Introduction
Eribulin, a synthetic analog of halichondrin B and
non-taxane microtubule dynamics inhibitor (1), is a U.S. Food and Drug
Administration-approved drug with proven clinical efficacy and
acceptable adverse events in patients with metastatic breast cancer
(MBC) (2-4).
MBC has numerous treatment options, but treatment
selection can be challenging because patient response can vary for
the same treatment. In the treatment of MBC, for prolonging the
overall response and progression-free survival (PFS), patient
groups showing efficacy can be identified; however, clear
indicators to identify patient groups with prolonged overall
survival (OS) among those with MBC undergoing eribulin therapy are
lacking. Various studies have been conducted to identify predictors
of eribulin efficacy in patients with MBC. Higher
neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte
ratio (PLR) have been reported to be associated with higher
mortality in several cancer types (5-8).
High absolute lymphocyte count (ALC), PLR and low NLR are
predictors of survival in patients with BC treated with eribulin
(9-12).
However, the global phase 3 EMBRACE trial suggested that NLR is a
general prognostic factor for improved OS, and ALC is an
independent predictor of OS, in eribulin-treated patients (10). However, the association between
peripheral immune status and MBC prognosis is controversial.
Liver function is assessed according to the
Child-Pugh (C-P) system. This system was originally developed to
predict the prognosis of patients being treated for portal
hypertension and variceal bleeding associated with cirrhosis
(13,14). However, the C-P classification is
not statistically constructed owing to concerns regarding
subjective and confounding factors, such as hepatic coma, ascites
and albumin (Alb). Previously, a new liver function assessment
tool, Alb-bilirubin (ALBI) grading, consisting only of Alb and
total bilirubin (TBil), has been proposed (15,16).
Compared with the C-P score, the ALBI score is a more appropriate
assessment as it only uses objective parameters (Alb and TBil).
In the present study, the relative effect of NLR and
PLR on survival was quantified in patients with recurrent/stage IV
BC and the clinical significance of NLR, PLR and other
clinicopathologic factors (including liver and kidney function
tests) on the prognostic value was evaluated.
Materials and methods
Patients
In the present study, 156 patients with
recurrent/stage IV BC disease who received eribulin monotherapy as
any treatment line at Saitama Medical University International
Medical Center, from April 2011 to March 2021, were enrolled. In
all patients, metastases were confirmed through diagnostic
radiography using computed tomography, whole-body bone
scintigraphy, or 2-[(18)F]-fluoro-2-deoxy-D-glucose positron
emission tomography. Patients with any type of simultaneous
metastatic cancer were excluded. Clinicopathological factors and
clinical outcome data were retrospectively extracted from the
medical records. Patients received eribulin at a dose of 1.4
mg/m2 on days one and eight of a 21-day cycle. The dose
was reduced, or the treatment postponed when toxicity developed,
and treatment cessation was decided based on confirmed disease
progression or intolerable toxicity.
Histological assessment
For the pathological examination of the tumors, the
surgically resected specimens were fixed in 10% formalin. The
tissues were embedded on paraffin wax blocks. The paraffin blocks
were cut to 3-4 µm sections for hematoxylin-eosin (H&E) and
immunohistochemical staining at room temperature. To determine the
histologic tumor type, H&E staining of sections of the tumor
specimens was performed. The expression statuses of estrogen
receptors (ER), progesterone receptors (PR), human epidermal growth
factor type 2 (HER2), and Ki67 labeling Index were assessed by
immunohistochemical staining. The following monoclonal antibodies
were used for immunohistochemistry: ER (SP1; cat. no. 790-4324,
prediluted); PR (1E2; cat. no. 790-2223, prediluted), HER2 (4B5;
cat. no. 790-2991, prediluted, all from Roche Tissue Diagnostics;
Roche Diagnostics, Ltd.) and Ki-67 (MIB-1; cat. no. M7240,
ready-to-use; Dako; Agilent Technologies, Inc.). Images were
captured using a light microscope (Olympus Corporation). According
to ASCO/CAP guideline (17), ER
and PgR positivity was determined when ≥1% of the nuclei in the
tumor were stained using immunohistochemistry. According to
ASCO/CAP guideline (18-20),
HER2 positivity was defined as an immunohistochemical score of 3+
or a positive result on fluorescence in situ hybridization.
According to the expression of ER, PR, HER2 and Ki67, patients were
divided into the triple-negative (TN) or non-TN groups, including
Luminal A or B, Luminal HER2 and HER2 types.
Blood sampling and evaluation of
predictive factors
On the same day or just before the start of the
first cycle of eribulin administration, whole blood samples and
baseline data for blood-based parameters were obtained. The cutoff
values for the baseline ALC, NLR, and PLR were set at 1,500/µl
(10,11), 3.0 (9,10,21)
and 150 (22,23), respectively.
ALBI grading was used to assess the liver function,
with ALBI scores and ALBI grades defined as follows: [log10
bilirubin (µmol/l) x 0.66] + [Alb (g/l) x (-)0.085] (grades 1, 2,
3=≤-2.60, >-2.60 to -1.39, and >-1.39, respectively)
(14).
Statistical analysis
Unless otherwise noted, data are presented as
percentage (%) or the mean. The relationship between OS and all
clinical factors was evaluated using univariate Cox proportional
hazards regression models. Candidate predictors with P<0.05 in
the univariate analysis were included in the multivariate
analysis.
OS for each group was calculated from the date of
the start of the first cycle of eribulin administration to the date
of death from any cause or the date of the last follow-up. OS was
calculated using the Kaplan-Meier method, and patient subgroups
were compared using the log-rank test. All statistical analyses
were performed using EZR version 1.52 (Saitama Medical Center,
Jichi Medical University, Saitama, Japan) (24), which is a graphical user interface
for R version 3.1.2 (The R Foundation for Statistical Computing,
Vienna, Austria). More precisely, it is a modified version of the R
commander designed to add statistical functions frequently used in
biostatistics.
Results
Characteristics of patients and
tumors
The clinicopathological characteristics of the 156
patients included in the present study are Listed in Table I. Tumors were mainly ductal (87.8%)
or lobular (5.7%) invasive carcinomas, while 41 (26.3%) were those
of TN disease. At the time of eribulin administration, 127 patients
(81.4%) had visceral metastases, of which 98 (62.8%) had liver
metastases. The mean time from confirmation of metastasis to start
of eribulin administration, mean time to treatment failure of
eribulin, and median follow-up duration for the 156 patients were
24.0, 6.0 and 18.3 months, respectively (Table II). Of the patients treated with
eribulin, 44.23% ultimately received a reduced dose (Table II). Tumor subtypes were classified
as TN (ER, PR, HER2-negative) and non-TN, including luminal
(ER-positive, PR-positive, HER2-negative); luminal HER2
(ER-positive, PR-PR-positive or negative, HER2-positive), and HER2
(ER-negative, PR-negative, HER2-positive) types, with proportions
of 26.3 and 73.7%, respectively (Table
I).
 | Table IPatient characteristics. |
Table I
Patient characteristics.
| Variable | Total number
(n=156) | Percentage, % |
|---|
| Median age, years
(range) | 57.1 (29-84) | |
|
<70 | 132 | 84.6 |
|
>70 | 24 | 15.4 |
| Histology | | |
|
aIDC | 137 | 87.8 |
|
bILC | 9 | 5.7 |
|
Others | 10 | 6.4 |
| Viceral
metastases | 127 | 81.4 |
| Liver
metastases | 98 | 62.8 |
| cHER2 status | | |
|
Negative | 128 | 82.1 |
|
Positive | 26 | 16.7 |
|
Unknown | 2 | 1.3 |
| dER status | | |
|
Negative | 55 | 35.3 |
|
Positive | 101 | 64.7 |
| ePR status | | |
|
Negative | 97 | 62.2 |
|
Positive | 59 | 37.8 |
| Triple (HER2/ER/PR)
negative | 41 | 26.3 |
| Mean of baseline
fWBC, µl (range) | 5,770
(2,550-13,100) | |
| Mean of baseline
gANC, µl (range) | 3,776
(1,238-10,461) | |
| Mean of baseline
hHb, g/dl
(range) | 12.1
(7.4-16.0) | |
|
<10 | 15 | 9.6 |
|
>10 | 141 | 90.4 |
| Mean of baseline
platelet, µl (range) | 255,000
(82,000-653,000) | |
| Mean of baseline
iALC, µl (range) | 1434
(439-6,255) | |
|
<1,500 | 94 | 60.3 |
|
>1,500 | 62 | 39.7 |
| jNLRs | 3.0 | |
|
<3.0 | 102 | 65.4 |
|
>3.0 | 54 | 34.6 |
| kPLRs | 204.4 | |
|
<150 | 59 | 37.8 |
|
>150 | 97 | 62.2 |
| lALBI grade | | |
|
1 | 49 | 31.4 |
|
2, 3 | 40 | 25.6 |
|
N/A | 67 | 42.9 |
| meGFR | | |
|
<60 | 13 | 8.3 |
|
>60 | 135 | 86.5 |
| nCRP | | |
|
<0.3 | 49 | 31.4 |
|
>0.3 | 40 | 25.6 |
|
oN/A | 67 | 42.9 |
| Table IIEribulin administration. |
Table II
Eribulin administration.
| Variable | Total number
(n=156) | Percentage,% |
|---|
| Median follow-up
time | 18.3
(1.6-76.1) | |
| Time to eribulin
administration for aMBC | 24.0 (0-114) | |
| Time to treatment
failure | 6.0 (1-68) | |
| Eribulin dose
reduction level | | |
|
0 | 87 | 55.77 |
|
-1 | 53 | 33.97 |
|
-2 | 16 | 10.26 |
Prognostic factors
As demonstrated in Table III, before eribulin
administration, OS was not affected by age, subtype, or renal
function decline, but patients with anemia (hemoglobin (Hb) <10
g/dl or liver dysfunction (ALBI grade 2 or 3) had significantly
shorter OS than those without it (P<0.001, respectively).
| Table IIIUnivariate and multivariate analyses
for the overall survival. |
Table III
Univariate and multivariate analyses
for the overall survival.
| | Univariate
analysis | Multivariate
analysis |
|---|
| Variable | | aHR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age | <70 | 1.144
(0.6474-2.023) | 0.6425 | | |
| Liver
metastases | Positive | 1.342
(0.8895-2.026) | 0.168 | | |
| bER status | Negative | 1.224
(0.8137-1.841) | 0.332 | | |
| cHER2 status | Positive | 0.6051
(0.3369-1.087) | 0.0927 | | |
| Subtype | dTN | 1.202
(0.7716-1872) | 0.416 | | |
| eALBI grade | 2, 3 | 2.575
(1.589-4.784) | <0.001 | 2.895
(1.602-5.234) | <0.001 |
| feGFR | <60 | 1.359
(0.7231-2.555) | 0.3406 | | |
| gHb | <10 | 4.029
(2.186-7.427) | <0.001 | 2.785
(1.329-5.836) | <0.01 |
| hCRP | Positive | 3.004
(1.971-4.578) | <0.001 | 1.629
(0.7797-3.403) | 0.19430 |
| iNLRs | >3.0 | 1.909
(1.28-2.847) | <0.01 | 1.311
(0.6768-2.538) | 0.42250 |
| jALC | <1,500 | 1.709
(1.133-2.578) | <0.05 | 1.020
(0.5063-2.055) | 0.95570 |
| kPLRs | >150 | 2.214
(1.443-3.396) | <0.001 | 2.124
(1.157-3.898) | <0.05 |
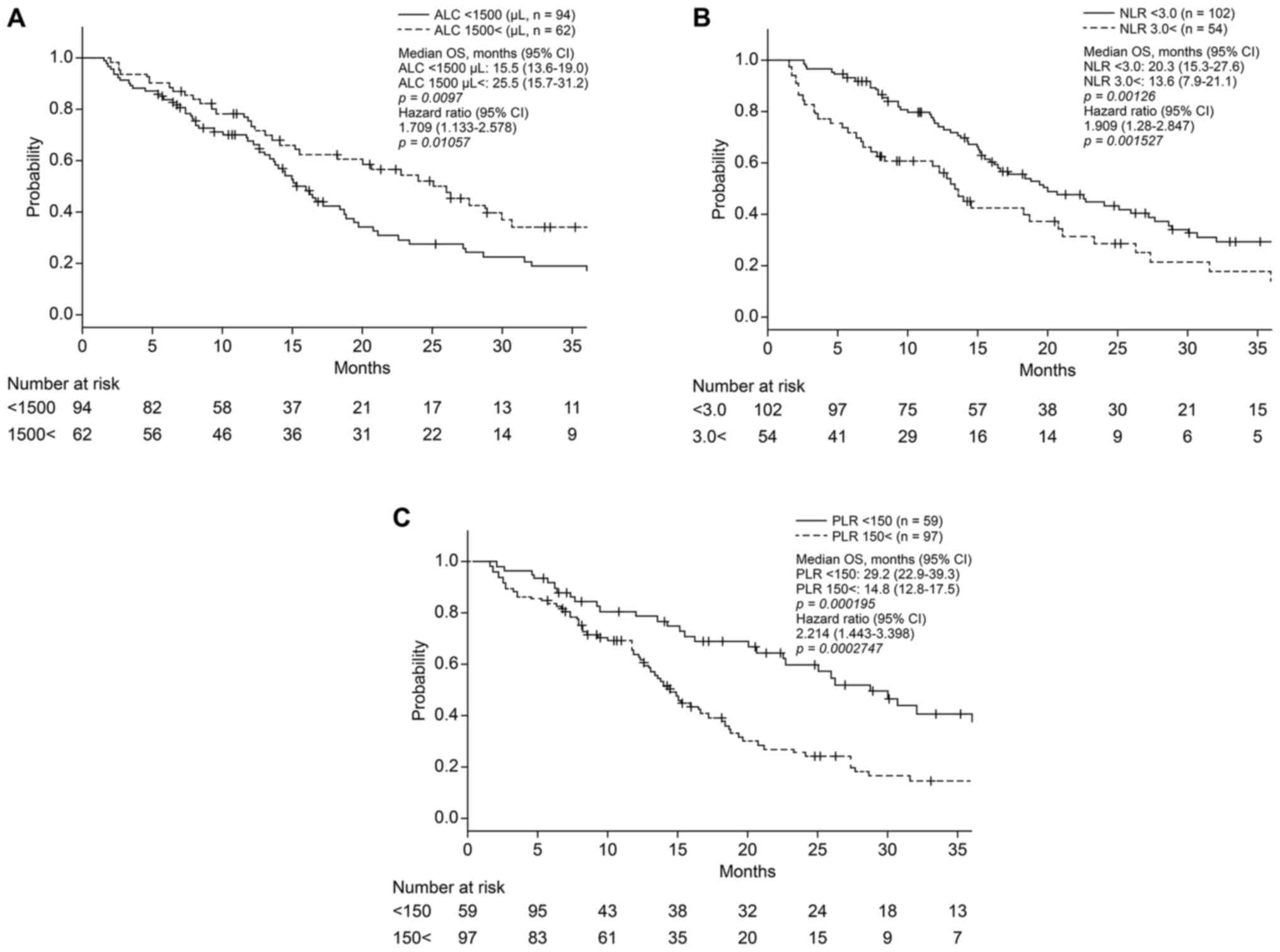
As revealed in Fig.
1A, before eribulin administration, patients with ALC
>1,500/µl had significantly longer OS than those with lower ALC
(median OS, 25.5 vs. 15.5 months; P<0.01). Patients with NLR
<3.0 and PLR <150 had significantly longer OS than those with
higher NLR and PLR [median OS, 20.3 vs. 13.6 months (P<0.01);
29.2 vs. 14.8 months (P<0.001); respectively] (Fig. 1B and C).
As shown in Table
III, there were no significant differences in OS based on age
and subtypes such as ER/HER2. Multivariate analysis demonstrated
that high ALBI grade (P<0.001) was an independent predictor of
shorter OS after eribulin treatment, regardless of the presence or
absence of liver metastases. Furthermore, high Hb (P<0.01), and
low PLRs (P<0.05) were independent factors that predicted longer
OS after eribulin administration (Table III).
Discussion
While it has become clear that the tumor
microenvironment significantly affects cancer cells and contributes
to the formation of cancer-specific properties (25-27),
it is interesting to examine its impact on the systemic immune
environment. In the present retrospective study, the baseline
blood-based clinical parameters were evaluated and PLR as a
predictor of OS in patients with MBC treated with eribulin was
confirmed. Additionally, high degrees of anemia (Hb <10 g/dl)
and liver dysfunction (ALBI grade 2 or 3) were significantly
associated with impaired OS in patients with MBC treated with
eribulin. The present study is the first one, to the best of the
authors' knowledge, to have comprehensively analyzed the peripheral
blood parameters and ratios in patients with MBC treated with
eribulin and revealed relevant predictors of OS. Predictors related
to systemic immune response and hepatic reserve in the treatment of
BC have not been considered in clinical practice.
Eribulin induces the remodeling of the tumor
vasculature and reoxygenation in patients with advanced BC and
decreases the levels of transforming growth factor-beta (TGF-β),
which is typically associated with hypoxic conditions (28). A retrospective analysis reported
decreased expression of programmed cell death-1 (PD-1), programmed
cell death ligand-1 (PD-L1), and forkhead box P3 (FoxP3) and
increased infiltrating CD8+ T cell levels in eribulin
responders (29). As PD-L1, FoxP3
and TGF-β have potent immunosuppressive effects, eribulin may have
exerted an immunomodulatory effect mediated through vascular
remodeling. Therefore, the analysis of the present study focused on
peripheral immunological biomarkers and organ reserve associated
with the efficacy of eribulin.
MBC treatment aims to maintain quality of life and
prolong OS, unlike numerous drugs that only prolong PFS. In a post
hoc analysis using the EMBRACE trial data (10), a high ALC (≥1,500/µl) was a
significant and independent predictor of prolonged OS in patients
treated with eribulin but not in those receiving a different
treatment of physician's choice, suggesting that NLRs may not be a
specific predictor of OS for eribulin but a general prognostic
factor. The present results suggested that a high PLR (≥150) is a
stronger prognostic factor for TN and non-TN BC than NLR and ALC,
which are characteristic of TNBC. However, this finding does not
imply that a high PLR (≥150) is a significant and independent
predictor of shorter OS during eribulin treatment (data not
shown).
Liver metastasis reduces the response rate and
worsens the prognosis of patients who receive immune-checkpoint
inhibitor therapy (30-32),
partly because lactic acid induces PD-1 expression by Treg cells in
liver metastatic lesions (33).
Liver tumors induce the loss of systemic tumor-specific effector T
cells by activation of Treg cells and/or hepatic macrophages
(34,35). There is evidence that as a
biomarker, ALBI grade can be used to optimize patient selection and
treatment planning in hepatocellular carcinoma (HCC) (36). In particular, changes in ALBI grade
after hepatic resection are independently associated with decreased
OS and recurrence-free survival (37). In the present study, the hepatic
reserve capacity due to liver metastasis and drug-induced liver
injury from previous line treatment in BC by ALBI grade was
evaluated, and it was demonstrated that liver dysfunction (ALBI
grade 2 or 3) affects the OS. Liu et al (38) revealed that the PALBI grade, which
incorporates platelet counts as an indicator of the severity of
portal hypertension into the ALBI grade, could be more clinically
feasible because of its superior prognostic power in HCC compared
with the ALBI grade. In HCC, the effect of reduced platelet counts
associated with portal hypertension should be considered but in the
present study, a high PLR (≥150) may have been an independent
prognostic factor that reflected a stronger immune response.
However, the interpretation of the present study is limited by the
fact that it is retrospective and that there were missing values in
the ALBI score data.
In conclusion, blood-based parameters and ratios are
easily calculated and are feasible adjunctive tools to predict
prognosis, relapse rates and treatment efficacy in various types of
cancers (39-42).
In the present study, PLR and Hb were closely correlated with
prognosis in patients with MBC who received eribulin therapy. Thus,
low PLR and anemia may be useful surrogate markers for OS in
patients with MBC. Blood count parameters can be easily measured
without the need for new equipment or invasive testing. Further
prospective studies are needed to confirm these preliminary results
and to investigate the correlations between MBC characteristics or
subtypes and PLR.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author upon reasonable
request.
Authors' contributions
HS, AF, KM, SK, AN, YI, AA, MO, HI, AO and TS
provided the clinical data included in the text and confirm the
authenticity of all the raw data. HS, AF, and KM wrote the
manuscript draft. SK and MO contributed to the conception of the
work and interpreted and revised the laboratory test results
included in the present study. AO, HI, and TS revised the
manuscript critically and modified the text. All authors read and
approved the final version of the manuscript.
Ethics approval and consent to
participate
All procedures performed in the present study were
in accordance with the ethical standards of committee of Saitama
Medical University International Medical Center (approval no.
19-224; Hidaka, Japan) and/or national research committee and in
accordance with the 1964 Helsinki Declaration and its later
amendments or comparable ethical standards. The requirement of
informed consent was waived given the retrospective nature of the
study.
Patient consent for publication
Not applicable.
Competing interests
Toshiaki Saeki received research grants from Eisai
Co., Ltd.; Taiho Pharmaceutical Co., Ltd.; and Chugai
Pharmaceutical Co., Ltd., and received personal fees from Taiho
Pharmaceutical Co. and Chugai Pharmaceutical Co. Akihiko Osaki
received research grants from AstraZeneca K.K., Eisai Co., Ltd.,
MSD K.K., Ono Pharmaceutical Co., Ltd., Kyowa Hakko Kirin Co.,
Ltd., Daiichi Sankyo Co., Ltd., Taiho Pharmaceutical Co., Ltd.,
Sawai Pharmaceutical Co., Ltd., Chugai Pharmaceutical Co., Ltd.,
Nippon Kayaku Co., Ltd., Novartis Pharma K.K., Hamamatsu Photonics
K.K., Parexel International Inc., and Fuji Pharma Co. Akihiko Osaki
also received personal fees from AstraZeneca K.K., Kyowa Hakko
Kirin Co., Ltd, Daiichi Sankyo Co., Ltd, Chugai Pharmaceutical Co.,
Ltd., and Novartis Pharma K.K. The authors declare that they have
no competing interests.
References
|
1
|
Towle MJ, Salvato KA, Budrow J, Wels BF,
Kuznetsov G, Aalfs KK, Welsh S, Zheng W, Seletsky BM, Palme MH, et
al: In vitro and in vivo anticancer activities of synthetic
macrocyclic ketone analogues of halichondrin B. Cancer Res.
61:1013–1021. 2001.PubMed/NCBI
|
|
2
|
Jain S and Vahdat LT: Eribulin mesylate.
Clin Cancer Res. 17:6615–6622. 2011.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Cortes J, O'Shaughnessy J, Loesch D, Blum
JL, Vahdat LT, Petrakova K, Chollet P, Manikas A, Diéras V,
Delozier T, et al: Eribulin monotherapy versus treatment of
physician's choice in patients with metastatic breast cancer
(EMBRACE): A phase 3 open-label randomised study. Lancet.
377:914–923. 2011.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Kaufman PA, Awada A, Twelves C, Yelle L,
Perez EA, Velikova G, Olivo MS, He Y, Dutcus CE and Cortes J: Phase
III open-label randomized study of eribulin mesylate versus
capecitabine in patients with locally advanced or metastatic breast
cancer previously treated with an anthracycline and a taxane. J
Clin Oncol. 33:594–601. 2015.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Yodying H, Matsuda A, Miyashita M,
Matsumoto S, Sakurazawa N, Yamada M and Uchida E: Prognostic
significance of neutrophil-to-lymphocyte ratio and
platelet-to-lymphocyte ratio in oncologic outcomes of esophageal
cancer: A systematic review and meta-analysis. Ann Surg Oncol.
23:646–654. 2016.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Tan D, Fu Y, Su Q and Wang H: Prognostic
role of platelet-lymphocyte ratio in colorectal cancer: A
systematic review and meta-analysis. Med (Baltim).
95(e3837)2016.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Zheng J, Cai J, Li H, Zeng K, He L, Fu H,
Zhang J, Chen L, Yao J, Zhang Y and Yang Y: Neutrophil to
lymphocyte ratio and platelet to lymphocyte ratio as prognostic
predictors for hepatocellular carcinoma patients with various
treatments: A meta-analysis and systematic review. Cell Physiol
Biochem. 44:967–981. 2017.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Prodromidou A, Andreakos P, Kazakos C,
Vlachos DE, Perrea D and Pergialiotis V: The diagnostic efficacy of
platelet-to-lymphocyte ratio and neutrophil-to-lymphocyte ratio in
ovarian cancer. Inflamm Res. 66:467–475. 2017.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Miyagawa Y, Araki K, Bun A, Ozawa H,
Fujimoto Y, Higuchi T, Nishimukai A, Kira A, Imamura M and Miyoshi
Y: Significant association between low baseline
neutrophil-to-lymphocyte ratio and improved progression-free
survival of patients with locally advanced or metastatic breast
cancer treated with eribulin but not with nab-paclitaxel. Clin
Breast Cancer. 18:400–409. 2018.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Miyoshi Y, Yoshimura Y, Saito K, Muramoto
K, Sugawara M, Alexis K, Nomoto K, Nakamura S, Saeki T, Watanabe J,
et al: High absolute lymphocyte counts are associated with longer
overall survival in patients with metastatic breast cancer treated
with eribulin-but not with treatment of physician's choice-in the
EMBRACE study. Breast Cancer. 27:706–715. 2020.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Araki K, Ito Y, Fukada I, Kobayashi K,
Miyagawa Y, Imamura M, Kira A, Takatsuka Y, Egawa C, Suwa H, et al:
Predictive impact of absolute lymphocyte counts for
progression-free survival in human epidermal growth factor receptor
2-positive advanced breast cancer treated with pertuzumab and
trastuzumab plus eribulin or nab-paclitaxel. BMC Cancer.
18(982)2018.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Takamizawa S, Shimoi T, Satomi-Tsushita N,
Yazaki S, Okuya T, Kojima Y, Sumiyoshi-Okuma H, Nishikawa T,
Tanioka M, Sudo K, et al: Neutrophil-to-lymphocyte ratio as a
prognostic factor for patients with metastatic or recurrent breast
cancer treated using capecitabine: A retrospective study. BMC
Cancer. 22(64)2022.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Child CG and Turcotte JG: Surgery and
portal hypertension. Major Probl Clin Surg. 1:1–85. 1964.PubMed/NCBI
|
|
14
|
Pugh RN, Murray-Lyon IM, Dawson JL,
Pietroni MC and Williams R: Transection of the oesophagus for
bleeding oesophageal varices. Br J Surg. 60:646–649.
1973.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Johnson PJ, Berhane S, Kagebayashi C,
Satomura S, Teng M, Reeves HL, O'Beirne J, Fox R, Skowronska A,
Palmer D, et al: Assessment of liver function in patients with
hepatocellular carcinoma: A new evidence-based approach-the ALBI
grade. J Clin Oncol. 33:550–558. 2015.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Hiraoka A, Michitaka K, Kumada T, Izumi N,
Kadoya M, Kokudo N, Kubo S, Matsuyama Y, Nakashima O, Sakamoto M,
et al: Validation and potential of albumin-bilirubin grade and
prognostication in a nationwide survey of 46,681 hepatocellular
carcinoma patients in Japan: The need for a more detailed
evaluation of hepatic function. Liver Cancer. 6:325–336.
2017.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Allison KH, Hammond MEH, Dowsett M,
McKernin SE, Carey LA, Fitzgibbons PL, Hayes DF, Lakhani SR,
Chavez-MacGregor M, Perlmutter J, et al: Estrogen and progesterone
receptor testing in breast cancer: ASCO/CAP guideline update. J
Clin Oncol. 38:1346–1366. 2020.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Wolff AC, Hammond MEH, Allison KH, Harvey
BE, Mangu PB, Bartlett JMS, Bilous M, Ellis IO, Fitzgibbons P,
Hanna W, et al: Human epidermal growth factor receptor 2 testing in
breast cancer: American Society of Clinical Oncology/College of
American Pathologists clinical practice guideline focused update. J
Clin Oncol. 36:2105–2122. 2018.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Farshid G, Dhatrak D, Gilhotra A, Koszyca
B and Nolan J: The impact of 2018 ASCO-CAP HER2 testing guidelines
on breast cancer HER2 results. An audit of 2132 consecutive cases
evaluated by immunohistochemistry and in situ hybridization. Mod
Pathol. 33:1783–1790. 2020.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Li A, Bai Q, Kong H, Zhou S, Lv H, Zhong
S, Li M, Bi R, Zhou X and Yang W: Impact of the updated 2018
American Society of Clinical Oncology/College of American
Pathologists Guideline for Human Epidermal Growth Factor Receptor 2
Testing in Breast Cancer. Arch Pathol Lab Med. 144:1097–1107.
2020.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Asano Y, Kashiwagi S, Onoda N, Noda S,
Kawajiri H, Takashima T, Ohsawa M, Kitagawa S and Hirakawa K:
Predictive value of neutrophil/lymphocyte ratio for efficacy of
preoperative chemotherapy in triple-negative breast cancer. Ann
Surg Oncol. 23:1104–1110. 2016.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Asano Y, Kashiwagi S, Onoda N, Noda S,
Kawajiri H, Takashima T, Ohsawa M, Kitagawa S and Hirakawa K:
Platelet-lymphocyte ratio as a useful predictor of the therapeutic
effect of neoadjuvant chemotherapy in breast cancer. PLoS One.
11(e0153459)2016.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Cuello-López J, Fidalgo-Zapata A,
López-Agudelo L and Vásquez-Trespalacios E: Platelet-to-lymphocyte
ratio as a predictive factor of complete pathologic response to
neoadjuvant chemotherapy in breast cancer. PLoS One.
13(e0207224)2018.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Kanda Y: Investigation of the freely
available easy-to-use software ‘EZR’ for medical statistics. Bone
Marrow Transplant. 48:452–458. 2013.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Kim J and Bae JS: Tumor-associated
macrophages and neutrophils in tumor microenvironment. Mediators
Inflamm. 2016(6058147)2016.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Hinshaw DC and Shevde LA: The tumor
microenvironment innately modulates cancer progression. Cancer Res.
79:4557–4566. 2019.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Gysler SM and Drapkin R: Tumor
innervation: Peripheral nerves take control of the tumor
microenvironment. J Clin Invest. 131(e147276)2021.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Ueda S, Saeki T, Takeuchi H, Shigekawa T,
Yamane T, Kuji I and Osaki A: In vivo imaging of eribulin-induced
reoxygenation in advanced breast cancer patients: A comparison to
bevacizumab. Br J Cancer. 114:1212–1218. 2016.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Goto W, Kashiwagi S, Asano Y, Takada K,
Morisaki T, Fujita H, Takashima T, Ohsawa M, Hirakawa K and Ohira
M: Eribulin promotes antitumor immune responses in patients with
locally advanced or metastatic breast cancer. Anticancer Res.
38:2929–2938. 2018.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Halabi S, Kelly WK, Ma H, Zhou H, Solomon
NC, Fizazi K, Tangen CM, Rosenthal M, Petrylak DP, Hussain M, et
al: Meta-analysis evaluating the impact of site of metastasis on
overall survival in men with castration-resistant prostate cancer.
J Clin Oncol. 34:1652–1659. 2016.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Sasaki A, Nakamura Y, Mishima S, Kawazoe
A, Kuboki Y, Bando H, Kojima T, Doi T, Ohtsu A, Yoshino T, et al:
Predictive factors for hyperprogressive disease during nivolumab as
anti-PD1 treatment in patients with advanced gastric cancer.
Gastric Cancer. 22:793–802. 2019.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Topalian SL, Hodi FS, Brahmer JR,
Gettinger SN, Smith DC, McDermott DF, Powderly JD, Sosman JA,
Atkins MB, Leming PD, et al: Five-year survival and correlates
among patients with advanced melanoma, renal cell carcinoma, or
non-small cell lung cancer treated with nivolumab. JAMA Oncol.
5:1411–1420. 2019.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Kumagai S, Koyama S, Itahashi K,
Tanegashima T, Lin YT, Togashi Y, Kamada T, Irie T, Okumura G, Kono
H, et al: Lactic acid promotes PD-1 expression in regulatory T
cells in highly glycolytic tumor microenvironments. Cancer Cell.
40:201–218.e9. 2022.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Lee JC, Mehdizadeh S, Smith J, Young A,
Mufazalov IA, Mowery CT, Daud A and Bluestone JA: Regulatory T cell
control of systemic immunity and immunotherapy response in liver
metastasis. Sci Immunol. 5(eaba0759)2020.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Yu J, Green MD, Li S, Sun Y, Journey SN,
Choi JE, Rizvi SM, Qin A, Waninger JJ, Lang X, et al: Liver
metastasis restrains immunotherapy efficacy via macrophage-mediated
T cell elimination. Nat Med. 27:152–164. 2021.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Ye L, Liang R, Zhang J, Chen C, Chen X,
Zhang Y, Wang G, Yang Y and Chen G: Postoperative albumin-bilirubin
grade and albumin-bilirubin change predict the outcomes of
hepatocellular carcinoma after hepatectomy. Ann Transl Med.
7(367)2019.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Demirtas CO, D'Alessio A, Rimassa L,
Sharma R and Pinato DJ: ALBI grade: Evidence for an improved model
for liver functional estimation in patients with hepatocellular
carcinoma. JHEP Rep. 3(100347)2021.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Liu PH, Hsu CY, Hsia CY, Lee YH, Chiou YY,
Huang YH, Lee FY, Lin HC, Hou MC and Huo TI: ALBI and PALBI grade
predict survival for HCC across treatment modalities and BCLC
stages in the MELD Era. J Gastroenterol Hepatol. 32:879–886.
2017.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Zhang P, Zong Y, Liu M, Tai Y, Cao Y and
Hu C: Prediction of outcome in breast cancer patients using test
parameters from complete blood count. Mol Clin Oncol. 4:918–924.
2016.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Stotz M, Liegl-Atzwanger B, Posch F, Mrsic
E, Thalhammer M, Stojakovic T, Bezan A, Pichler M, Gerger A and
Szkandera J: Blood-based biomarkers are associated with disease
recurrence and survival in gastrointestinal stroma tumor patients
after surgical resection. PLoS One. 11(e0159448)2016.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Ying HQ, Deng QW, He BS, Pan YQ, Wang F,
Sun HL, Chen J, Liu X and Wang SK: The prognostic value of
preoperative NLR, d-NLR, PLR and LMR for predicting clinical
outcome in surgical colorectal cancer patients. Med Oncol.
31(305)2014.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Deng Q, He B, Liu X, Yue J, Ying H, Pan Y,
Sun H, Chen J, Wang F, Gao T, et al: Prognostic value of
pre-operative inflammatory response biomarkers in gastric cancer
patients and the construction of a predictive model. J Transl Med.
13(66)2015.PubMed/NCBI View Article : Google Scholar
|