Introduction
Uterine fibroids or leiomyomas are benign pelvic
masses, representing the most common gynecological condition to
date (1). There are three primary
types of uterine leiomyomas: Submucosal, intramural and subserosal
leiomyomas. Submucosal and subserosal leiomyomas may be attached to
the uterus via a vascular pedicle, known as pedunculated leiomyomas
(2). Depending on their location,
pedunculated uterine leiomyomas may protrude both within the
uterine cavity or extend outside it, into the vagina (as in the
case described herein). Alternatively, they may prolapse outside
the vagina or protrude into the peritoneal cavity, often posing a
serious challenge for differential diagnosis (3).
The case described in the present study emphasizes
the significant obstructive bilateral hydroureteronephrosis,
accompanied by severe renal dysfunction resulting from ureteral
compression by a large pedunculated submucosal uterine leiomyoma
that prolapsed into the vagina. Simultaneously, it highlights the
substantial challenges in differential diagnosis, particularly with
large intracervical leiomyomas, and emphasizes the imperative need
for early and effective surgical intervention to prevent permanent
damage of the renal parenchyma.
Case report
The present study describes the case of a
65-year-old menopausal patient, who presented to the Emergency
Department of the General Hospital of Trikala (Trikala, Greece)
with severe uterine bleeding persisting for 20 days, leading to
marked anemia. The blood tests of the patient upon admission to the
Department of Gynecology the General Hospital of Trikala are
presented in detail in Table I. The
patient had given birth to two children by vaginal delivery. From
the personal medical history of the patient, it was found that she
had no prior surgeries. Conditions, such as hypothyroidism
secondary to non-toxic multinodular goiter, chronic atrial
fibrillation, arterial hypertension and type II diabetes mellitus
were reported. These conditions were effectively managed with
medication. The patient reported no bowel disorders or weight loss.
Sporadic episodes of frequent urination, without accompanying
urinary tract infection, were mentioned by the patient.
Additionally, there was no history of chronic renal disease or
recurrent urinary tract infections in recent years.
 | Table IPre- and post-operative laboratory
test results of the patient with prolapsed pedunculated submucosal
leiomyoma of the uterus. |
Table I
Pre- and post-operative laboratory
test results of the patient with prolapsed pedunculated submucosal
leiomyoma of the uterus.
| Laboratory tests | Day of admission to
the clinic | 3rd day of
hospitalization | Post-operatively | 2nd Post-operative
day after laparotomy | 5th post-operative
day after laparotomy | 3 Months after
surgery | 6 Months after
surgery | Normal laboratory
values |
|---|
| Ht | 15.4% | 29% | 32.5% | 30.1% | 28.7% | 31.2% | 33.6% | 37.7-49.7% |
| Hb | 4.1 g/dl | 9.6 g/dl | 10.1 g/dl | 9.5 g/dl | 8.7 g/dl | 10.5 g/dl | 11.1 g/dl | 11.8-17.8 gr/dl |
| PLT |
483x103/ml |
327x103/ml |
400x103/ml |
357x103/ml |
382x103/ml |
257x103/ml |
241x103/ml |
150-350x103/ml |
| WBC |
17.3x103/ml |
11.9x103/ml |
9.7x103/ml |
11.3x103/ml |
7.4x103/ml |
8.9x103/ml |
8.5x103/ml |
4-10.8x103/ml |
| NEUT | 85.9% | 88.3% | 61% | 90.4% | 65.8% | 56.7% | 54% | 40-75% |
| CRP | 0.67 mg/dl | 0.51 mg/dl | | | | | | <0.7 mg/dl |
| APTT | 34.8 sec | 34.1 sec | 27.8 sec | | | | 29.3 sec | 24.0-35.0 sec |
| INR | 1.25 | 1.18 | 1.00 | | | | 1.01 | 0.8-1.2 |
| FIB | 316 mg/dl | 351 mg/dl | 498 mg/dl | | | | 358 mg/dl | 200-400 mg/dl |
| U | 64 mg/dl | 71 mg/dl | 61 mg/dl | 55 mg/dl | 41 mg/dl | 40 mg/dl | 37 mg/dl | 10-50 mg/dl |
| Cr | 1.74 mg/dl | 2.87 mg/dl | 1.95 mg/dl | 1.63 mg/dl | 1.28 mg/dl | 1.21 mg/dl | 1.1 mg/dl | 0.40-1.10 mg/dl |
| Κ+ | 3.7 mmol/l | 4.1 mmol/l | 4.8 mmol/l | 5.1 mmol/l | 4.5 mmol/l | 3.9 mmol/l | 3.7 mmol/l | 3.5-5.1 mmol/l |
| Να+ | 138 mmol/L | 141 mmol/l | 138.4 mmol/l | 134.4 mmol/l | 138.6 mmol/l | 138 mmol/l | 139.2 mmol/L | 136-145 mmol/l |
| B | 0.45 mg/dl | 0.85 mg/dl | 0.42 mg/dl | | | | 0.38 mg/dl | 0.3-1.2 mg/dl |
| AST | 32 IU/l | 37 IU/l | 29 IU/l | | | | 28 IU/l | 5-33 IU/l |
| 0ALT | 35 IU/l | 41 IU/l | 10 IU/l | | | | 25 IU/l | 10-37 IU/l |
Upon a gynecological examination and upon the
inspection of the vagina with a speculum, the cervix was not
visible. In the upper third of the vagina, in the anatomical
position of the cervix, a large solid mass was observed; the
position of the external cervical os could not be clearly
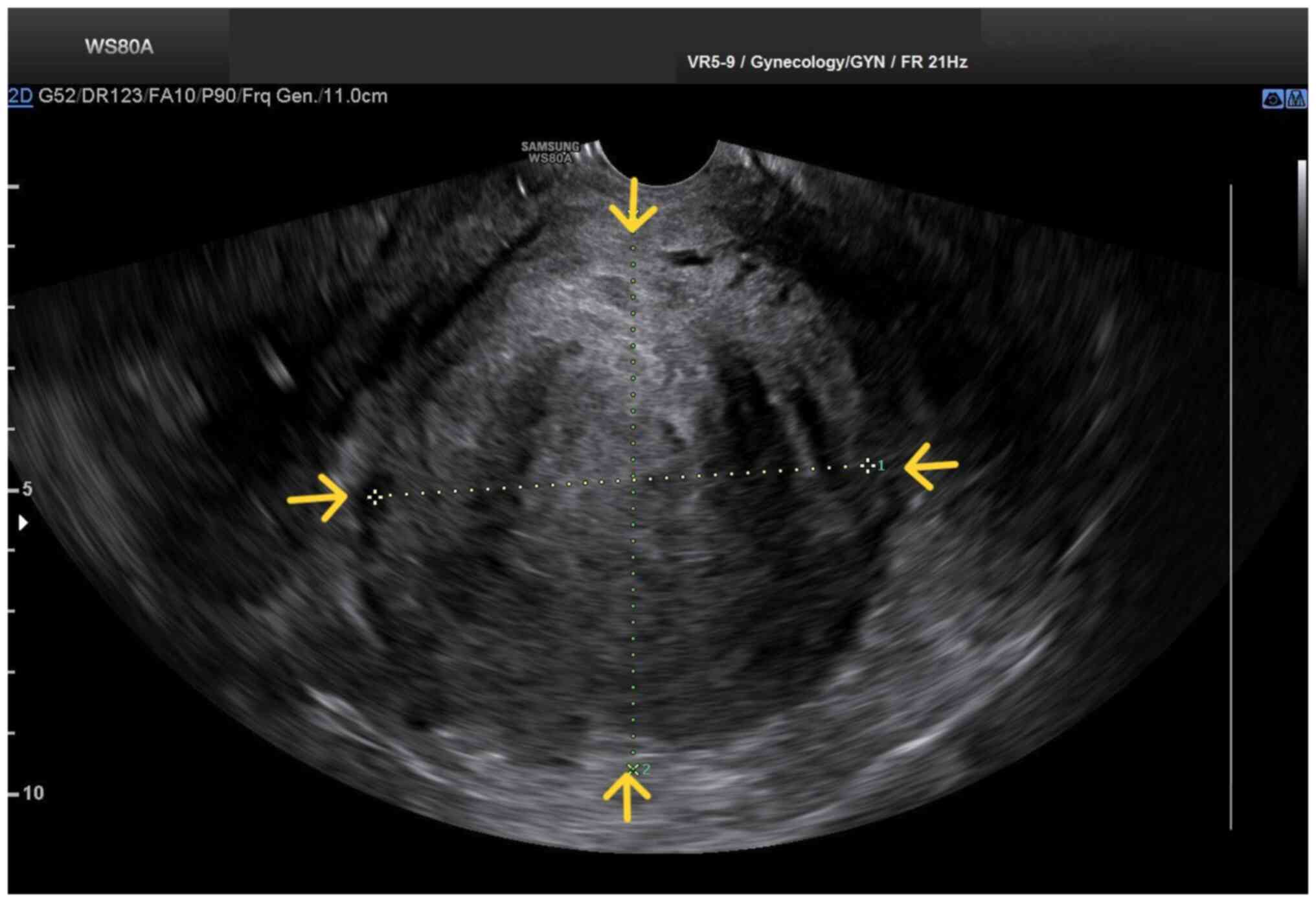
identified by visual inspection or palpation (Fig. 1). The transvaginal ultrasonographic
findings were inconclusive. The scan detected the presence of a
large well-circumscribed mass, with a maximum diameter of 10 cm, at
the anatomical position of the cervix, raising suspicion of an
intracervical leiomyoma (Fig. 2). A
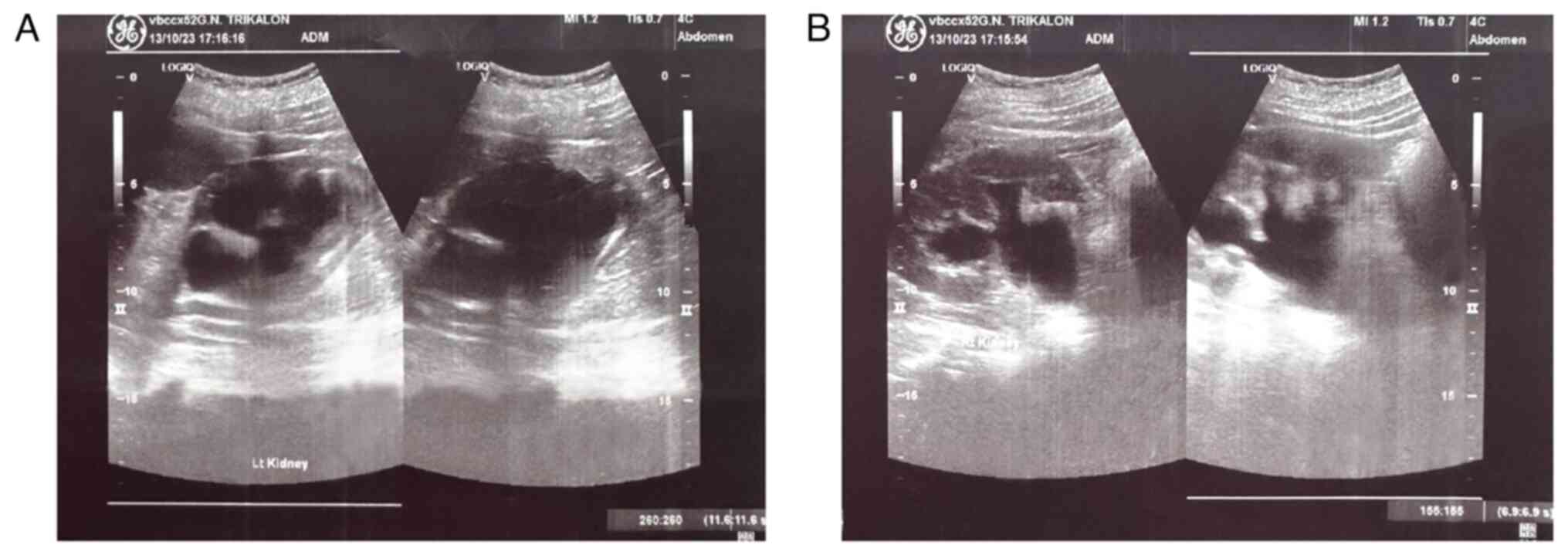
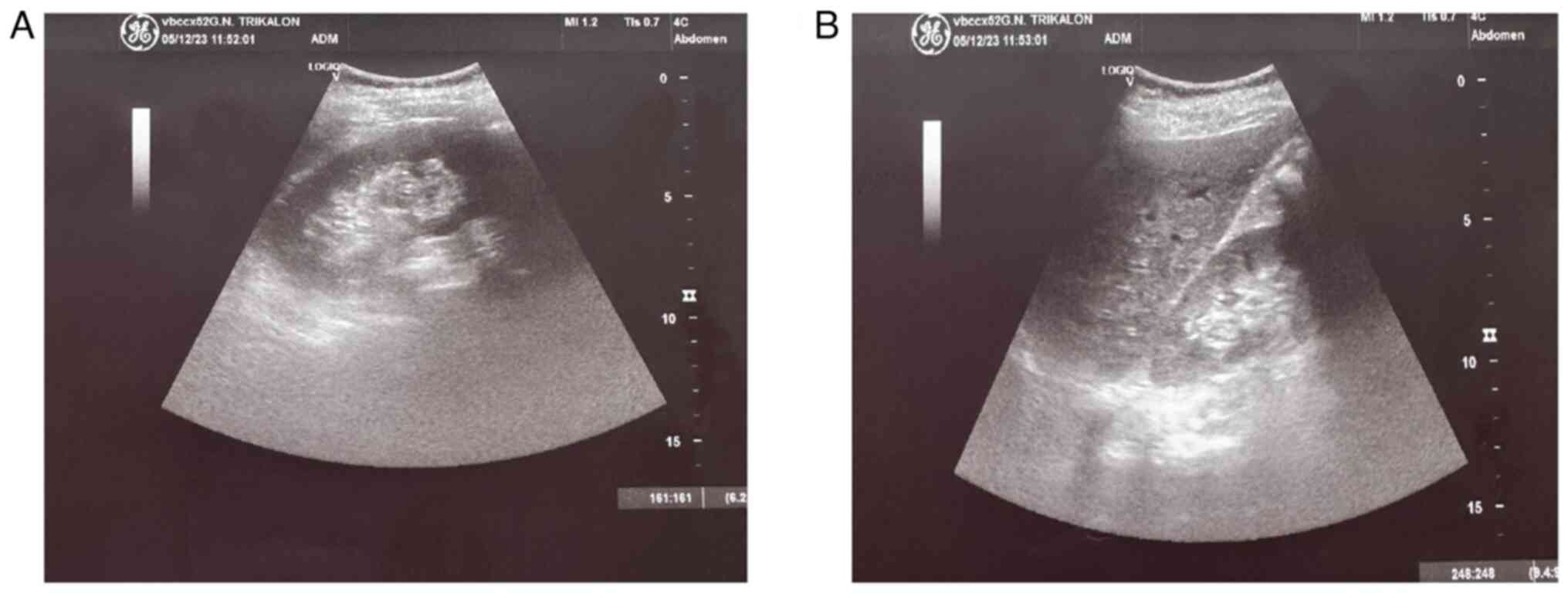
renal ultrasound revealed the bilateral dilatation of the
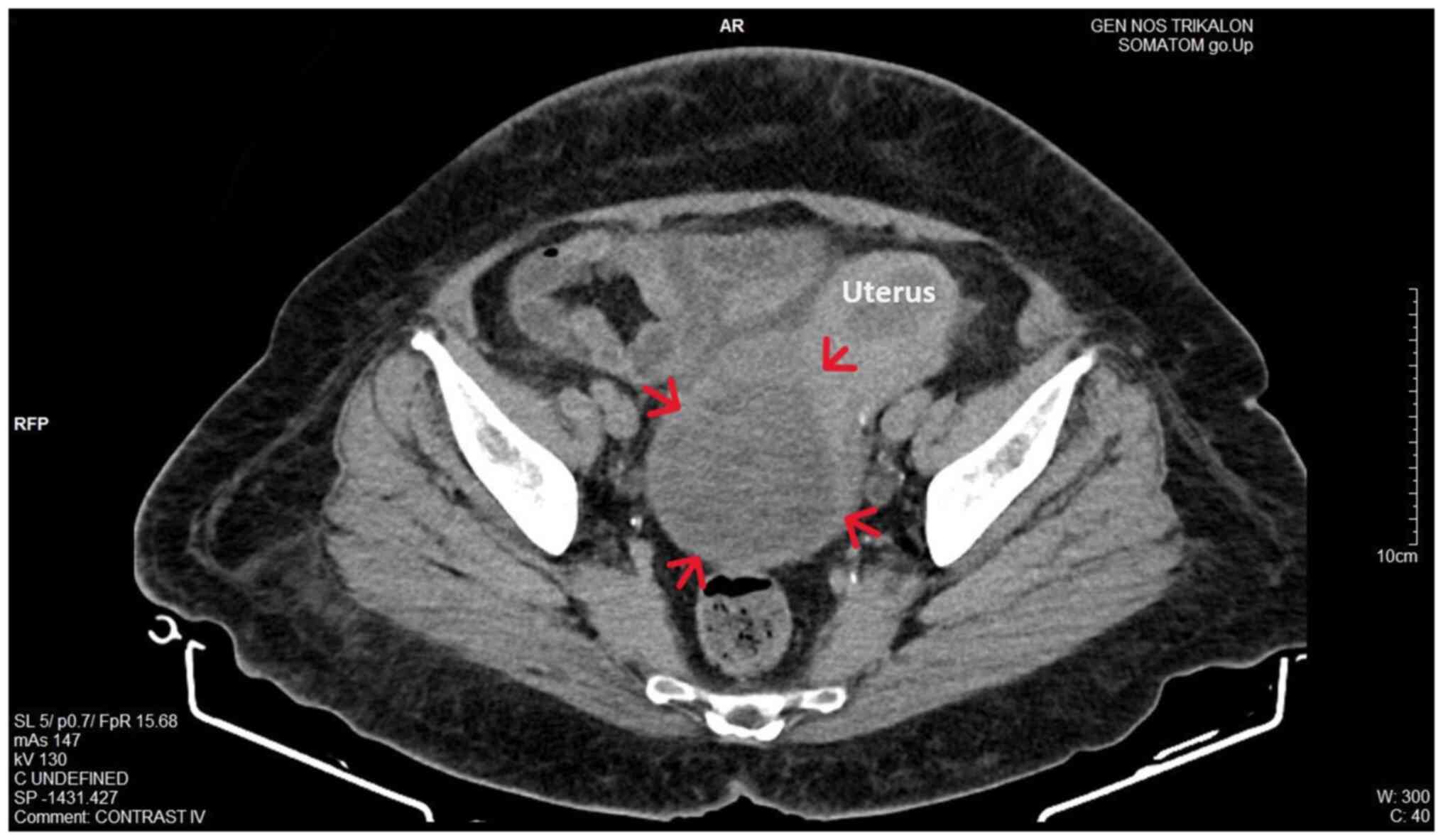
pelvicalyceal system and the ipsilateral proximal ureter (Fig. 3). Furthermore, a computed tomography
scan was performed, which revealed significant bladder dilatation
and internal non-homogeneity of the cervical canal throughout its
entire length, measuring 105x95x90 mm. This lesion caused the
thinning of the external wall of the cervix and anterior
displacement of the bladder. At the same time, it exerted
compression on the posterior wall of the bladder, and malignancy
arising from the cervix could not be excluded (Fig. 4). Additionally, computed tomography
confirmed the dilatation of the pelvicalyceal system bilaterally up
to the ureterovesical junction, accompanied by localized renal
cortical thinning and lobulated contour of the left kidney.
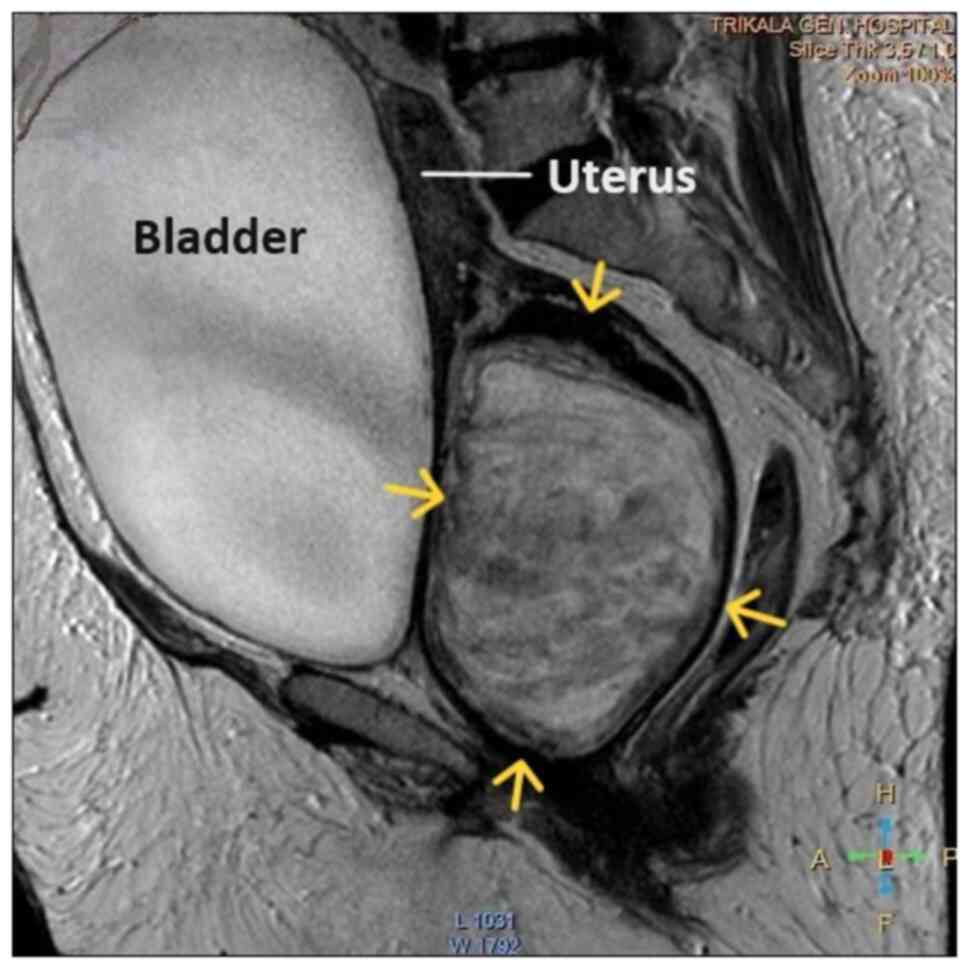
Magnetic resonance imaging was performed to further elucidate the
findings of computed tomography. Magnetic resonance imaging
revealed marked bladder distention with internal non-homogeneity of
the cervical canal and the presence of a lobulated lesion that
protruded intracanal with dimensions of 100x85x105 mm (Fig. 5). This finding was attributed to a
large intracervical leiomyoma, strongly ruling out the possibility
of cervical malignancy. The levels of tumor markers, namely
carcinoembryonic antigen, cancer antigen 125, cancer antigen 15-3
and cancer antigen 19-9 were within the normal range.
The initial conservative management of uterine
bleeding involved the administration of tranexamic acid (Transamin
at 500 mg/5 ml injectable solution by Help Pharmaceuticals), two
ampules in 0.9% NaCl solution infused intravenously three times a
day for 4 days, the treatment of anemia through transfusion with 4
units of packed red cells and the use of broad-spectrum
antibiotics, specifically cefoxitin (Mefoxil at 2 g/vial injectable
solution by Vianex Pharmaceutical Manufacturers) administered
intravenously every 8 h until the day of surgery. Due to the
deterioration of renal function following obstructive uropathy, a
ureteral stent was placed in the left ureter and a nephrostomy was
performed on the right kidney by the urologists. The placement of
the right nephrostomy was decided due to the unsuccessful access of
the ureteral stent to the right ureter. Following the urological
intervention, there was an improvement in renal function. The
variations of urea and creatinine values are detailed in Table I. Subsequently, following the
improvement of renal function and patient counseling, it was
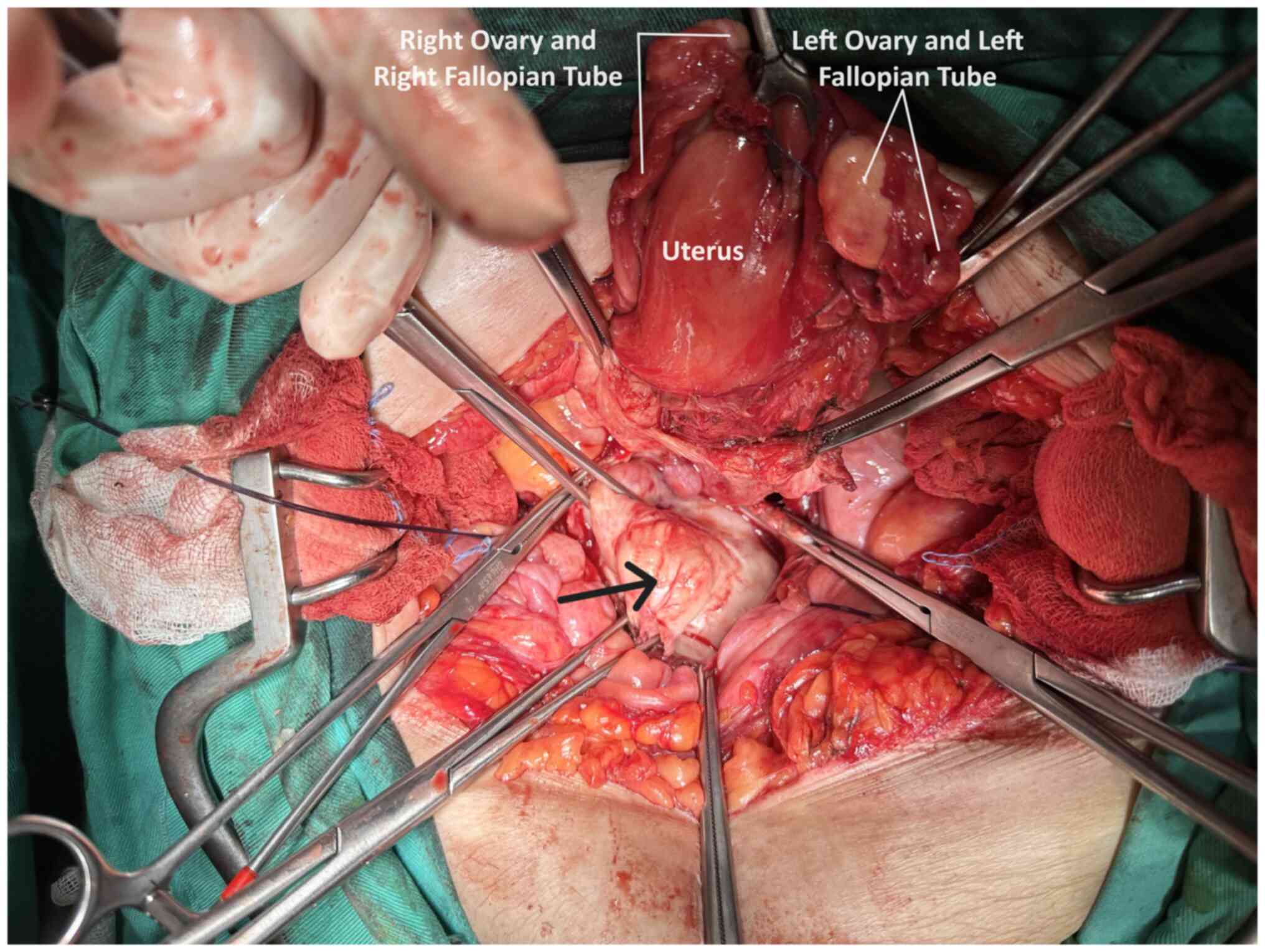
decided to perform an exploratory laparotomy. Intraoperatively,
normal uterus and adnexa were observed, and the presence of a large
pedunculated submucosal leiomyoma prolapsing into the vagina was
identified (Fig. 6). Following the
resection of the leiomyoma, an abdominal total hysterectomy with
bilateral salpingectomy-oophorectomy was performed. At the end of
the surgery, it was possible to place a ureteral stent in the right
ureter as well.
The collected specimens were sent for
histopathological analysis. This was carried out at the Anatomic
Pathology Laboratory of the General Hospital of Trikala. The
thickness of the obtained tissue sections was 5 µm and they were
paraffin-embedded. A buffered formalin 10% solution was used as the
fixative agent, for 36 h at room temperature. Hematoxylin and eosin
0.5% alcohol (Diachel A.E.) staining was used, at room temperature
with a 12-min duration. All microscopic examinations were performed
using a LEICA DM2000 optical microscope (Leica Microsystems GmbH).
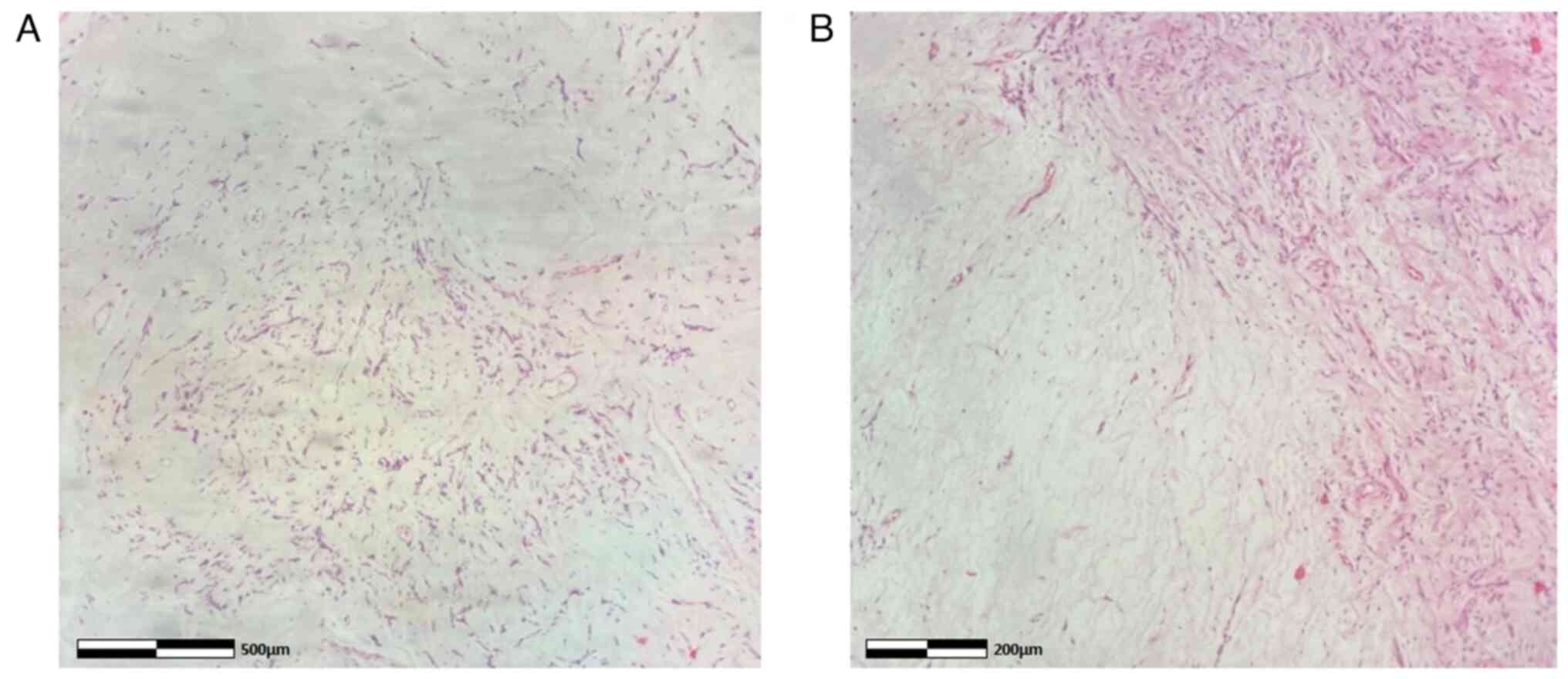
The histological examination of the surgical specimen confirmed the
diagnosis of pedunculated submucosal uterine leiomyoma (Fig. 7). Supplementary immunohistochemical
analysis was performed. The sections used were 4 µm in thickness,
were paraffin-embedded and they were dewaxed for 40 min at 70˚C.
Analysis was performed via the automated BOND-LEICA system (Leica
Biosystems). Sections were placed sequentially in BOND™ Dewax
solution, 100% v/v ethanol solution and BOND™ wash solution. For
antigen retrieval, BOND™ Epitope Retrieval ER2 Solution, HIER, was
used for cluster of differentiation 10 (CD10) and cytokeratin 7
(CK7) for 20 min in 100˚C, while ER1 solution (pH 7) for 20 min was
used for smooth muscle actin (SMA) and estrogen receptor (ER). The
block peroxide kit (Bond; Leica Biosystems) was used for 5 min. For
CD10 antibody, protein block solution was used for 20 min. As
regards primary antibody dilution this was: Dilution for CD10
(Menarini Hellas A.E.) ready-to-use antibody (cat. no. 44 217 CD10
RTU), for SMA (Zytomed Systems) ready-to-use (cat. no. 1A4
A00002-IFU-IVD-0002), for ER (Dako) 1:40 (cat. no. M3643) and for
CK7 (Dako) 1:100 with proprietary Leica (Bond; Leica Biosystems)
dilution agent. A duration of incubation of 30 min was used for all
antibodies. The post-primary kit was used for a duration of 10 min
at an incubation temperature of 100˚C. Subsequently, a secondary
detection kit polymer (Bond; Leica Biosystems) was used for a
duration of 10 min and the DAB kit (Bond; Leica Biosystems) for 10
min to facilitate visualization. Hematoxylin was applied for 5 min
as a counterstain at room temperature and the sections were
dehydrated, mounted and coverslipped. The resulting slides were
examined under a LEICA DM2000 optical microscope (Leica
Microsystems GmbH), at a magnification of x40, x100 and x400. The
specimen demonstrated strong diffuse positive staining for SMA and
ER, positive for CD10 and negative for cytokeratin 7 (CK7) (images
not available; data not shown).
Finally, the Alcian blue histochemical stain was
used. Sections of 4 µm in thickness were dewaxed for 40 min at a
temperature of 70˚C. The sections were placed in xylene for 10 min
in room temperature. Subsequently, they were hydrated in
decreasingly graded alcohols, submerged 10-15 times in each of the
following solutions: 100% v/v ethanol, 96% v/v ethanol, 80% v/v
ethanol and 70% v/v ethanol. Subsequently, the sections were washed
using tap water and then distilled water, finally being ready for
staining. A few drops of Alcian Blue stain [1% in 3% acetic acid
(pH 2.5); Atom Scientific] were added and left there for 30 min.
The sections were blotted and oxidized with 1% periodic acid
solution for 10 min and then washed, firstly for 5 min using tap
water and for 2 min using distilled water. Subsequently, Schiff
reagent solution was added for 20 min; the section was washed with
tap water for 5 min and rinsed with distilled water. Finally,
Mayer's hematoxylin (Atom Scientific) was added for 5 min, and the
section was washed in tap water for 5 min and rinsed in distilled
water and finally, it underwent hydration in increasingly graded
alcohols (same as before, in reverse), was mounted and
coverslipped. The slides were studied under the same optical
microscope (LEICA DM2000; magnification, x40, x100 and x400) as
aforementioned. Alcian blue staining of the specimen ultimately
revealed myxoid differentiation (images not available; data not
shown). The immunohistochemical analysis, along with histological
findings indicating no nuclear atypia, necrosis, mitoses, or
invasive pattern, strongly suggested a diagnosis of leiomyoma with
myxoid degeneration. These findings also supported the exclusion of
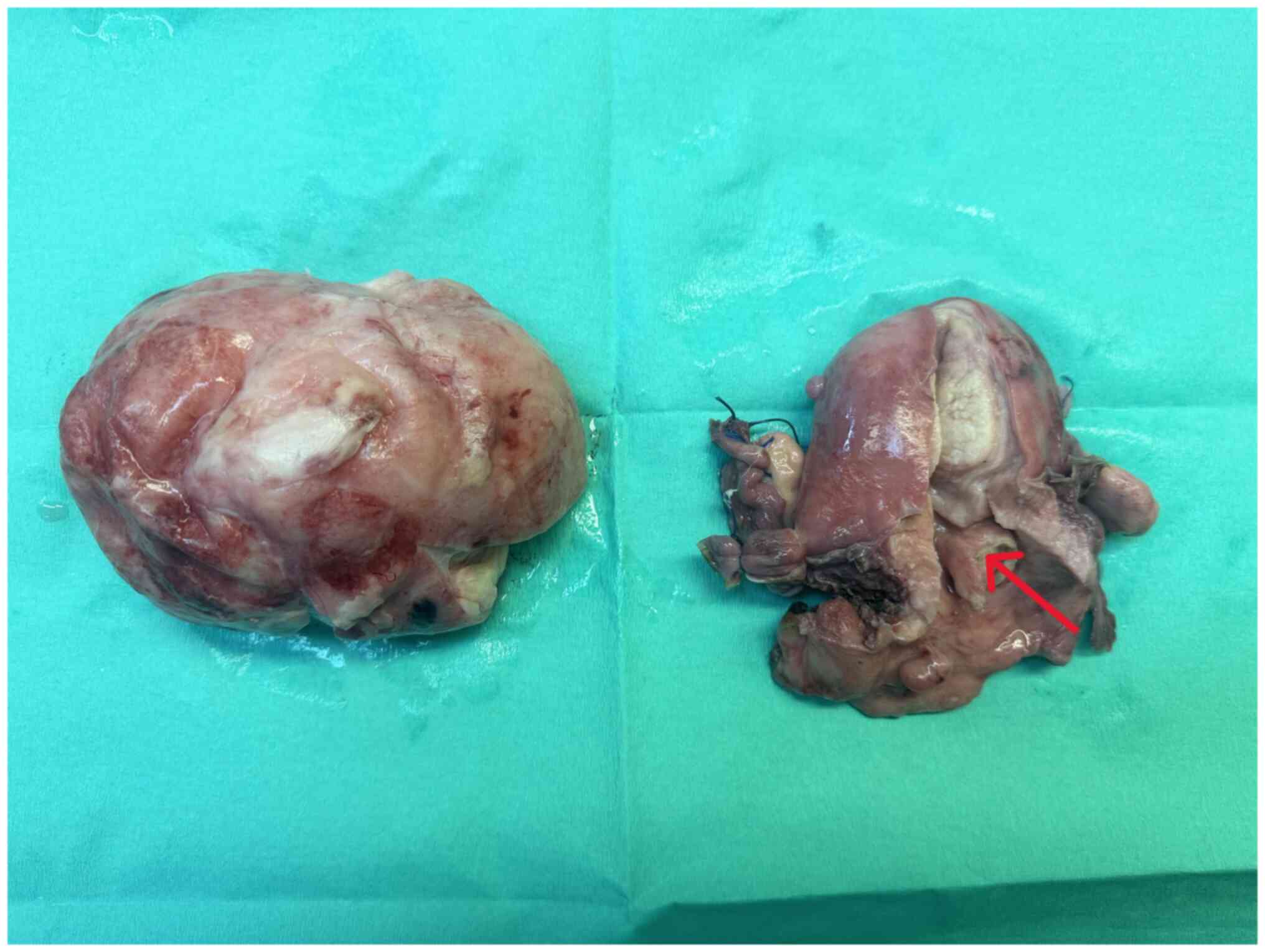
other tumors, such as leiomyosarcoma. Macroscopically, an
oval-shaped tumor with a maximum diameter of 10 cm exhibited a
smooth outer surface entirely covered by serosa and the presence of
a pedicle originating from the uterine isthmus was observed
(Fig. 8). Following a smooth
post-operative course and a distinct immediate improvement in renal
function (Table I), the patient was
discharged from the clinic on the 5th post-operative day. After 6
months, without the presence of ureteral stents, renal morphology
and function had fully recovered (Fig.
9). The serum creatinine level was 1.1 mg/dl. The patient
remains under regular follow-up evaluation at the Nephrology and
Gynecology outpatient Department of the General Hospital of
Trikala.
Discussion
Uterine fibroids are the most common benign
neoplasms of the uterus and a significant cause of morbidity among
women of reproductive age, affecting up to 68.6% of the female
population (4,5). Submucosal leiomyomas represent ~15-20%
of these cases (6). Prolapsed
uterine leiomyomas are pedunculated submucosal fibroids, which,
depending on the length of the vascular pedicle, can descend
through the cervical canal into the vagina or protrude outside the
vaginal opening (7). The exact
percentage of pedunculated submucosal leiomyomas that prolapse into
the vagina via the cervix is not precisely known. A previous study
reported that the estimated prevalence of prolapsed pedunculated
submucosal uterine leiomyomas was 2.5% among patients undergoing
surgery (8).
The clinical diagnosis of a prolapsed pedunculated
submucosal uterine leiomyoma within the vagina can be challenging,
particularly in cases where the leiomyoma is of A notable size and
has a short vascular pedicle. Prolapse of a pedunculated submucosal
leiomyoma through the cervix may either be asymptomatic or manifest
with symptoms, such as vaginal bleeding, vaginal discharge, or
pelvic pain (9). In the patient
described in the present study, the association of a prolapsed
pedunculated submucosal uterine leiomyoma with bilateral chronic
obstructive uropathy and renal dysfunction appears to be unique in
the English literature. Most likely, the large pedunculated
submucosal fibroid that prolapsed into the vagina, at the site of
the contiguity of the ureters with the upper segment of the vagina,
caused severe and chronic ureteral compression, resulting in
bilateral hydroureteronephrosis and renal dysfunction. In addition,
in the patient described herein, the diagnosis of a prolapsed
fibroid was challenging during gynecological examination.
Initially, it was incorrectly hypothesized that the cervix was not
visible due to its deformation by the large intracervical leiomyoma
and the compression exerted by the vaginal walls. In fact, however,
the solid mass observed upon the examination of the vagina with a
speculum (Fig. 1), was the prolapsed
leiomyoma and not the cervical wall thinned by the compression of
the tumor. Due to its large dimensions and a short vascular
pedicle, the prolapsed leiomyoma covered the entire upper third of
the vagina, hindering both visualization and palpation of the
cervix.
Consequently, it is considered that the diagnostic
analysis of patients with prolapsed pedunculated submucosal uterine
leiomyoma can be confusing, since the gynecological examination may
not be able to exclude uterine prolapse or uterine inversion
(7,10). Additionally, the elongation and
torsion of the vascular pedicle may lead to hemorrhagic and
gangrenous degeneration of the prolapsed submucosal leiomyoma,
posing a significant challenge in the differential diagnosis from
uterine leiomyosarcoma. Endometrial stromal tumor or giant
endometrial polyps should often be included in the differential
diagnosis of prolapsed pedunculated submucosal uterine leiomyoma
(11). Furthermore, bilateral
obstructive uropathy with renal dysfunction could more readily be
attributed to a large intracervical uterine leiomyoma than to a
prolapsed pedunculated submucosal leiomyoma in the upper third of
the vagina (12).
Imaging plays a crucial role in the pre-operative
diagnosis of patients with prolapsed pedunculated submucosal
leiomyoma. In these patients, computed tomography can distinctly
reveal a well-circumscribed pelvic mass with mixed echogenicity,
incorporating degenerative changes and necrotic lesions, thereby
facilitating an early and accurate diagnosis (13). Magnetic resonance imaging can also
provide critical imaging information regarding the precise location
of the leiomyoma in relation to the myometrium, the degree of
vascularization and the position of adjacent anatomical structures,
significantly contributing to the planning of optimal surgery
(14,15). In the patient in the present study,
however, the pre-operative imaging diagnosis of prolapsed
pedunculated submucosal uterine leiomyoma posed significant
challenges. None of the imaging modalities used (ultrasound,
computed tomography or magnetic resonance imaging) was able to
pre-operatively establish the diagnosis of prolapsed pedunculated
submucosal uterine leiomyoma. The ultrasound initially misdiagnosed
a large intracervical fibroid. Computed tomography confirmed the
ultrasound findings, but could not exclude the possibility of
cervical malignancy. Magnetic resonance imaging incorrectly
confirmed the diagnosis of intracervical fibroid and almost ruled
out the possibility of cervical malignancy.
The treatment of a prolapsed pedunculated submucosal
leiomyoma of the uterus is typically surgical (myomectomy or
abdominal total hysterectomy with bilateral
salpingectomy-oophorectomy). Factors, such as the desire for
fertility preservation, the absence of co-existing uterine
leiomyomas and the small size of the prolapsed submucosal leiomyoma
may favor the therapeutic option of vaginal myomectomy over
abdominal total hysterectomy with bilateral
salpingectomy-oophorectomy (16).
The absolute indication for abdominal total hysterectomy is severe
uterine bleeding, sepsis or an unsuccessful vaginal approach
(17). Vaginal myomectomy is
considered a safe and easy surgery for the treatment of prolapsed
pedunculated submucosal uterine leiomyoma, as it is associated with
a low recurrence rate and minimal morbidity (18,19).
Conversely, the increased risk of intraoperative hemorrhage that
may be associated with some pedunculated submucosal leiomyomas can
be controlled with hysteroscopy. Vaginal myomectomy followed by an
operative hysteroscopy to complete the resection of the leiomyoma's
residual vascular pedicle, following gentle cervical torsion around
the hysteroscope, which prevents the leakage of the distension
liquid, provides excellent visibility for hemorrhage control and
ensures the complete resection of the pedicle. This approach
significantly reduces the risk of recurrence (20).
In the patient described herein, the scarcity of
sufficient published data regarding the association between
prolapsed submucosal uterine leiomyoma and severe obstructive
uropathy with renal dysfunction was the main reason for both the
diagnostic and therapeutic challenges that were encountered.
Consequently, due to the pre-operative misdiagnosis of a
pedunculated submucosal uterine leiomyoma as an intracervical
fibroid, performing an exploratory laparotomy emerged as the only
treatment option for the patient. There was no option between
abdominal total hysterectomy with bilateral salpingo-oophorectomy
and vaginal myomectomy. The diagnosis of a prolapsed pedunculated
submucosal uterine leiomyoma in the patient described herein was
made intraoperatively, following the dissection of the anterior
vaginal wall and access into the vagina (Fig. 6). Nevertheless, it is noted that the
presence of a short and thick vascular pedicle originating from the
uterine isthmus, combined with the presence of a large leiomyoma
are conditions that may not ensure the success of a myomectomy via
vaginal approach.
There are certain possible limitations to the
present study that should be mentioned. The present study reports a
very rare case of a large pedunculated submucosal uterine leiomyoma
with prolapse into the vagina, which was associated with bilateral
obstructive uropathy and severe renal dysfunction. The extremely
rare manifestation of bilateral obstructive uropathy accompanied by
severe renal dysfunction that can be caused by prolapse of a large
pedunculated submucosal leiomyoma into the vagina created a serious
differential diagnostic challenge compared with intracervical
leiomyomas and led to misdiagnosis. It is considered that the
association of a prolapse of pedunculated submucosal uterine
leiomyoma with chronic bilateral obstructive uropathy and renal
dysfunction appears to be a unique clinical case in the English
literature. In addition, during the gynecological examination, the
prolapsed leiomyoma due to its large size and short vascular
pedicle did not allow either the inspection or palpation of the
cervix. Furthermore, the bilateral obstructive uropathy with renal
dysfunction that presented in the patient could more easily be
attributed to a large intracervical uterine leiomyoma than to a
prolapse of a pedunculated submucosal leiomyoma into the vagina.
Additionally, in the patient described herein, none of the imaging
modalities used were able to prevent a misdiagnosis of
intracervical leiomyoma preoperatively. It is likely that the lack
of sufficient published data regarding the association between the
prolapse of pedunculated submucosal uterine leiomyoma and
obstructive uropathy with severe renal dysfunction was the main
reason for the diagnostic difficulties that were encountered.
Therefore, although uterine submucosal leiomyomas prolapsing into
the vagina are common, in the patient described herein, the
diagnosis was made at a late stage and intraoperatively.
In conclusion, the case presented herein, involving
bilateral obstructive uropathy with renal dysfunction associated
with large prolapsed pedunculated submucosal leiomyoma of the
uterus, is unique in the English literature, at least to the best
of our knowledge. A pre-operative diagnosis, particularly in cases
where the leiomyomas are large and prolapse into the vagina, poses
several challenges. A thorough clinical and imaging preoperative
evaluation is crucial for the early diagnosis of
hydroureteronephrosis and renal dysfunction attributed to a pelvic
tumor. Early and accurate diagnosis facilitates the immediate
utilization of the optimal treatment options, preventing permanent
renal damage and ensuring the continued health and quality of life
of these patients.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
ET, AT, EX and AZ participated in the conception and
design of the study, and in the international literature search.
VG, EK and IP were involved in the conception and design of the
study, in the provision of study materials (such as blood tests,
culture test and imaging) or patient data, as well as in data
collection and aggregation, and data analysis and interpretation.
ES and MM participated in the conception and design of the study,
and in the international literature search, as well as in the
provision of study materials (histological images). IT was involved
in the conception and design of the study, in administrative
support, in the provision of study materials (such as blood tests,
culture test and imaging) or patient data, in patient care, in data
collection, in manuscript writing and analysis, and had the overall
supervision of the manuscript. All authors (ET, AT, VG, EX, AZ, EK,
IP, ES, MM and IT) confirm the authenticity of all raw data. All
authors participated in the writing of the manuscript, contributed
to the revision of the manuscript, and have read and approved the
final version of the manuscript.
Ethics approval and consent to
participate
The present study was conducted according to the
guidelines of the Declaration of Helsinki. Written informed consent
was obtained from the patient described herein.
Patient consent for publication
The patient in the present study provided signed
consent for the publication of her medical case anonymously.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Lazaridis A, Hirsch M, Pistofidis G and
Odejinmi F: Surgical management of uterine fibroids. Curr Opin
Obstet Gynecol. 35:440–445. 2023.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Cook H, Ezzati M, Segars JH and McCarthy
K: The impact of uterine leiomyomas on reproductive outcomes.
Minerva Ginecol. 62:225–236. 2010.PubMed/NCBI
|
|
3
|
Klatsky PC, Tran ND, Caughey AB and
Fujimoto VY: Fibroids and reproductive outcomes: A systematic
literature review from conception to delivery. Am J Obstet Gynecol.
198:357–366. 2008.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Giuliani E, As-Sanie S and Marsh EE:
Epidemiology and management of uterine fibroids. Int J Gynaecol
Obstet. 149:3–9. 2020.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Stewart EA, Cookson CL, Gandolfo RA and
Schulze-Rath R: Epidemiology of uterine fibroids: A systematic
review. BJOG. 124:1501–1512. 2017.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Buttram VC Jr and Reiter RC: Uterine
leiomyomata: Etiology, symptomatology, and management. Fertil
Steril. 36:433–445. 1981.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Turhan N, Simavli S, Kaygusuz I and Kasap
B: Totally inverted cervix due to a huge prolapsed cervical myoma
simulating chronic non-puerperal uterine inversion. Int J Surg Case
Rep. 5:513–515. 2014.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Ben-Baruch G, Schiff E, Menashe Y and
Menczer J: Immediate and late outcome of vaginal myomectomy for
prolapsed pedunculated submucous myoma. Obstet Gynecol. 72:858–861.
1988.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Al-Shukri M, Al-Ghafri W, Al-Dhuhli H and
Gowri V: Vaginal myomectomy for prolapsed submucous fibroid: It is
not only about size. Oman Med J. 34:556–559. 2019.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Corte LD, Giampaolino P, Fabozzi A, Sardo
AD and Bifulco G: An exceptional uterine inversion in a virgo
patient affected by submucosal leiomyoma: Case report and review of
the literature. J Obstet Gynaecol Res. 45:466–472. 2019.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Zacharakis D, Athanasiou S, Kathopoulis N,
Michala L, Pontikaki A, Angelou K and Grigoriadis T: Large
pedunculated submucosal leiomyoma mimicking uterine prolapse. Clin
Case Rep. 9(e04319)2021.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Thanasa E, Thanasa A, Kamaretsos E,
Paraoulakis I, Ziogas A, Kontogeorgis G, Grapsidi V, Gerokostas EE,
Kontochristos V and Thanasas I: Large cervical leiomyoma of the
uterus: A rare cause of chronic pelvic pain associated with
obstructive uropathy and renal dysfunction: A case report. Cureus.
15(e33387)2023.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Wang J, Li Z and Sun Y: Prolapsed
submucosal pyomyoma postpartum, a rare complication of fibroids.
BMC Pregnancy Childbirth. 21(132)2021.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Torrance SM, Muhn N, Ellis S, Rebello R
and Ramanna R: Role of dynamic MRI in surgical decision-making for
a postpartum woman with a prolapsed degenerating uterine leiomyoma.
J Obstet Gynaecol Can. 31:446–451. 2009.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Li L, Shen J, Gao Z, Wang X, Tian D, Yang
X, Zhou H, Li B, Tang D and Zhang Q: Transvaginal prolapsed
submucosal leiomyoma after cesarean section misdiagnosed as bladder
prolapse: A case report with literature review. Front Surg.
10(1071247)2023.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Aydın S, Çelik HG, Maraşlı M and Bakar RZ:
Clinical predictors of successful vaginal myomectomy for prolapsed
pedunculated uterine leiomyoma. J Turk Ger Gynecol Assoc.
19:146–150. 2018.PubMed/NCBI View Article : Google Scholar
|
|
17
|
da Silva BB, da Silva-Sampaio JP and
Lopes-Costa PV: Huge prolapsed pedunculated necrotizing submucosal
leiomyoma. J Minim Invasive Gynecol. 25:1128–1129. 2018.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Golan A, Zachalka N, Lurie S, Sagiv R and
Glezerman M: Vaginal removal of prolapsed pedunculated submucous
myoma: A short, simple, and definitive procedure with minimal
morbidity. Arch Gynecol Obstet. 271:11–13. 2005.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Sleiman Z, Ayed A, Christoforou C, Noventa
M, Vitagliano A, Laganà AS and Buzzaccarini G: Hymen conservative
techniques for vaginal surgery-a practical approach. Prz
Menopauzalny. 21:64–68. 2022.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Mauri F, Emery SL and Dubuisson J: A
hybrid technique for the removal of a large prolapsed pedunculated
submucous leiomyoma. J Gynecol Obstet Hum Reprod.
51(102365)2022.PubMed/NCBI View Article : Google Scholar
|