Introduction
With the significant advancement in diagnostic
modalities and treatment options, providing care for patients with
cancer has become increasingly complex. Input from various
disciplines and specialties has become crucial for appropriate
patient management (1,2). Multidisciplinary tumor boards (MDT)
are a forum where several physicians from different specialties,
meet to review and discuss the diagnosis, medical condition, and
management of patients with cancer (3,4).
This collaboration provides an opportunity for experts from
different specialties and expertise to pool and complement each
other's experience and inputs (5-8).
Disciplines include medical oncology, radiation oncology,
radiology, pathology, surgery, among others. Although the
multidisciplinary approach in treatment of patients with cancer was
first described in 1975, it was not until the late 1990s when it
was formally implemented into the care of patients with cancer
(2). Several factors affect the
MDT discussions, including the meeting's structure, time
management, and expert leadership (1). More recently, the technological
advances, on one hand, and the COVID-19 pandemic, on the other,
have facilitated the collaboration among tumor boards' members
through virtual online and hybrid (live and online) meetings
(2,9,10).
MDT have been considered the optimal model for
management of patients with cancer. They are generally utilized in
large academic centers and in specialized cancer care centers,
including developing countries (2,9,11-13).
A survey that included 338 oncology specialists from developing
Arab countries showed that 60% of physicians resorted to MDT in
order to seek the medical opinion of their colleagues to help with
the management of their patients with cancer (14). Another survey conducted by the
American Society of Clinical Oncology (ASCO) included 501 ASCO
members. A total of 96% of respondents reported that the benefit of
MDT outweighs the time and effort spent and that changes in surgery
type and/or treatment plans generally occur in 25 to 50% of
patients (11). Moreover, in a
prospective cohort study that included patients with lung and
esophageal cancer, MDT changed the treatment plan in 40% of
patients and the staging and assessment plans in 60% of patients.
Upon follow-up on patients, recommendations were followed in 97% of
the cases (15). On the other
hand, a survey by Keating et al (16) reported only little association
between MDT and cancer care quality and survival and stressed the
importance of improving the quality of tumor boards
discussions.
The Thoracic MDT at the American University of
Beirut Medical Center (AUBMC) is a weekly meeting that has been
taking place since 2015. In order to assess the impact of thoracic
MDTs, their utilization and efficacy, a retrospective study was
conducted to review the process of thoracic MDTs, their plans of
therapy, and changes in diagnosis and treatment plans for patients
with cancer.
Materials and methods
This was a retrospective study that comprised a
chart review for all patients with cancer who were presented in the
thoracic MDTs at AUBMC over the period of one year, from January 1,
2021, until December 31, 2021. The study coordinators reviewed the
electronic medical charts for all patients presented over this
period. They filled the ‘Data Entry Form’, provided in Tables SI and SII, which consists of 3 pages, namely
data available in the chart prior to case presentation, data
available after the tumor board presentation, and case discussion
evaluation. In addition, study coordinators filled the patients'
log sheet where each patient was provided by a study code. All
information filled was treated as confidential. All of the analysis
was performed using SPSS statistical software (version 23; IBM
Corp.).
The MDTs are composed of members from the various
specialties, including radiology, radiation-oncology, pulmonary
medicine, thoracic surgery, pathology, in addition to medical
oncology. At least one representative physician from each specialty
should have been present in order for the MDTs discussion to be
held. MDTs occurred on a weekly basis. The patients could be shared
with other physicians, and the documentation of discussion was kept
in the medical chart of the presented patients and accessible by
all treating physicians who take care of the patient from the
various departments. Discussion items that physicians included
during MDTs were the presenting symptoms, revision of images,
revision of prior treatment regimens, role of surgery, radiation
therapy, and/or systemic therapy, among other pertinent items that
arose during the discussion.
Data was obtained from the clinic chart and the
hospital admission charts. These data were included in the page for
data before case presentation in the data entry sheet: i) Clinical
data related to the patient's cancer (brief history and physical
findings) and ii) Other data (pertinent lab findings, radiological
findings, pathology, diagnosis, and TNM stage). The primary outcome
measure was the percentage of patients presented at the thoracic
MDT who had a change in their treatment plan after the
presentation.
The present study was approved (approval no.
BIO-2022-0049) by the Institutional Review Board (IRB) at AUBMC
(Beirut, Lebanon). All measures to maintain confidentiality were
taken, including a password protected database that is managed by
the investigators. Patients were anonymized by using a log sheet as
there was no need to include the patients' names in the data entry
sheet. All records were stored in a locked file cabinet in the
office of the principal investigator. Only the principal
investigator and the study coordinators have access to the cabinet.
Data will be stored for 5 years after which it will be shredded.
Patients were not contacted by the study coordinators at any point,
and the study consisted only of retrospective chart review.
Results
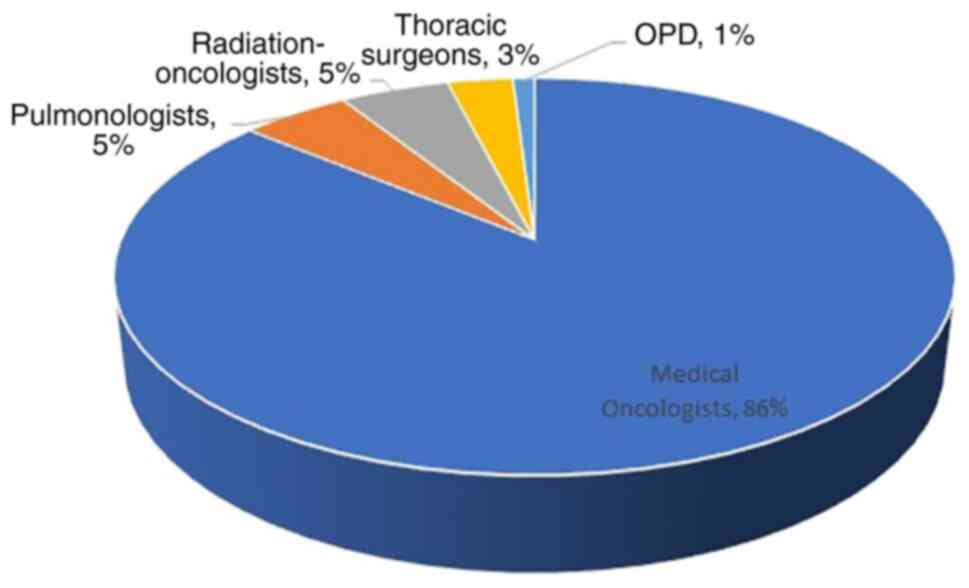
A total of 214 cases were scheduled for thoracic MDT
during the study period. Of these, 19 (8.9%) cases were scheduled
yet not presented. These were patients who were placed on the MDT
schedule before their imaging studies were uploaded on the
electronic health record system for revision during the MDT. A
total of 184 (86%) were scheduled by medical oncologists, 11 (5.1%)
by pulmonologists, 11 (5.1%) by radiation-oncologists and 7 (3.3%)
by thoracic surgeons. Only 1 case (0.5%) was scheduled by the
Outpatient Department (OPD) team, which is an outpatient clinic led
by clinical fellows in-training, that offers ambulatory cancer care
to patients with limited income and with minimal charges (Fig. 1). 189 (88.32%) cases were for
patients with primary lung cancer, while the remaining cases
consisted of patients with head and neck cancer, lung metastasis
from other primary cancers, or carcinoma of unknown primary. The
distribution of cases across the 12 months of the year was
homogeneous, ranging from 4.2% for March and 4.7% for December to
the greatest percentage of cases scheduled, 13.1%, for the month of
July. A total of 87 (44.6%) cases had the stage at diagnosis
specified, 69 (79.3%) of which were stage III or IV.
Of the 214 cases scheduled, the majority, 132
(61.7%) did not have a treatment plan before presenting in the MDT
(Table I). When it was observed
whether the treatment plan and/or diagnosis were changed after
presentation in MDT, of the 195 cases presented, only 43 (22.0%)
did not have a change in their plan, while almost half of the cases
presented, 88 (45.2%), had a change in their treatment plan. These
changes included recommending observation in 21 (10.8%) cases,
radiation therapy only in 11 (5.6%) cases, systemic therapy only in
26 (13.3%) cases, and both, radiation therapy and systemic therapy,
in 14 (7.2%) cases. A total of 16 (8.2%) cases were recommended to
have surgery combined with other treatments, namely systemic
therapy and radiation therapy. A total of 64 (32.8%) cases
consisted of discussion of the diagnosis during MDT with either
confirmation or modification of the patients' diagnosis (Table II).
 | Table ITreatment plan and diagnosis for
scheduled MDT cases. |
Table I
Treatment plan and diagnosis for
scheduled MDT cases.
| Treatment plan prior
to presentation | No treatment plan
prior to presentation | Total MDT
scheduled |
|---|
| 82 (38.3%) | 132 (61.7%) | 214 (100%) |
| Table IITreatment plan and diagnosis for
presented MDT cases. |
Table II
Treatment plan and diagnosis for
presented MDT cases.
| Change in treatment
plan | |
|---|
| 88 (45.2%) | |
|---|
| Observation | RT only | Systemic therapy
only | RT and systemic
therapy | Surgery with other
therapies | No change in
treatment plan | Discussion of
diagnosis | Total MDT
presented |
|---|
| 21
(10.8%*) | 11 (5.6%*) | 26
(13.3%*) | 14 (7.2%*) | 16 (8.2%*) | 43 (22.0%) | 64 (32.8%) | 195 (100%) |
A total of 3 (1.4%) cases were referred to
additional tumor boards for further discussion, 2 of which were
referred to the Gastrointestinal (GI) Oncology MDT and 1 of which
was referred to the radiation-oncology MDT. A total of 73 (34.1%)
cases recommended additional tests, which included tumor biopsy,
additional immunohistochemistry stains, molecular testing, lymph
node sampling, and PET-CT scan. Of the 195 cases that were
presented, the majority, 170 (87.2%), had their recommended
treatment plan implemented after the MDT discussion, while 8 (4.1%)
cases had a different treatment plan implemented after the MDT from
that decided upon during the MDT. It is worth noting that 17 (8.7%)
were lost to follow up. A total of 10 (4.7%) patients were not
alive on last follow up at AUBMC at the time of data collection,
while the majority, 204 (95.3%) were still alive on last follow
up.
A total of 148 (69.2%) cases had the MDT decision
documented by an MDT note only, while 16 (7.5%) cases had the
decision documented only through the primary physician office note
and 18 (8.4%) cases had the decision documented only through an
inpatient note. A total of 32 (15%) cases had their decisions
documented through more than one method, namely MDT note, office
note, and inpatient note. All cases that were scheduled yet not
documented had an MDT note documenting this.
There was no association between the presenting
physician, on one hand, and whether there was a treatment plan
prior to presentation or not (P=1.000), whether additional tests
were requested during the MDT (P=0.175), whether referral to
additional MDT was recommended (P=0.974), whether the plan was
changed during the MDT (P=0.310), on the other. There was, however,
an association between the stage of cancer at the time of
presentation and requesting additional tests (P=0.021), but there
was no association between the stage of cancer and change in
treatment plan (P=0.177) nor with implementation of recommendation
(P=0.217). While the majority of patients with stage I, III and IV,
did not require additional testing, with 81.8, 79.3, and 80%,
respectively, not requiring additional tests, almost half, 42.9%,
of those with stage II required additional tests as part of the MDT
recommendations. Notably, there was also an association between the
stage at presentation with scheduling yet not presenting a case
(P=0.029) and with diagnosis (P=0.001). Of the 19 cases that were
scheduled yet not presented, 6 cases did not specify the stage at
presentation, and 8 (42.1%) had stage IV disease. Also, among the
10 cases that were not primary lung cancer and whose stage was
specified, 6 (60%) were stage IV.
Discussion
Although our study was designed with the primary
objective of assessing changes of plans of patient management at
thoracic MDT, the main finding of the present study was that, at
our institution, the majority of multidisciplinary treatment plans
are, in fact, made at the MDT. The majority of cases did not have a
treatment plan before presentation in the MDT. Moreover, one-third
of the cases presented discussed the diagnosis during MDT with
either confirmation or modification of the patients' diagnosis on
presentation, in addition to the almost half of the cases presented
that had a change in their treatment plan. The present study showed
that thoracic MDT at AUBMC is used as a forum for group
multidisciplinary consultations for primary physicians that gives
them the opportunity to involve specialists from different
disciplines, including thoracic surgeons, pulmonologists, and
radiation oncologists. This is considered as a positive trend
towards improved integrative multidisciplinary care of patients
with lung cancer. It was noted from the present study that plans
made at the MDT did not only consist of systemic therapy but that
also 75.9% of cases had plans such as radiation therapy, surgery,
and systemic therapy, and 10.8% of cases had observation as the
primary recommendation following the discussion of the MDT
attendees. This indicated that the presence of attendees from
several disciplines, in addition to medical oncologists, can
contribute to recommendations that are not limited to systemic
therapy. Our data parallels current trends published in literature
for multidisciplinary management recommendations, including
radiation therapy and surgery, for almost all cases, for both
early-stage and metastatic lung cancer (5). Notably, almost half of presented
patients with stage II required additional tests as part of the MDT
recommendations with a statistically significant association. This
suggested that patients within this stage category, that is neither
considered very early not advanced disease, may need more
diagnostic tests conducted prior to presenting in MDT.
It was also noted that medical oncologists were more
likely to bring cases to the thoracic MDT than were pulmonologists,
thoracic surgeons or radiation oncologists. This may be due to
other obligations, including scheduled operations and sessions for
surgeons and radiation oncologists respectively. A prospective
observational survey by Kehl et al (7), from the Cancer Care Outcomes Research
and Surveillance Consortium (CanCORS), which assessed care patterns
of patients with lung and colorectal cancer, showed that surgeons
are less likely to attend weekly MDT than are medical oncologists
and radiation oncologists. The CanCORS study showed that regular
frequent physician attendance in MDT meetings was associated with
more clinical trial participation and with higher rates of
curative-intent surgery for early-stage non-small cell lung cancer,
but not with overall survival. In its exploratory subgroup
analysis, frequent MDT attendance was associated with enhanced
survival among patients with extensive small-cell lung cancer and
stage IV colorectal cancer.
The results from our institution revealed that the
use of MDT enhances the implementation of multidisciplinary
management of patients with cancer and should be helpful to health
care providers worldwide, including those practicing in remote
areas and in low- and middle-income countries. In a study by Saghir
et al (14), the authors
concluded that MDT are also beneficial rural areas or
limited-resources settings, where only a small group of specialists
is available. It was suggested that mini-tumor boards may still be
considered with whomever is available to make improved management
decisions and plans than when only the primary physician is
involved (3,14). In a study by Charara et al
(17) which prospectively
investigated the impact of MDT on cancer cases at AUBMC,
videoconferences were suggested by the authors at that time in 2017
in order to enhance multidisciplinary attendance. By the time the
present study was conducted for thoracic MDT, and due to the
COVID-19 pandemic, hybrid venues have been implemented over the
past 2 years, instead of the in-person only venue. This is similar
to regular educational MDT videoconferences that we usually conduct
at AUBMC with Memorial Sloan Kettering Cancer Center and with MD
Anderson Cancer Center (18,19).
Videoconference platform could, in fact, be a useful addition to
the live venue in circumstances where not all attendees can present
in-person. Current advances in technology allows video meetings and
virtual platforms to be made available, allowing all physicians,
including those practicing in remote areas, to render
multidisciplinary management plans for their patients (20).
El Saghir et al (21) conducted a survey for international
ASCO members. It was showed that improvement in the efficiency of
MDT is needed through more effective moderators of discussions,
improved time management at meetings, improved criteria for the
selection of cases, and the provision of written summaries of cases
to attendees can better reduce the time and resources needed for
MDT. Although medical oncologists presented the majority of cases
at our institution and thoracic surgeons presented the least number
of cases, surgeons were essential in discussions and final
management plans as seen in the cases where surgical management was
recommended. The study by Charara et al (17) not only showed that upfront
multidisciplinary decision making shall be considered as an
indicator of benefit from MDT but also that, similar to our data,
surgeons should be more involved in MDT (17). This differs from other institutions
where surgeons or radiation oncologists may lead the MDT. All
members of the multidisciplinary management team should be
considered as important contributors to the success of MDT and
should participate in cases preparation, presentation, discussion
of management plans. Adding cases and actively presenting them
should be viewed as important as the participation attendees other
than medical oncologists and shall expand multidisciplinary care to
patients with lung cancer at each institution.
A limitation to the present study is that its design
is retrospective. Retrospective studies are susceptible to
selection and memory bias. The included cases over the selected
period of time may not be representative of all thoracic cases and
reasons for non-selection may not be ascertainable. Moreover, MDT
conclusions may have been influenced by the presenting physicians,
who were from a variety of specialties. This may have resulted in
anchoring bias whereby the primary specialty of the presenting
physician could have influenced the discussion and decisions
made.
Furthermore, data available in the charts were not
collected for research purposes. As such, certain data may be
missing for some patients. This was observed in the lack of stage
on presentation of MDT in several cases, for example. Lack of
homogeneity is another concern in a retrospective design. Different
people are involved at different times in patient care and data
entry, particularly when studies look at charts over several months
such as the present study, which spanned 12 months. In addition,
neither survival in a retrospective design nor the reason behind
loss to follow-up can be determined. Reasons for lost follow-ups
often cannot be ascertained in retrospective studies and can
potentially bias the results as well. In the present study, 8.7% of
patients did not follow up at our institution after the MDT
discussion, which can be attributed to financial limitations and
limited ability of numerous patients to afford treatment. This has
recently become of particular significance in the setting of
socio-economic challenges that have faced patients in our community
over the past 2 years, particularly that our institution may be
considered a referral center in the region that may not always be
affordable to all socio-economic classes.
In conclusion, in the modern era of oncology
practice, multidisciplinary management of patients with lung cancer
ensues. The present data demonstrated that MDT are used to make
upfront management decisions. In addition to considering change in
management plans as an indicator of the benefit of MDT, it is
suggested that making upfront multidisciplinary plans for patient
management be considered an additional component of indicators of
the benefit of MDT. Although thoracic surgeons presented the least
number of cases at our MDT, they attended and actively participated
in discussions of diagnosis and management plans as seen in the
cases where surgical management was recommended. Utilizing hybrid
meetings enabled more attendees to join and, hence, enriches the
multidisciplinary discussions. Promoting multidisciplinary
teamwork, including greater participation by clinical fellows from
OPD, and more research are needed. The effects on management,
outcome, and survival should be assessed prospectively at various
centers and for different cancers.
Supplementary Material
Impact of thoracic multidisciplinary
Tumor Boards on management of patients with cancer
Impact of thoracic multidisciplinary
Tumor Boards on management of patients with cancer.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
FK and AT participated in data collection, analysis,
and manuscript writing. AT participated in the study design. Both
authors read and approved the final version of the manuscript. Both
authors confirm the authenticity of all the raw data.
Ethics approval and consent to
participate
The present study was approved (approval no.
BIO-2022-0049) by the Institutional Review Board at AUBMC (Beirut,
Lebanon). Informed oral consent was provided by all patients prior
to participation in the retrospective chart review.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
El Saghir NS, Keating NL, Carlson RW,
Khoury KE and Fallowfield L: Tumor boards: Optimizing the structure
and improving efficiency of multidisciplinary management of
patients with cancer worldwide. Am Soc Clin Oncol Ed Book.
e461–e466. 2014.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Specchia ML, Frisicale EM, Carini E, Di
Pilla A, Cappa D, Barbara A, Ricciardi W and Damiani G: The impact
of tumor board on cancer care: Evidence from an umbrella review.
BMC Health Serv Res. 20(73)2020.PubMed/NCBI View Article : Google Scholar
|
|
3
|
National Cancer Institute (NCI):
Dictionary of Cancer Terms: Tumor Board Review. https://www.cancer.gov/publications/dictionaries/cancer-terms/def/tumor-board-review.
|
|
4
|
Soukup T, Sevdalis N, Green JSA, Lamb BW,
Chapman C and Skolarus TA: Making tumor boards more
patient-centered: Let's start with the name. JCO Oncol Pract.
17:591–593. 2021.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Chang JH, Vines E, Bertsch H, Fraker DL,
Czerniecki BJ, Rosato EF, Lawton T, Conant EF, Orel SG, Schuchter
L, et al: The impact of a multidisciplinary breast cancer center on
recommendations for patient management: The University of
Pennsylvania experience. Cancer. 91:1231–1237. 2001.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Petty JK and Vetto JT: Beyond doughnuts:
Tumor board recommendations influence patient care. J Cancer Educ.
17:97–100. 2002.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Kehl KL, Landrum MB, Kahn KL, Gray SW,
Chen AB and Keating NL: Tumor board participation among physicians
caring for patients with lung or colorectal cancer. J Oncol Pract.
11:e267–e278. 2015.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Wong BO, Blythe JA, Wu A, Batten JN,
Kennedy KM, Kouaho AS and Wren SM: Exploration of clinician
perspectives on multidisciplinary tumor board function beyond
clinical decision-making. JAMA Oncol. 8:1210–1212. 2022.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Dharmarajan H, Anderson JL, Kim S,
Sridharan S, Duvvuri U, Ferris RL, Solari MG, Clump DA II, Skinner
HD, Ohr JP, et al: Transition to a virtual multidisciplinary tumor
board during the COVID-19 pandemic: University of Pittsburgh
experience. Head Neck. 42:1310–1316. 2020.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Blasi L, Bordonaro R, Serretta V, Piazza
D, Firenze A and Gebbia V: Virtual clinical and precision medicine
tumor boards-cloud-based platform-mediated implementation of
multidisciplinary reviews Among oncology centers in the COVID-19
Era: Protocol for an observational study. JMIR Res Protoc.
10(e26220)2021.PubMed/NCBI View
Article : Google Scholar
|
|
11
|
El Saghir NS, Charara RN, Kreidieh FY,
Eaton V, Litvin K, Farhat RA, Khoury KE, Breidy J, Tamim H and Eid
TA: Global practice and efficiency of multidisciplinary tumor
boards: Results of an American society of clinical oncology
International survey. J Glob Oncol. 1:57–64. 2015.PubMed/NCBI View Article : Google Scholar
|
|
12
|
El Saghir NS, Farhat RA, Charara RN and
Khoury KE: Enhancing cancer care in areas of limited resources: Our
next steps. Future Oncol. 10:1953–1965. 2014.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Mano MS, Çitaku FT and Barach P:
Implementing multidisciplinary tumor boards in oncology: A
narrative review. Future Oncol. 18:375–384. 2022.PubMed/NCBI View Article : Google Scholar
|
|
14
|
El Saghir NS, El-Asmar N, Hajj C, Eid T,
Khatib S, Bounedjar A, Ajarim D, Shamseddine A, Geara F, Jazieh A,
et al: Survey of utilization of multidisciplinary management tumor
boards in Arab countries. Breast. 20 (Suppl 2):S70–S74.
2011.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Schmidt HM, Roberts JM, Bodnar AM, Kunz S,
Kirtland SH, Koehler RP, Hubka M and Low DE: Thoracic
multidisciplinary tumor board routinely impacts therapeutic plans
in patients with lung and esophageal cancer: A prospective cohort
study. Ann Thorac Surg. 99:1719–1724. 2015.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Keating NL, Landrum MB, Lamont EB, Bozeman
SR, Shulman LN and McNeil BJ: Tumor boards and the quality of
cancer care. J Natl Cancer Inst. 105:113–121. 2013.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Charara RN, Kreidieh FY, Farhat RA,
Al-Feghali KA, Khoury KE, Haydar A, Nassar L, Berjawi G,
Shamseddine A and El Saghir NS: Practice and impact of
multidisciplinary tumor boards on patient management: A prospective
study. J Glob Oncol. 3:242–249. 2016.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Snyder A, Kemeny N, Shamseddine A,
Al-Olayan A, El-Merhi F, Kelsen DP, Jamali F, Sidani M, Mukherji D,
El-Naghy M, et al: Liver-directed conversion therapy in metastatic
colon cancer. J Gastrointest Oncol. 6:322–328. 2015.PubMed/NCBI View Article : Google Scholar
|
|
19
|
El Saghir N: ABC of Breast Diseases,
Awareness, Prevention, Treatment (ed 3). Beirut, Lebanon, Arab
Scientific Publishers,. 2013, pp 261-267, 2013. https://www.neelwafurat.com/itempage.aspx?id=lbb132751-92883&search=books.
|
|
20
|
Stevenson MM, Irwin T, Lowry T, Ahmed MZ,
Walden TL, Watson M and Sutton L: Development of a virtual
multidisciplinary lung cancer tumor board in a community setting. J
Oncol Pract. 9:e77–e80. 2013.PubMed/NCBI View Article : Google Scholar
|
|
21
|
El Saghir NS, Charana R, Eaton VJ, Litvin
K, Farhat R, Khoury K, Breidy J and Tamim H: ASCO Survey: Use and
efficiency of multidisciplinary tumor boards worldwide. Ann Oncol.
25(iv373)2014.
|