Introduction
Neuroendocrine tumors (NET) include a spectrum of
malignancies arising from neuroendocrine cells throughout the body.
These tumors secrete peptides and neuropeptides that may cause
distinct clinical syndromes, such as the carcinoid syndrome. A
number of carcinoid tumors are clinically silent until their late
presentation with mass effect. Carcinoid tumors account for
<5.0% of all digestive tumors (1–5).
According to the World Health Organization (WHO) 2010
classification (6),
gastroenteropancreatic-NET (GEP-NET) are subdivided into
well-differentiated NET (WDET), well-differentiated neuroendocrine
carcinomas (WDEC) and poorly differentiated neuroendocrine
carcinomas (PDEC), whereas the old classification indicated only
three types: foregut, midgut and hindgut tumors. Although they
share some common characteristics, these tumors exhibit significant
differences in clinical behavior, genetic characteristics,
molecular and biochemical profiles and therapeutic approach.
GEP-NET are considered as fairly rare disease entities that pose
several clinical challenges.
Approximately 75.0% of all NET cases manifest in the
GEP system (5). Recent data from
the Surveillance, Epidemiology and End Results (SEER) program in
the United States, which is the largest series of NET cases
reported to date with a focus on incidence, prevalence and
prognosis factors, suggest that the incidence and prevalence of NET
have increased significantly over the past 3 decades. The incidence
of NET in the United States in 2004 was 5.09–5.42/100,000 and the
prevalence was 35/100,000 individuals (7), which may be explained by the
increased awareness and improved diagnostic techniques. Whether
this also reflects a true increase of incidence remains unclear
(8,9). Unlike the increase in incidence and
prevalence observed in SEER, there was no statistically significant
difference in survival duration among patients with local and
regional NET. The complexity, heterogeneity and rarity of NET have
contributed to the slow development of therapies for this disease.
GEP-NET are known for their lack of defining symptoms, which may
lead to a delay in diagnosis. However, on metastasis, the patients
may develop debilitating symptoms associated with the release of
highly bioactive substances.
These symptoms of metastasis, referred to as the
carcinoid syndrome, are associated with significant morbidity and
are quite vague, frequently leading to misdiagnosis of a more
common disorder, such as irritable bowel syndrome. Misdiagnosis
puts carcinoid syndrome patients at higher risk for carcinoid
crisis, the most immediate life-threatening complication of
carcinoid syndrome. In Argentina, awareness of GEP-NET is
significantly lower compared to that in the United States and
Europe. No epidemiological survey or NET registry has yet been
conducted, accounting for the total lack of accurate data on their
incidence and prevalence. This lack of consensus on the diagnosis
and management of GEP-NET in Argentina and the scarcity of data in
our region (Latin America) (10),
may account for their late diagnosis.
This study focuses on NET patients from Argentina.
We decided to include patients with bronchial NET (BNET) (typical
and atypical carcinoids only). Various treatment modalities,
including surgery, nuclear radiation and systemic and targeted
therapies, are topics of ongoing debate as practice patterns
evolve. The management of toxicity, recurrence and progression is
among the primary concerns of practitioners who make decisions on
the clinical management of this relatively rare disease.
Data on this NET population may be of particular
value in obtaining information on current and emerging treatment
patterns in Argentina and providing insight into the optimal
clinical practices.
The aim of this prospective study was to describe
the clinical symptoms, diagnostic procedures, treatment and
follow-up of NET in Argentina. This approach to routine clinical
practice may enhance our understanding of and clinical experience
with this uncommon tumor. To the best of our knowledge, this is the
first study providing information on NET patients in Latin
America.
Patients and methods
Study population
The population included in this study was obtained
from a large database launched by a scientific work group in
Argentina (the ARGENTUM group). Patients treated by oncologists,
surgeons, or gastroenterologists and those seen at institutions
affiliated with the ARGENTUM group were referred to the Bonorino
Udaondo Hospital (Buenos Aires, Argentina) for inclusion in this
observational study. The patients were categorized by tumor site
and histological subtype, according to the latest WHO
classification (6), as WDET, WDEC,
PDEC, or mixed exocrine-endocrine carcinoma. All the cases were
centrally evaluated (when necessary or required) by the
pathologists in our group. The tissue samples were examined using
hematoxylin and eosin and immunohistochemical staining techniques
to confirm the diagnosis of GEP-NET.
Data collection
The medical records were reviewed to collect the
following data: age, gender, functional syndrome, familial
hereditary syndrome, diagnostic procedures, site and size of
primary tumor, histopathological characteristics (based on the WHO
classification), immunohistochemical staining, grade and tumor
stage at diagnosis, metastatic pattern, therapeutic interventions
and results (surgery, locoregional therapies, hormone therapy,
chemotherapy, radiotherapy, radionuclide therapy and new targeted
therapies). Other collected data included date of diagnosis and
date of last visit or death.
The tumor stages were classified as locoregional
(with invasion of surrounding organs or tissues or compromise of
regional lymph nodes) or as distant metastases (the specific sites
of distant metastases were also recorded). The most relevant
clinical parameters were classified using descriptive
statistics.
Statistical analysis
Data are described using averages and standard
deviations for continuous variables with normal distribution or
using medians and interquartile ranges (IQRs) in controversial
cases. The distribution normality was assessed with the visual
inspection of the box diagrams (box plots), histograms and
quartile-quartile graphs and with the Shapiro-Wilk test.
Categorical data were described using absolute numbers and
percentages. The denominators used in the calculations are
specified in each table (n=xxx).
To compare categorical variables, the χ2
test (with appropriate degrees of freedom according to the category
of the variables compared) or the Fisher’s exact test were used. To
evaluate linear trend among categories, the Cochran-Armitage test
was used. To compare continuous variables among groups, the
Student’s t-test was used for variables with a normal distribution.
Otherwise, the Mann-Whitney U test was used to compare two groups
and the Kruskal-Wallis test was used to analyze more than two
groups. Cumulative survival and survival graphs were calculated
with the Kaplan-Meier method and survival functions in different
groups were compared using the log-rank test. All the tests were
two-tailed and P<0.05 was considered an indicator of
statistically significant differences. No adjustments were made for
multiple comparisons.
Results
Patient population
Of the 532 assessable patients with a diagnosis of
NET, 461 (86.6%) had GEP-NET and 71 (13.4%) had BNET. In the
primary analysis, the GEP-NET data were used. The median age at
diagnosis was 53.2 years and 26.0% of the GEP-NET patients
presented with hormone hypersecretion symptoms, with no significant
differences according to gender. Hereditary syndromes associated
with NET were diagnosed in 10 patients (2.2%), the majority of whom
were women (Table I). Of the 71
patients with NET of bronchopulmonary origin, 43 were women (61.0%)
and 28 were men (39.0%); their median age was 38 years (range,
13–67 years) (data not shown).
 | Table ICharacteristics of study population of
GEP-NET. |
Table I
Characteristics of study population of
GEP-NET.
| Variables | All patients (n=461)
GEP-NET | Female (n=255) | Male (n=206) | P-value |
|---|
| Age, years (SD),
(n=459) | 53.2 (15.1) | 52.0 (15.6) | 54.7 (14.4) | 0.063a |
| Male, n (%),
(n=461) | 206 (44.7) | - | - | - |
| Carcinoid syndrome, n
(%), (n=461) | 120 (26.0) | 58 (22.7) | 62 (30.1) | 0.074b |
| Incidental diagnosis,
n (%), (n=434) | 49 (10.6) | 28 (11.0) | 21 (10.2) | 0.785b |
| Symptoms, n (%),
(n=434) |
| Diarrhea | 75 (17.3) | 37 (15.5) | 38 (19.4) | 0.292b |
| Abdominal pain | 139 (32.0) | 80 (33.6) | 59 (30.1) | 0.435b |
| Flushing | 19 (4.4) | 10 (4.2) | 9 (4.6) | 0.843b |
| Digestive
hemorrhage | 19 (4.4) | 8 (3.4) | 11 (5.6) | 0.254b |
| Weight loss | 14 (3.2) | 10 (4.2) | 4 (2.0) | 0.205b |
| Intestinal
obstruction | 29 (6.7) | 15 (6.3) | 14 (7.1) | 0.727 |
| Histological
diagnosis, n (%), (n=457) |
| Well-differentiated
NET | 92 (20.1) | 58 (22.8) | 34 (16.8) | 0.432b |
| Well-differentiated
NEC | 304 (66.5) | 166 (65.1) | 138 (68.3) | |
| Poorly
differentiated NEC | 47 (10.3) | 24 (9.4) | 23 (11.4) | |
| Other | 14 (3.1) | 7 (2.7) | 7 (3.5) | |
| Hereditary
syndrome, n (%)c, (n=459) | 10 (2.2) | 6 (2.4) | 4 (1.9) | 1.00d |
| Staging at the time
of diagnosis, (n=461) |
| Local | 118 (25.6) | 75 (29.4) | 43 (20.8) | 0.062b |
| Locally
advanced | 68 (14.8) | 39 (15.3) | 29 (14.1) | |
| Metastatic | 273 (59.2) | 141 (55.3) | 132 (64.1) | |
| Not reported | 2 (0.4) | 0 (0.0) | 2 (1.0) | |
| Local tumors, n
(%) | 118 (25.6) | 75 (29.4) | 43 (20.9) | 0.037b |
| Size, median (IQR),
(n=298) | 2.0 (1.0–4.0) | 2.0 (1.0–4.0) | 2.0 (1.0–4.0) | 0.426e |
| Size, n (%),
(n=461) |
| ≤2 | 163 (35.4) | 98 (38.4) | 65 (31.6) | 0.391b,f |
| >2 and ≤4 | 68 (14.7) | 36 (14.1) | 32 (15.5) | |
| >4 | 67 (14.5) | 38 (14.9) | 29 (14.1) | |
| Not reported | 163 (35.4) | 83 (32.6) | 80 (38.8) | |
| Tumors, n (%),
(n=461) |
| Unicentric | 333 (72.2) | 187 (73.3) | 146 (70.9) | 0.842b |
| Multicentric | 45 (9.8) | 24 (9.4) | 21 (10.2) | |
| Not reported | 83 (18.0) | 44 (17.3) | 39 (18.9) | |
| Location, n (%),
(n=461g) |
| Esophagus | 13 (2.8) | 7 (2.7) | 6 (2.9) | 0.914b |
| Stomach | 32 (6.9) | 17 (6.7) | 15 (7.3) | 0.796b |
| Duodenum | 9 (1.9) | 3 (1.2) | 6 (2.9) | 0.197d |
| Small bowel | 124 (26.9) | 62 (24.3) | 62 (30.1) | 0.164b |
| Appendix | 35 (7.6) | 24 (9.4) | 11 (5.4) | 0.101b |
|
Colon-rectum-anus | 57 (12.4) | 38 (14.9) | 19 (9.2) | 0.066b |
| Pancreas | 116 (25.2) | 63 (24.7) | 53 (25.7) | 0.801b |
| Unknown | 75 (16.3) | 41 (16.1) | 34 (16.5) | 0.902b |
| Ki-67, median
(IQR), (n=239) | 5.0 (2.0–12.0) | 5.0 (2.0–10.0) | 5.0 (3.0–13.0) | 0.580 |
| Ki-67 categories, n
(%), (n=461) |
| ≤2% | 135 (29.3) | 84 (32.9) | 51 (24.8) | 0.212b |
| 3–20% | 164 (35.6) | 90 (35.3) | 74 (35.9) | |
| >20% | 41 (8.9) | 20 (7.8) | 21 (10.2) | |
| Not reported | 121 (26.2) | 61 (23.9) | 60 (29.1) | |
| Metastasis, n (%),
(n=454)h |
| Lymph nodes | 165 (36.3) | 89 (35.5) | 76 (37.4) | 0.663b |
| Liver | 254 (55.9) | 131 (52.2) | 123 (60.6) | 0.073b |
| Peritoneum | 49 (10.8) | 25 (10.0) | 24 (11.8) | 0.525b |
| Lung | 10 (2.2) | 5 (2.0) | 5 (2.5) | 0.758e |
| Bone | 5 (1.1) | 2 (0.8) | 3 (1.5) | 0.660d |
| Other | 12 (2.6) | 8 (3.2) | 4 (2.0) | 0.422b |
| Delay from onset of
symptoms to diagnosis, in months, median (IQR), (n=282) | 9.0 (3.0–24.0) | 10.0
(3.0–27.0) | 8.0
(3.25–20.0) | 0.467 |
According to the WHO 2000 classification (6,11),
92 patients (20.1%) with NET in various locations were classified
as WDET, 304 (66.5%) as WDEC and 47 (10.3%) as PDEC. According to
the current (2010) WHO classification (12), 135 (29.5%) of the 457 patients were
reclassified as NET grade 1 (G1), 164 (35.9%) as NET G2 and 41
(9.0%) as neuroendocrine carcinoma G3 (Table II).
| Table IIComparison between WHO 2000 (6,11)
and WHO 2010 (12) classifications
of GEP-NETa. |
Table II
Comparison between WHO 2000 (6,11)
and WHO 2010 (12) classifications
of GEP-NETa.
| | WHO 2010
classification, n (%) |
|---|
| |
|
|---|
| GEP-NET | WHO 2000
classification, n (%)b | No datac | NET G1 | NET G2 | NEC G3 |
|---|
| WDET | 92 (20.1) | 28 (30.4) | 51 (55.5) | 13 (14.1) | 0 (0.0) |
| WDEC | 304 (66.5) | 72 (23.7) | 82 (27.0) | 144 (47.4) | 6 (1.9) |
| PDEC | 47 (10.3) | 11 (23.4) | 0 (0.0) | 4 (8.5) | 32 (68.1) |
| Others | 14 (3.1) | 6 (42.9) | 2 (14.3) | 3 (21.4) | 3 (21.4) |
| Total | 457 (100.0) | 117 (25.6) | 135 (29.5) | 164 (35.9) | 41 (9.0) |
Diagnostic procedures
Incidental diagnosis occurred in 10.6% of the
patients (Table I). The diagnoses
were made primarily by performing incisional and excisional
biopsies in 30.1 and 59.6% of the patients, respectively. In
addition, 18.1% of the patients required more than one diagnostic
procedure (repeat biopsy). Biochemical tests, such as measurement
of serum chromogranin A and urinary 5-hydroxyindoleacetic acid
levels, were performed in 72.8 and 41.7% of the patients,
respectively. Scintigraphy with radiolabeled octreotide
(octreoscan) was performed in 46.5% of the patients, with positive
results in 79.0% of the cases. Immunohistochemical staining for
chromogranin A and synaptophysin was performed in 85.6 and 79.9% of
the tumors. The Ki-67 index was calculated in 73.7% of the tumors.
Echocardiography was performed in 30.4% of the reported cases and
the results were positive in 22.1% of the cases. The diagnostic
procedures are summarized in Table
III.
| Table IIIDiagnostic procedures. |
Table III
Diagnostic procedures.
| Procedures | Patients |
|---|
| Biopsy, n (%),
(n=448a) |
| Incisional | 135 (30.1) |
| Excisional | 267 (59.6) |
| Fine-needle
aspiration | 67 (15.0) |
| Core-needle
biopsy | 69 (15.4) |
| Biopsy, n (%),
(n=448) |
| 1 procedure | 367 (81.9) |
| 2 repeat
biopsies | 72 (16.1) |
| 3 repeat
biopsies | 9 (2.0) |
|
Immunohistochemistry, n (%), (n=459) |
| Synaptophysin |
| Performed | 367 (79.9) |
| Positive | 360 (78.4)
(98.1b) |
| Negative | 7 (1.5)
(1.9b) |
| Not
performed | 92 (20.1) |
| Chromogranin
A |
| Performed | 393 (85.6) |
| Positive | 338 (73.6)
(86.0b) |
| Negative | 55 (12.0)
(14.0b) |
| Not
performed | 66 (14.4) |
| TTF-1 |
| Performed | 33 (7.2) |
| Positive | 3 (0.7)
(9.1b) |
| Negative | 30 (6.5)
(90.9b) |
| Not
performed | 426 (92.8) |
| Biopsy material, n
(%), (n=458) |
| Primary
tumor | 227 (49.6) |
| Primary tumor +
metastasis | 95 (20.7) |
| Metastasis | 136 (29.7) |
| Biopsy location, n
(%), (n=457) |
| Intestines | 183 (40.1) |
| Liver | 124 (27.1) |
| Lymph nodes | 18 (3.9) |
| Lung | - |
| Other | 132 (28.9) |
| Diagnostic studies,
n (%) |
| Chromogranin A in
serum (n=459) |
| Yes | 334 (72.8) |
| No | 104 (22.6) |
| Not
performed | 21 (4.6) |
| 5-HIAA
(n=460) |
| Performed | 192 (41.7) |
| Positive | 71 (15.4)
(37.0b) |
| Negative | 121 (26.3)
(63.0b) |
| Not
performed | 268 (58.3) |
| Peptides
(n=460) |
| Performed | 107 (23.3) |
| Positive | 43 (9.4)
(40.2b) |
| Negative | 64 (13.9)
(50.8b) |
| Not
performed | 353 (76.7) |
| Octreoscan
(n=460) |
| Performed | 214 (46.5) |
| Positive | 169 (36.7)
(79.0b) |
| Negative | 45 (9.8)
(21.0b) |
| Not
performed | 246 (53.5) |
| Ki67 (n=461) |
| Reported | 340 (73.8) |
| Not reported | 121 (26.2) |
| Echocardiogram
(n=460) |
| Performed | 140 (30.4) |
|
Carcinoid-positive | 31 (6.7)
(22.1b) |
|
Carcinoid-negative | 109 (23.7)
(77.9b) |
| Not
performed | 320 (69.6) |
Tumor characteristics
Of the patients with GEP-NET, 118 (25.6%) had local
tumors at diagnosis, 68 (14.8%) had locally advanced disease and
273 (59.2%) had distant metastases. Over 35.4% of the patients with
GEP-NET had tumors sized <2 cm, whereas 68 of the tumors (14.8%)
were sized 2–4 cm and 14.5% were >4 cm. We were unable to obtain
information regarding tumor size in 163 patients (35.4%). In 9.8%
of the patients the tumors were multicentric. The Ki-67 index was
≤2% in 29.3%, 3–20% in 35.6% and >20% in 8.9% of the assessed
tumors (Table I). In BNET, 63
patients (89.0%) had typical and 8 had atypical carcinoids. Nine
typical (15.0%) and 5 atypical carcinoids (63.0%) presented with N2
lymph node metastasis (P=0.002), with median tumor sizes of 2.8 cm
(range, 5–7 cm) and 3.25 cm (range, 2–5 cm), respectively (data not
shown).
We analyzed metastatic sites in patients with
GEP-NET (Table IV). Hepatic
compromise was observed in 56.0% of the patients, followed by lymph
node compromise in 36.3%, peritoneum in 11.0%, lung in 2.2% and
bone in 1.1% of the cases. A 9-month delay from the onset of
symptoms to the time of diagnosis was observed; this information,
not often described in current studies, is important, although
interpretation bias may limit its value.
| Table IVLocations of metastases and primary
tumors in GEP-NET. |
Table IV
Locations of metastases and primary
tumors in GEP-NET.
| Locations of
primary tumora, n (%) | |
|---|
|
| |
|---|
| Locations of
metastases, n (%) | Esophagus
(n=13) | Stomach (n=32) | Duodenum (n=9) | Small bowel
(n=124) | Pancreas
(n=116) | Appendix
(n=35) | Colon (n=16) | Rectum (n=41) | P-value |
|---|
| Lymph nodes | 4 (30.8) | 6 (18.8) | 2 (22.2) | 74 (59.7) | 44 (37.9) | 3 (8.6) | 7 (43.8) | 5 (12.2) | <0.001 |
| Liver | 3 (23.1) | 5 (15.6) | 3 (33.3) | 87 (70.2) | 74 (63.8) | 0 (0.0) | 11 (68.8) | 5 (12.2) | <0.001 |
| Peritoneum | 0 (0.0) | 0 (0.0) | 2 (22.2) | 33 (26.6) | 5 (4.3) | 0 (0.0) | 1 (6.2) | 0 (0.0) | <0.001 |
| Lung | 1 (7.7) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 4 (3.4) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0.109 |
| Bone | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.8) | 2 (1.7) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0.928 |
| Ovary | 0 (0.0) | 0 (0.0) | 0 (0.0) | 2 (1.6)b | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0.751 |
| Brain | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.9) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0.939 |
| Liver + other | 1 (7.7) | 2 (6.2) | 0 (0.0) | 66 (53.2) | 32 (27.6) | 0 (0.0) | 5 (31.2) | 2 (4.9) | <0.001 |
Staging at diagnosis was significantly different,
depending on the primary tumor location, tumor type and grade
(Table V). The most common tumor
types were gastrointestinal carcinoids (59.0%), followed by
pancreatic endocrine tumors (25.0%) and metastatic NEC of unknown
primary location (16.0%). Functioning pancreatic endocrine tumors
were identified in 8.62% of all patients with pancreatic NET (pNET)
and in 2.1% of the total population. The gastrointestinal tract was
the primary tumor site in 270 patients (58.6%) and the pancreas in
116 patients (25.2%); in 73 patients (15.9%), the primary tumor
site was unknown. Among gastrointestinal tumors, the small bowel
(45.9%), colon-rectum (21.1%), appendix (13.0%) and stomach (11.9%)
were the most frequent sites of origin (Table V).
| Table VStaging at time of diagnosis
according to location of primary tumor and tumor type in
GEP-NET. |
Table V
Staging at time of diagnosis
according to location of primary tumor and tumor type in
GEP-NET.
|
Characteristicsa | All (n=459) | Local tumors
(n=118) | Regional invasion
(n=68) | Metastatic
(n=273) | P-value |
|---|
| Tumor type, n (%),
(n=459) | | | | | <0.001 |
| Intestinal | 270 (100.0) | 102 (37.8) | 39 (14.4) | 129 (47.8) | |
| Non-functioning
pancreatic | 106 (100.0) | 15 (14.2) | 26 (24.5) | 65 (61.3) | |
| Functioning
pancreatic | 10 (100.0) | 1 (10.0) | 0 (0.0) | 9 (90.0) | |
| Primary
unknown | 73 (100.0) | - | 3 (4.1)b | 70 (95.9) | |
| Tumor site
(n=459) | | | | | |
| Gastrointestinal
tract | 270 (100.0) | 102 (37.8) | 39 (14.4) | 129 (47.8) | <0.001 |
| Esophagus | 13 (100.0)
(4.8c) | 5 (38.4)
(4.9c) | 4 (30.8)
(10.3c) | 4 (30.8)
(3.1c) | 0.082 |
| Stomach | 32 (100.0)
(11.9c) | 22 (68.8)
(21.6c) | 4 (12.5)
(10.3c) | 6 (18.7))
(4.7c) | <0.001 |
| Duodenum | 9 (100.0)
(3.3c) | 3 (33.3)
(2.9c) | 1 (11.1)
(2.5c) | 5 (55.6)
(3.9c) | 0.854 |
|
Jejunum-ileum | 124 (100.0)
(45.9c) | 7 (5.7)
(6.9c) | 23 (18.5)
(58.9c) | 94 (75.8)
(72.9c) | <0.001 |
| Appendix | 35 (100.0)
(13.0c) | 30 (85.7)
(29.4c) | 3 (8.6)
(7.7c) | 2 (5.7)
(1.5c) | <0.001 |
| Colon-rectum | 57 (100.0)
(21.1c) | 35 (61.4)
(34.3c) | 4 (7.0)
(10.3c) | 18 (31.6)
(13.9c) | <0.001 |
| Pancreas | 116 (100.0) | 16 (13.8) | 26 (22.4) | 74 (63.8) | 0.001 |
| Unknown | 73 (100.0) | - | 3 (4.1) | 70 (95.9) | <0.001 |
| Histopathology, n
(%), (n=457) | | | | | |
| ≤2% | 135 (100.0) | 53 (39.3) | 17 (12.6) | 65 (48.1) | <0.001 |
| 3–20% | 164 (100.0) | 26 (15.9) | 23 (14.0) | 115 (70.1) | |
| >20% | 41 (100.0) | 5 (12.2) | 9 (21.9) | 27 (65.9) | |
| Not performed | 117 (100.0) | 33 (28.2) | 19 (16.2) | 65 (55.6) | |
| Ki-67, median
(IQR), (n=239) | 5.0 (2.0–12.0) | 3.0 (2.0–9.5) | 6.0 (3.0–21.0) | 5.0 (3.0–12.0) | 0.02d |
| Tumor
differentiation degree, n (%), (n=456) | | | | | |
|
Well-differentiated NET | 92 (100.0) | 79 (85.9) | 3 (3.2) | 10 (10.9) | <0.001 |
| Differentiated
NEC | 303 (100.0) | 22 (7.3) | 52 (17.1) | 229 (75.6) | |
| Poorly
differentiated NEC | 47 (100.0) | 8 (17.0) | 12 (25.5) | 27 (57.5) | |
| Other | 14 (100.0) | 8 (57.24) | 1 (7.1) | 5 (35.7) | |
| Delay from symptom
onset to time of diagnosis, in months, median (IQR), (n=282) | 9.0 (3.0–24.0) | 8.0 (4.0–18.0) | 8.5 (2.3–25.3) | 10.0
(3.0–27.0) | 0.876 |
The small bowel was the primary tumor site in the
majority (75.8%) of patients with a higher incidence of hepatic
involvement. In NET of gastrointestinal origin, the esophagus
(30.8%) and the colon-rectum (13.9%) were most frequently involved.
The majority (63.8%) of patients with pNET had metastases at
diagnosis. Functioning pancreatic tumors (90.0%) were those most
commonly associated with widespread disease. A different pattern
was observed in patients with primary tumors of the appendix and
the stomach. Only 1.5 and 4.7% of those patients, respectively, had
tumors that had already metastasized at the time of diagnosis. A
significant proportion (57.4%) of patients with PDEC had
metastases, as did 75.6% of WDEC and 10.9% of WDET patients.
Therapeutic interventions
Overall, 67.3% of the GEP-NET patients underwent
surgery, 41.2% with curative intent and 26.1% for palliative
purposes. Curative intent surgery was more frequent in patients
with local disease (54.5%) and locally advanced disease (23.8%).
Palliative surgery was performed in 91.7% of patients with
metastatic disease. Locoregional therapies, such as embolization,
chemoembolization, radiofrequency and other ablative techniques
were uncommon (8.7%); chemoembolization was the mostly frequently
used locoregional therapy (60.0% of regional therapies) (Table VI).
| Table VITherapeutic interventions for
patients with GEP-NET. |
Table VI
Therapeutic interventions for
patients with GEP-NET.
| Interventions | All (n=459) | Local tumor
(n=118) | Regional invasion
(n=68) | Metastatic
(n=273) | P-value |
|---|
| Surgery, n (%),
(n=309) |
| | <0.001 | | | |
| Curative | 189 (100.0) | 103 (54.5) | 45 (23.8) | 41 (21.7) | |
| Palliative | 120 (100.0) | 1 (0.8) | 9 (7.5) | 110 (91.7) | |
| Regional procedure,
n (%), (n=459) | 40 (100.0) | 0 (0.0) | 1 (2.5) | 39 (97.5) | <0.001a |
|
Chemoembolization | 24 (100.0) | 0 (0.0) | 1 (4.2) | 23 (95.8) | 0.877b |
|
Radiofrequency | 7 (100.0) | 0 (0.0) | 0 (0.0) | 7 (100.0) | |
| Embolization | 4 (100.0) | 0 (0.0) | 0 (0.0) | 4 (100.0) | |
| Other | 5 (100.0) | 0 (0.0) | 0 (0.0) | 5 (100.0) | |
|
Radiopharmaceuticals, n (%) (n=459) | 8 (100.0) | 0 (0.0) | 0 (0.0) | 8 (100.0) | 0.062 |
| Radiotherapy, n
(%), (n=421) | 30 (100.0) | 5 (16.7) | 9 (30.0) | 16 (53.3) | 0.045 |
| Medical treatment,
n (%), (n=458) |
| Analogues and/or
interferon | 461 (100.0) | 144 (31.2) | 62 (13.5) | 255 (55.3) | 0.810a |
| Analogue-only
receivers | 140 (100.0)
(30.3c) | 0 (0.0) | 12 (8.6)
(19.4c) | 128 (91.4)
(50.1c) | <0.001b |
| Interferon-only
receivers | 41 (100.0)
(8.9c) | 0 (0.0) | 0 (0.0) | 41 (100.0)
(16.1c) | |
| Both | 22 (100.0)
(4.8c) | 0 (0.0) | 3 (13.6)
(4.8c) | 19 (86.4)
(7.4c) | |
| Chemotherapy, n
(%), (n=456) | 133 (100.0) | 10 (7.5) | 18 (13.5) | 105 (79.0) | <0.001d |
| Chemotherapy
cycles, n (%), (n=123e) |
| 1 cycle | 94 (100.0) | 10 (10.7) | 13 (13.8) | 71 (75.5) | 0.246 |
| 2 cycles | 19 (100.0) | 0 (0.0) | 2 (10.5) | 17 (89.5) | |
| 3 cycles | 10 (100.0) | 0 (0.0) | 3 (30.0) | 7 (70.0) | |
| Sunitinib, n (%),
(n=422) | 21 (100.0) | 0 (0.0) | 2 (9.5) | 19 (90.5) | 0.086f |
| Everolimus, n (%),
(n=423) | 15 (100.0) | 0 (0.0) | 1 (6.6) | 14 (93.4) | 0.048f |
| New drugs, n (%),
(n=419) | 36 (100.0) | 0 (0.0) | 3 (8.3) | 33 (91.7) | 0.004a |
A total of 203 patients received some type of
systemic treatment, including chemotherapy received by 133
patients, during the course of their disease: somatostatin
analogues (30.3%), interferon (8.9%) and combined treatment with
somatostatin analogues plus interferon (4.8%). A total of 94
patients (29.0%) underwent at least one chemotherapy cycle and 36
(7.8%) received a new drug (everolimus or sunitinib). These
percentages were higher among patients with advanced disease
(somatostatin analogues, 91.4%; interferon, 100.0%; combined
treatment, 86.3%). A total of 75.5% of patients who underwent
chemotherapy had advanced disease, as did 91.6% of patients treated
with new drugs (Table VI).
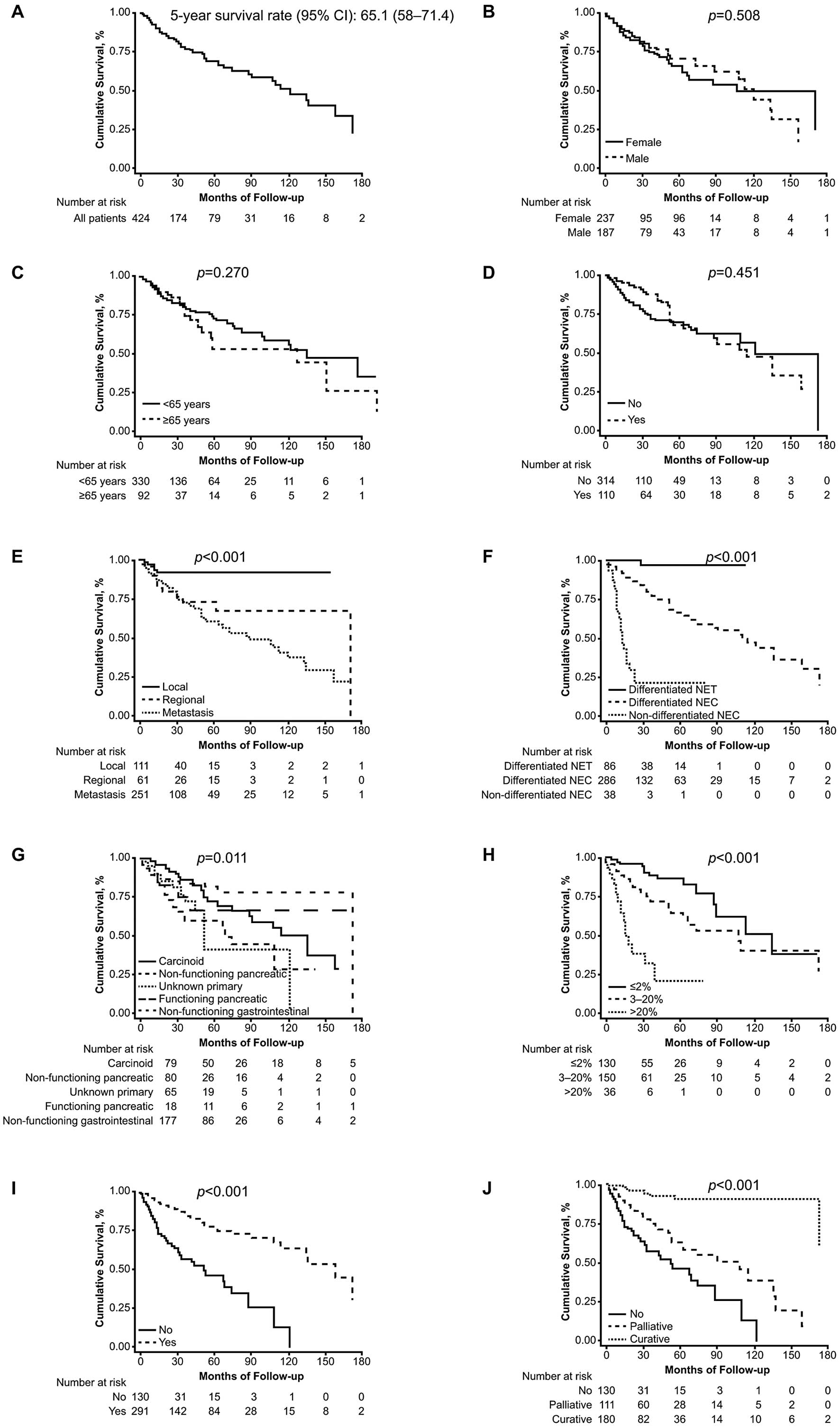
Survival and prognostic factors
The association between the overall survival and
prognostic factors is summarised in Fig. 1. The overall survival of the
GEP-NET patients in this study was 65.1 months (range, 58–71.4
months). A total of 46 patients (10.0%) were given different
histological diagnoses following examination by the pathologists in
our group: hepatocellular carcinoma (13.04%), poorly differentiated
carcinoma (8.7%), lymphoproliferative disease (8.7%), primary
unknown adenocarcinoma (6.5%), colon adenocarcinoma (6.5%) and not
otherwise specified (61.0%) (data not shown). Based on
epidemiological data from SEER (1950–1999) (5), 22.4% of the cases of non-carcinoid
second primary tumors have been described in patients with
diagnoses of NET; a high percentage of associated tumors occurred
in small intestinal carcinoids (29.0%). The incidence of this type
of tumors varies, depending on the series assessed.
Synchronous or metachronous second tumors developed
in 50 patients (11.0%): colorectal (24.0%), prostate (14.0%),
breast (6.0%), melanoma (6.0%), bladder (6.0%), thyroid (6.0%),
kidney (4.0%), pituitary tumor (2.0%), skin epidermoid carcinoma
(2.0%), head and neck (2.0%), gastric (2.0%), cervical (2.0%) and
not otherwise specified (24.0%) (data not shown). Twenty percent of
the tumors were synchronous and 80.0% were metachronous.
Non-endocrine neoplasms had been previously diagnosed in 70.0%% of
the patients. Little information is available in the literature
regarding the true incidence of second neoplasms in patients with
NET (13–15). The association rate was 11.0% in
our series, primarily with NET of the small bowel and pancreas
(data not shown).
The overall survival was significantly higher for
patients whose tumors were diagnosed at an early stage, were of
gastrointestinal origin, or were well-differentiated or low-grade.
The prognosis also differed according to tumor type, including
non-functioning gastrointestinal, small bowel carcinoid,
functioning pancreatic, non-functioning pancreatic and unknown
primary tumors (Table VII). The
multivariate analysis confirmed stage at diagnosis, tumor subtype,
tumor grade and evidence of surgery as independent prognostic
factors for survival (Table
VIII).
| Table VIISurvival and prognostic factors in
GEP-NET. |
Table VII
Survival and prognostic factors in
GEP-NET.
| Patients | No. | Median
(months) | 5-year survival
rate (%) | 95% confidence
interval | P-value |
|---|
| All | 424 | 121 | 65.1 | 58.0–71.4 | - |
| Gender | 424 | | | | |
| Female | 237 | 108 | 62.1 | 51.7–70.9 | 0.508 |
| Male | 187 | 121 | 68.3 | 58.0–76.7 | |
| Age (years) | 422 | | | | |
| ≥65 | 92 | 114 | 50.7 | 34.2–65.1 | 0.270 |
| <65 | 330 | 121 | 69.1 | 61.4–75.7 | |
| Carcinoid
syndrome | 424 | | | | |
| Yes | 110 | 114 | 64.5 | 50.4–75.6 | 0.451 |
| No | 314 | 121 | 66.5 | 58.4–73.4 | |
| Stage at
diagnosis | 423 | | | | |
| Local | 111 | NSa | 91.8 | 82.5–96.3 | <0.001 |
| Regionally
advanced | 61 | 172 | 68.3 | 50.2–81.0 | |
| Metastatic | 251 | 90 | 55.9 | 46.7–64.2 | |
| Location | 358 | | | | |
| Gastrointestinal
tract | 253 | 136 | 74.0 | 65.1–80.9 | 0.011 |
| Pancreas | 105 | 74 | 56.3 | 42.6–67.9 | |
| Tumor type | 421 | | | | |
| Carcinoid | 79 | 135 | 68.0 | 52.4–79.4 | 0.011 |
| Non-functioning
pancreatic | 80 | 68 | 55.1 | 38.7–68.9 | |
| Primary
unknown | 66 | 52 | 38.1 | 16.0–60.3 | |
| Functioning
pancreatic non-carcinoid | 19 | NSa | 63.3 | 34.8–82.1 | |
| Non-functioning
gastrointestinal | 177 | 172 | 78.8 | 68.7–86.0 | |
| Ki-67 category | 316 | | | | |
| ≤2% | 130 | 135 | 85.0 | 72.2–92.2b | <0.001 |
| 3–20% | 150 | 108 | 61.7 | 49.8–71.6b | |
| >20% | 36 | 16 | 15.7 | 3.2–36.9b | |
| Binary Ki-67 | 220 | | | | |
| ≥5 | 125 | 63 | 47.1 | 34.7–58.5b | <0.001 |
| <5 | 95 | 172 | 85.7 | 71.4–93.2b | |
| Tumor grade | 410 | | | | |
| Differentiated
NET | 86 | NSa | 97.4 | 82.8–99.6 | <0.001 |
| Differentiated
NEC | 286 | 114 | 63.6 | 54.8–71.0 | |
| Poorly
differentiated NEC | 38 | 13 | 18.4 | 5.7–36.7 | |
| Table VIIICox multivariate analysis for overall
survival in GEP-NET (model 1a,
n=376). |
Table VIII
Cox multivariate analysis for overall
survival in GEP-NET (model 1a,
n=376).
| Variables | Odds ratio | 95% confidence
interval | P-value |
|---|
| Age | 0.99 | 0.97–1.01 | 0.583 |
| Male gender | 0.90 | 0.53–1.53 | 0.706 |
| Tumor stage |
| Local | (Reference) | - | - |
| Regional | 2.44 | 0.73–8.23 | 0.150 |
| Metastatic | 3.12 | 1.02–9.56 | 0.047 |
| Tumor type |
| Carcinoid | (Reference) | - | - |
| Non-functioning
pancreatic | 0.75 | 0.33–1.69 | 0.483 |
| Primary
unknown | 0.33 | 0.13–0.83 | 0.018 |
| Functioning
pancreatic non-carcinoid | 0.58 | 0.19–1.79 | 0.338 |
| Non-functioning
gastrointestinal | 0.39 | 0.17–0.90 | 0.027 |
| Tumor grade |
| Differentiated
NET | (Reference) | - | - |
| Differentiated
NEC | 11.40 | 1.40–92.68 | 0.023 |
|
Non-differentiated | 67.41 | 7.95–571.67 | <0.001 |
| Surgery | 0.43 | 0.23–0.81 | 0.008 |
Discussion
This study provides relevant information regarding
the epidemiology, incidence and management of NET in Argentina.
Although other countries have their own registries (2–4), we
considered it important to use Argentina-specific data in order to
achieve a better understanding of the disease in this area and to
optimize available diagnostic and therapeutic resources.
We distinguished the different clinical
presentations. Abdominal pain was the most frequent symptom (32.0%
of the patients), followed by diarrhea (17.3% of the patients).
Both symptoms are non-specific, which may explain the late
diagnosis and advanced disease stage in 59.2% of the patients. The
initial presentation pattern was carcinoid syndrome in 26.0% of the
patients, which was similar to what has been reported in other
recent series (16,17). We observed a different biological
behavior confirming the heterogeneity of NET. Survival differed
based on histological subtype, although the study’s total
population maintained a 5-year survival rate of 65.1%. Our series
demonstrated a distribution similar to that observed in the
recently published study of the National Cancer Registry of Spain
(Grupo Español de Tumores Neuroendocrinos; GETNE) (17). As expected, the gastrointestinal
tract (58.6%) was the most prevalent site, followed by the pancreas
(25.2%) and primary unknown (16.3%). The small bowel (26.9%) was
the most frequent location of primary gastrointestinal tumors,
followed by the colon-rectum (12.4%) and appendix (7.6%). The
incidence of colon-rectum reported by the GETNE group (17) was marginally lower (10.5%) and the
other most frequent locations were reported to be the
jejunum-ileum, appendix and stomach, which was different from our
results. Other series or registries of European countries also
indicated the small bowel as the most frequent tumor location
(18). An observation that was
shared by our study and others (16,17)
is the presence of disseminated disease at diagnosis (59.2% of
patients in the present study); however, this may have been biased
in our study. In Argentina, patients with disseminated disease at
diagnosis are frequently reported and followed up by oncologists;
thus, our study may involve a certain extent of underreporting by
endocrinologists, gastroenterologists and other specialists. The
presence of non-specific symptoms may delay diagnosis; in our
series, the most frequently observed non-specific symptom was
abdominal pain (32.0%). The primary locations most frequently
associated with metastasis were the jejunum-ileum (72.9%), pancreas
(63.8%) and colon-rectum (13.9%). These differ from SEER data,
which indicate the pancreas (64.0%), colon (4.0%) and jejunum-ileum
(30.0%) as the most frequent sites associated with advanced-stage
disease (9).
Patients with poorly differentiated carcinomas
exhibited a worse prognosis (18.4% with 5-year survival) and
presented with metastatic disease at the time of diagnosis (57.4%
of the patients). In 457 of the 461 patients, diagnosis was
established according to guidelines of the European Consensus
through the European Neuroendocrine Tumor Society, following the
parameters of the WHO 2000 classification. In 340 of the 457
patients, there was a correlation with the new WHO 2010
classification; to the best of our knowledge, this constituted the
first such correlation with patient data in Latin America. After
the ARGENTUM work group was created in our country, we noted the
high percentage of serum chromogranin A studies (72.8% of the
patients) and the use of octreoscan (gold standard) to adequately
stratify patients with NET (46.5% of the patients). These data are
considered relevant when compared, for example, with data from
Spanish investigators (41.0% for chromogranin A determination and
50.0% for octreoscan) (17). In
2009, German investigators reported the use of somatostatin
receptor scintigraphy (56.0%) and specific laboratory tests (67.0%)
(19). Conversely, in some Latin
American countries, chromogranin A determinations are not used as
part of the routine work-up in NET patients. We also observed the
application of immunohistochemistry, with the study of at least two
NET markers, such as synaptophysin and chromogranin, in tumor
tissues (79.9 and 85.6%, respectively). Ki-67 studies were
conducted in 73.7% of patients, comparing favorably with the GETNE
data (17), which reported 36.0%
for this prognostic factor.
We observed a rate of 10.6% of incidental diagnosis
vs. 22.0% in the GETNE group. The diagnostic yield with incisional
or excisional biopsy was high. Diagnoses were reached in 89.7% of
the patients, with immunohistochemistry techniques performed in the
samples obtained.
We made extensive use of systemic treatment, such as
somatostatin analogues (30.3%) and surgery with curative or
palliative intent (67.32%) and less frequent use of locoregional
ablative approaches, such as regional procedures (8.7%) and
radionuclide therapy (1.7%), indicating the different practices
performed in different centers and the deficit in teams able to
perform these types of procedures.
The 5-year survival rate of 65.1% in the total
population was considered favorable. As reported in other series,
we observed significant differences in this measure between
gastrointestinal and pancreatic tumors (74.0 vs. 56.3%; P=0.011).
Survival was significantly higher in early disease stages and
low-grade tumors. The prognosis also differed significantly
according to tumor type, primary tumor site, Ki-67 and grading
tumor classification. In the multivariate analysis model, we
identified stage at diagnosis, tumor subtype, tumor grade and
surgery as independent outcome predictors.
In conclusion, we described diverse aspects
associated with the treatment of patients with NET and the use of
different treatment strategies, diagnostic procedures and follow-up
modalities by our work group, ARGENTUM. However, despite the recent
improvements, delayed diagnosis remains high in NET patients. To
the best of our knowldge, this study constitutes the first account
of NET patients in our region with adequate follow-up and survival
data.
Acknowledgements
Funding for this study was provided by Novartis
Argentina. We would like to thank Lucila Lavigna and all the
physicians who assisted with this project. We would also like to
thank Maria Monneret de Villars, who provided medical writing
assistance. We particularly thank Dr Gianfranco Delle Fave for his
invaluable support with this project.
References
|
1
|
Newton JN, Swerdlow AJ, dos Santos Silva
IM, Vessey MP, Grahame-Smith DG, Primatesta P and Reynolds DJ: The
epidemiology of carcinoid tumours in England and Scotland. Br J
Cancer. 70:939–942. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Janson ET, Holmberg L, Stridsberg M,
Eriksson B, Theodorsson E, Wilander E and Oberg K: Carcinoid
tumors: analysis of prognostic factors and survival in 301 patients
from a referral center. Ann Oncol. 8:685–690. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Levi F, Te VC, Randimbison L, Rindi G and
La Vecchia C: Epidemiology of carcinoid neoplasms in Vaud,
Switzerland, 1974–97. Br J Cancer. 83:952–955. 2000.PubMed/NCBI
|
|
4
|
Quaedvlieg PF, Visser O, Lamers CB,
Janssen-Heijen ML and Taal BG: Epidemiology and survival in
patients with carcinoid disease in The Netherlands. An
epidemiological study with 2391 patients. Ann Oncol. 12:1295–1300.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Modlin IM, Lye KD and Kidd M: A 5-decade
analysis of 13,715 carcinoid tumors. Cancer. 97:934–959. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kloppel G, Perren A and Heitz PU: The
gastroenteropancreatic neuroendocrine cell system and its tumors:
the WHO classification. Ann NY Acad Sci. 1014:13–27. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Yao JC, Hassan M, Phan A, Dagohoy C, Leary
C, Mares JE, Abdalla EK, Fleming JB, Vauthey JN, Rashid A and Evans
DB: One hundred years after ‘carcinoid’: epidemiology of and
prognostic factors for neuroendocrine tumors in 35,825 cases in the
United States. J Clin Oncol. 26:3063–3072. 2008.
|
|
8
|
Modlin IM, Oberg K, Chung DC, et al:
Gastroenteropancreatic neuroendocrine tumours. Lancet Oncol.
9:61–72. 2008. View Article : Google Scholar
|
|
9
|
Öberg K: What can be achieved in NET
management today? In: Presented at 5th Annual ENETS Conference for
The diagnosis and treatment of neuroendocrine tumor disease; March
6–8, 2008; Paris, France
|
|
10
|
Costa F, Domenichini E, Garavito G,
Medrano R, Mendez G, O’Connor J, Rojas W, Torres S, Younes RN,
Delle Fave G and Oberg K: Management of neuroendocrine tumors: a
meeting of experts from Latin America. Neuroendocrinology.
88:235–242. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Klöppel G, Couvelard A, Perren A, et al:
Mallorca Consensus Conference participants; European Neuroendocrine
Tumor Society: ENETS Consensus Guidelines for the Standards of Care
in Neuroendocrine Tumors: towards a standardized approach to the
diagnosis of gastroenteropancreatic neuroendocrine tumors and their
prognostic stratification. Neuroendocrinology. 90:162–166.
2009.
|
|
12
|
Bosman FT, Carneiro F, Hruban RH and
Theise ND: WHO Classification of Tumours of the Digestive System.
IARC Press; Lyon: 77–82. pp. 137–139. 2010
|
|
13
|
Habal N, Sims C and Bilchik AJ:
Gastrointestinal carcinoid tumors and second primary malignancies.
J Surg Oncol. 75:310–316. 2000. View Article : Google Scholar
|
|
14
|
Tichansky DS, Cagir B, Borrazzo E, Topham
A, Palazzo J, Weaver EJ, Lange A and Fry RD: Risk of second cancers
in patients with colorectal carcinoids. Dis Colon Rectum. 45:91–97.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Fendrich V, Waldmann J, Bartsch DK,
Schlosser K, Rothmund M and Gerdes B: Multiple primary malignancies
in patients with sporadic pancreatic endocrine tumors. J Surg
Oncol. 97:592–595. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Niederle MB and Niederle B: Diagnosis and
treatment of gastroenteropancreatic neuroendocrine tumors: current
data on a prospectively collected, retrospectively analyzed
clinical multicenter investigation. Oncologist. 16:602–613. 2011.
View Article : Google Scholar
|
|
17
|
Garcia-Carbonero R, Capdevila J,
Crespo-Herrero G, et al: Incidence, patterns of care and prognostic
factors for outcome of gastroenteropancreatic neuroendocrine tumors
(GEP-NETs): results from the National Cancer Registry of Spain
(RGETNE). Ann Oncol. 21:1794–1803. 2010. View Article : Google Scholar
|
|
18
|
Hauso O, Gustafsson BI, Kidd M, Waldum HL,
Drozdov I, Chan AK and Modlin IM: Neuroendocrine tumor
epidemiology: contrasting Norway and North America. Cancer.
113:2655–2664. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Ploeckinger U, Kloeppel G, Wiedenmann B
and Lohmann R; representatives of 21 German NET centers. The German
NET-registry: an audit on the diagnosis and therapy of
neuroendocrine tumors. Neuroendocrinology. 90:349–363. 2009.
View Article : Google Scholar : PubMed/NCBI
|