Introduction
Candida is a fungus that is indigenous to the oral
cavity. It has been proven that it is the most frequently observed
mycosis, carried by 15–60% of healthy individuals (1,2).
Although it may be present in the healthy organism it usually
causes no disorders. However, following the long-term use of
antibiotics, steroids or due to an overall decline in the immune
system function, it may multiply opportunistically and become
pathogenic (3).
Candidiasis may be classified as superficial or
deep. Superficial candidiasis appears in the oral cavity, vaginal
mucous membranes, skin and nails, whereas deep candidiasis appears
in the gastrointestinal and urinary tracts, lungs, heart and
cerebrospinal compartment. When severe, it may prove fatal. It is
considered that superficially located Candida may reach every organ
in the body via the blood stream or by way of the esophagus and
trachea. In addition, the oral cavity may provide access to the
alimentary tract and the lungs. Therefore, it is hypothesized that
superficial Candida in the oral cavity may be the cause of deep
candidiasis (4).
Previously, it was demonstrated that professional
oral care prevents fever caused by pneumonia in the elderly
(5). Furthermore, Kikuchi et
al (6) demonstrated in an
experiment on the elderly using isotopes that saliva from the oral
cavity constantly flows into the lungs. Therefore, it is critical
for the prevention of aspiration pneumonia to decrease the bacteria
and fungi in the oral cavity through oral hygiene. Candida is one
of the fungi that may cause aspiration pneumonia and there is a
possibility that Candida in the oral cavity descends into the lungs
and exacerbates pneumonia (7). As
regards denture candidiasis, it is hypothesized that dentures and
the multiplication of Candida are significantly associated.
Consequently, it is considered significant from the viewpoint of
oral care to elucidate the association between Candida and the
fitting surface of the denture (8).
A therapeutic trial was performed using miconazole
on a patient with dentures who suffered from oral candidiasis. A
microbiological examination for Candida was conducted in the
lesions, the inner side of the fitting surface of the denture and
material from the deep portions of the denture, confirming the
presence of Candida inside the denture material (9).
In the present study, to better understand candidal
contamination of denture materials, an experiment was performed by
adhering four species of Candida clinical strains onto samples of
denture material. The strains had been presumptively identified in
CHROMagar Candida culture medium (Chromaagar, Paris, France), which
has good selective property and is able to easily identify fungal
species (7,10). It was proven using scanning electron
microscopy that all four Candida species exhibited a tendency to
adhere to the denture material.
Materials and methods
Patients and specimens
The present study included 20 patients with dentures
who underwent medical examinations at the Dental and Oral Medical
Center, Kurume University Hospital. The patients provided written
informed consent in order to participate in the study. The study
protocol conformed to the ethical guidelines of the Declaration of
Helsinki as reflected by prior approval by the Institutional Ethics
Committee of the Kurume University School of Medicine. The patients
presented with white spots on the mucosal membrane, which were
diagnosed as oral candidiasis. The patients consented to sample
collection from their dentures for our experiments.
The subjects included 9 males and 11 females. Their
ages were as follows: 50–60 years, 1 patient; 60–70 years, 2
patients; 70–80 years, 5 patients; 80–90 years, 8 patients; and
>90 years, 4 patients. The average age of the subjects was 79.5
years. The main complaint of 11 subjects was a strange sensation in
their mouth; 5 subjects complained of a burning sensation on their
tongue; 2 complained of pseudomembrane formation; and the remaining
2 subjects complained of dental pain. In addition, all the subjects
suffered from oral candidiasis. As regards other complications, 18
subjects had suffered cerebral infarction, 17 had diabetes, 14 had
hypertension, 11 had heart disease, while other complications
included fractures of the pelvis or the collarbone. The subjects in
this study were mainly elderly individuals and had overlapping
underlying diseases. There was no administration of oral
antibiotics or use of steroids at the time of sample
collection.
Diagnosis of oral candidiasis was confirmed
following Candida detection in the lesions by microscopic
examination. Sixteen of these cases involved the dorsum of the
tongue, 2 involved the hard palate mucosa and the remaining 2 cases
the buccal mucosa. There was no evidence of candidiasis on the
upper or lower gums. As regards the type of dentures, our study was
limited to hot polymerized resin-based dentures, complete or
partial. Nine patients had both upper and lower dentures. One had
only an upper denture and the remaining 10 had lower dentures.
Experimental conditions
Experiment 1: Collection of clinical
Candida strains and identification of species
Sample collection. Samples were collected
from three locations (lesions, inside the fitting surface and deep
portions of the denture material) with the use of sterile swabs. As
regards the lesions, 16 samples were collected from the dorsal
mucosal membrane of the tongue, 2 from the hard palate mucosa and 2
from the buccal mucosa.
For lesions on the tongue or the buccal mucosa, 18
samples were collected from the nearest spot on the inside of the
fitting surface of the lower denture. For lesions on the hard
palate mucosa, 2 samples were collected from the fitting surface of
the upper denture close to the axle of the tooth crest of the
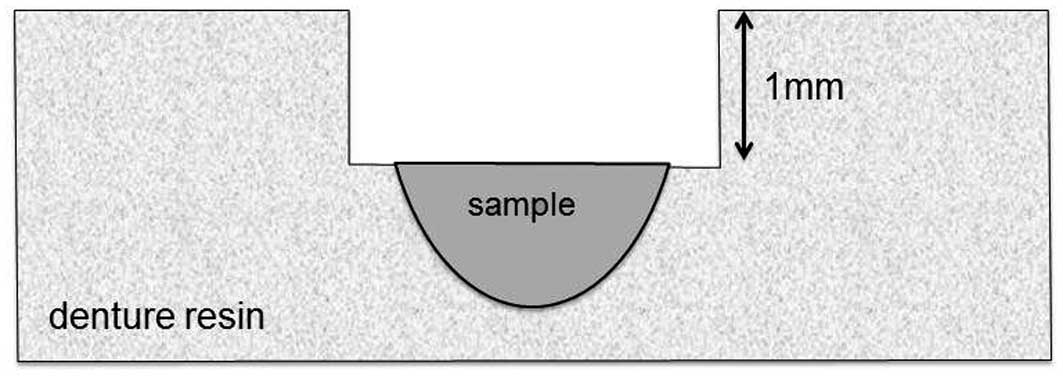
alveolar bone. In order to collect samples from the deep portions
of the denture material the following procedure was performed: the
denture was thoroughly washed with physiological saline solution.
Subsequently, ∼1 mm3 of material was milled out using a
round bur from the same location on the fitting surface where the
previous samples had been collected (Fig. 1). The material was then placed on
sterile cotton swabs soaked in physiological saline solution and
used as a sample. The milled out material was replaced by new
resin. It was decided that the collection of lesion and denture
samples should be performed on 1 of our patients only.
Isolation of Candida. Isolation of Candida
from the samples was performed with BBL™ CHROMagar™ Candida medium
(Becton Dickinson, Sparks, MD, USA) (10,11).
This medium was selected since each colony develops a specific
colorization that renders it readily identifiable. The samples were
then inoculated into the medium and aerobically cultured for 3 days
at 35°C.
Presence or absence of Candida and identification
of isolated strains. The presence of Candida was determined by
counting the number of colonies and then classifying them into 3
levels as follows: a, (1–100); b, (101–1,000); and c, (≥1,001). For
the identification of isolated strains, the API 20C Auxanogram kit
(Analytab Products, Inc., Systems SA, Marcy l’Etoile, France) was
used and the fungal species were identified by their biochemical
characteristics. The API 20C Auxanogram is a system consisting of
20 microtubes on a single plate with 19 dehydrated substrates used
in biochemical tests to identify the pathogenic yeast (12,13).
The medium was diluted by physiological saline
(0.85°C) with 2 drops of fungal liquid suspended in a concentration
of McFarland no. 2. It was then transferred by pipetting into the
microtubes to the horizontal level and incubated for 48–72 h at
30°C. The development of the fungus in each microtube was observed
and identifications were made using the positive rate table and
APILAB software. As regards low selectivity identification that
required microscopic morphology for confirmation, a slide culture
was conducted using Tween-80 combined with Corn Meal Agar.
Identification was based on these observations (14–16).
Experiment 2: Candida culture in the
medium with sample of denture resin
Cultures of isolate strains with denture
material. Sabouraud bouillon medium (10 ml) was used as a
multiplication medium in the test tubes. Samples were collected
from the resin base of the dentures from 1 patient by 3×5-mm
sections. For used dentures, 2 types of resin base samples were
prepared, 1 with and 1 without a fissure. Four Candida species were
used in this study, Candida albicans, Candida glabrata,
Candida tropicalis and Candida parapsilosis. Two test
tubes for each species were prepared by inoculating the Sabouraud
bouillon medium with the fungal colonies. The two types of resin
samples collected from the test denture material were placed into
the test tube medium and incubated while shaking for 14 h at 35°C.
Prior to incubation the test tubes and resin samples were cleaned
using an ultrasonic cleaner and sterilized.
Scanning electron microscope (SEM). To
conduct the SEM observation, the resin samples were removed from
the culture medium and fixed in 2% glutaraldehyde (100 mM phosphate
buffer, pH 7.2) for 1 h at 4°C. After washing in distilled water,
the samples were fixed in 2% osmic acid solution (100 mM phosphate
buffer, pH 7.2) for 5 min at 4°C. Subsequently, the resin samples
were dehydrated through a graded series of ethanols (50, 60, 70,
80, 90 and 100% for 15 min each). The ethanol was replaced with
tert-butyl-alcohol and the samples were freeze-dried for 12 h. The
samples were then capsule-coated with metal and used for scanning
electron microscopic observation, which was performed with the
S-800 SEM (Hitachi High-Technologies Corporation, Tokyo, Japan)
(17–19).
Results
Positive rates of Candida
The number of colonies were classified as: a,
(1–100); b, (101–1,000); and c, (≥1,001) and the association was
determined between the location from which the samples were
collected, the positive rate of fungus detection and the isolated
fungus. Irrespective of the species of isolated fungus, the
presence of Candida was confirmed in all the samples from the
lesions and the inner side of the denture fitting surface. The
presence of Candida was also observed in 60% of the samples
collected from the deeper portions of the denture material. The
association between the isolated fungi and the locations where they
were encountered were as follows: Candida albicans was the
most common, being detected in 54% of the lesions, 37% of the inner
sides of the fitting surfaces and 39% of the deep portions of the
denture base materials. The number of colonies was <100, which
was quite limited. Candida albicans ranked high among the
other species in each of the locations where Candida was detected.
All four species were present in all the samples collected from the
lesions, regardless of the location.
Moreover, as regards the inner side of the denture
fitting surfaces, Candida albicans was present in 51% and
Candida glabrata in 34% of samples. In the samples collected
from the deep portions of the denture materials, Candida
albicans was the most common with a detection rate of 61%,
whereas few other fungal species were identified (Table I).
 | Table I.Detection sites and rates for Candida
and number of colonies detected for each of the four species (C.
albicans, C. glabrata, C. parapsilosis, C.
tropicalis).a |
Table I.
Detection sites and rates for Candida
and number of colonies detected for each of the four species (C.
albicans, C. glabrata, C. parapsilosis, C.
tropicalis).a
| Species | Site [n/total
(detection rate)]
|
|---|
Lesions 20/20 (100%)
| Inner fitting surface
20/20 (100%)
| Deep portions of
denture resin 16/20 (80%)
|
|---|
| a | b | c | a | b | c | a | b | c |
|---|
| C.
albicans | 14 | 3 | 0 | 16 | 2 | 0 | 9 | 2 | 0 |
| C.
glabrata | 8 | 1 | 1 | 11 | 1 | 0 | 4 | 1 | 0 |
| C.
parapsilosis | 2 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 0 |
| C.
tropicalis | 1 | 1 | 0 | 2 | 1 | 0 | 1 | 1 | 0 |
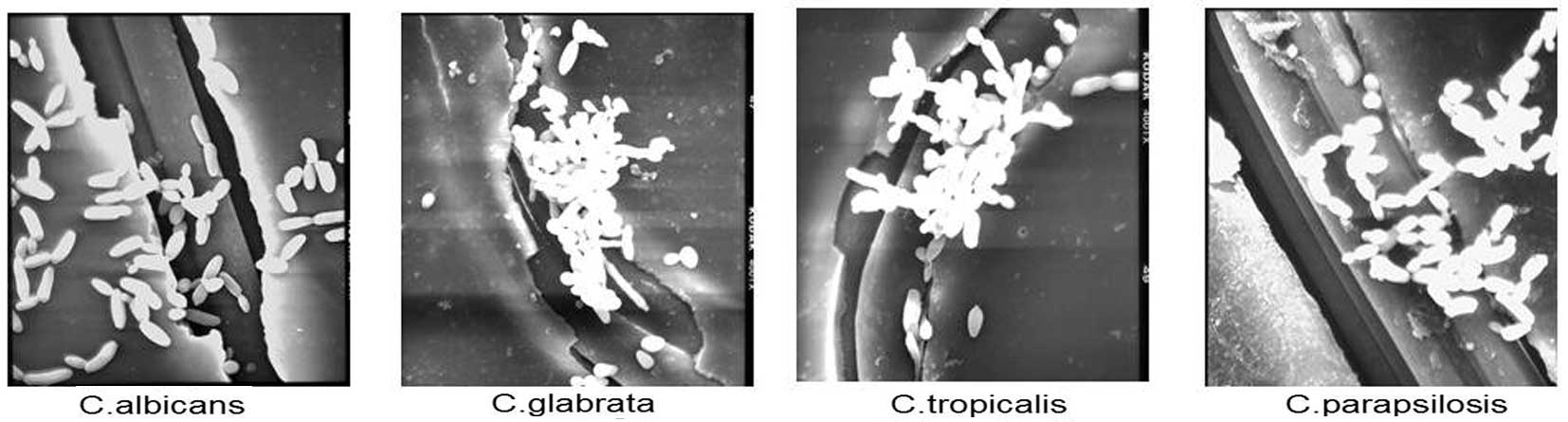
Results of SEM
The electron micrographs of Candida albicans,
Candida glabrata, Candida tropicalis and Candida
parapsilosis adhering onto the surface of the denture are shown
in Fig. 2. Yeasts of all four
species of Candida, whose shapes were either round (bulb) or oval
(elliptical) multiplied on the surface of the denture. No
differences in the size or shape of the fungi were detected in the
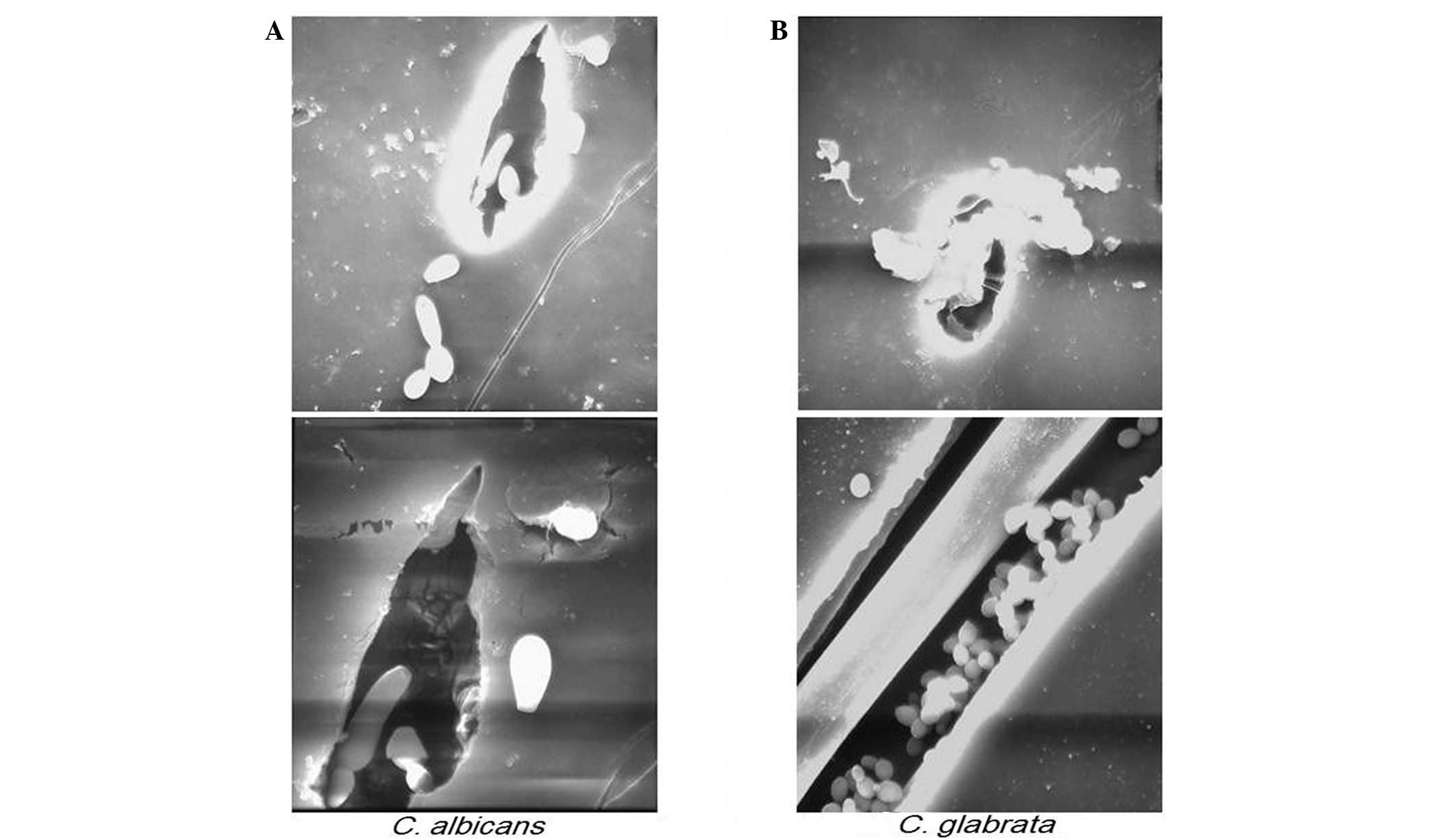
present study. Candida albicans was most frequently observed
as budding yeast, as shown in the cross section of the fissure
(Fig. 3A). In addition, in
incomplete polymerized resin base material, i.e., in places
presenting with the formation of micro-bubbles, Candida
glabrata was detected (Fig.
3B). No other yeasts were identified.
Discussion
The health of elderly individuals may be
compromised, rendering them susceptible to infection, particularly
by intraoral bacteria and general infection may lead to aspiration
pneumonia and respiratory infections (5,6).
Ichikawa et al (20)
investigated the association between oral hygiene and infectious
diseases, such as the association between methicillin-resistant
Staphylococcus aureus (MRSA), Helicobacter pylori and
denture plaque.
Moreover, studies on the number of pharyngeal
bacteria have been conducted in elderly and young populations. The
results of these studies demonstrated that the numbers of Candida
and blue pus bacillus were significantly higher among the elderly
(21). During the early stage of
plaque formation, the rate of adherence increases along with
anaerobic bacteria, mainly Streptococcus. Furthermore, Candida and
Staphylococcus increase proportionately in denture plaques
(22). Therefore, it is
hypothesized that oral hygiene decreases the overall number of
bacteria and in particular Candida, blue pus bacillus and
Staphylococcus, which have a relatively strong pathogenicity
and may be the cause of opportunistic infectious diseases. Plaque
formed by healthy flora is considered important (23–25).
Notably, Kotani et al (26)
reported that the number of Candida is an index that reflects the
level of the condition of oral hygiene.
As demonstrated by our results, although Candida was
detected in all the lesions, its detection rate was 55% in the
samples collected from the inner side of the fitting surface of the
upper denture and 60% in those from the lower denture. As regards
the samples collected from the deep portions of the resin material
of the denture, Candida was detected in 45% of samples from the
upper denture material and in 20% of samples from the lower denture
material. According to previous studies, Candida albicans
strongly adheres to resin, the base material of dentures and forms
a biofilm which then becomes the foundation for denture plaque
formation (27,28). It was hypothesized that the Candida
detected on the inner side of the denture was caused by denture
plaque that adhered to the denture base material. However, in the
case of Candida detected in the deep portions of the denture, this
hypothesis seemed unlikely. Consequently, it was apparent that
Candida existed deep within the resin base material. Therefore, we
conducted Experiment 2 using an electron microscope. Since it is
difficult to examine dentures that are actually being used, Candida
was cultured onto the resin surface of used dentures and the
cultures were used in our investigation.
The presence of all four species of Candida (yeast)
on the resin surface was confirmed through the use of the electron
microscope. However, Candida was not detected in the solid resin.
In the Candida albicans medium, yeast was observed on
incomplete polymerized resin base material, or where micro-bubbles
were present. In addition, the presence of yeast was detected where
the resin was cracked. These results suggest that, although Candida
does not penetrate the resin, Candida invasion may result from the
formation of microbubbles during the making of the denture or
through seams created during repairs, enabling Candida to exist in
the state of yeast. Dentures which have been in use for a long
period of time may have undergone multiple repairs or have
microbubbles in the resin base formed during the making process,
potentially allowing Candida to penetrate and reside deep inside
the resin. Therefore, it seems necessary to re-examine the cleaning
methods used, in order to improve oral hygiene (29).
In addition, all the samples that were observed
under an electron microscope during our study demonstrated a state
of growth without threads. However, there was a previous study on
electron microscopic images showing Candida with fungal threads in
softened dentine and invading deeply into the dental canaliculi
(30). Additional investigations
are required, since there exists a possibility of obtaining
different results from media resembling saliva and interstitial
fluid (31,32).
Acknowledgements
The authors gratefully thank Professor
emeritus Tadamitu Kameyama for excellent experimental advice and
support.
References
|
1
|
Barlow AJ and Chattaway FW: Observations
on the carriage of Candida albicans in man. Br J Dermatol.
81:103–106. 1969.PubMed/NCBI
|
|
2
|
Samaranayake LP: Oral candidosis: an old
disease in new guises. Dent Update. 17:36–38. 1990.PubMed/NCBI
|
|
3
|
Epstein JB: Oral and pharyngeal
candidiasis. Topical agents for management and prevention. Postgrad
Med. 85:257–258. 263–265. 268–269. 1989.PubMed/NCBI
|
|
4
|
Arendorf TM and Walker DM: Oral candidal
populations in health and disease. Br Dent J. 147:267–272. 1979.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Rose HD and Sheth NK: Pulmonary
candidiasis. A clinical and pathological correlation. Arch Intern
Med. 138:964–965. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kikuchi R, Watabe N, Konno T, Mishina N,
Sekizawa K and Sasaki H: High incidence of silent aspiration in
elderly patients with community-acquired pneumonia. Am J Respir
Crit Care Med. 150:251–253. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Yoneyama T, Yoshida M, Matsui T and Sasaki
H: Oral care and pneumonia. Oral Care Working Group. Lancet.
354:5151999. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kurokawa H, Mizuguchi S, Takeda S,
Nakamura T and Takanashi T: Relationship between oral mucosal
lesions and the detection of Candida. Jpn J Oral Diagn/Oral
Med. 15:26–30. 2002.
|
|
9
|
Nakamura C, Koga C, Kuhara S, et al:
Clinical study of miconazole gel for Candida stomatosis of
denture wearing patients. Shikai Tenbou. 97:1117–1123. 2001.
|
|
10
|
Odds FC and Bernaerts R: CHROMagar
Candida, a new differential isolation medium for presumptive
identification of clinically important Candida species. J
Clin Microbiol. 32:1923–1929. 1994.
|
|
11
|
Beighton D, Ludford R, Clark DT, et al:
Use of CHROMagar Candida medium for isolation of yeasts from
dental samples. J Clin Microbiol. 33:3025–3027. 1995.
|
|
12
|
Heelan JS, Sotomayor E, Coon K and
D’Arezzo JB: Comparison of the rapid yeast plus panel with the
API20C yeast system for identification of clinically significant
isolates of Candida species. J Clin Microbiol. 36:1443–1445.
1998.PubMed/NCBI
|
|
13
|
Schuffenecker I, Freydiere A, de Montclos
H and Gille Y: Evaluation of four commercial systems for
identification of medically important yeasts. Eur J Clin Microbiol
Infect Dis. 12:255–260. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Deak R, Bodai L, Aarts HJ and Maraz A:
Development of a novel, simple and rapid molecular identification
system for clinical Candida species. Med Mycol. 42:311–318.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Dealler SF: Candida albicans colony
identification in 5 minutes in a general microbiology laboratory. J
Clin Microbiol. 29:1081–1082. 1991.
|
|
16
|
Crivori P, Morelli A, Pezzetta D,
Rocchetti M and Poggesi I: Development and validation of in silico
models for estimating drug preformulation risk in PEG400/water and
Tween80/water systems. Eur J Pharm Sci. 32:169–181. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Vitkov L, Krautgartner WD, Hannig M,
Weitgasser R and Stoiber W: Candida attachment to oral
epithelium. Oral Microbiol Immunol. 17:60–64. 2002. View Article : Google Scholar
|
|
18
|
Wilborn WH and Montes LF: Scanning
electron microscopy of oral lesions in chronic mucocutaneous
candidiasis. JAMA. 244:2294–2297. 1980. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Radford DR and Radford JR: A SEM study of
denture plaque and oral mucosa of denture-related stomatitis. J
Dent. 21:87–93. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ichikawa T, Terada Y, Hirota K, Miyake Y
and Hoshino K: Study of oral health care and general health of
elderly. Nihon Shika Igakkai Zasshi. 19:75–80. 2000.(In
Japanese).
|
|
21
|
Preston AJ, Gosney MA, Noon S and Martin
MV: Oral flora of elderly patients following acute medical
admission. Gerontology. 45:49–52. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Shinada K, Teraoka K, Asaka T, et al:
Distribution of Candida species and mutans streptococci
related to oral conditions in elderly persons. Kokubyo Gakkai
Zasshi. 64:512–517. 1997.(In Japanese).
|
|
23
|
Thein ZM, Samaranayake YH and Samaranayake
LP: In vitro biofilm formation of Candida albicans and
non-albicans Candida species under dynamic and anaerobic
conditions. Arch Oral Biol. 52:761–767. 2007.PubMed/NCBI
|
|
24
|
Branting C, Sund ML and Linder LE: The
influence of Streptococcus mutans on adhesion of Candida
albicans to acrylic surfaces in vitro. Arch Oral Biol.
34:347–353. 1989.
|
|
25
|
Pereira-Cenci T, Deng DM, Kraneveld EA, et
al: The effect of Streptococcus mutans and Candida
glabrata on Candida albicans biofilms formed on
different surfaces. Arch Oral Biol. 53:755–764. 2008.
|
|
26
|
Kotani H, Sadamori S, Nikawa H and Hamada
T: Clinical survey on denture stomatitis. 1. Relation between
denture plaque and denture stomatitis. Nihon Hotetsu Shika Gakkai
Zasshi. 33:208–214. 1989.(In Japanese).
|
|
27
|
Vasilas A, Molina L, Hoffman M and
Haidaris CG: The influence of morphological variation on Candida
albicans adhesion to denture acrylic in vitro. Arch Oral Biol.
37:613–622. 1992.
|
|
28
|
Thein ZM, Samaranayake YH and Samaranayake
LP: Characteristics of dual species Candida biofilms on
denture acrylic surfaces. Arch Oral Biol. 52:1200–1208. 2007.
|
|
29
|
Samaranayake YH, Cheung BP, Parahitiyawa
N, et al: Synergistic activity of lysozyme and antifungal agents
against Candida albicans biofilms on denture acrylic
surfaces. Arch Oral Biol. 54:115–126. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Sen BH, Safavi KE and Spangberg LS:
Colonization of Candida albicans on cleaned human dental
hard tissues. Arch Oral Biol. 42:513–520. 1997.
|
|
31
|
Nikawa H, Samaranayake LP, Tenovuo J, Pang
KM and Hamada T: The fungicidal effect of human lactoferrin on
Candida albicans and Candida krusei. Arch Oral Biol.
38:1057–1063. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Nikawa H and Hamada T: Binding of salivary
or serum proteins to Candida albicans in vitro. Arch Oral
Biol. 35:571–573. 1990. View Article : Google Scholar : PubMed/NCBI
|