Introduction
The cervical esophagus is the short part of the
esophagus between the lower border of the cricoid cartilage and the
thoracic inlet, 18 cm from the incisor teeth (1). Cervical esophageal carcinoma (CESCC)
is less common than thoracic esophageal carcinoma (ESCC),
accounting for less than 5% of all esophageal carcinoma (2). The management of CESCC differs from
cancers of the other parts of the esophagus in that CESCCs are
often locally advanced at the time of diagnosis infiltrating nearby
anatomical structures including the thyroid, carotid artery, and
trachea. Moreover, patients with CESCC often present with lymph
node metastases1. Some of CESCC are not treatable by
surgery even when diagnosed at an early stage, as this would
involve mutilating resections including
pharyngo-laryngo-esophagectomy. Therefore, definitive
chemoradiation (dCRT) is the standard treatment modality for CESCC
recommended by the National Comprehensive Cancer Network and
European Society for Medical Oncology (ESMO) guidelines (3,4).
Several diagnostic and predictive markers have been studied, but no
biomarker to clearly determine patient treatment. Recently, many
new biomarkers related to carcinogenesis, prognosis or response to
therapies for several carcinomas are known. In addition, HPV
infection is known to be a major etiologic factor in oropharyngeal
squamous cell carcinomas, as a strong and independent prognostic
marker (5-7).
Indeed, patients with HPV-positive oropharyngeal carcinomas have a
significantly decreased mortality risk compared with HPV-negative
oropharyngeal carcinoma patients (7). While some articles have described the
HPV status of esophageal carcinoma patients, HPV status as a
prognostic or predictive biomarker of ESCC is not yet established.
We therefore explored HPV infection status in patients with CESCC.
CESCC is suspected to demonstrate more similar characteristics with
oropharyngeal carcinomas than ESCCs at other sites. Genomic
analyses of EGFR, KRAS, NRAS, and
PIK3CA, also seem to be potent biomarkers for targeted
therapy, such as anti-EGFR therapy or PIK3CA
inhibitor therapy. The present study aimed at determining how many
CESCC patients are HPV-infected and/or EGFR- and SCC-related
gene mutations by analyzing each patient's tumor sample.
Patients and methods
Patients
This retrospective study enrolled 33 CESCC patients
who received CRT or surgery at National Cancer Center Hospital from
March 2001 to September 2006. The clinical criteria for enrollment
were as follows: Archive tissue available, no other malignancies,
written informed consent given and a primary lesion existing in the
cervical esophagus. The cervical esophagus is defined as the upper
side without extension to the inferior margin of the hyoid bone or
the lower side of the primary without extension to the superior
margin of the carina. The institutional review board of the NCCH
(no. 2008-119) approved this study and it was performed in
accordance with the Declaration of Helsinki.
Treatment: dCRT regimens and surgical
procedures for CESCC patients
The dCRT regimen for CESCC patients comprised of 70
mg/m2 of cisplatin (CDDP) administered intravenously for
120 min on days 1 and 29, 700 mg/m2 of 5-FU administered
continuously on days 1-4 and 29 to 32, and radiation therapy at a
dose of 60 Gy irradiated concurrently. If the therapeutic effect
was observed, 2 repeated cycles of 80 mg/m2 of CDDP and
800 mg/m2 of 5-FU were administered on day 1 and days 1
to 5, respectively, every 4 weeks. Concerning radical surgical
resection, cervical esophagus resection preserving the larynx or
pharyngo-laryngo-esophagectomy was performed. The patients who
underwent curative resection did not receive preoperative
irradiation.
Tumor sample collection and tissue
processing procedure Polymerase chain reaction
We briefly stained deparaffinized sections with
hematoxylin and used them for DNA extraction. The carcinoma
components were separately dissected using sterilized toothpicks
under a microscope. The proper muscle tissue distant from the tumor
was used as a non-tumor sample. The dissected samples were
incubated in 100 µl of DNA extraction buffer [50 mmol/l Tris-HCl,
pH 8.0, 1 mmol/l ethylenediaminetetraacetic acid, 0.5% (v/v)
Tween-20, 200 µg/ml proteinase K] at 55˚C overnight. We then heated
the samples at 100˚C for 10 min to inactivate proteinase K and
directly subjected them to polymerase chain reaction (PCR). DNA
samples were obtained from cervical carcinomas with known human
papillomavirus 16 (HPV16) infection and the HeLa cell line positive
for HPV18 were used as positive controls. PCR was performed using
HPV consensus primers GP5+/6+ (8) and two pairs of genotype-specific
primers for HPV16 and HPV18, as previously described (9,10).
Primer sequences of the elongated 23-mer GP5 (named
GP5+) and 25-mer GP6 (named GP6+) are
indicated (10). ACTB was amplified
to ensure proper DNA extraction. The PCR products were
electrophoresed in a 2% (w/v) agarose gel and visualized under
ultraviolet light with ethidium bromide staining.
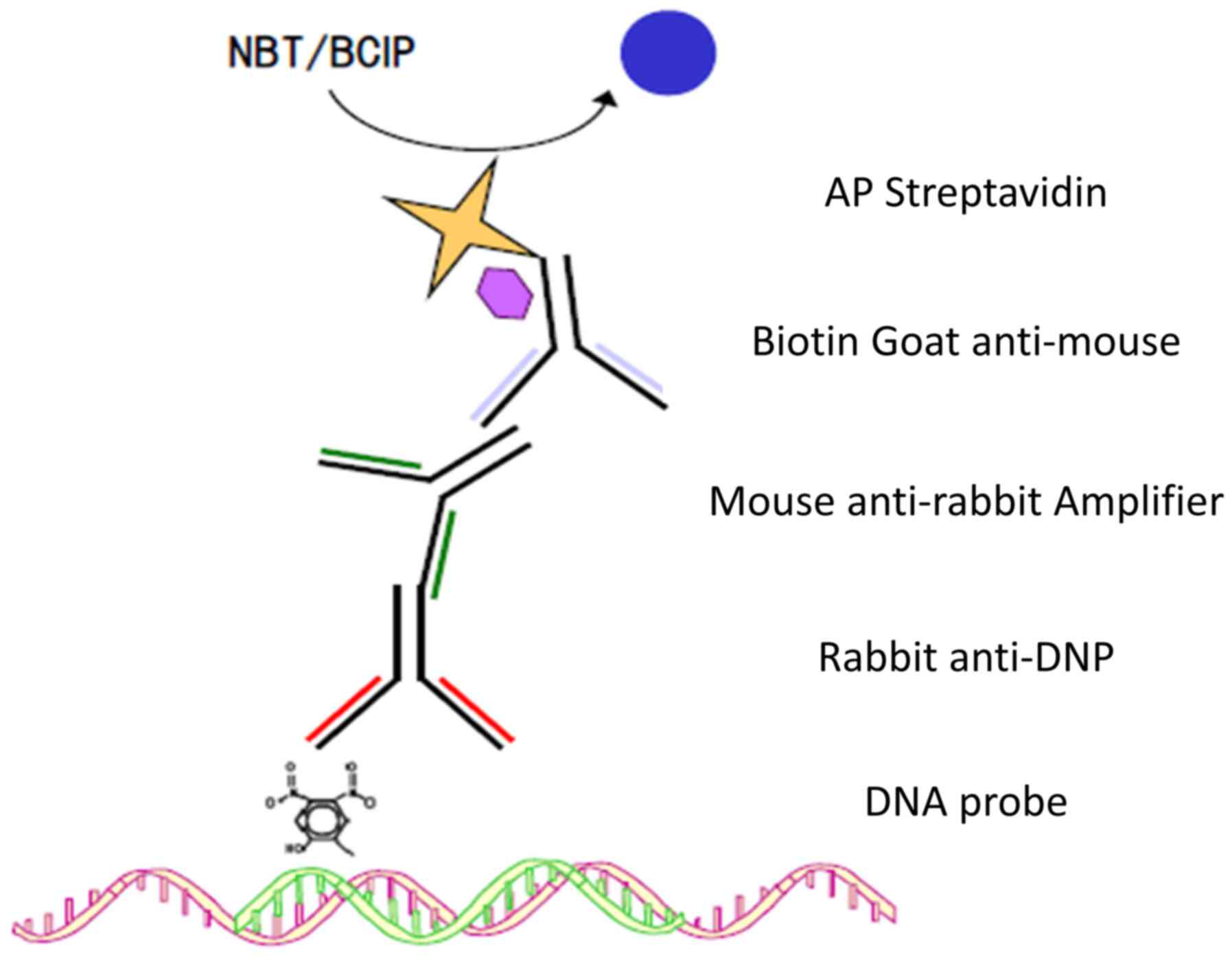
In situ hybridization
DNA ISH was performed on formalin-fixed,
paraffin-embedded (FFPE) tissue blocks from each case using the ISH
I View Blue Plus Detection Kit (Ventana Medical System, Inc.) in
accordance with the manufacturer's instructions. The assay used the
Ventana HPV III Family 16, Probe B, a cocktail recognizing the HPV
types 16, 18, 31, 33, 35, 45, 51, 52, 56, 59, 68 and 70. Ventana
Red Counterstain II (Ventana Medical System, Inc.) was used
(Fig. 1).
Controls in each run included a known HPV
16-positive HeLa cell line. A pathologist read the cases, and blue
nuclear dots were considered positive staining. Any definitive
nuclear staining in the tumor cells was considered positive. Cases
were classified in a binary manner as either positive or
negative.
Mutation analyses of EGFR, KRAS, BRAF,
PIK3CA and NRAS
We collected FFPE tissue, and the DNA of samples
were extracted from FFPE tumor tissue sections. The tumor cell-rich
areas in the hematoxylin and eosin section were marked under a
microscope, and the tissue was scratched from the area of another
deparaffinized unstained section. The EGFR mutation statuses were
evaluated by the PCR-invader method (BML, Inc.) analysis. DNA from
pieces of the scratched tissue sample was isolated using the QIAamp
DNA FFPE Tissue Kit (Qiagen KK). Exon 2 (codon 12, 13), exon 3
(codon 61) and exon 4 (codon 146) of the KRAS gene; exon 15
(codon 600) of the BRAF gene; exon 9 (codon 542, 545) and
exon 20 (exon) of the PIK3CA gene and; exon 2 (codon 12, 13)
and exon 3 (codon 61) of the NRAS gene were amplified by PCR
(GeneAmp PCR System 9700 Thermal Cycler). We visualized the PCR
products using agarose gel electrophoresis with ethidium bromide
staining and directly sequenced using an ABI 3130x Genetic Analyzer
[Life Technologies Japan (Applied Biosystems), Tokyo, Japan] in
accordance with the manufacturer's instructions.
Statistical analysis
All enrolled patients were divided into two groups:
i) Patients who have some mutations and ii) did not have any
mutation. The median OS was statistically compared between the two
groups using the log-rank test. The statistical analyses were
performed with SAS 9.4 (SAS Institute Inc.).
Results
Patient characteristics
We enrolled 33 CESCC patients in this study
according to the present criteria. The background characteristics
of the CESCC patients are shown in Table I. Most patients (88%) were males,
with only 4 were females (12%). 25 patients (75%) were diagnosed
with clinical Stage III or IV (lymph node) (UICC-TNM 6th) (11), while 8 patients (25%) were clinical
Stage I or II. Surgery was performed in 13 patients (35%), and dCRT
in 20 patients (65%).
 | Table IBaseline patient characteristics
(n=33). |
Table I
Baseline patient characteristics
(n=33).
|
Characteristics | N (%) |
|---|
| Sex | |
|
Male | 29(88) |
|
Female | 4(12) |
| Tumor stage | |
|
1 | 5(16) |
|
2 | 3(9) |
|
3 | 19(57) |
|
4 | 6(18) |
| Nodal stage | |
|
0 | 21(63) |
|
1 | 12(37) |
| CStage | |
|
I | 2(6) |
|
II | 6(18) |
|
III | 10(31) |
|
IV (lymph
node) | 15(45) |
| Treatment | |
|
Surgery | 13(35) |
|
Chemoradiation | 20(65) |
HPV analyses
Only one patient was HPV 16-positive (3.0%) on ISH
and PCR. This patient was a 41-year-old male with a light alcoholic
and non-smoking history who had been diagnosed as clinical T1N0M1
Stage IV. He received CRT and achieved a complete response. He
later underwent salvage resection of the esophagus for local
recurrence and is presently alive.
Mutations of EGFR, KRAS, BRAF, PIK3CA
and NRAS
Direct sequencing of the tissue samples in CESCC
patients determined the proportion of mutations of EGFR,
KRAS, BRAF, PIK3CA, and NRAS (Table II). EGFR mutations were
observed in T790 (9.0%, n=3/33), G719S and L858R (3.0%, n=1/33),
KRAS mutations in codon 13 (3.0%, n=1/33), BRAF
mutations in V600E (3.5%, n=1/28), PIK3CA mutations in exon
9 (3.0%, n=1/33), and NRAS mutations in codons 12 (3.3%,
n=1/30) and 13 (3.3%, n=1/30). No mutations were observed in
KRAS codon 61, KRAS codon 146 or other NRAS
codons. No patient among the CESCC patients with gene mutations in
their tumor tissue had multiple mutations. The tumor cell in the
HPV 16-positive patient did not show any gene mutation.
| Table IIProportion of mutations in the
EGFR-related genes in the tissue samples of the patients with
cervical esophageal squamous cell carcinoma. |
Table II
Proportion of mutations in the
EGFR-related genes in the tissue samples of the patients with
cervical esophageal squamous cell carcinoma.
| Gene mutations | Proportion (%) |
|---|
| EGFR mutations | 5/33 (15.1) |
| KRAS mutations
Codon 13 | 1/33 (3.0) |
| BRAF mutations
V600E | 1/28 (3.5) |
| PIK3CA mutations
exon 9 | 1/33 (3.0) |
| NRAS mutations
Codon 12 | 1/30 (3.3) |
| NRAS mutations
Codon 13 | 1/30 (3.3) |
Given these findings, no significant relationship
was noted between HPV infection and EGFR, KRAS,
BRAF, PIK3CA and NRAS gene mutations with
clinical prognostic factors in CESCC patients.
Discussion
CESCC is a less common disease and often locally
advanced at the time of diagnosis resulting in limited locoregional
disease control and poor survival. Due to the presence of locally
advanced disease at the time of diagnosis and the carcinoma being
close to larynx, spinal cord, and upper airway, sometimes
non-surgical treatment seems to be the appropriate option. Several
different CRT schedules and techniques have been investigated in
the past, but no consensus has been reached concerning the optimal
treatment for CESCC patients. Many institutions used CDDP/5-FU
regimen and a concurrent radiation dose of 60 Gy, which was the
community standard treatment. There is no indication to choose the
treatment and its response or prognosis in patients with CESCC.
Researches investigating the potential association
between HPV infection and ESCC show contradicting results. In the
present study, the HPV infection rate in CESCC patients was only
3.0%. Geographical locations with a high incidence of ESCC tend to
have a higher incidence of HPV infection; it is more frequent in
Asia (26.3%) and less frequent in other Western countries (14.0%)
(12). A few reports have shown
that the rate of HPV infection in ESCC patients range from 9.4 to
24.1% in Japan (12). HPV-related
esophageal cancer may correlate with lifestyle, culture, economic
conditions, and may be an epidemiological theme in the future. The
HPV-positive CESCC patients who underwent CRT achieved cure and had
a good long-term survival. HPV-infected CESCC can be a predictive
biomarker in sampling and analyzing the survival and efficacy of
HPV-positive CESCC cases who underwent CRT.
Though some studies on genetic mutations in ESCC
were done, to the best of our knowledge, there are no studies
investigating only genetic mutations in patients with CESCC only.
The most common genetic mutations consist of p53, RB1
(retinoblastoma protein), ALDH1 (Aldehyde dehydrogenase-2
gene), MTHFR (methylene tetrahydrofolate reductase
gene), EGR1 (early growth response gene-1), CCND1
(cycline D1) and cMYC (13-17).
MAPK signaling pathways are one of the upregulated genes in
ESCC (18). However, the clinical
roles of these gene mutations in the prognosis and clinical
response of the CRT in patients with CESCC is unclear. In the
present study, we analyzed the mutational status of EGFR and
its pathway-related gene mutations, KRAS, BRAF,
NRAS and PIK3CA which are unknown as biomarkers in
predicting the prognosis of patients with CESCC. However, we
observed KRAS, BRAF and PIK3CA gene mutations
in one patient each. Two CESCC patients had NRAS mutations.
We found a small number and no significant relationship was
observed between any gene mutation and the clinical prognostic
factors in CESCC patients. We compared our results with those from
comprehensive gene analysis of 71 ESCC patients (Table III) (19). The frequency of KRAS,
NRAS and BRAF mutations was rare. However,
EGFR mutation was 15.1 vs. 8%, PIK3CA mutation was 3
vs. 24% in CESCC and ESCC, respectively. In addition, in the
reports that examined only the KRAS and BRAF
mutations in ESCC, KRAS mutation was 0.5% (1/203) and
BRAF was 0% (0/203), respectively (20). Similarly, in a report examining only
EGFR gene mutations, L858R missense was found in a minority,
6.3% (8/127) (21). Comparing the
results of the reports with our result, we found that our results
were similar to those of ESCC.
| Table IIIComparison between CESCC and ESCC
gene mutations. |
Table III
Comparison between CESCC and ESCC
gene mutations.
| Gene | CESCC cases (n=33),
% | ESCC cases (n=71),
% |
|---|
| EGFR | 15.1 | 8.0 |
| PIK3CA | 3.0 | 24.0 |
| KRAS | 3.0 | 6.0 |
| NRAS | 6.6 | 3.0 |
| BRAF | 3.5 | N.E. |
In patients with non-small cell lung cancer,
EGFR mutation is an important predictive factor for using
EGFR-TKI. The COG trial, a phase Ⅲ trial conducted in patients with
esophageal cancer, could not show the superiority of Gefitinib in
overall survival (22). However,
the results of biomarker analysis showed that EGFR copy gain was a
predictor of efficacy (23).
Considering the remarkable progress of EGFR-TKI in non-small cell
lung cancer, target treatment for esophageal squamous cell
carcinoma may be reconsidered.
Recently, the efficacy of novel molecular-targeted
drugs, such as the immune checkpoint inhibitor programmed cell
death-1 (PD-1) inhibitors, in ESCC patients has been demonstrated
in several studies. Several recent studies described a significant
increased density of both effector T lymphocytes and regulatory
tumor infiltrating T lymphocytes in HPV-positive compared to
HPV-negative oropharyngeal squamous cell carcinoma, and highlighted
the predictive value of effector lymphocytes infiltrates (24). We hope that future studies will
clarify the association between HPV infection, tumorigenic
mutational statuses, and the expression of PD-L1 or the efficacy of
novel drugs in CESCC patients.
Several limitations associated with the present
study warrant mention. First, CESCC was less than 5% of ESCC, so
there was insufficient number of enrolled patients. Second, some
data on the patients' background characteristics, such as the
staging and treatment modality, were unavailable. However, it is a
significant research because it is an area rarely reported.
In conclusion, the present study indicated that HPV
infection and EGFR and its pathway-related gene mutations
were present in low proportions in CESCC patients. Furthermore,
these biomarkers might not be associated with the prognosis of
CESCC patients. A future study in a larger population including all
types of esophageal carcinoma patients will be required to clarify
the detailed role of HPV infection, EGFR and its
pathway-related gene mutations in CESCC patients.
Acknowledgements
The authors would like to thank Ms. Hideko Morita
(National Cancer Center Hospital, Tokyo, Japan) for her valuable
assistance with the present research and Dr Suguru Fukahori
VDepartment of Pediatric Surgery, Kurume University School of
Medicine, Kurume, Japan) for proofreading the manuscript.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
MF and KK analyzed and interpreted the patient data
on cervical esophageal squamous cell carcinomas. MF, KK, RO and HT
wrote the manuscript. NT, HS, YH and SI made substantial
contributions in data analysis and interpretation. HT and RO
performed the histological examination of the lesions. AT, TH, YY,
YS, YI, JI, NH, HI, YT, KM and TT helped in acquiring the data for
the work. KK and NB conceived the concept and designed the study.
All authors read and approved the final manuscript.
Ethics approval and consent to
participate
The local Ethics Committee of the National Cancer
Center Hospital (Tokyo, Japan) approved the present study. The
requirement for written informed consent from patients was waived
due to the retrospective design of the study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Grass GD, Cooper SL, Armeson K,
Garrett-Mayer E and Sharma A: Cervical esophageal cancer: A
population-based study. Head Neck. 37:808–814. 2015.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Mendenhall WM, Sombeck MD, Parsons JT,
Kasper ME, Stringer SP and Vogel SB: Management of cervical
esophageal carcinoma. Semin Radiat Oncol. 4:179–191.
1994.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Ajani JA, D'Amico TA, Almhanna K, Bentrem
DJ, Besh S, Chao J, Das P, Denlinger C, Fanta P, Fuchs CS, et al:
Esophageal and esophagogastric junction cancers, version 1.2015. J
Natl Compr Canc Netw. 13:194–227. 2015.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Lordick F, Mariette C, Haustermans K,
Obermannová R and Arnold D: ESMO Guidelines Committee. Oesophageal
cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment
and follow-up. Ann Oncol. 27 (Suppl 5):v50–v57. 2016.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Li G and Sturgis EM: The role of human
papillomavirus in squamous carcinoma of the head and neck. Curr
Oncol Rep. 8:130–139. 2006.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Allum WH, Stenning SP, Bancewicz J, Clark
PI and Langley RE: Long-term results of a randomized trial of
surgery with or without preoperative chemotherapy in esophageal
cancer. J Clin Oncol. 27:5062–5067. 2009.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Ang KK, Harris J, Wheeler R, Weber R,
Rosenthal DI, Nguyen-Tân PF, Westra WH, Chung CH, Jordan RC, Lu C,
et al: Human papillomavirus and survival of patients with
oropharyngeal cancer. N Engl J Med. 363:24–35. 2010.PubMed/NCBI View Article : Google Scholar
|
|
8
|
de Roda Husman AM, Walboomers JM, van den
Brule AJ, Meijer CJ and Snijders PJ: The use of general primers GP5
and GP6 elongated at their 3'ends with adjacent highly conserved
sequences improves human papillomavirus detection by PCR. J Gen
Virol. 76:1057–1062. 1995.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Riethdorf S, Riethdorf L, Milde-Langosch
K, Park TW and Löning T: Differences in HPV 16- and HPV 18 E6/E7
oncogene expression between in situ and invasive adenocarcinomas of
the cervix uteri. Virchows Arch. 437:491–500. 2000.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Nishiwaki M, Yamamoto T, Tone S, Murai T,
Ohkawara T, Matsunami T, Koizumi M, Takagi Y, Yamaguchi J, Kondo N,
et al: Genotyping of human papillomaviruses by a novel one-step
typing method with multiplex PCR and clinical applications. J Clin
Microbiol. 46:1161–1168. 2008.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Sobin LH and Wittekind C (eds): TNM
classification of malignant tumorurs, 6th edition. John Wiley &
Sons, Hoboken, NJ, 2002.
|
|
12
|
Li X, Gao C, Yang Y, Zhou F, Li M, Jin Q
and Gao L: Systematic review with meta-analysis: The association
between human papillomavirus infection and oesophageal cancer.
Aliment Pharmacol Ther. 39:270–281. 2014.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Goto A, Li CP, Ota S, Niki T, Ohtsuki Y,
Kitajima S, Yonezawa S, Koriyama C, Akiba S, Uchima H, et al: Human
papillomavirus infection in lung and esophageal cancers: Analysis
of 485 Asian cases. J Med Virol. 83:1383–1390. 2011.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Wu MY, Liang YR, Wu XY and Zhuang CX:
Relationship between Egr-1 gene expression and apoptosis in
esophageal carcinoma and precancerous lesions. World J
Gastroenterol. 8:971–975. 2002.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Li QD, Li H, Wang MS, Diao TY, Zhou ZY,
Fang QX, Yang FY and Li QH: Multi-susceptibility genes associated
with the risk of the development stages of esophageal squamous cell
cancer in Feicheng County. BMC Gastroenterol. 11(74)2011.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Yasuda M, Kuwano H, Watanabe M, Toh Y,
Ohno S and Sugimachi K: p53 expression in squamous dysplasia
associated with carcinoma of the oesophagus: Evidence for field
carcinogenesis. Br J Cancer. 83:1033–1038. 2000.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Montesano R, Hollstein M and Hainaut P:
Genetic alterations in esophageal cancer and their relevance to
etiology and pathogenesis: A review. Int J Cancer. 69:225–235.
1996.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Zhan C, Yan L, Wang L, Jiang W, Zhang Y,
Xi J, Jin Y, Chen L, Shi Y, Lin Z and Wang Q: Landscape of
expression profiles in esophageal carcinoma by the cancer genome
atlas data. Dis Esophagus. 29:920–928. 2016.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Wang K, Johnson A, Ali SM, Klempner SJ,
Bekaii-Saab T, Vacirca JL, Khaira D, Yelensky R, Chmielecki J,
Elvin JA, et al: Comprehensive genomic profiling of advanced
esophageal squamous cell carcinomas and esophageal adenocarcinomas
reveals similarities and differences. Oncologist. 20:1132–1139.
2015.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Shigaki H, Baba Y, Watanabe M, Miyake K,
Murata A, Iwagami S, Ishimoto T, Iwatsuki M, Yoshida N and Baba H:
KRAS and BRAF mutations in 203 esophageal squamous cell carcinomas:
Pyrosequencing technology and literature review. Ann Surg Oncol. 20
(Suppl 3):S485–S491. 2013.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Cui Y, Chang D, Liu M, Lin C, Zhao B,
Zhang X and Gong M: Identification of exon 19 and 21 mutations of
EGFR gene in Chinese patients with esophageal squamous cell
carcinoma. World J Surg Oncol. 11(266)2013.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Dutton SJ, Ferry DR, Blazeby JM, Abbas H,
Dahle-Smith A, Mansoor W, Thompson J, Harrison M, Chatterjee A,
Falk S, et al: Gefitinib for oesophageal cancer progressing after
chemotherapy (COG): A phase 3, multicentre, double-blind,
placebo-controlled randomised trial. Lancet Oncol. 15:894–904.
2014.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Petty RD, Dahle-Smith A, Stevenson DAJ,
Osborne A, Massie D, Clark C, Murray GI, Dutton SJ, Roberts C,
Chong IY, et al: Gefitinib and EGFR gene copy number aberrations in
esophageal cancer. J Clin Oncol. 35:2279–2287. 2017.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Matlung SE, Wilhelmina van Kempen PM,
Bovenschen N, van Baarle D and Willems SM: Differences in T-cell
infiltrates and survival between HPV+ and HPV-oropharyngeal
squamous cell carcinoma. Future Sci OA. 2(FSO88)2016.PubMed/NCBI View Article : Google Scholar
|