1. Introduction
Worldwide, in the past few decades, lung cancer has
become the most prolific malignant tumor endangering human health,
and the number of cases and associated deaths from lung cancer has
been on the rise (1,2). Lung cancer accounts for 21% of all
tumors and 27% of all cancer-associated deaths. In 2018, an
estimated 2.1 million people were newly found to have lung cancer,
including ~1.38 million cases of lung cancer in men, with the
highest incidence in Eastern Asia (>40/100,000 in China, Korea
and Japan), Micronesia/Polynesia and much of Europe
(>50/100,000), especially in Eastern Europe (49.3/100,000). At
the same time, lung cancer rates in men in Africa remain generally
low. Overall, in women, lung cancer rates are lower than those in
men, with the highest incidence rates occurring in Western Europe
(25.7/100,000), Northern Europe (26.9/100,000) and North America
(30.7/100,000) (2). Furthermore,
there is a geographical difference in the incidence of smoking
among women compared with men, which may be ascribed to differences
in smoking history among different regions (1,2). It
should be noted that the incidence rate among Chinese women
(22.8/100,000) is no different from that of western European
countries such as France (22.5/100,000), despite the epidemiology
of smoking being different in the two countries (lower smoking rate
among Chinese women) (2). However,
the high incidence of this type of lung cancer reflects the
possible increased exposure to charcoal burning or smoke production
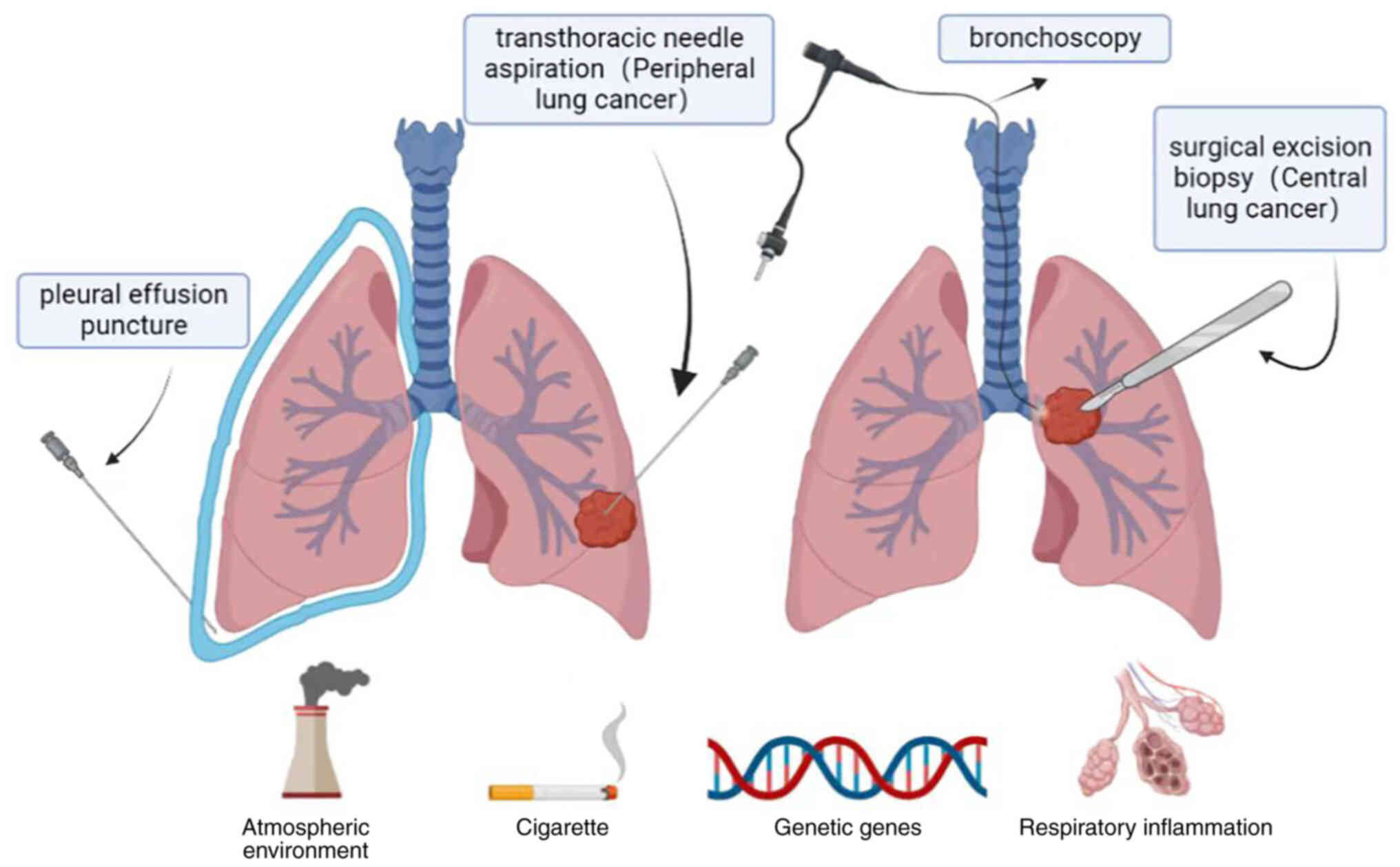
(3). There are two histological
types of lung cancer: NSCLC (80-85%) and SCLC. Although the
etiology of lung cancer is not completely clear, it is mainly
related to the following risk factors: Smoking, occupational
exposure (such as asbestos and radon), ionizing radiation, exposure
to second-hand smoke, genetic factors and infectious or
non-infectious respiratory diseases (2) (Fig.
1). One current treatment for NSCLC is the dual inhibition of
the EGFR and VEGF pathways, as EGFR and VEGF play an important role
in the development of NSCLC. According to a previous study, the
EGFR and VEGF pathways are correlated, and double inhibition has a
good therapeutic effect compared with the simple inhibition of the
EGFR pathway (4). The present
study reviews the causes of lung cancer, effective therapeutic
measures, and the advantages of EGFR and VEGF dual inhibition in
the treatment of NSCLC.
2. Risk factors of lung cancer
The pathogenesis of lung cancer is very complex,
involving multiple gene mutations, such as EGFR/KEAS/TP53/P13KCAA
mutations, ALK/RET/ROS1 rearrangements and EGFR/MET/FGFR1
amplifications (2,5). Some cascade reactions in lung cancer
have been confirmed in broncho-lung cancer studies:
Acinar/BA-lepidic/micro-papillary patterns express TTF1 and mutated
EGFR; bronchial-pulmonary adenocarcinomas in non-smoking females
exhibit mutated EGFR and ERCC1 expression; vimentin/RB/ERCC1 was
expressed in micropapillary tumors; EGFR and HER2 multibody and
CK7/vimentin are expressed in epidermoid carcinoma, and this
expression can be used for epithelial-mesenchymal transformation
into non-pure epidermoid carcinoma (5,6).
Lung cancer is also connected with smoking, exposure to second-hand
smoke, occupational exposure, ionizing radiation, infectious or
non-infectious respiratory diseases, and genetic factors (5).
Tobacco smoking
The most important risk factor for lung cancer is
tobacco smoking (7). According to
statistics, the risk of lung cancer in smokers is 20 times that of
lifelong non-smokers, and this risk is related to the number of
years of smoking and the number of cigarettes smoked per day
(8-10). Tobacco smoke contains thousands of
compounds in the gas and particle phases. The 'Hoffman List'
(11) highlights >60
carcinogens in cigarette smoke that are known as major carcinogens
and includes nitrosamines, polycyclic aromatic hydrocarbons,
volatile organic compounds, aromatic amines, aldehydes and metals,
among others (11). Seven
tobacco-specific nitrosamines have been found in tobacco products,
but two of these, 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanone
(NNK) and N'-nitroso or nicotine, are the most important due to
their carcinogenic activity (11).
NNK requires metabolic activation by cytochrome P450-catalyzed
α-hydroxylation to exert its carcinogenic properties. This process
is the key to its carcinogenicity. NNK and its main metabolite
[4-(methylnitrosa mino)-1-(3-pyridyl)-1-butanol] are formed by the
reaction of methanediazosynthesis with DNA to form well-known DNA
adducts, which lead to mutations and lung tumors (12,13).
Tobacco exposure can lead to mutations in KRAS and
TP53 genes, which in turn are closely related to the occurrence of
lung cancer. Tobacco smoke components or its metabolic activation
products directly damage the TP53 tumor suppressor gene, leading to
mutation and loss of the control mechanism of normal cell growth,
and the change in p53 plays an important role in malignant
transformation, invasion and metastasis (14,15).
A study has shown that these mutations are caused by DNA adducts of
tobacco carcinogens (14).
Exposure to second-hand smoke
Second-hand smoke is a form of indirect carcinogenic
exposure from burning tobacco. Carcinogens related to lung cancer
can be detected in second-hand smoke, including nitrosamines,
polycyclic aromatic hydrocarbons and aromatic amines (2). Studies have shown that the risk of
lung cancer from second-hand smoke is strongly related to the
duration of exposure. Long-term exposure to secondhand smoke is
estimated to increase the risk by 18-23% (16). A study evaluating the connection
between second-hand smoke exposure and lung cancer among
non-smokers in Japan reported a 28% increased risk compared with
the risk in unexposed non-smokers (17). Therefore, for the prevention of
lung cancer in non-smokers, it is very important to reduce their
exposure to second-hand smoke. At the same time, the implementation
of relevant measures to reduce the exposure to second-hand smoke
can also reduce the opportunities for smoking overall, thus
achieving a win-win effect of tobacco control and second-hand smoke
exposure control (16,18).
Occupational exposure and lung
cancer
Occupational exposure is also an important cause of
lung cancer, for which asbestos is the most common exposure factor.
Asbestos includes amphibole and chrysotile, which are widely used
in building materials, car brakes, asbestos panels and insulation
(2,19-21).
The mechanism of asbestos-induced lung cancer is very complex and
is currently considered to be related to changes in apoptosis
regulation, oxidative stress response, chronic and persistent
inflammation, genetic and epigenetic changes, cytotoxicity and
fibrosis (2,19). At the same time, research has shown
that asbestos exposure and smoking have a synergistic effect to
increase the risk of lung cancer (1,20,22).
However, the current synergy between tobacco smoke and asbestos
exposure, and the specific mechanism for its induction of lung
cancer is not entirely clear. This mechanism may be related to
improving chemical carcinogens, promoting the absorption of
carcinogens in smoke, chronic inflammation and promoting tumor
proliferation (19,20). In addition to asbestos exposure,
there is now good evidence that lung cancer is linked to the
exposure to arsenic, chromium, and paint, diesel and welding fumes
(2,23).
Infectious or non-infectious respiratory
disease
Some diseases of the respiratory tract, including
chronic obstructive pulmonary disease (COPD) (chronic bronchitis,
emphysema), pneumonia, tuberculosis and asthma, and the occurrence
of lung cancer also have a certain relationship. Both COPD and
asthma are chronic airway inflammatory diseases. The former is an
irreversible change, while the latter is mainly manifested by
airway hyper-responsiveness (2).
Published meta-analyses have shown that patients with COPD and
asthma have an increased risk of lung cancer, and that patients
with a history of COPD have a 2-3 times higher risk of the cancer
(2,24,25).
The mechanism behind this may be related to long-term inflammation
in the respiratory tract. At present, several mechanisms have been
suggested: i) Ciliary dysfunction caused by COPD may lead to longer
exposure to carcinogens in the airway; ii) inflammatory responses
can damage DNA and lead to mutations; and iii) oxidative stress
responses can also damage DNA and lead to mutations (26,27).
Pneumonia, tuberculosis and other infectious lung diseases can also
increase the risk of lung cancer (25,28).
The mechanism of pneumonia-induced lung cancer may be related to
substances in chronic local inflammatory mediators, which can lead
to DNA damage mutations, signal transduction and
neovascularization. Tuberculosis, on the other hand, can induce
inflammation and fibrosis, changes that can lead to a higher
mutation rate (28), and a pooled
analysis found that a history of tuberculosis increased the risk of
lung cancer by 48% (29).
Inherited genetics
Among the causes of lung cancer, environmental
factors (such as smoking) are the most important (3), but genetic variation accounts for
12-21% of the risk of lung cancer (30,31).
Over the past few decades, genome-wide association studies (GWASs)
have certified a variety of genetic risk factors connected with
lung cancer susceptibility (32,33).
GWASs have also identified 45 lung cancer risk loci in different
populations (34). Based on a
large-scale GWAS of lung cancer, 6 new loci of variation were
identified and 13 previously reported mutations associated with the
development of NSCLC were validated (34). It is of great importance to
understand the relationship between genetics and lung cancer, and
to predict the risk of lung cancer for individual prevention and
the screening of lung cancer.
3. Diagnosis of NSCLC
The diagnostic methods of NSCLC could be roughly
divided into imaging examination, lung biopsy and biomarker
examination. Each test has its own advantages and disadvantages.
The pathological biopsy of lung tissue is the gold standard for the
diagnosis of NSCLC.
Imaging examination
Computed tomography (CT) is more effective than
plain radiographs in detecting peripheral lung lesions, but is less
sensitive to centrally located tumors (35,36).
In patients with suspected metastatic lung cancer, positron
emission tomography is a non-invasive examination that can be used
in addition to a routine chest CT scan. The two together are more
effective than either approach alone. As a relatively inexpensive
and non-invasive test, a CT scan has become the preferred method of
lung cancer screening (37,38).
Lung biopsy
Biopsies are the gold standard for the diagnosis of
malignant tumors, as they have a very high accuracy and can be used
to determine the subtype of lung cancer, which is of great
significance for diagnosis and treatment (39). There are several techniques
available through which physicians can obtain tissue specimens,
including bronchoscopy, transthoracic needle aspiration, surgical
excision biopsy and pleural effusion puncture (Fig. 1). Experiments show that for
patients with peripheral lung cancer, pleural aspiration is more
sensitive than bronchoscopy (40).
However, these methods are expensive and prone to complications
(39).
Biomarkers
Sputum cytology is an adjunctive examination that is
highly sensitive to tumors in the larger bronchi and less sensitive
to peripheral tumors. The sensitivity of sputum cytology to early
lung cancer is 20-30% (41). The
role of plasma microRNA in the early detection of lung cancer has
been investigated. Studies have shown differences in the miRNAs in
the plasma of patients with lung cancer compared with healthy
individuals (42). The role of
microRNA biomarkers in sputum samples has also been explored and
found to be helpful in the diagnosis of lung cancer (43).
Bronchoalveolar lavage (BAL) is another method of
using molecular markers to diagnose lung cancer by pathological
analysis of the cells obtained. Some studies have compared tumor
and BAL cells with lung cancer molecular markers and found that
they have high sensitivity. The exact genes related to
tumorigenesis can be found in BAL samples. Therefore, it is of
positive significance to study these molecular markers for the
early diagnosis of tumors (44).
Peripheral blood and urine specimens are readily
available and are non-invasive. With advances in technology, it has
been found that the amount of DNA in the blood and urine of
patients with cancer is approximately four times higher than the
amount of free DNA in healthy individuals. Urine also has some
potential with regard to the detection of biomarkers for lung
cancer, such as volatile organic compounds (VOCs). While VOCs are
promising, more clinical studies are needed to prove their
usefulness (45).
Biomarkers are easy to obtain, so it is currently
the direction of early lung cancer diagnosis research. Biomarkers
are not limited to the aforementioned sputum cytology, BAL and
peripheral blood and urine specimens, so more clinical studies to
verify the role of biomarkers in the early diagnosis of lung cancer
are required.
For patients diagnosed with advanced NSCLC,
biomarkers derived from blood or other tissues are also needed to
guide tumor treatment. The detection of biomarkers is of great help
to precision treatment and to the improvement of the therapeutic
effect (46). The European Society
for Medical Oncology (ESMO) Clinical Practice Guidelines recommend
routine testing for ALK, ROS1and EGFR. Meanwhile, in 2018, the ESMO
and the Chinese Society of Clinical Oncology jointly issued
Pan-Asian guidelines recommending routine testing for ALK
rearrangement, EGFR mutation, BRAF mutation, ROS1 rearrangement and
programmed cell death-ligand 1 (PD-L1) immunohistochemistry for
patients with advanced NSCLC (47,48).
In addition to conventional biomarkers activating HER2 mutations
(49), MET exon 14 skipping
mutations (50) and RET
rearrangements (51) may also be
present in NSCLC. Detection of NTRK gene rearrangements and KRAS
mutations is also of some value (52,53).
In general, all patients with advanced NSCLS should be routinely
tested for at least the ROS1 rearrangements, and ALK and EGFR
mutations. PD-L1, RET, MET, HER2 and KRAS and BRAF mutations and
immunohistochemistry should also be evaluated in a broader search
for affected genes.
4. Treatment of NSCLC
Lung cancer can be divided into SCLC and NSCLC. The
main treatment methods include surgery, drug therapy (chemotherapy,
targeted therapy and immunotherapy), radiotherapy, and a
combination of several treatments (e.g., chemotherapy combined with
immunotherapy or surgery, radiotherapy or targeted therapy)
(54-57). The choice of specific treatment is
related to the type and stage of cancer, and although there are
numerous treatment methods, except for that in a few local cancer
types, the treatment effect of other therapies is mostly poor.
Treatment of stage I and stage II
NSCLC
The main and best treatment for early lung cancer is
surgery (58). Although
platinum-assisted chemotherapy is recommended for stage II NSCLC
and increases the survival rate by 5 years, recurrence rates and
toxicity are high (59).
Postoperative adjuvant chemotherapy has not been proven to be
beneficial for stage I patients. Molecular targeted therapy for
early lung cancer also has no obvious therapeutic effect; it may
also lead to early entry into the ranks of those with advanced
cancer (59).
Treatment of stage III NSCLC
In total, >70% of patients with NSCLC are
diagnosed with advanced stage disease (60), and treatment for these patients
often depends on the location of the tumor and whether it can be
resected. Some patients in stage IIIA have operable disease, for
which the standard treatment is surgery and chemotherapy. Studies
have shown that adjuvant chemotherapy can prolong overall survival
(OS) rates, and that neoadjuvant chemotherapy can increase the
5-year survival rate by 5-6%. For patients with inoperable stage
IIIA and IIIB disease, the standard of care consists of sequential
or concurrent chemotherapy and radiation therapy (54,55,61,62).
Treatment of stage IV NSCLC
Stage IV NSCLC accounts for 40% of cases. The choice
of treatment is influenced by a variety of factors (such as
physical condition, whether the tumor is metastatic and whether it
is sensitive to radiotherapy and chemotherapy) and the specific
standard regimen includes palliative external radiotherapy,
combination chemotherapy, combination chemotherapy with targeted
therapy, and other treatments that may alleviate the patient's
symptoms. Surgical treatment may be used in some cases to relieve
symptoms, but is not the preferred treatment (56).
Targeted therapy
Targeted therapy has a positive effect on improving
the prognosis of patients with advanced NSCLC. Inhibitors targeting
alterations in certain genes (EGFR, ALK, ROS1, RET, BRAF V600E,
MET14 exons and NTRK) are currently certified for the treatment of
patients with NSCLC (63). These
drugs can improve the median OS and progression-free survival (PFS)
times of patients (64).
Immunotherapy has also been shown to benefit survival in patients
with advanced NSCLC by improving OS time (65,66).
Immunotherapy
Immunotherapy alone is generally better than
first-line chemotherapy for tumors with high expression of PD-L1.
No matter how PD-L1 is expressed in the tumor, combination
therapies of chemotherapy and immunotherapy have also been proved
to be superior to chemotherapy (57). For patients with advanced squamous
cell carcinoma or non-squamous cell carcinoma without
contraindications to programmed death 1/PD-L1 inhibitors,
monotherapy or combination therapy is now the standard first-line
treatment (63). In KEYNOTE-024, a
phase III randomized trial comparing the efficacy of pembrolizumab
monotherapy with platinum chemotherapy in patients with untreated
stage IV NSCLC, pembrolizumab monotherapy was found to be superior
to chemotherapy in terms of response rate (44.8 vs. 27.8%) and OS
time [median OS, 30.0 months (95% CI, 18.3-not reached) vs. 14.2
months (95% CI, 9.8 vs. 19.0) (57).
5. EGFR and inhibition of the EGFR pathway
in NSCLC
EGFR, also referred to as human EGF receptor-1
(HER-1), is a member of the HER/erbB family of receptor tyrosine
kinases (67,68); it is a multi-domain glycoprotein
consisting of an extracellular ligand binding domain, a hydrophobic
transmembrane domain and a cytoplasmic domain containing a tyrosine
kinase domain (67,69). Currently, the possible mechanisms
behind EGFR leading to malignant phenotypes include EGFR
overexpression and increased EGFR signaling pathway activity. Based
on the fact that EGFR is upregulated in numerous tumors, we can
speculate that increased expression of EGFR-mediated signaling
pathways may promote the initiation of unregulated cell
proliferation, leading to the emergence of a malignant phenotype
(70). EGFR pathway activation is
mainly due to endogenous ligands, such as EGF, TGF-α, epiregulin or
heparin-binding EGF, which bind to the extracellular domain of EGFR
and form dimers (67-69,71,72).
His dimerization activates the cytoplasmic EGFR tyrosine kinase,
leading to autophosphorylation, and the phosphorylated EGFR
tyrosine kinase regulates cell proliferation and apoptosis by
stimulating downstream intracellular signal transduction cascades
through several pathways (73).
EGFR is associated with the formation and development of a number
of tumors. Solid tumors such as breast, colon and non-small cell
carcinoma express EGFR, and EGFR is also involved in the occurrence
and development of tumors (68,71).
The activation of the EGFR pathway is associated with the
metastasis, proliferation, differentiation and migration of tumor
cells (68). EGFR mutations occur
in 7-37% of Caucasian patients and 40-60% of Asian patients with
NSCLC (74).
Cetuximab and panitumumab
Cetuximab and panitumumab are antibodies that bind
to the extracellular domain of EGFR, inhibit receptor activation
and block signal transduction (75,76).
A study of patients treated with locally advanced squamous cell
carcinoma of the head and neck showed that patients receiving
cetuximab plus radiotherapy experienced an improvement in median
survival time by nearly 20 months compared with patients treated
with radiotherapy alone (77). In
addition, cetuximab combined with gemcitabine has shown a
significant clinical response in the treatment of pancreatic cancer
(78). Cetuximab combined with
docetaxel also has certain beneficial clinical activity in the
second-line treatment of NSCLC. Based on this phenomenon, a further
study is evaluating the use of cetuximab in combination with
chemotherapeutic agents in first-line treatment of NSCLC (79).
EGFR tyrosine kinase inhibitors
(TKIs)
EGFR TKIs are small molecules that bind to the
cytoplasmic domain of EGFR containing the tyrosine kinase domain to
inhibit EGFR autophosphorylation, thus inhibiting receptor
activation and signal transduction. EGFR TKIs include erlotinib and
gefitinib (first generation), afatinib and dacomitinib (second
generation), and osimertinib and vandetanib (third generation)
(4).
6. VEGF and inhibition of the VEGF pathway
in NSCLC
Angiogenesis, the formation of new blood vessels,
plays an important role in human life activities. Angiogenesis is
regulated by both antiangiogenic factors and pro-angiogenic factors
(71,80). VEGF belongs to the platelet-derived
growth factor family, including VEGF-A, B, C and D (81). VEGF-A is a main stimulator in
angiogenesis, and its expression is of great significance to the
tissue angiogenesis system. Other family members are involved in
lymphatic angiogenesis and embryo angiogenesis (82-84).
In patients with cancer, tumor cells secrete VEGF, which forms new
blood vessels by acting on endothelial cells in existing blood
vessels and promoting their migration (71). The genesis of this pathological
blood vessel provides a pathway for tumor growth and metastasis
(85). VEGF mainly binds to VEGF
receptor 1 and VEGF receptor 2, and the receptor is made up of
extracellular, transmembrane and intracellular domains. Studies
have shown that the binding ability of VEGF with VEGF receptor 2 is
lower than that of VEGF1, but VEGF receptor 2 has been shown to be
the primary receptor for VEGF signaling in endothelial cells and to
play a key role in angiogenesis. After the binding of VEGF and VEGF
receptor 2, a dimer is formed, resulting in a phosphorylated
activation pathway that promotes endothelial cell proliferation and
angiogenesis (82,86,87).
The expression of VEGF is affected by a number of
factors, EGF receptor 2, methylation, transforming growth factor
(TGF)-α and β, and TNF-α, among which oxygen tension is the most
important for pathological angiogenesis (88,89).
Hypoxia can rapidly induce VEGF mRNA expression through
hypoxia-inducible factor-1 (HIF-1), thus promoting downstream
signal transduction (90). In a
normal oxygen tension environment, HIF-1 is degraded and
downregulated (82), while in a
hypoxic environment, the HIF-1 degradation pathway is blocked
(90) and HIF-1 is phosphorylated
through an oncogenic signal, thus binding to the promoter of the
VEGF gene, promoting the transcription of VEGF genes and
participating in angiogenesis. Hypoxia may be the most important
regulator of VEGF mRNA expression (91,92).
The activation of the VEGF pathway can act on existing vascular
endothelial cells to promote their migration, thus forming new
blood vessels and promoting tumor growth (71). There are several targeted drugs
that inhibit VEGF pathway expression, including some that bind to
the intracellular domain of VEGFR-2, such as vandetanib,
nintedanib, axitinib, cediranib and ramucirumab, a monoclonal
antibody that binds to the extracellular domain of VEGFR-2 and a
monoclonal antibody (bevacizumab) that inhibits VEGF-A protein. The
targeted therapies inhibit angiogenesis and tumor growth by binding
to VEGF and inhibiting its activity (93).
In the treatment of NSCLC, EGFR inhibition is an
important therapeutic strategy, and the inhibition of the VEGF
pathway is an important potential complementary target (81). EGF and VEGF share a common
downstream signaling pathway and may play an independent role in
tumorigenesis. Various ligands bind to EGFR and VEGF-2 to trigger
activation of both PI3K/AKT and RAS/RAF/ERK pathways. At the same
time, EGFR activation can promote the expression of the VEGF gene,
which is involved in HIF-1 upregulation (4).
7. Dual-inhibition of EGFR-VEGF
EGFR- or VEGF-targeted drugs have been shown to be
effective in the treatment of NSCLC, but have limited therapeutic
effects when used alone. As aforementioned, cetuximab in
combination with chemotherapeutic agents is more effective than the
chemotherapeutic agents alone. However, the combination of
different targeted agents may be more useful in improving the
efficacy and may avoid the safety and tolerability problems
associated with the use of chemotherapeutic agents compared with
the combination of chemotherapy agents (94). At the same time, there are also
drug resistance, escape of certain targets and other problems. The
activation of the EGFR pathway can promote HIF-1 production, thus
upregulating VEGF expression. However, an EGFR inhibitor alone
cannot completely block the production of VEGF, as the expression
of VEGF is affected by numerous factors, and it is impossible to
completely inhibit the release of VEGF in the interstitium.
Therefore, the effect of an EGFR inhibitor alone is not sufficient
(4,94). Several studies have also shown that
tumor cell resistance to EGFR inhibitors is related to increased
VEGF levels, and that this overexpression increases tumor cell
resistance (95,96). VEGF expression can promote
angiogenesis, and as the disease progresses, the pro-angiogenesis
pathway increases, and the dependence of tumor cells on VEGF may
decrease (97). Some tumors drive
pericyte activation through PDGF receptors, showing VEGF-resistance
through an escape mechanism, as this process is not VEGF-dependent
in endothelial cells (97-99). To address these concerns, the
combined use of EGFR inhibitors and VEGF inhibitors may help
(Fig. 2).
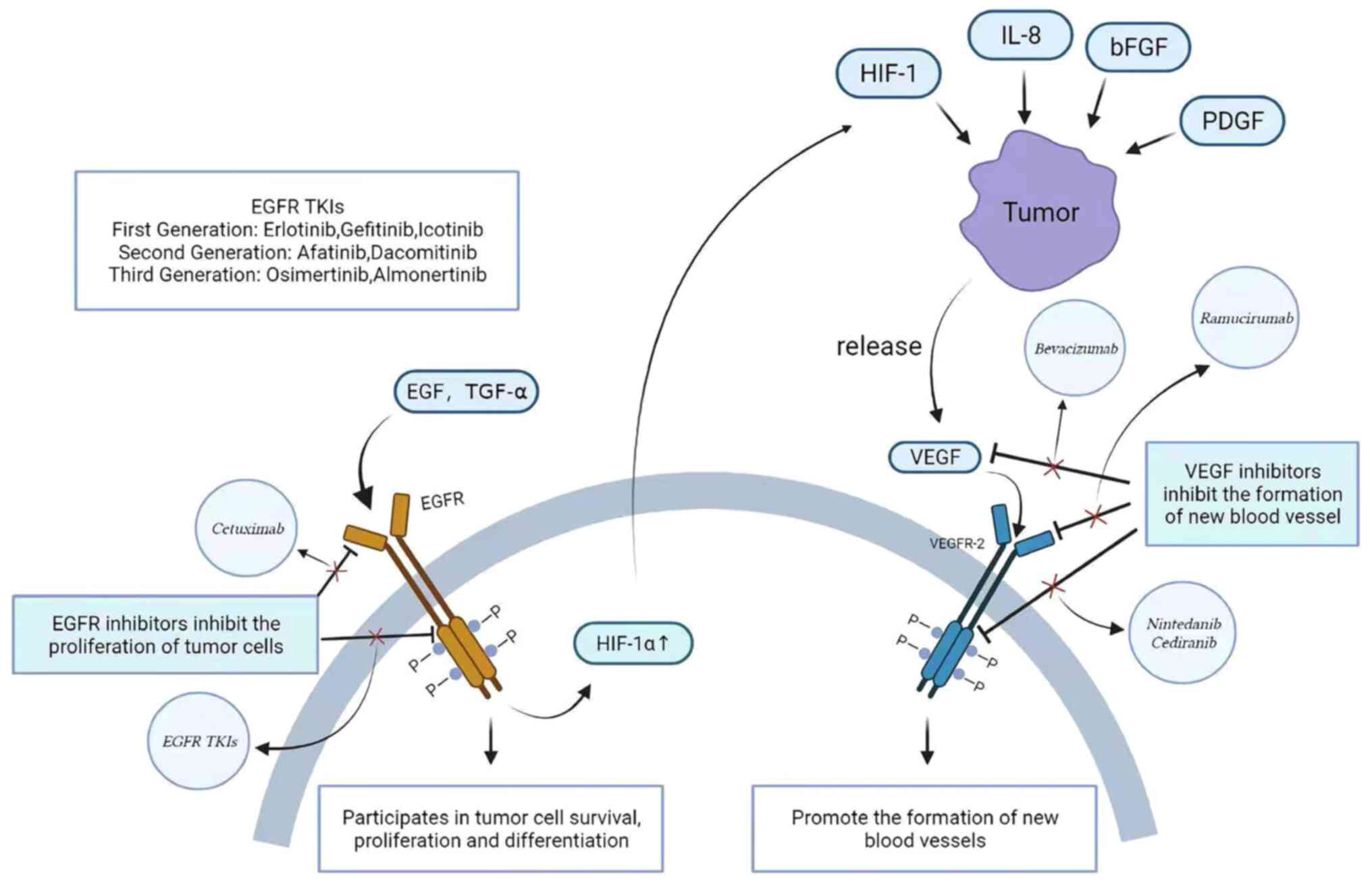 | Figure 2Association and inhibition of EGFR
and VEGF pathways. EGFR is activated when EGF and TGF-α bind to it
and is involved in the growth, proliferation and differentiation of
tumor cells through the conduction of downstream pathways. After
EGFR activation, HIF-1 can be upregulated, resulting in VEGF gene
expression. HIF-1, IL-8, bFGF and PDGF can promote the release of
VEGF by tumors, thereby activating the VEGF pathway and promoting
the formation of new blood vessels. Drugs targeting the EGFR and
VEGF pathways are also used clinically, including EGFR inhibitors
and VEGF-2 inhibitors. EGFR binds to the intracellular domain of
EGFR cell TKIs (erlotinib, gefitinib, icotinib, dacomitinib,
afatinib, almonertinib and osimertinib). Mechanisms of VEGF
inhibitors include interference with VEGF (bevacizumab), binding to
VEGFR-2 intracellular domains (nintedanib and cediranib) and
interfering with VEGFR-2 extracellular domains (ramucirumab). The
use of EGFR inhibitors can downregulate HIF-1 expression, but the
activation of the VEGF pathway is affected by a variety of factors,
so EGFR inhibitors alone are not effective in the treatment of
advanced non-small cell lung cancer. TKI, tyrosine kinase
inhibitor; HIF-1, hypoxia-inducible factor. |
8. Advantages of dual inhibition of
EGFR-VEGF
Dual inhibition resists acquired
resistance of tumor cells to EGFR inhibitors
As aforementioned, simple EGFR inhibitors cannot
completely prevent VEGF from promoting angiogenesis, and the
overexpression of VEGF can also cause the drug resistance of tumor
cells to EGFR inhibitors. Several studies have also demonstrated
this phenomenon. Long-term administration of EGFR inhibitors in
mice with colon cancer showed that mice could produce
drug-resistant colon cancer cell lines with VEGF overexpression,
which could make tumor cells resistant to EGFR inhibitors. As VEGF
levels increased, tumor angiogenesis potential also increased
(96). If a treatment requires
EGFR inhibitors, a combination of VEGF inhibitors is needed to
inhibit angiogenesis. Combination therapy is more effective than
blocking a single pathway, and may also help overcome tumor
resistance mechanisms.
Dual inhibition increases PFS times
The JO25567 trial of 154 Japanese patients, showed
that erlotinib combined with bevacizumab compared with erlotinib
alone exhibited a significantly increased PFS time (median PFS
time, 16.0 vs. 9.7 months; HR, 0.54; P=0.0015) (100). The phase 3 NEJ026 trial also
evaluated erlotinib alone and erlotinib with bevacizumab in
patients with complete NSCLC with EGFR mutation. The results showed
that the combination of erlotinib and bevacizumab increased the PFS
time (16.9 vs. 13.3 months; HR, 0.605; P=0.016) (101). Erlotinib + ramucirumab vs.
erlotinib + placebo was evaluated in the phase 3 RELAY trial, which
showed a significant increase in PFS time for the erlotinib +
ramucirumab group (median PFS, 19.4 vs. 12.4 months; HR, 0.59;
P<0.0001) (64). In a
randomized controlled trial meta-analysis of 1,918 patients with
advanced NSCLC, the dual inhibition of EGFR and VEGF pathways
significantly improved the PFS time (HR, 0.71; 95% CI, 0.58-0.86;
P<0.001) (102). A
meta-analysis comparing the efficacy of targeted combination
therapy vs. erlotinib alone in advanced NSCLC showed that the
combination therapy significantly improved the OS time (HR, 0.90;
95% CI, 0.82-0.99; P=0.024), PFS time (HR, 0.83; 95% CI, 0.72-0.97;
P=0.018) and overall response rate (OR, 1.35; 95% CI, 1.01-1.80;
P=0.04) in 2,417 patients (103)
(Table I). Based on these data,
the combination of EGFR and VEGF inhibitors can significantly
increase PFS time. The National Comprehensive Cancer Network
Clinical Practice Guidelines for Oncology has identified erlotinib
plus ramucirumab and erlotinib plus bevacizumab as first-line
therapies for EGFR-mutated NSCLC (101).
 | Table IClinical results after double
inhibition of EGFR-VEGF and related meta-analysis results. |
Table I
Clinical results after double
inhibition of EGFR-VEGF and related meta-analysis results.
| First author,
year | Study | Test area | Sample size, n | EGFR inhibitor | Dual inhibition of
EGFR-VEGF | Median PFS (alone
vs. combined), months | PFS (hazard
ratio) | Added PFS time,
months | (Refs.) |
|---|
| Seto et
al | JO25567 trial,
phase 2 | Japan | 154 | Erlotinib | Erlotinib +
bevacizumab | 9.7 vs. 16.0 | 0.540 | 6.3 | (100) |
| Saito et
al | NEJ026 trial, phase
3 | Japan | 228 | Erlotinib | Erlotinib +
bevacizumab | 13.3 vs. 16.9 | 0.605 | 3.5 | (101) |
| Nakagawa et
al | RELAY trial, phase
3 | Global | 449 | Erlotinib | Erlotinib +
ramucirumab | 12.4 vs. 19.4 | 0.590 | 7.0 | (64) |
| Qi et
al | Meta-analysis of 5
randomized controlled trials | / | 1736 | Erlotinib | Erlotinib +
ramucirumab | / | 0.63 | / | (103) |
| Zhanget
al | Meta-analysis of 4
randomized controlled trials | / | 1918 | EGFR-TKIs | EGFR-TKIs + VEGF
inhibitors | / | 0.71 | / | (102) |
9. Conclusions
EGF and VEGF have the same downstream signaling
pathway and play a very important role in tumor growth. EGFR
inhibitors alone cannot completely inhibit the
angiogenesis-promoting effect of VEGF, and the overexpression of
VEGF will also increase the resistance of tumor cells to EGFR
inhibitors, so the combination of drugs becomes a good choice. A
large body of data has shown that dual inhibition of EGFR and VEGF
pathways significantly reduces tumor cell resistance to EGFR
inhibitors and improves PFS time compared with EGFR inhibitors
alone. Under the support and guidance of a large number of clinical
trials, the pathways and targets that are not yet understood will
be solved one by one. The dual inhibition of EGFR-VEGF in the
treatment of advanced NSCLC applied to a greater extent, which will
be of great help to improve the survival of patients. Of course,
the double inhibition of the EGFR-VEGF pathway has also been
applied in other malignant tumors (such as colorectal, head and
neck, and breast cancer), but the use of EGFR-VEGF dual inhibition
in the treatment of tumors such as breast cancer, gastrointestinal
cancer, renal cancer, and head and neck tumors, is limited by the
lack of clinical trials. The field of combination therapy for NSCLC
with EGFR mutation is still being studied, and solutions to adverse
reactions (such as renal dysfunction) and cost increases after
double inhibition are also being actively sought. It is believed
that in the future, double inhibition to treat EGFR mutations in
NSCLC and other tumors associated with the EGFR-VEGF pathway will
be more widely used in clinical practice.
Availability of data and materials
Not applicable.
Authors' contributions
LS and MZ designed the research and were responsible
for the project conception. QW and AZ drafted the manuscript. LS
and MZ revised the manuscript. All authors read and approved the
final version of the manuscript. Data authentication is not
applicable.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
All authors declare that they have no competing
interests.
Acknowledgments
Not applicable.
Funding
This study was supported by the Foundation of the Xinglin
Project of Chengdu University of Traditional Chinese Medicine
(grant no. MPRC2021012).
References
|
1
|
Bade BC and Dela Cruz CS: Lung cancer
2020: Epidemiology, etiology, and prevention. Clin Chest Med.
41:1–24. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Schabath MB and Cote ML: Cancer progress
and priorities: Lung cancer. Cancer Epidemiol Biomarkers Prev.
28:1563–1579. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Bray F, Ferlay J, Soerjomataram I, Siegel
RL, Torre LA and Jemal A: Global cancer statistics 2018: GLOBOCAN
estimates of incidence and mortality worldwide for 36 cancers in
185 countries. CA Cancer J Clin. 68:394–424. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Le X, Nilsson M, Goldman J, Reck M,
Nakagawa K, Kato T, Ares LP, Frimodt-Moller B, Wolff K,
Visseren-Grul C, et al: Dual EGFR-VEGF pathway inhibition: A
promising strategy for patients with EGFR-Mutant NSCLC. J Thorac
Oncol. 16:205–215. 2021. View Article : Google Scholar
|
|
5
|
de Sousa VML and Carvalho L: Heterogeneity
in lung cancer. Pathobiology. 85:96–107. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Sousa V, Espírito Santo J, Silva M, Cabral
T, Alarcão AM, Gomes A, Couceiro P and Carvalho L: EGFR/erB-1,
HER2/erB-2, CK7, LP34, Ki67 and P53 expression in preneoplastic
lesions of bronchial epithelium: An immunohistochemical and genetic
study. Virchows Arch. 458:571–581. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Thun MJ: Early landmark studies of smoking
and lung cancer. Lancet Oncol. 11:12002010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Warren GW, Alberg AJ, Kraft AS and
Cummings KM: The 2014 surgeon general's report: 'The health
consequences of smoking-50 years of progress ': A paradigm shift in
cancer care. Cancer. 120:1914–1916. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Alberg AJ, Brock MV, Ford JG, Samet JM and
Spivack SD: Epidemiology of lung cancer: Diagnosis and management
of lung cancer, 3rd ed: American college of chest physicians
evidence-based clinical practice guidelines. Chest. 143(5 Suppl):
e1S–e29S. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Peto J: That the effects of smoking should
be measured in pack-years: Misconceptions 4. Br J Cancer.
107:406–407. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
IARC Working Group on the Evaluation of
Carcinogenic Risks to Humans: Tobacco smoke and involuntary
smoking. IARC Monogr Eval Carcinog Risks Hum. 83:1–1438.
2004.PubMed/NCBI
|
|
12
|
Murphy SE, Palomino A, Hecht SS and
Hoffmann D: Dose-response study of DNA and hemoglobin adduct
formation by 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanone in F344
rats. Cancer Res. 50:5446–5452. 1990.PubMed/NCBI
|
|
13
|
Jalas JR, McIntee EJ, Kenney PM, Upadhyaya
P, Peterson LA and Hecht SS: Stereospecific deuterium substitution
attenuates the tumorigenicity and metabolism of the
tobacco-specific nitrosamine
4-(methylnitrosamino)-1-(3-pyridyl)-1-butanone (NNK). Dose-response
study of DNA and hemoglobin adduct formation by
4-(methylnitrosamino)-1-(3-pyridyl)-1-butanone in F344 rats. Chem
Res Toxicol. 16:794–806. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Hecht SS: Progress and challenges in
selected areas of tobacco carcinogenesis. Chem Res Toxicol.
21:160–171. 2008. View Article : Google Scholar
|
|
15
|
Gibbons DL, Byers LA and Kurie JM:
Smoking, p53 mutation, and lung cancer. Mol Cancer Res. 12:3–13.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Brennan P, Buffler PA, Reynolds P, Wu AH,
Wichmann HE, Agudo A, Pershagen G, Jöckel KH, Benhamou S, Greenberg
RS, et al: Secondhand smoke exposure in adulthood and risk of lung
cancer among never smokers: A pooled analysis of two large studies.
Int J Cancer. 109:125–131. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Hori M, Tanaka H, Wakai K, Sasazuki S and
Katanoda K: Secondhand smoke exposure and risk of lung cancer in
Japan: A systematic review and meta-analysis of epidemiologic
studies. Jpn J Clin Oncol. 46:942–951. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Heloma A, Jaakkola MS, Kähkönen E and
Reijula K: The short-term impact of national smoke-free workplace
legislation on passive smoking and tobacco use. Am J Public Health.
91:1416–1418. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Klebe S, Leigh J, Henderson DW and
Nurminen M: Asbestos, smoking and lung cancer: An update. Int J
Environ Res Public Health. 17:2582019. View Article : Google Scholar
|
|
20
|
Ngamwong Y, Tangamornsuksan W, Lohitnavy
O, Chaiyakunapruk N, Scholfield CN, Reisfeld B and Lohitnavy M:
Additive synergism between asbestos and smoking in lung cancer
risk: A systematic review and meta-analysis. PLoS One.
10:e01357982015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Villeneuve PJ, Parent MÉ, Harris SA and
Johnson KC; Canadian Cancer Registries Epidemiology Research Group:
Occupational exposure to asbestos and lung cancer in men: Evidence
from a population-based case-control study in eight Canadian
provinces. BMC Cancer. 12:5952012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Topinka JB, Loli P, Dusinská M, Hurbánková
M, Kováciková Z, Volkovová K, Kazimírová A, Barancoková M, Tatrai
E, Wolff T, et al: Mutagenesis by man-made mineral fibres in the
lung of rats. Mutat Res. 595:174–183. 2006. View Article : Google Scholar
|
|
23
|
Ketfi A, Zanoun N, Laouedj I, Gharnaout M
and Fraga S: Primary lung cancer and occupational exposure in a
North African population. Pan Afr Med J. 37:1202020.In French.
|
|
24
|
Zhang X, Jiang N, Wang L, Liu H and He R:
Chronic obstructive pulmonary disease and risk of lung cancer: A
meta-analysis of prospective cohort studies. Oncotarget.
8:78044–78056. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Qu YL, Liu J, Zhang LX, Wu CM, Chu AJ, Wen
BL, Ma C, Yan XY, Zhang X, Wang DM, et al: Asthma and the risk of
lung cancer: A meta-analysis. Oncotarget. 8:11614–11620. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Bozinovski S, Vlahos R, Anthony D,
McQualter J, Anderson G, Irving L and Steinfort D: COPD and
squamous cell lung cancer: Aberrant inflammation and immunity is
the common link. Br J Pharmacol. 173:635–648. 2016. View Article : Google Scholar :
|
|
27
|
Ghosh A, Boucher RC and Tarran R: Airway
hydration and COPD. Cell Mol Life Sci. 72:3637–3652. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Keikha M and Esfahani BN: The relationship
between tuberculosis and lung cancer. Adv Biomed Res. 7:582018.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Brenner DR, McLaughlin JR and Hung RJ:
Previous lung diseases and lung cancer risk: A systematic review
and meta-analysis. PLoS One. 6:e174792011. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Wang C, Zhu M, Zhou W, Du J, Xiang Y, Shu
XO, Hu Z, Zhou W, Chen K, Xu J, et al: Estimation of heritability
for nine common cancers using data from genome-wide association
studies in Chinese population. Int J Cancer. 140:329–336. 2017.
View Article : Google Scholar :
|
|
31
|
Sampson JN, Wheeler WA, Yeager M,
Panagiotou O, Wang Z, Berndt SI, Lan Q, Abnet CC, Amundadottir LT,
Figueroa JD, et al: Analysis of heritability and shared
heritability based on genome-wide association studies for thirteen
cancer types. J Natl Cancer Inst. 107:djv2792015. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
McKay JD, Hung RJ, Han Y, Zong X,
Carreras-Torres R, Christiani DC, Caporaso NE, Johansson M, Xiao X,
Li Y, et al: Large-scale association analysis identifies new lung
cancer susceptibility loci and heterogeneity in genetic
susceptibility across histological subtypes. Nat Genet 4.
9:1126–1132. 2017. View Article : Google Scholar
|
|
33
|
Bossé Y and Amos CI: A decade of GWAS
results in lung cancer. Cancer Epidemiol Biomarkers Prev.
27:363–379. 2018. View Article : Google Scholar
|
|
34
|
Dai J, Lv J, Zhu M, Wang Y, Qin N, Ma H,
He YQ, Zhang R, Tan W, Fan J, et al: Identification of risk loci
and a polygenic risk score for lung cancer: A large-scale
prospective cohort study in Chinese populations. Lancet Respir Med.
7:881–891. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Sobue T, Moriyama N, Kaneko M, Kusumoto M,
Kobayashi T, Tsuchiya R, Kakinuma R, Ohmatsu H, Nagai K, Nishiyama
H, et al: Screening for lung cancer with low-dose helical computed
tomography: Anti-lung cancer association project. J Clin Oncol.
20:911–920. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Toyoda Y, Nakayama T, Kusunoki Y, Iso H
and Suzuki T: Sensitivity and specificity of lung cancer screening
using chest low-dose computed tomography. Br J Cancer.
98:1602–1607. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Lardinois D, Weder W, Hany TF, Kamel EM,
Korom S, Seifert B, von Schulthess GK and Steinert HC: Staging of
non-small-cell lung cancer with integrated positron-emission
tomography and computed tomography. N Engl J Med. 348:2500–2507.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Guhlmann A, Storck M, Kotzerke J, Moog F,
Sunder-Plassmann L and Reske SN: Lymph node staging in non-small
cell lung cancer: Evaluation by [18F]FDG positron emission
tomography (PET). Thorax. 52:438–441. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Hirsch FR, Prindiville SA, Miller YE,
Franklin WA, Dempsey EC, Murphy JR, Bunn PA Jr and Kennedy TC:
Fluorescence versus white-light bronchoscopy for detection of
preneoplastic lesions: A randomized study. J Natl Cancer Inst.
93:1385–1391. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Arroliga AC and Matthay RA: The role of
bronchoscopy in lung cancer. Clin Chest Med. 14:87–98. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Risse EK, Vooijs GP and van't Hof MA:
Relationship between the cellular composition of sputum and the
cytologic diagnosis of lung cancer. Acta Cytol. 31:170–176.
1987.PubMed/NCBI
|
|
42
|
Tsoulos N, Papadopoulou E, Metaxa-Mariatou
V, Tsaousis G, Efstathiadou C, Tounta G, Scapeti A, Bourkoula E,
Zarogoulidis P, Pentheroudakis G, et al: Tumor molecular profiling
of NSCLC patients using next generation sequencing. Oncol Rep.
38:3419–3429. 2017.PubMed/NCBI
|
|
43
|
Xie Y, Todd NW, Liu Z, Zhan M, Fang H,
Peng H, Alattar M, Deepak J, Stass SA and Jiang F: Altered miRNA
expression in sputum for diagnosis of non-small cell lung cancer.
Lung Cancer 6. 7:170–176. 2010. View Article : Google Scholar
|
|
44
|
Spira A, Beane JE, Shah V, Steiling K, Liu
G, Schembri F, Gilman S, Dumas YM, Calner P, Sebastiani P, et al:
Airway epithelial gene expression in the diagnostic evaluation of
smokers with suspect lung cancer. Nat Med. 13:361–366. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Rotunno M, Hu N, Su H, Wang C, Goldstein
AM, Bergen AW, Consonni D, Pesatori AC, Bertazzi PA, Wacholder S,
et al: A gene expression signature from peripheral whole blood for
stage I lung adenocarcinoma. Cancer Prev Res (Phila). 4:1599–1608.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Pennell NA, Arcila ME, Gandara DR and West
H: Biomarker testing for patients with advanced non-small cell lung
cancer: Real-world issues and tough choices. Am Soc Clin Oncol Educ
Book. 39:531–542. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Planchard D, Popat S, Kerr K, Novello S,
Smit EF, Faivre-Finn C, Mok TS, Reck M, Van Schil PE, Hellmann MD,
et al: Metastatic non-small cell lung cancer: ESMO clinical
practice guidelines for diagnosis, treatment and follow-up. Ann
Oncol. 29(Suppl 4): iv192–iv237. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Wu YL, Planchard D, Lu S, Sun H, Yamamoto
N, Kim DW, Tan DSW, Yang JC, Azrif M, Mitsudomi T, et al: Pan-Asian
adapted clinical practice guidelines for the management of patients
with metastatic non-small-cell lung cancer: A CSCO-ESMO initiative
endorsed by JSMO, KSMO, MOS, SSO and TOS. Ann Oncol. 30:171–210.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Li BT, Ross DS, Aisner DL, Chaft JE, Hsu
M, Kako SL, Kris MG, Varella-Garcia M and Arcila ME: HER2
amplification and HER2 mutation are distinct molecular targets in
lung cancers. J Thorac Oncol. 11:414–419. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Reungwetwattana T, Liang Y, Zhu V and Ou
SI: The race to target MET exon 14 skipping alterations in
non-small cell lung cancer: The why, the how, the who, the unknown,
and the inevitable. Lung Cancer. 103:27–37. 2017. View Article : Google Scholar
|
|
51
|
Subbiah V, Velcheti V, Tuch BB, Ebata K,
Busaidy NL, Cabanillas ME, Wirth LJ, Stock S, Smith S, Lauriault V,
et al: Selective RET kinase inhibition for patients with
RET-altered cancers. Ann Oncol. 29:1869–1876. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Cocco E, Scaltriti M and Drilon A: NTRK
fusion-positive cancers and TRK inhibitor therapy. Nat Rev Clin
Oncol. 15:731–747. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Ferrer I, Zugazagoitia J, Herbertz S, John
W, Paz-Ares L and Schmid-Bindert G: KRAS-mutant non-small cell lung
cancer: From biology to therapy. Lung Cancer. 124:53–64. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Edell ES and Cortese DA: Photodynamic
therapy in the management of early superficial squamous cell
carcinoma as an alternative to surgical resection. Chest.
102:1319–1322. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Hotta K, Matsuo K, Ueoka H, Kiura K,
Tabata M and Tanimoto M: Role of adjuvant chemotherapy in patients
with resected non-small-cell lung cancer: Reappraisal with a
meta-analysis of randomized controlled trials. J Clin Oncol.
22:3860–3867. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Lemjabbar-Alaoui H, Hassan OU, Yang YW and
Buchanan P: Lung cancer: Biology and treatment options. Biochim
Biophys Acta. 1856:189–210. 2015.PubMed/NCBI
|
|
57
|
Reck M, Rodríguez-Abreu D, Robinson AG,
Hui R, Csőszi T, Fülöp A, Gottfried M, Peled N, Tafreshi A, Cuffe
S, et al: Pembrolizumab versus chemotherapy for PD-L1-positive
non-small-cell lung cancer. N Engl J Med. 375:1823–1833. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Sangha R, Price J and Butts CA: Adjuvant
therapy in non-small cell lung cancer: Current and future
directions. Oncologist. 15:862–872. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Pignon JP, Tribodet H, Scagliotti GV,
Douillard JY, Shepherd FA, Stephens RJ, Dunant A, Torri V, Rosell
R, Seymour L, et al: Lung adjuvant cisplatin evaluation: A pooled
analysis by the LACE collaborative group. J Clin Oncol.
26:3552–3559. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Travis WD, Brambilla E and Riely GJ: New
pathologic classification of lung cancer: Relevance for clinical
practice and clinical trials. J Clin Oncol. 31:992–1001. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Scagliotti GV, Fossati R, Torri V, Crinò
L, Giaccone G, Silvano G, Martelli M, Clerici M, Cognetti F and
Tonato M; Adjuvant Lung Project Italy/European Organisation for
Research Treatment of Cancer-Lung Cancer Cooperative Group
Investigators: Randomized study of adjuvant chemotherapy for
completely resected stage I, II, or IIIA non-small-cell Lung
cancer. J Natl Cancer Inst. 95:1453–1461. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Winton T, Livingston R, Johnson D, Rigas
J, Johnston M, Butts C, Cormier Y, Goss G, Inculet R, Vallieres E,
et al: Vinorelbine plus cisplatin vs observation in resected
non-small-cell lung cancer. N Engl J Med. 352:2589–2597. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Alexander M, Kim SY and Cheng H: Update
2020: Management of non-small cell lung cancer. Lung. 198:897–907.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Nakagawa K, Garon EB, Seto T, Nishio M,
Ponce Aix S, Paz-Ares L, Chiu CH, Park K, Novello S, Nadal E, et
al: Ramucirumab plus erlotinib in patients with untreated,
EGFR-mutated, advanced non-small-cell lung cancer (RELAY): A
randomised, double-blind, placebo-controlled, phase 3 trial. Lancet
Oncol. 20:1655–1669. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Gray JE, Villegas A, Daniel D, Vicente D,
Murakami S, Hui R, Kurata T, Chiappori A, Lee KH, Cho BC, et al:
Three-year overall survival with durvalumab after chemoradiotherapy
in stage III NSCLC-update from PACIFIC. J Thorac Oncol. 15:288–293.
2020. View Article : Google Scholar
|
|
66
|
Antonia SJ, Villegas A, Daniel D, Vicente
D, Murakami S, Hui R, Yokoi T, Chiappori A, Lee KH, de Wit M, et
al: Durvalumab after chemoradiotherapy in stage III non-small-cell
lung cancer. N Engl J Med. 377:1919–1929. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Arteaga CL: The epidermal growth factor
receptor: From mutant oncogene in nonhuman cancers to therapeutic
target in human neoplasia. J Clin Oncol. 19(Suppl 18): 32S–40S.
2001.PubMed/NCBI
|
|
68
|
Yarden Y and Sliwkowski MX: Untangling the
ErbB signalling network. Nat Rev Mol Cell Biol. 2:127–137. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Herbst RS: Review of epidermal growth
factor receptor biology. Int J Radiat Oncol Biol Phys. 59(Suppl 2):
S21–S26. 2004. View Article : Google Scholar
|
|
70
|
Laskin JJ and Sandler AB: Epidermal growth
factor receptor inhibitors in lung cancer therapy. Semin Respir
Crit Care Med. 25(Suppl 1): S17–S27. 2004. View Article : Google Scholar
|
|
71
|
Ellis LM: Epidermal growth factor receptor
in tumor angiogenesis. Hematol Oncol Clin North Am. 18:1007–1021.
viii2004. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Salomon DS, Brandt R, Ciardiello F and
Normanno N: Epidermal growth factor-related peptides and their
receptors in human malignancies. Crit Rev Oncol Hematol.
19:183–232. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Hirsch FR, Scagliotti GV, Langer CJ,
Varella-Garcia M and Franklin WA: Epidermal growth factor family of
receptors in preneoplasia and lung cancer: Perspectives for
targeted therapies. Lung Cancer. 41(Suppl 1): S29–S42. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Midha A, Dearden S and McCormack R: EGFR
mutation incidence in non-small-cell lung cancer of adenocarcinoma
histology: A systematic review and global map by ethnicity
(mutMapII). Am J Cancer Res. 5:2892–2911. 2015.PubMed/NCBI
|
|
75
|
Goldstein NI, Prewett M, Zuklys K,
Rockwell P and Mendelsohn J: Biological efficacy of a chimeric
antibody to the epidermal growth factor receptor in a human tumor
xenograft model. Clin Cancer Res. 1:1311–1318. 1995.PubMed/NCBI
|
|
76
|
Prewett M, Rothman M, Waksal H, Feldman M,
Bander NH and Hicklin DJ: Mouse-human chimeric anti-epidermal
growth factor receptor antibody C225 inhibits the growth of human
renal cell carcinoma xenografts in nude mice. Clin Cancer Res.
4:2957–2966. 1998.PubMed/NCBI
|
|
77
|
Bonner JA, Harari PM, Giralt J, Azarnia N,
Shin DM, Cohen RB, Jones CU, Sur R, Raben D, Jassem J, et al:
Radiotherapy plus cetuximab for squamous-cell carcinoma of the head
and neck. N Engl J Med. 354:567–578. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Xiong HQ, Rosenberg A, LoBuglio A, Schmidt
W, Wolff RA, Deutsch J, Needle M and Abbruzzese JL: Cetuximab, a
monoclonal antibody targeting the epidermal growth factor receptor,
in combination with gemcitabine for advanced pancreatic cancer: A
multicenter phase II Trial. J Clin Oncol. 22:2610–2616. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Kim ES: Cetuximab as a single agent or in
combination with chemotherapy in lung cancer. Clin Lung Cancer.
6(Suppl 2): S80–S84. 2004. View Article : Google Scholar
|
|
80
|
Carmeliet P: Angiogenesis in health and
disease. Nat Med. 9:653–660. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Ferrara N and Adamis AP: Ten years of
anti-vascular endothelial growth factor therapy. Nat Rev Drug
Discov. 15:385–403. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Ferrara N, Gerber HP and LeCouter J: The
biology of VEGF and its receptors. Nat Med. 9:669–676. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Karkkainen MJ, Mäkinen T and Alitalo K:
Lymphatic endothelium: A new frontier of metastasis research. Nat
Cell Biol. 4:E2–E5. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Melincovici CS, Boşca AB, Şuşman S,
Mărginean M, Mihu C, Istrate M, Moldovan IM, Roman AL and Mihu CM:
Vascular endothelial growth factor (VEGF)-key factor in normal and
pathological angiogenesis. Rom J Morphol Embryol. 59:455–467.
2018.
|
|
85
|
Folkman J: Tumor angiogenesis: Therapeutic
implications. N Engl J Med. 285:1182–1186. 1971. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Gille H, Kowalski J, Li B, LeCouter J,
Moffat B, Zioncheck TF, Pelletier N and Ferrara N: Analysis of
biological effects and signaling properties of Flt-1 (VEGFR-1) and
KDR (VEGFR-2). A reassessment using novel receptor-specific
vascular endothelial growth factor mutants. J Biol Chem.
276:3222–3230. 2001. View Article : Google Scholar
|
|
87
|
Muñoz-Chápuli R, Quesada AR and Angel
Medina M: Angiogenesis and signal transduction in endothelial
cells. Cell Mol Life Sci. 61:2224–2243. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Roengvoraphoj M, Tsongalis GJ, Dragnev KH
and Rigas JR: Epidermal growth factor receptor tyrosine kinase
inhibitors as initial therapy for non-small cell lung cancer: Focus
on epidermal growth factor receptor mutation testing and
mutation-positive patients. Cancer Treat Rev. 39:839–850. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Li N, Zeng A, Wang Q, Chen M, Zhu S and
Song L: Regulatory function of DNA methylation mediated lncRNAs in
gastric cancer. Cancer Cell Int. 22:2272022. View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Tammela T, Enholm B, Alitalo K and
Paavonen K: The biology of vascular endothelial growth factors.
Cardiovasc Res. 65:550–563. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Ferrara N: Role of vascular endothelial
growth factor in physiologic and pathologic angiogenesis:
Therapeutic implications. Semin Oncol. 29(Suppl 6): S10–S14. 2002.
View Article : Google Scholar
|
|
92
|
Longo R, Sarmiento R, Fanelli M,
Capaccetti B, Gattuso D and Gasparini G: Anti-angiogenic therapy:
Rationale, challenges and clinical studies. Angiogenesis.
5:237–256. 2002. View Article : Google Scholar
|
|
93
|
Manzo A, Montanino A, Carillio G, Costanzo
R, Sandomenico C, Normanno N, Piccirillo MC, Daniele G, Perrone F,
Rocco G and Morabito A: Angiogenesis inhibitors in NSCLC. Int J Mol
Sci. 18:20212017. View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Tabernero J: The role of VEGF and EGFR
inhibition: Implications for combining anti-VEGF and anti-EGFR
agents. Mol Cancer Res. 5:203–220. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
95
|
Vallböhmer D, Zhang W, Gordon M, Yang DY,
Yun J, Press OA, Rhodes KE, Sherrod AE, Iqbal S, Danenberg KD, et
al: Molecular determinants of cetuximab efficacy. J Clin Oncol.
23:3536–3544. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Viloria-Petit A, Crombet T, Jothy S,
Hicklin D, Bohlen P, Schlaeppi JM, Rak J and Kerbel RS: Acquired
resistance to the antitumor effect of epidermal growth factor
receptor-blocking antibodies in vivo: A role for altered tumor
angiogenesis. Cancer Res. 61:5090–5101. 2001.PubMed/NCBI
|
|
97
|
Rak J, Yu JL, Kerbel RS and Coomber BL:
What do oncogenic mutations have to do with angiogenesis/vascular
dependence of tumors? Cancer Res. 62:1931–1934. 2002.PubMed/NCBI
|
|
98
|
Bergers G, Song S, Meyer-Morse N,
Bergsland E and Hanahan D: Benefits of targeting both pericytes and
endothelial cells in the tumor vasculature with kinase inhibitors.
J Clin Invest. 111:1287–1295. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
99
|
Viloria-Petit AM and Kerbel RS: Acquired
resistance to EGFR inhibitors: Mechanisms and prevention
strategies. Int J Radiat Oncol Biol Phys. 58:914–926. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Seto T, Kato T, Nishio M, Goto K, Atagi S,
Hosomi Y, Yamamoto N, Hida T, Maemondo M, Nakagawa K, et al:
Erlotinib alone or with bevacizumab as first-line therapy in
patients with advanced non-squamous non-small-cell lung cancer
harbouring EGFR mutations (JO25567): An open-label, randomised,
multicentre, phase 2 study. Lancet Oncol. 15:1236–1244. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
101
|
Saito H, Fukuhara T, Furuya N, Watanabe K,
Sugawara S, Iwasawa S, Tsunezuka Y, Yamaguchi O, Okada M, Yoshimori
K, et al: Erlotinib plus bevacizumab versus erlotinib alone in
patients with EGFR-positive advanced non-squamous non-small-cell
lung cancer (NEJ026): Interim analysis of an open-label,
randomised, multicentre, phase 3 trial. Lancet Oncol. 20:625–635.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Zhang TT, Wang RM, Yang Z and Chen GB:
Dual inhibiting EGFR and VEGF pathways versus EGFR-TKIs alone in
the treatment of advanced non-small-cell lung cancer: A
meta-analysis of randomized controlled trials. Clin Transl Oncol.
18:576–581. 2016. View Article : Google Scholar
|
|
103
|
Qi WX, Wang Q, Jiang YL, Sun YJ, Tang LN,
He AN, Min DL, Lin F, Shen Z and Yao Y: Overall survival benefits
for combining targeted therapy as second-line treatment for
advanced non-small-cell-lung cancer: A meta-analysis of published
data. PLoS One. 8:e556372013. View Article : Google Scholar : PubMed/NCBI
|