Introduction
Diffuse large B-cell lymphoma (DLBCL) constitutes
25-30% of adult non-Hodgkin lymphomas in developed countries, with
higher percentages in developing countries. This pathology is more
common among elderly individuals (1). Many investigators have investigated
prognostic factors for DLBCL. We have previously reported various
prognostic factors for DLBCL (2-13).
Today, the most reliable and established prognostic factors for
DLBCL are the International Prognostic Index (IPI) and the revised
IPI (R-IPI) (14,15). Usually, the pathogenesis of cancer
cells is considered to involve high levels of reactive oxygen
species (ROS) because of metabolic and signaling abnormalities. ROS
are believed to promote cancer progression through the activation
of oncogenic signaling pathways and damage to DNA (16). Oxidative stress can be defined as an
imbalance between the pro- and anti-oxidant responses of the cell.
Oxidative stress may also result from overproduction of ROS or
insufficient neutralization of ROS by anti-oxidants (17).
The measured concentration is considered to be
directly proportional to the quantity of reactive oxygen
metabolites (ROMs) affected by active ROS and free radicals.
Measuring ROMs thus enables quantitative evaluation of the
condition of oxidative stress throughout the human body (18). Quantification of derivatives of ROMs
(d-ROMs) is a simple method for detecting hydroperoxide levels
(19), and clinical trials have
shown that the d-ROMs test is useful for evaluating oxidative
stress (19,20). Biological antioxidant potential
(BAP) can be measured simultaneously.
ROS function may be a key to many impaired
biological processes, including cancers. Various investigators have
reported that oxidative stress plays an important role in
carcinogenesis, including for lung cancer (21-23),
hepatocellular carcinoma (24,25),
colorectal cancer (26), and
ovarian cancer (27). However, we
could only identify one report that investigated associations
between oxidative stress and hematological malignancies (28). Here, we aimed to investigate the
role of oxidative stress as a prognostic factor for DLBCL in a
retrospective analysis.
Patients and methods
Study design
This retrospective study was organized by Gifu
University Graduate School of Medicine (Gifu, Japan). Participants
were patients with untreated CD20-positive DLBCL at Gifu University
Hospital. The initial cohort comprised 55 consecutive patients
histologically diagnosed with DLBCL between December 2012 and March
2016 according to the 2008 classification of the World Health
Organization (WHO) (29). All
follow-up data were updated as of April 12, 2019. Thirty-six
healthy volunteers (10 men, 26 women) served as a control group.
All patients provided written informed consent to participate in
the study according to the guidelines of our institution and the
Declaration of Helsinki. Samples were acquired during routine
diagnostic assessments. This study was approved by the
institutional review board at our institution (Gifu University
Graduate School of Medicine, approval no. 2018-003).
Oxidative stress and other
determinations
Oxidative stress was investigated by measuring serum
hydroperoxide concentrations according to the d-ROMs test (Diacron
International srl) using a free radical elective evaluator, FREE
(Diacron International srl), as described previously (19,20,24,30).
Similarly, a commercially available BAP test was used to assess
antioxidant levels (Diacron International srl), as described
previously (31). The
antioxidative/oxidative stress ratio was calculated as BAP/d-ROMs.
Peripheral white blood cell count (WBC) and serum concentrations of
lactate dehydrogenase (LDH), soluble interleukin 2 receptor
(sIL-2R), and C-reactive protein (CRP) were determined on
admission.
Treatment strategy
Patients received 6-8 cycles of either R-CHOP or
R-THP-COP. These regimens comprised rituximab (R; 375
mg/m2, as a 4-h intravenous (i.v.) drip infusion on day
1), cyclophosphamide (C; 750 mg/m2, as a 2-h i.v. drip
infusion on day 3), doxorubicin (H; 50 mg/m2, as a
30-min i.v. drip infusion on day 3) or tetrahydropyranyl-adriamycin
(THP; 50 mg/m2, as a 30-min i.v. drip infusion on day
3), vincristine (O; 1.4 mg/m2, maximal dose 2.0 mg i.v.
as a bolus over 5 min on day 3), and prednisolone [P; 100 mg/day
per os (p.o.) on days 3-7]. The R-THP-COP regimen included THP, an
anthracycline derivative of doxorubicin reportedly offering lower
cardiotoxicity than doxorubicin (32,33).
Our previous prospective randomized study found no significant
differences in remission or survival rates between CHOP and THP-COP
therapies (34). In addition, we
reported the utility and safety of R-THP-COP from a single-arm
phase II study (35,36) and a randomized phase III study
(37). Granulocyte
colony-stimulating factor (G-CSF) was administered at the
discretion of the physician. Patients with a bulky mass received
radiotherapy after chemotherapy. Patients who relapsed or in whom
disease progressed after R-CHOP or R-THP-COP, and those who were
resistant to R-CHOP or R-THP-COP underwent salvage chemotherapy
with R-P-IMVP-16/CBDCA (rituximab, methylprednisolone, ifosfamide,
methotrexate, etoposide, and carboplatin) (38,39). A
proportion of patients with refractory or relapsed DLBCL who
responded to R-P-IMVP-16/CBDCA received high-dose chemotherapy
followed by autologous peripheral blood stem cell
transplantation.
Response criteria
Treatment response was evaluated after the 2nd, 4th,
6th, and final cycles of chemotherapy. Treatment responses were
categorized after repeated physical examinations, radiological
studies, gallium scintigraphy, fluorodeoxyglucose-positron emission
tomography, and bone-marrow evaluation according to the 2007
International Working Group Criteria (40).
Statistical analysis
Data are expressed as median. Differences in mean
values were tested using the nonparametric Mann-Whitney U-test and
Kruskal-Wallis test. For comparisons among ≥3 groups, differences
in mean values were tested using the nonparametric Kruskal-Wallis
test followed by Dunn's post hoc test. Spearman's correlation
coefficient was used to test correlations between d-ROMs and other
serum markers. Effects of d-ROMs and other serum markers of
survival were examined by univariate analyses using the log-rank
test based on Kaplan and Meier methods (41). Multivariate analysis was performed
using the Cox proportional-hazards regression technique to define
the prognostic significance of selected variables including d-ROM
and BAP. Values of P<0.05 were considered significant.
Results
Patient characteristics
A total of 55 patients were enrolled in the present
study. Table I summarizes the
clinical characteristics of patients (median age, 72 years; range,
36-93 years). Thirty-six healthy volunteers were enrolled (median
age, 50.5 years; range, 25-82 years) (Table I). A significant difference in age
was identified between DLBCL patients and controls (P<0.01).
 | Table IClinical characteristics of the
patients with diffuse large B cell lymphoma (n=55). |
Table I
Clinical characteristics of the
patients with diffuse large B cell lymphoma (n=55).
| Variable | No. (%) |
|---|
| Sex | |
|
Male | 36 (65.0) |
|
Female | 19 (35.0) |
| Age, years | |
|
<61 | 7 (12.7) |
|
≥61 | 48 (87.3) |
| PS | |
|
0, 1 | 46 (84.0) |
|
2-4 | 9 (16.0) |
| LDH | |
|
Normal | 19 (35.00 |
|
Increased | 36 (65.0) |
| Extranodal
sites | |
|
0, 1 | 37 (67.3) |
|
≥2 | 18 (32.7) |
| Clinical stage | |
|
I/II | 17 (31.0) |
|
III/IV | 38 (69.0) |
| B symptom | |
|
Absence | 13 (24.0) |
|
Presence | 42 (76.0) |
| Bulky disease | |
|
Absence | 47 (85.0) |
|
Presence | 8 (15.0) |
| sIL-2R, U/ml | |
|
<2,000 | 38 (69.0) |
|
≥2,000 | 17 (31.0) |
| IPI | |
|
Low | 11 (20.0) |
|
Low-intermediate | 13 (24.0) |
|
High-intermediate | 21 (38.0) |
|
High | 10 (18.0) |
| R-IPI | |
|
Very
good | 1 (1.8) |
|
Good | 24 (43.6) |
|
Poor | 30 (54.50 |
d-ROMs and BAP in DLBCL patients and
healthy controls
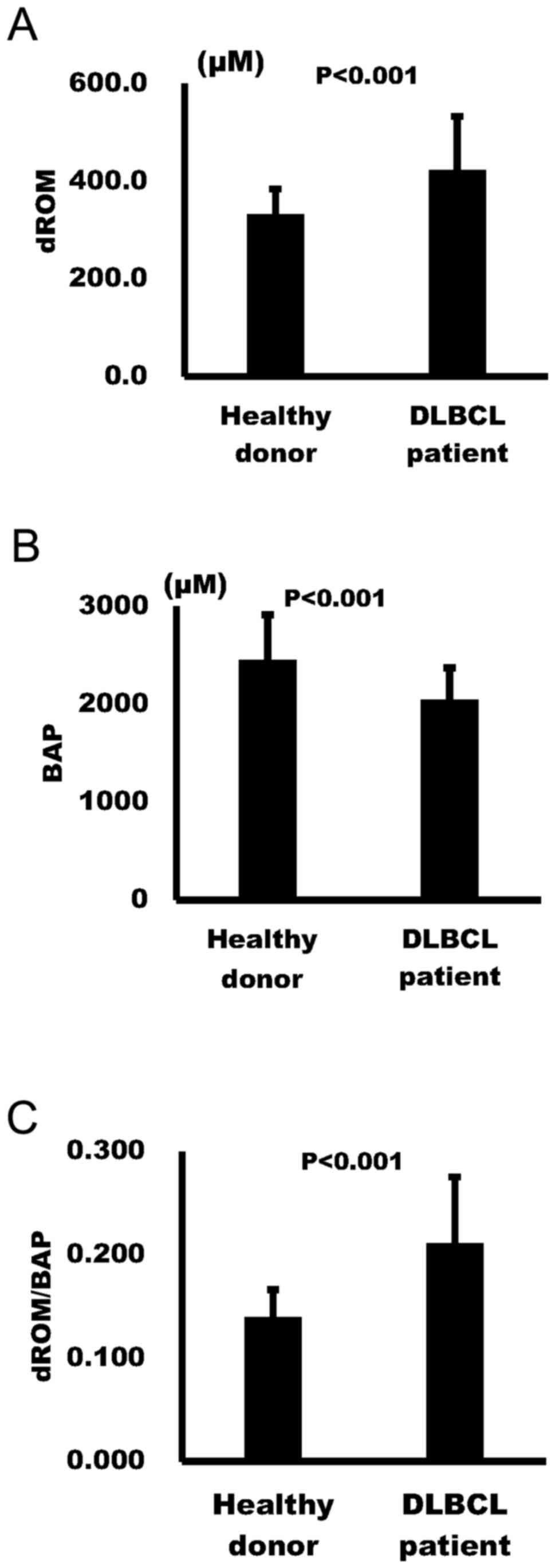
Median d-ROMs concentration was significantly
increased among healthy volunteers (329 µM) compared to DLBCL
patients (425 µM; P<0.001) (Fig.
1A). In contrast, median BAP values were significantly
decreased in DLBCL patients (2,002 µM) compared to healthy
volunteers (2,352 µM; P<0.001) (Fig.
1B). In addition, the d-ROMs/BAP ratio was significantly higher
in DLBCL patients (0.203) than in healthy volunteers (0.137;
P<0.001) (Fig. 1C). Cut-offs
were 425 µM for d-ROMs, 2,002 µM for BAP, and 0.203 for d-ROM/BAP,
all of which essentially represented median values for all DLBCL
patients.
Correlations between d-ROMs and other
markers in DLBCL patients
Table II shows
correlations between d-ROMs, BAP, d-ROMs/BAP and other markers in
DLBCL patients. No significant correlation existed between d-ROMs
and clinical stage in DLBCL patients. Significant correlations
existed between d-ROMs and LDH (P<0.01), between d-ROMs and
sIL-2R (P<0.001), between d-ROMs and IPI (P<0.05), between
d-ROMs and B symptoms (P<0.001), and between d-ROMs and bulky
disease (P<0.01) in patients with DLBCL. Significant
correlations existed between BAP and IPI (P<0.001). No
significant correlations existed between BAP and clinical stage,
between BAP and sIL-2R, between BAP and B symptoms, between BAP and
LDH, between BAP and performance status (PS) or between BAP and
bulky disease in patients with DLBCL. Significant correlations
existed between d-ROM/BAP and clinical stage (P<0.05), between
d-ROM/BAP and sIL-2R (P<0.0001), between d-ROM/BAP and IPI
(P<0.05), and between d-ROM/BAP and B symptoms (P<0.001) in
patients with DLBCL.
| Table IIAssociation between oxidative stress
markers and other markers in diffuse large B cell lymphoma. |
Table II
Association between oxidative stress
markers and other markers in diffuse large B cell lymphoma.
| | d-ROM (µM) | BAP (µM) | d-ROM/BAP |
|---|
| Variable | Median | Range | P-value | Median | Range | P-value | Median | Range | P-value |
|---|
| Sex | | | | | | | | | |
|
Male | 426 | 262-660 | 0.3427 | 1999 | 1468-2653 | 0.8527 | 0.20 | 0.124-0.432 | 0.7028 |
|
Female | 381 | 171-658 | | 2126 | 1571-2812 | | 0.21 | 0.100-0.360 | |
| Age, years | | | | | | | | | |
|
<61 | 415 | 303-660 | 0.6483 | 2213 | 1640-2609 | 0.2450 | 0.23 | 0.129-0.253 | 0.6483 |
|
≥61 | 426 | 171-658 | | 1998 | 1468-2812 | | 0.20 | 0.100-0.432 | |
| PS | | | | | | | | | |
|
0, 1 | 402 | 171-660 | 0.3011 | 2129 | 1538-2812 | 0.0248 | 0.19 | 0.100-0.360 | 0.0248 |
|
2-4 | 497 | 280-634 | | 1728 | 1468-2457 | | 0.29 | 0.181-0.432 | |
| LDH | | | | | | | | | |
|
Normal | 364 | 247-474 | 0.0372 | 2175 | 1626-2563 | 0.4515 | 0.17 | 0.100-0.266 | 0.0491 |
|
Increased | 440 | 171-660 | | 1981 | 1484-2812 | | 0.23 | 0.101-0.432 | |
| Extranodal
sites | | | | | | | | | |
|
0, 1 | 435 | 171-660 | 0.6307 | 1998 | 1468-2609 | 0.2911 | 0.19 | 0.101-0.432 | 0.5036 |
|
≥2 | 434 | 247-622 | | 2113 | 2113-2812 | | 0.21 | 0.100-0.297 | |
| Clinical stage | | | | | | | | | |
|
I/II | 378 | 269-474 | 0.0618 | 2178 | 1571-2572 | 0.0900 | 0.17 | 0.124-0.245 | 0.0469 |
|
III/IV | 435 | 171-660 | | 1981 | 1468-2812 | | 0.22 | 0.100-0.432 | |
| B symptom | | | | | | | | | |
|
Absence | 378 | 171-660 | 0.0054 | 2138 | 1538-2653 | 0.3043 | 0.19 | 0.100-0.293 | 0.0021 |
|
Presence | 553 | 321-658 | | 1908 | 1468-2812 | | 0.29 | 0.165-0.432 | |
| Bulky disease | | | | | | | | | |
|
Absence | 389 | 171-658 | 0.0089 | 2059 | 1538-2812 | 0.4118 | 0.19 | 0.100-0.360 | 0.0018 |
|
Presence | 552 | 381-660 | | 1736 | 1468-2609 | | 0.26 | 0.242-0.432 | |
| sIL-2R, U/ml | | | | | | | | | |
|
<2,000 | 378 | 247-660 | 0.0112 | 2168 | 1538-2812 | 0.0121 | 0.18 | 0.100-0.266 | 0.0066 |
|
≥2,000 | 507 | 171-658 | | 1825 | 1468-2543 | | 0.28 | 0.101-0.432 | |
| IPI | | | | | | | | | |
|
Low | 364 | 292-474 | 0.0394 | 2203 | 1782-2563 | 0.0023 | 0.17 | 0.129-0.228 | 0.0122 |
|
Low-intermediate | 389 | 269-660 | | 2126 | 1697-2609 | | 0.19 | 0.124-0.266 | |
|
High-intermediate | 415 | 171-658 | | 1773 | 1468-2482 | | 0.24 | 0.1-0.432 | |
|
High | 521 | 343-622 | | 2195 | 1825-2812 | | 0.22 | 0.129-0.297 | |
| R-IPI | | | | | | | | | |
|
Very good (0
points)a | 378 | 378 | 0.1507 | 2213 | 2213 | 0.0956 | 0.17 | 0.171 | 0.0470 |
|
Good (1 and
2 points) | 376 | 269-660 | | 2176 | 1697-2609 | | 0.18 | 0.124-0.266 | |
|
Poor (3-5
points) | 442 | 171-658 | | 1904 | 1468-2812 | | 0.23 | 0.10-0.432 | |
Analysis of response to therapy
Table III shows
the results of analysis of complete remission (CR) rates in DLBCL
patients. The CR rate for all DLBCL patients was 83.6%. CR rates of
patients with d-ROM <425 and ≥425 µM were 81.5 and 85.7%,
respectively [not significant (NS)]. CR rates of patients with BAP
<2,002 and ≥2,002 µM were 77.8 and 88.9%, respectively (NS). CR
rates of patients with d-ROM/BAP <0.203 and ≥0.203 were 88.9 and
77.8%, respectively (NS). No factors were significantly associated
with CR rates in DLBCL patients.
| Table IIIUnivariate analysis of remission rate
in diffuse large B cell lymphoma. |
Table III
Univariate analysis of remission rate
in diffuse large B cell lymphoma.
| | CR |
|---|
| Variable | Total no. of
patients | % | P-value |
|---|
| All patients | 55 | 83.6 | |
| Sex | | | |
|
Male | 36 | 78.9 | 0.4947 |
|
Female | 19 | 86.1 | |
| Age, years | | | |
|
<61 | 7 | 85.7 | 0.8736 |
|
≥61 | 48 | 83.3 | |
| PS | | | |
|
0, 1 | 46 | 84.8 | 0.6034 |
|
2-4 | 9 | 77.8 | |
| LDH | | | |
|
Normal | 19 | 94.7 | 0.106 |
|
Increased | 36 | 77.8 | |
| Extranodal
sites | | | |
|
0, 1 | 37 | 86.5 | 0.9662 |
|
≥2 | 18 | 77.8 | |
| Clinical stage | | | |
|
I/II | 17 | 88.2 | 0.6198 |
|
III/IV | 38 | 81.6 | |
| B symptom | | | |
|
Absence | 13 | 81.0 | 0.3335 |
|
Presence | 42 | 92.3 | |
| Bulky disease | | | |
|
Absence | 47 | 87.2 | 0.0804 |
|
Presence | 8 | 62.5 | |
| sIL-2R, U/ml | | | |
|
<2,000 | 38 | 81.6 | 0.5375 |
|
≥2,000 | 17 | 88.2 | |
| IPI | | | |
|
Low | 11 | 100.0 | 0.0577 |
|
Low-intermediate | 13 | 92.3 | |
|
High-intermediate | 21 | 66.7 | |
|
High | 10 | 90.0 | |
| R-IPI | | | |
|
Very
good | 1 | 100.0 | 0.0982 |
|
Good | 24 | 91.7 | |
|
Poor | 30 | 76.7 | |
| d-ROM | | | |
|
<425
µM | 22 | 81.5 | 0.6714 |
|
≥425 µM | 24 | 85.7 | |
| BAP | | | |
|
≥2,002
µM | 24 | 88.9 | 0.2488 |
|
<2,002
µM | 21 | 77.8 | |
| d-ROM/BAP | | | |
|
<0.203 | 24 | 88.9 | 0.2488 |
|
≥0.203 | 21 | 77.8 | |
Oxidative stress as a prognostic
factor in DLBCL
Table IV shows the
results of univariate analyses for survival rates in DLBCL. Median
follow-up period was 26.2 months. Three-year overall survival (OS)
rates for patients with d-ROMs <425 and ≥425 µM were 67.2 and
72.0%, respectively (NS, Fig. 2A).
Three-year OS rates for patients with BAP <2,002 and ≥2,002 µM
were 60.9 and 75.9%, respectively (NS, Fig. 2B). Three-year OS rates for patients
with d-ROMs/BAP <0.203 and ≥0.203 were 65.5 and 71.6%,
respectively (NS, Fig. 2C). Other
factors associated with significantly worse OS were poor PS (>1)
and unfavorable IPI (high intermediate and high risk groups).
Three-year progression-free survival (PFS) rates for patients with
d-ROMs <425 and ≥425 µM were 66.7 and 65.1%, respectively (NS,
Fig. 2D). Three-year PFS rates for
patients with BAP <2,002 and ≥2,002 µM were 54.0 and 73.7%,
respectively (NS, Fig. 2E).
Three-year PFS rates for patients with d-ROMs/BAP <0.203 and
≥0.203 were 66.7 and 65.1%, respectively (NS, Fig. 2F). Other factors associated with
significantly worsened PFS were advanced stage (III or IV), and
unfavorable IPI (HI and H risk groups) (Table I).
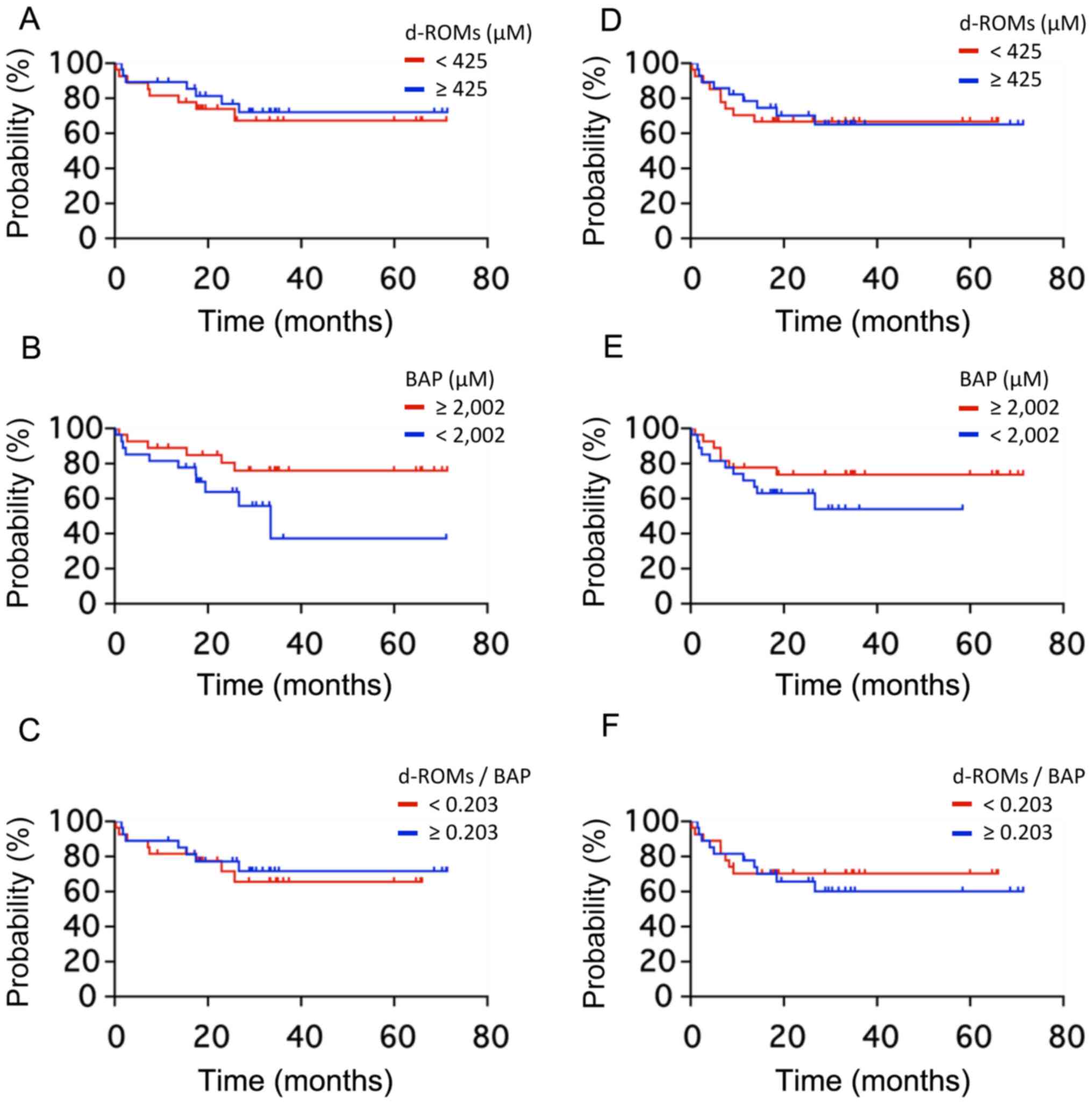 | Figure 2OS and PFS curves according to
d-ROMs, BAP and d-ROMs/BAP ratio in patients with DLBCL. (A) 3-year
OS rates for patients with d-ROMs <425 and ≥425 µM were 67.2 and
72.0%, respectively (NS). (B) 3-year OS rates for patients with BAP
<2,002 and ≥2,002 µM were 60.9 and 75.9%, respectively (NS). (C)
3-year OS rates for patients with d-ROMs/BAP <0.203 and ≥0.203
were 65.5 and 71.6%, respectively (NS). (D) 3-year PFS rates for
patients with d-ROMs <425 and ≥425 µM were 66.7 and 65.1%,
respectively (NS). (E) 3-year PFS rates for patients with BAP
<2,002 and ≥2,002 µM were 54.0 and 73.7%, respectively (NS). (F)
3-year PFS rates for patients with d-ROMs/BAP <0.203 and ≥0.203
were 66.7 and 65.1%, respectively (NS). OS, overall survival; PFS,
progression-free survival; d-ROMs, derivatives of reactive oxygen
metabolites; BAP, biological antioxidant potential; DLBCL, diffuse
large B-cell lymphoma; NS, not significant. |
| Table IVUnivariate analysis of survival rate
in diffuse large B cell lymphoma. |
Table IV
Univariate analysis of survival rate
in diffuse large B cell lymphoma.
| | 3 year-OS | 3 year-PFS |
|---|
| Variable | No. of
patients | % | P-value | No. of
patients | % | P-value |
|---|
| All patients | 55 | 69.3 | | 55 | 65.5 | |
| Age, years | | | | | | |
|
<61 | 7 | 100.0 | 0.1129 | 7 | 71.4 | 0.5840 |
|
≥61 | 48 | 58.1 | | 48 | 47.8 | |
| PS | | | | | | |
|
0, 1 | 46 | 76.1 | 0.0101 | 46 | 71.3 | 0.0940 |
|
2-4 | 9 | NR | | 9 | NR | |
| LDH | | | | | | |
|
Normal | 19 | 86.1 | 0.0541 | 19 | 89.1 | 0.0311 |
|
Increased | 36 | 50.2 | | 36 | 45.0 | |
| Extranodal
sites | | | | | | |
|
0, 1 | 37 | 72.0 | 0.8239 | 37 | 70.8 | 0.4569 |
|
≥2 | 18 | 63.8 | | 18 | 53.9 | |
| Clinical stage | | | | | | |
|
I/II | 17 | 87.8 | 0.3399 | 17 | 87.8 | 0.0433 |
|
III/IV | 38 | 61.6 | | 38 | 55.7 | |
| B symptom | | | | | | |
|
Absence | 13 | 64.9 | 0.2503 | 13 | 66.1 | 0.3018 |
|
Presence | 42 | 61.5 | | 42 | 48.5 | |
| Bulky disease | | | | | | |
|
Absence | 47 | 70.1 | 0.5217 | 47 | 71.1 | 0.1580 |
|
Presence | 8 | 37.5 | | 8 | 25.0 | |
| sIL-2R, U/ml | | | | | | |
|
<2,000 | 38 | 70.6 | 0.8837 | 38 | 70.6 | 0.7164 |
|
≥2,000 | 17 | 66.5 | | 17 | 54.5 | |
| IPI | | | | | | |
|
Low | 11 | 100.0 | 0.0382 | 11 | 100.0 | 0.0232 |
|
Low-intermediate | 13 | 82.1 | | 13 | 76.9 | |
|
High-intermediate | 21 | 52.7 | | 21 | 49.0 | |
|
High | 10 | 54.9 | | 10 | 43.8 | |
| R-IPI | | | | | | |
|
Very
good | 1 | NR | 0.0533 | 1 | 100.0 | 0.0169 |
|
Good | 24 | 85.4 | | 24 | 82.9 | |
|
Poor | 30 | 54.9 | | 30 | 50.2 | |
| d-ROM | | | | | | |
|
<425
µM | 27 | 67.2 | 0.4369 | 27 | 66.7 | 0.4104 |
|
≥425 µM | 28 | 72.0 | | 28 | 65.1 | |
| BAP | | | | | | |
|
≥2,002
µM | 27 | 75.9 | 0.2510 | 27 | 73.7 | 0.2055 |
|
<2,002
µM | 27 | 60.9 | | 27 | 54.0 | |
| d-ROM/BAP | | | | | | |
|
<0.203 | 27 | 65.5 | 0.9217 | 27 | 60.2 | 0.8086 |
|
≥0.203 | 27 | 71.6 | | 27 | 70.4 | |
Multivariate analyses for OS and PFS
(Table V)
Multivariate analyses identified age, PS, clinical
stage, and sIL-2R as independent prognostic factors for OS, and
LDH, clinical stage, and d-ROMs as independent prognostic factors
for PFS.
Discussion
Oxidative stress might play an important role in
carcinogenesis. Excessive production of ROS has been reported to
cause damage to cellular macromolecules such as DNA (42), and can increase levels of various
types of DNA damage, including DNA base damage and single- and
double-strand breaks (43,44). In addition, excessive production of
ROS could interrupt the tumor cell signaling pathways, which are
involved in cell growth and survival. This obstruction might lead
to cancer promotion and progression. Indeed, many reports have
shown that oxidative stress might play important roles in
carcinogenesis for some malignancies (21-27).
Tsukioka et al (21)
reported preoperative serum levels of ROMs as a significant
independent predictor of nodal involvement in patients with
clinical stage I lung adenocarcinoma. Oxidative stress could be
reasonably expected to impact the progression of lung cancer,
because the lung is the organ most affected by increased oxidative
stress. Gencer et al (23)
reported that serum levels of ROMs were increased in patients with
different types of lung cancers and speculated that serum levels of
ROMs may offer an index parameter for lung cancer. The role of ROS
in colorectal cancer was examined by Inokuma et al (26). They reported that serum ROS levels
were elevated in proportion to tumor invasion and showed a
significant positive correlation with tumor size. Suzuki et
al (24) reported that
hepatocellular carcinoma patients with increased levels of
oxidative stress were prone to recurrence after curative
treatment.
The present study found a significant difference in
age between DLBCL patients and controls. A previous study reported
that oxidative stress was associated with mortality in older ages
(45). We could not exclude the
potential impact of aging on the production of oxidative stressors.
Generally, elderly individuals comprise the majority of DLBCL
patients, and age represents an important prognostic factor for
DLBCL. We suspected that the production of oxidative stress might
affect not only the carcinogenesis of DLBCL but also the poor
prognosis in elderly patients with DLBCL. One possibility is that
d-ROMs, BAP, and d-ROMs/BAP ratio might reflect the risk of
inflammatory complications such as pneumonia in DLBCL patients. We
cannot deny the possibility that inflammatory complications
affected d-ROMs and BAP concentrations. When d-ROMs and BAP were
measured in DLBCL patients on admission, no cases were complicated
with inflammatory diseases such as pneumonia. Indeed, a significant
correlation existed between d-ROMs and B symptoms.
In the present study, d-ROMs in DLBCL patients were
increased compared to those in healthy volunteers. Similarly, BAP
in DLBCL patients was decreased compared to that in healthy
volunteers. As a result, the d-ROMs/BAP ratio was significantly
higher in DLBCL patients than in healthy volunteers. These results
suggest that oxidative stress contributes to carcinogenesis in
DLBCL by damaging DNA. Our study could not find any positive
correlation between d-ROMs and clinical stage. This result suggests
that d-ROMs might not reflect the volume of lymphoma cells
directly. Meanwhile, d-ROMs correlated significantly with both
sIL-2R and IPI, which are recognized as powerful prognostic factors
for DLBCL. Unfortunately, no significant difference in CR rates was
seen between patients with d-ROMs <425 and ≥425 µM, BAP
<2,002 and ≥2,002 µM, or d-ROMs/BAP <0.203 and ≥0.203. In
addition, no significant differences in 3-year OS rates were
identified between patients with d-ROMs <425 and ≥425 µM.
Similarly, no significant differences were observed for BAP and
d-ROMs/BAP ratio. However, multivariate analysis revealed d-ROMs as
an independent prognostic factor for DLBCL patients in PFS. This
result showed that oxidative stress may impact prognosis in DLBCL
patients. At the same time, we should discuss the discrepancy
between the results from uni- and multivariate analyses. We
considered that some differences in background characteristics
exist between high- and low-d-ROMs patients. Such differences in
background may have contributed to discrepancies between results
from uni- and multivariate analyses. If we could match backgrounds
between high- and low-d-ROMs patients, univariate analyses might
reveal some significant differences. Multivariate analysis offers a
useful method to address the issue of differences in background
characteristics. Indeed, the present study found significant
deviations in LDH, B symptoms, and sIL-2R (data not shown). To
clarify these problems, prospective studies are required. Recently,
Nojima et al (28) reported
the role of oxidative stress in DLBCL. They measured d-ROMs and BAP
in patients with non-Hodgkin's lymphoma (NHL), similar to our
study. Defining oxidation stress index (OSI) as OSI=C x
(d-ROMs/BAP), where C denotes a coefficient for standardization to
set the mean OSI in healthy individuals at 1.0), they reported OSI
as significantly higher in DLBCL patients with advanced clinical
stage compared to localized stage. They therefore claimed that the
OSI might offer a useful clinical marker for NHL. However, they did
not show differences in either CR rates or survival rates according
to oxidative stress.
The issue of d-ROMs and BAP in lymphoma tissue is
very interesting, but unfortunately we did not measure these
concentrations in lymphoid tumor tissue. We therefore could not
clarify the associations between d-ROMs and BAP concentrations in
lymphoma tissue and serum. We consider that d-ROMs and BAP
concentrations in lymphoid tumor tissue may correlate with serum
concentrations, but serum concentrations of d-ROMs and BAP may also
reflect immune responses of the whole body to lymphoid
malignancies. Measurement of d-ROMs and BAP concentrations in
lymphoid tumor tissue may clarify which cells produce the oxidative
stress and the mechanisms by which oxidative stress affects the
carcinogenesis of DLBCL.
In the present study, cases with high LDH levels
showed higher levels of d-ROMs than those with low LDH levels. This
may indicate that LDH reflects global dynamic metabolic reactions,
including ROS. In addition, a previous study of population-based
cohorts found that levels of d-ROMs were strongly associated with
cancer mortality (46). In the
present study, concentrations of d-ROMs were significantly higher
in DLBCL patients than in healthy volunteers, and oxidative stress
may also be associated with an increased risk of DLBCL (47).
In conclusion, levels of d-ROMs were significantly
higher in DLBCL patients than in healthy volunteers. Although
univariate analysis revealed that oxidative stress did not impact
the prognosis of untreated patients with DLBCL, multivariate
analysis revealed d-ROMs as an independent prognostic factor for
DLBCL patients in PFS. These results showed that oxidative stress
plays important roles in carcinogenesis for DLBCL patients.
Acknowledgements
The authors would like to thank the participating
physicians, Dr Yoshikazu Ikoma, Dr Kaneda Yuto, Dr Kimihiro
Yamaguchi and Dr Eri Takada. The authors are also grateful to Ms.
Chiyoko Sano, Ms. Hitomi Fujisawa, Ms. Miho Yagi and Ms. Eriko
Kunishima (all First Department of Internal Medicine, Gifu
University Graduate School of Medicine, Gifu, Japan) for their
administrative and technical assistance. This abstract was
presented at the 17th Japanese Society of Medical Oncology Annual
Meeting (July 18-20, 2019 in Kyoto, Japan) and was published as
Abstract no. P3-085.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
HT, MS and TH designed the present study. HN, RM,
TM, NN, JK and YK developed the methodology and assessed the
authenticity of the raw data. TM, NN, SN, JK, YK, TsT, TM and TaT
provided resources. HN, SN, NN, NK, TsT, TM and TaT performed the
experiments. HN and TH wrote the original draft. MS and HT reviewed
and edited the manuscript. All authors read and approved the final
version of the manuscript.
Ethics approval and consent to
participate
Investigations were performed in compliance with the
principles of good clinical practice outlined in the Declaration of
Helsinki and federal guidelines, and had approval by the Medical
Review Board of Gifu University Graduate School of Medicine, Gifu,
Japan (approval no. 2018-003). Written informed consent was
obtained from each participant.
Patient consent for publication
Consent for publication was obtained from any
individual person whose data are included in this manuscript.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Swerdlow SH, Campo E, Harris NL, Jaffe ES,
Pileri SA and Stein H (eds): WHO Classification of Tumours of
Haematopoietic and Lymphoid Tissues. IARC Press, Lyon, pp 291-297,
2017.
|
|
2
|
Yamamoto Y, Goto N, Takemura M, Yamasuge
W, Yabe K, Takami T, Miyazaki T, Takeuchi T, Shiraki M, Shimizu M,
et al: Association between increased serum GP88 (progranulin)
concentrations and prognosis in patients with malignant lymphomas.
Clin Chim Acta. 473:139–146. 2017.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Nakamura N, Hara T, Shibata Y, Matsumoto
T, Nakamura H, Ninomiya S, Kito Y, Kitagawa J, Kanemura N, Goto N,
et al: Sarcopenia is an independent prognostic factor in male
patients with diffuse large B-cell lymphoma. Ann Hematol.
94:2043–2053. 2015.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Nakamura N, Goto N, Tsurumi H, Takemura M,
Kanemura N, Kasahara S, Hara T, Yasuda I, Shimizu M, Sawada M, et
al: Serum level of soluble tumor necrosis factor receptor 2 is
associated with the outcome of patients with diffuse large B-cell
lymphoma treated with the R-CHOP regimen. Eur J Haematol.
91:322–331. 2013.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Goto N, Tsurumi H, Takemura M, Kanemura N,
Kasahara S, Hara T, Yasuda I, Shimizu M, Yamada T, Sawada M, et al:
Serum soluble CD27 level is associated with outcome in patients
with diffuse large B-cell lymphoma treated with rituximab,
cyclophosphamide, doxorubicin, vincristine and prednisolone. Leuk
Lymphoma. 53:1494–1500. 2012.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Goto N, Tsurumi H, Goto H, Shimomura YI,
Kasahara S, Hara T, Yasuda I, Shimizu M, Murakami N, Yoshikawa T,
et al: Serum soluble interleukin-2 receptor (sIL-2R) level is
associated with the outcome of patients with diffuse large B cell
lymphoma treated with R-CHOP regimens. Ann Hematol. 91:705–714.
2012.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Ninomiya S, Hara T, Tsurumi H, Goto N,
Saito K, Seishima M, Takami T and Moriwaki H: Indoleamine
2,3-dioxygenase expression and serum kynurenine concentrations in
patients with diffuse large B-cell lymphoma. Leuk Lymphoma.
53:1143–1145. 2012.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Goto N, Tsurumi H, Kasahara S, Kanemura N,
Hara T, Yasuda I, Shimizu M, Murakami N, Sawada M, Yamada T, et al:
Serum interleukin-18 level is associated with the outcome of
patients with diffuse large B-cell lymphoma treated with CHOP or
R-CHOP regimens. Eur J Haematol. 87:217–227. 2011.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Ninomiya S, Hara T, Tsurumi H, Hoshi M,
Kanemura N, Goto N, Kasahara S, Shimizu M, Ito H, Saito K, et al:
Indoleamine 2,3-dioxygenase in tumor tissue indicates prognosis in
patients with diffuse large B-cell lymphoma treated with R-CHOP.
Ann Hematol. 90:409–416. 2011.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Yoshikawa T, Hara T, Tsurumi H, Goto N,
Hoshi M, Kitagawa J, Kanemura N, Kasahara S, Ito H, Takemura M, et
al: Serum concentration of L-kynurenine predicts the clinical
outcome of patients with diffuse large B-cell lymphoma treated with
R-CHOP. Eur J Haematol. 84:304–309. 2010.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Hara T, Tsurumi H, Goto N, Kanemura N,
Yoshikawa T, Kasahara S, Yamada T, Sawada M, Goto H, Fukuno K, et
al: Serum soluble Fas level determines clinical outcome of patients
with diffuse large B-cell lymphoma treated with CHOP and R-CHOP. J
Cancer Res Clin Oncol. 135:1421–1428. 2009.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Kojima Y, Tsurumi H, Goto N, Shimizu M,
Kasahara S, Yamada T, Kanemura N, Hara T, Sawada M, Saio M, et al:
Fas and Fas ligand expression on germinal center type-diffuse large
B-cell lymphoma is associated with the clinical outcome. Eur J
Haematol. 76:465–472. 2006.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Watanuki-Miyauchi R1, Kojima Y, Tsurumi H,
Hara T, Goto N, Kasahara S, Saio M, Moriwaki H and Takami T:
Expression of survivin and of antigen detected by a novel
monoclonal antibody, T332, is associated with outcome of diffuse
large B-cell lymphoma and its subtypes. Pathol Int. 55:324–330.
2005.PubMed/NCBI View Article : Google Scholar
|
|
14
|
International Non-Hodgkin's Lymphoma
Prognostic Factors Project. A predictive model for aggressive
non-Hodgkin's lymphoma. N Engl J Med. 329:987–994. 1993.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Sehn LH, Berry B, Chhanabhai M, Fitzgerald
C, Gill K, Hoskins P, Klasa R, Savage KJ, Shenkier T, Sutherland J,
et al: The revised International Prognostic Index(R-IPI)is a better
predictor of outcome than the standard IPI for patients with
diffuse large B-cell lymphoma treated with R-CHOP. Blood.
109:1857–1861. 2007.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Gorrini C, Harris IS and Mak TW:
Modulation of oxidative stress as an anticancer strategy. Nat Rev
Drug Discov. 12:931–947. 2013.PubMed/NCBI View
Article : Google Scholar
|
|
17
|
Salzman R, Pácal L, Kaňková K, Tomandl J,
Horáková Z, Tóthová E and Kostřica R: High perioperative level of
oxidative stress as a prognostic tool for identifying patients with
a high risk of recurrence of head and neck squamous cell carcinoma.
Int J Clin Oncol. 15:565–570. 2010.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Cesarone MR, Belcaro G, Carratelli M,
Cornelli U, De Sanctis MT, Incandela L, Barsotti A, Terranova R and
Nicolaides A: A simple test to monitor oxidative stress. Int
Angiol. 18:127–130. 1999.PubMed/NCBI
|
|
19
|
Trotti R, Carratelli M and Barbieri M:
Performance and clinical application of a new, fast method for the
detection of hydroperoxides in serum. Panminerva Med. 44:37–40.
2002.PubMed/NCBI
|
|
20
|
Hirose H, Kawabe H, Komiya N and Saito I:
Relations between serum reactive oxygen metabolites (ROMs) and
various inflammatory and metabolic parameters in a Japanese
population. J Atheroscler Thromb. 16:77–82. 2009.PubMed/NCBI View
Article : Google Scholar
|
|
21
|
Tsukioka T, Nishiyama N, Iwata T, Nagano
K, Tei K and Suehiro S: Preoperative serum oxidative stress marker
as a strong indicator of nodal involvement in clinical stage I lung
adenocarcinoma. Int J Clin Oncol. 17:250–255. 2012.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Miyazaki T, Takagi K, Mine M, Yamasaki N,
Tsuchiya T, Matsumoto K, Hatachi G, Izumino H, Doi R, Machino R and
Nagayasu T: Video-assisted thoracic surgery attenuates
perioperative oxidative stress response in lung cancer patients: A
preliminary study. Acta Med Nagasaki. 59:19–25. 2014.
|
|
23
|
Gencer M, Ceylan E, Aksoy N and Uzun K:
Association of serum reactive oxygen metabolite levels with
different histopathological types of lung cancer. Respiration.
73:520–524. 2006.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Suzuki Y, Imai K, Takai K, Hanai T,
Hayashi H, Naiki T, Nishigaki Y, Tomita E, Shimizu M and Moriwaki
H: Hepatocellular carcinoma patients with increased oxidative
stress levels are prone to recurrence after curative treatment: A
prospective case series study using the d-ROM test. J Cancer Res
Clin Oncol. 139:845–852. 2013.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Sasaki Y: Does oxidative stress
participate in the development of hepatocellular carcinoma? J
Gastroenterol. 41:1135–1148. 2006.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Inokuma T, Haraguchi M, Fujita F, Tajima Y
and Kanematsu T: Oxidative stress and tumor progression in
colorectal cancer. Hepatogastroenterology. 56:343–347.
2009.PubMed/NCBI
|
|
27
|
Hou D, Liu Z, Xu X, Liu Q, Zhang X, Kong
B, Wei JJ, Gong Y and Shao C: Increased oxidative stress mediates
the antitumor effect of PARP inhibition in ovarian cancer. Redox
Biol. 17:99–111. 2018.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Nojima J, Motoki Y, Tsuneoka H, Kuratsune
H, Matsui T, Yamamoto M, Yanagihara M, Hinoda Y and Ichihara K:
‘Oxidation stress index’ as a possible clinical marker for the
evaluation of non-Hodgkin lymphoma. Br J Haematol. 155:528–530.
2011.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Jaffe ES, Harris NL, Stein H and Vardiman
JW: World Health Organization classification of tumors, pathology
and genetics tumors of haematopoietic and lymphoid tissues. IARC
Press, Lyon, pp 109-236, 2001.
|
|
30
|
Sugiura T, Dohi Y, Takase H, Yamashita S,
Tanaka S and Kimura G: Increased reactive oxygen metabolites is
associated with cardiovascular risk factors and vascular
endothelial damage in middle-aged Japanese subjects. Vasc Health
Risk Manag. 7:475–482. 2011.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Kakita H, Hussein MH, Daoud GA, Kato T,
Murai H, Sugiura T, Mizuno K, Yamada Y, Ito T, Fukuda S, et al:
Total hydroperoxide and biological antioxidant potentials in a
neonatal sepsis model. Pediatr Res. 60:675–679. 2006.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Takagi T and Oguro M:
(2'-R)-4'-o-tetrahydropyranyladriamycin, a new anthracycline
derivative; its effectiveness in lymphoid malignancies. Cancer
Chemother Pharmacol. 20:151–154. 1987.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Miller AA and Salewski E: Prospects for
pirarubicin. Med Pediatr Oncol. 22:261–268. 1994.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Tsurumi H, Yamada T, Sawada M, Kasahara S,
Kanemura N, Kojima Y, Fukuno K, Hara T, Saio M, Takahashi T, et al:
Biweekly CHOP or THP-COP regimens in the treatment of newly
diagnosed aggressive non-Hodgkin's lymphoma. A comparison of
doxorubicin and pirarubicin: A randomized phase II study. J Cancer
Res Clin Oncol. 130:107–113. 2004.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Hara T, Tsurumi H, Goto N, Kitagawa J,
Kanemura N, Yoshikawa T, Kasahara S, Goto H, Fukuno K, Yamada T, et
al: Phase II study of Rituximab combined with THP-COP as first-line
therapy for patients younger than 70 years with diffuse large B
cell lymphoma. J Cancer Res Clin Oncol. 136:65–70. 2010.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Kasahara S, Hara T, Tsurumi H, Goto N,
Kitagawa J, Kanemura N, Yoshikawa T, Goto H, Fukuno K, Yamada T, et
al: Phase II study of the tetrahydropyranyl
adriamycin-cyclophosphamide, vincristine, and prednisolone regimen
combined with rituximab as first-line treatment for elderly
patients with diffuse large B-cell lymphoma. Leuk Lymphoma.
52:629–634. 2011.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Hara T, Yoshikawa T, Goto H, Sawada M,
Yamada T, Fukuno K, Kasahara S, Shibata Y, Matsumoto T, Mabuchi R,
et al: R-THP-COP versus R-CHOP in patients younger than 70 years
with untreated diffuse large B-cell lymphoma: A randomized,
open-label, non-inferiority phase 3 trial. Hematol Oncol.
36:638–644. 2018.PubMed/NCBI View
Article : Google Scholar
|
|
38
|
Sawada M, Tsurumi H, Yamada T, Hara T,
Fukuno K, Goto H, Shimizu M, Kasahara S, Yoshikawa T, Kanemura N,
et al: A prospective study of P-IMVP-16/CBDCA: A novel salvage
chemotherapy for patients with aggressive non-Hodgkin's lymphoma
who had previously received CHOP therapy as first-line
chemotherapy. Eur J Haematol. 68:354–361. 2002.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Matsumoto T, Hara T, Shibata Y, Nakamura
N, Nakamura H, Ninomiya S, Kitagawa J, Kanemura N, Goto N, Kito Y,
et al: A salvage chemotherapy of R-P-IMVP16/CBDCA consisting of
rituximab, methylprednisolone, ifosfamide, methotrexate, etoposide,
and carboplatin for patients with diffuse large B cell lymphoma who
had previously received R-CHOP therapy as first-line chemotherapy.
Hematol Oncol. 35:288–295. 2017.PubMed/NCBI View
Article : Google Scholar
|
|
40
|
Cheson BD, Pfistner B, Juweid ME, Gascoyne
RD, Specht L, Horning SJ, Coiffier B, Fisher RI, Hagenbeek A, Zucca
E, et al: Revised response criteria for malignant lymphoma. J Clin
Oncol. 25:579–586. 2007.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Kaplan EL and Meier P: Nonparametric
estimation from incomplete observations. J Am Stat Assoc.
53:457–481. 1958.
|
|
42
|
Valko M, Leibfritz D, Moncol J, Cronin MT,
Mazur M and Telser J: Free radicals and antioxidants in normal
physiological functions and human disease. Int J Biochem Cell Biol.
39:44–84. 2007.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Bjelland S and Seeberg E: Mutagenicity,
toxicity and repair of DNA base damage induced by oxidation. Mutat
Res. 531:37–80. 2003.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Kryston TB, Georgiev AB, Pissis P and
Georgakilas AG: Role of oxidative stress and DNA damage in human
carcinogenesis. Mutat Res. 711:193–201. 2011.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Schöttker B, Saum KU, Jansen EH, Boffetta
P, Trichopoulou A, Holleczek B, Dieffenbach AK and Brenner H:
Oxidative stress markers and all-cause mortality at older age: A
population-based cohort study. J Gerontol A Biol Sci Med Sci.
70:518–524. 2015.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Schöttker B, Brenner H, Jansen EH,
Gardiner J, Peasey A, Kubínová R, Pająk A, Topor-Madry R,
Tamosiunas A, Saum KU, et al: Evidence for the free
radical/oxidative stress theory of ageing from the CHANCES
consortium: A meta-analysis of individual participant data. BMC
Med. 13(300)2015.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Lan Q, Zheng T, Shen M, Zhang Y, Wang SS,
Zahm SH, Holford TR, Leaderer B, Boyle P and Chanock S: Genetic
polymorphisms in the oxidative stress pathway and susceptibility to
non-Hodgkin lymphoma. Hum Genet. 121:161–168. 2007.PubMed/NCBI View Article : Google Scholar
|