosis.
| No. | Author, year | Age/sex | History | Symptoms | Number of
lesions | CT | PET | Treatment | (Refs.) |
|---|
| 1 | Giovinale et
al, 2009 | 32/F | - | Epigastric pain | Multiple | Low-density
nodule | - | Operation (LS) | (2) |
| 2 | Giovinale et
al, 2009 | 53/F | - | Abdominal pain | Single | Low-density
nodule | - | Operation (LS) | (2) |
| 3 | Joglekar et
al, 2009 | 46/F | Sciatica | Back and leg
pain | Multiple | Mild splenomegaly
with multiple low-density nodules | - | Operation (OS) | (3) |
| 4 | Cuilliere-Dartigues
et al, 2010 | 18/M | None | Night sweat | Multiple | Mild splenomegaly
with low-density nodule | Intense uptake | Operation (LS) | (4) |
| 5 | Ogiwara et al,
2010 | 74/F | - | Night sweats,
palpitation | Single | High-density
nodule | No remarkable
change | Operation (OS) | (5) |
| 6 | Palade et al,
2012 | 66/F | - | Anemia | - | Multiple low-density
nodules | - | Operation (LS) | (6) |
| 7 | Bauones et al,
2014 | 37/F | - | Chronic abdominal
discomfort | Multiple | - | - | Operation
(Unknown) | (7) |
| 8 | Souto et al,
2014 | 29/F | None | - | Multiple | Multiple high-density
nodules | No remarkable
change | Operation (LS) | (8) |
| 9 | Dennis et al,
2014 | 65/M | - | Headache, weight
loss | - | Mild
splenomegaly | Intense uptake | Operation (HALS) | (9) |
| 10 | Sreelesh et
al, 2017 | 50/F | Uterine fibroids | Weight loss | Multiple | - | - | Operation (OS) | (10) |
| 11 | Bachmeyer et
al, 2017 | 56/F | Beta thalassemia | Weight loss | Multiple | Splenomegaly | Intense uptake | Steroid (3
months) | (11) |
| 12 | Gaudemer et
al, 2018 | 42/F | - | Epigastric pain | Multiple | No remarkable
change | No remarkable
change | - | (12) |
| 13 | Present study | 76/F | Renal pelvic cancer,
breast cancer | None | Multiple | Multiple low-density
nodules | Intense uptake | Operation (LS) | - |
The lesions are often numerous (9 among 11 cases;
81.8%) and, CT showed low-density multiple nodules (5 among 10
cases; 50%), and splenomegaly (4 among 10 cases; 40%). PET-CT
showed abnormal accumulation of [18F]-FDG (4 among 6 cases; 66.7%).
In 10 cases, splenectomy was performed for the diagnosis. In one
case, treatment with steroids were administered after confirmation
of diagnosis.
In our case, for which the patient's past history
was provided, included malignant tumor. The pathogenesis of sarcoid
granulomas includes a complex interplay of immune cells, including
macrophages dendritic cells, T helper lymphocytes, T regulatory
cells, and their mediators. Although several studies have suggested
that T-cell receptor V beta, one of the subtypes of the T-cell
antigen receptor, is associated with the conventional antigenic
stimulation, the mechanism through which this stimulation causes
sarcoidosis remains unclear (16).
Malignant tumors might affect the body's immune system and be
responsible for the development of sarcoidosis in the spleen, which
is a hematopoietic lymphoid organ. There are no reports clarifying
them, so further case accumulation might be necessary.
In conclusion, we experienced a rare case of
isolated sarcoidosis of the spleen. Sarcoidosis should be included
in the differential diagnosis when multiple splenic tumors are
detected and sarcoidosis might be associated with malignant
tumors.
Acknowledgements
The authors would like to thank Dr Hiroaki Aoki,
Associate General Manager of the Surgical Department at Jikei
University, for his kindness and for the fruitful discussion we had
at the 852nd Annual Meeting of the Tokyo Surgical Society.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study available from the corresponding author on reasonable
request.
Authors' contributions
KK and TE were involved in drafting the manuscript,
revising it critically for important intellectual content, and made
substantial contributions to acquisition of data. IF, TT and JA
analyzed and interpreted the patient data, and contributed to
manuscript preparation. SS and HS made substantial contributions to
analysis and interpretation of data. YM and TI made substantial
contributions to conception and design. YK, HT, KH and HU made
substantial contributions to conception and design, and gave final
approval of the version to be published. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
This case report was approved by the Institutional
Review Board of the National Defense Medical College (approval no.
4115).
Patient consent for publication
Written informed consent for publication of their
clinical details and/or clinical images was obtained from the
patient.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Baughman RP, Teirstein AS, Judson MA,
Rossman MD, Yeager H Jr, Bresnitz EA, DePalo L, Hunninghake G,
Iannuzzi MC, Johns CJ, et al: Clinical characteristics of patients
in case control study of sarcoidosis. Am J Respir Crit Care Med.
164:1885–1889. 2001.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Giovinale M, Fonnesu C, Soriano A,
Cerquaglia C, Curigliano V, Verrecchia E, De Socio G, Gasbarrini G
and Manna R: Atypical sarcoidosis: Case reports and review of the
literature. Eur Rev Med Pharmacol Sci. 13:37–44. 2009.PubMed/NCBI
|
|
3
|
Joglekar SP, Hudson RL, Lgasundaram R and
Pereira JH: ‘Surgical cure’ for non parathyroid hypercalcemia.
World J Surg Oncol. 7(23)2009.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Cuilliere-Dartigues P, Meyohas MC,
Balladur P, Gorin NC and Coppo P: Splenic sarcoidosis: An unusual
aetiology of agranulocytosis. Am J Hematol. 85(891)2010.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Ogiwara Y, Mori S, Iwama M, Sawabe M,
Kanazawa N, Takemoto M, Kanazawa N, Fukuda I, Kondo Y, Kimbara Y,
et al: Hypoglycemia due to ectopic secretion of insulin-like growth
factor-I in a patient with an isolated sarcoidosis of the spleen.
Endocr J. 57:325–330. 2010.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Palade R, Voiculescu D, Suliman E and
Simion G: Splenic sarcoidosis-a case report. Chirurgia (Bucur).
107:670–674. 2012.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Bauones S, Le Corroller T, Durieux O,
Guenoun D, Del Grande J, Pirro N and Champsaur P: Splenic
sarcoidosis mimicking neoplastic disease. J Clin Ultrasound.
42:38–41. 2014.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Souto MM, Tempes BC, Lambert BF, Trindade
EN and Trindade MR: Laparoscopic splenectomy for isolated splenic
sarcoidosis. JSLS. 18:155–159. 2014.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Dennis BA, Jajosky RP and Harper RJ:
Splenic sarcoidosis without focal nodularity: A case of
1,25-dihydroxyvitamin D-mediated hypercalcemia localized with FDG
PET/CT. Endocr Pract. 20:e28–e33. 2014.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Sreelesh KP, Kumar ML and Anoop TM:
Primary splenic sarcoidosis. Proc (Bayl Univ Med Cent). 27:344–345.
2014.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Bachmeyer C, Fayand A, Georgin-Lavialle S,
Fedida B, Naccache JM, Lionnet F and Amiot X: Massive splenomegaly
indicating sarcoidosis. Am J Med. 130:e141–e142. 2017.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Gaudemer A, Sauvet G, Hij A, Stanciu R,
Farge-Bancel D and Algayres JP: Splenic sarcoidosis diagnosed by
US-guided biopsy: About a case. Rev Med Interne. 39:200–202.
2018.PubMed/NCBI View Article : Google Scholar : (In French).
|
|
13
|
Warshauer DM and Lee JK: Imaging
manifestations of abdominal sarcoidosis. AJR Am J Roentgenol.
182:15–28. 2004.PubMed/NCBI View Article : Google Scholar
|
|
14
|
O'Maley DP, George TI, Orazi A and
Abbondanzo SL: Atlas of Nontumor Pathology Benign and Reactive
Conditions of Lymph Node and Spleen. America Amer Registry of
Pathology, 2009.
|
|
15
|
Statement on sarcoidosis. Joint statement
of the American thoracic society (ATS), the European respiratory
society (ERS) and the world association of sarcoidosis and other
granulomatous disorders (WASOG) adopted by the ATS Board of
Directors and by the ERS Executive Committee, February 1999. Am J
Respir Crit Care Med. 160:736–755. 1999.
|
|
16
|
Andrew F and Talmadge E: Pathology and
pathogenesis of sarcoidosis. urihttps://www.uptodate.com/contents/pathology-and-pathogenesis-of-sarcoidosis?search=Pathology%20and%20pathogenesis%20of%20sarcoidosis&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1simplehttps://www.uptodate.com/contents/pathology-and-pathogenesis-of-sarcoidosis?search=Pathology%20and%20pathogenesis%20of%20sarcoidosis&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1.
Accessed 09 Apr 2018.
|