Introduction
Lung cancer is the leading cause of cancer death
worldwide (1), and evidence
indicates that cigarette smoking is the major established risk
factor (2). Additionally, exposure
to environmental-chemical carcinogens are other associated risk
factors (3). The mechanism of lung
tumorigenesis is not fully understood. Epidemiological evidence
indicates that complex interactions between numerous genetic and
environmental factors are significant in the carcinogenesis of lung
carcinoma (4).
The p53 gene is a well-known tumor suppressor
gene that encodes a sequence-specific DNA-binding transcription
factor that targets various genes that govern specific cellular
processes (5). The murine double
minute 2 (MDM2) protein plays an important role in regulating cell
proliferation and apoptosis by transcriptional inhibition via
direct physical binding to p53 and ubiquitination and
proteasome-mediated degradation of p53 via its E3 ubiquitin
ligase activity (6,7). A MDM2 single nucleotide
polymorphism at the 309th nucleotide in the first intron
(rs2279744), with a T to G change, could increase the affinity for
stimulatory protein 1 (Sp1) binding and result in increased MDM2
expression (8) and subsequent
attenuation of the P53 pathway. In humans, the SNP (c.309T>G) in
the MDM2 gene has been correlated with the earlier onset of
tumor formation in hereditary and sporadic cancers (9). A previous meta-analysis reported that
the G/G genotype of c.309T>G was associated with a significantly
increased risk for lung, colorectal, gastric and bladder cancers
and a significantly decreased risk for prostate cancer (10). Molecular epidemiological studies of
c.309T>G and lung cancer susceptibility (11–21)
and survival rate (22–24) have reported disparate findings. It
is noteworthy that there is a large difference among
African-American, Caucasian and Asian populations with respect to
the 309G allele frequency in lung cancer cases (25). The 309G allele is present at a
higher frequency in the Asian population, including Japan, compared
to Caucasians and African-Americans. Significant associations have
been observed for c.309T>G in Japanese squamous cell lung cancer
patients (20). Future studies
analyzing the ethnic group-dependent susceptibility to cancer are
required. Several genome-wide association studies (GWASs) on SNPs
have identified the genomic loci associated with the risk of lung
cancer in Caucasians (26–28), Europeans (29) and Asians (30–34).
However, the associations of the MDM2 polymorphisms were not
investigated in the aforementioned GWASs due to a lack of probes
used to discriminate between the polymorphisms (20).
The aim of the present study was to investigate
whether a functionally important SNP, MDM2 SNP309, was
associated with the risk of lung cancer in a Japanese population.
The genomic DNA was examined from blood samples for c.309T>G
using the Smart Amplification Process (SmartAmp), which is a rapid,
sensitive and simple mutation-detection assay that has been
described previously (35,36). Subsequently, the association between
c.309T>G and the lung cancer risk was examined. To the best of
our knowledge, this is the first study to investigate the role of
c.309T>G in the MDM2 gene in all the types of lung cancer
in a Japanese population.
Materials and methods
Subjects
The study included 762 patients with lung cancer and
700 cancer-free controls. All the cases were histologically
confirmed primary lung cancer patients who were diagnosed and
recruited between January 2003 and June 2013 at Gunma University
Hospital, Maebashi Red Cross Hospital and National Nishi-Gunma
Hospital (Gunma, Japan). The control group consisted of hospital
and population controls. The hospital controls were recruited from
the same hospital as the patients. The population controls were
recruited from a health survey for the evaluation of metabolic
syndrome in Gunma. The potential controls that had a previous
diagnosis of malignancy were excluded from the study. The protocols
for sample collection, sample anonymity, storage and genomic DNA
analysis were approved by the Institutional Review Board for the
Ethics Committee for Human Genome Analysis at each hospital.
Written informed consent from all the participants was obtained.
The clinical study was conducted according to the Declaration of
Helsinki Principles.
Patient demographics
The demographics, cancer history and smoking history
of the subjects were documented using a structured chart review.
The patients were categorized based on the smoking status. The
cumulative cigarette dose [pack-years (PY)] was calculated using
the following formula: PY = packs per day × years smoked.
Never-smokers were defined as individuals with PY=0, mild smokers
were PY<50 and heavy smokers were PY≥50.
Genotyping for polymorphisms and gene
mutation analysis
Peripheral venous blood samples were collected and
DNA was extracted using a DNeasy Blood and Tissue kit (Qiagen,
Hilden, Germany) according to the manufacturer’s instructions.
Genotyping of c.309T>G in the MDM2 gene was performed by
the Duplex SmartAmp method as described previously (36) with an Mx3000P PCR system (Agilent
Technologies, Santa Clara, CA, USA). The lung cancer tissues were
immediately frozen following surgical removal and stored at −80°C
until DNA extraction using a Wizard Genomic DNA purification kit
(Promega Corporation, Madison, WI, USA). The epidermal growth
factor receptor (EGFR) mutations were analyzed by peptide
nucleic acid-enriched sequencing, as described previously (37).
Statistical analyses
The demographic and clinical information were
compared across genotypes and cancer stages using Pearson’s
χ2 tests (for categorical variables) and Kruskal-Wallis
tests (for continuous variables) where appropriate. The strengths
of the associations between the genotypes and risk were measured as
odds ratios (ORs) adjusted for gender, age and PY of smoking with
95% confidence intervals (CIs) by unconditional logistic regression
analysis. All the statistical analyses were conducted at the
two-sided P=0.05 level and SPSS Statistics version 20 (SPSS, Inc.,
Chicago, IL, USA) was used. P<0.05 was considered to indicate a
statistically significant difference.
Results
Demographics
A total of 762 primary lung cancer patients and 700
controls were included in the analysis and Table I shows the associated demographics.
Compared to the controls, the patients were older with a higher
proportion of males. The mean PY value was higher in the cases
compared to the controls (Table I).
Complete matching was not achieved for gender, age and smoking
history. Therefore, these factors were adjusted in the logistic
model. The frequency of c.309T>G did not differ between the
hospital and population controls (P=0.74; data not shown).
Therefore, the controls were treated as a single group. The
distributions of c.309T>G (T/T, T/G, G/G) were 20.1, 49.7, 30.2%
in the patient group and 21.7, 47.9, 30.4% in the healthy-control
group. There were no significant differences in the c.309T>G
genotypes between cases and controls. The allele frequencies of the
G allele in the case and control groups were 0.551 and 0.544,
respectively.
 | Table ICharacteristics of lung cancer cases
and healthy controls. |
Table I
Characteristics of lung cancer cases
and healthy controls.
| Cases (n=762) | Controls
(n=700) | |
|---|
|
|
| |
|---|
| Variable | n (%) | n (%) | P-value |
|---|
| Gender | | | <0.001a |
| Male | 472 (61.9) | 326 (46.6) | |
| Female | 290 (38.1) | 374 (53.4) | |
| Age, years | | | <0.001b |
| Mean ± SD | 68.4±9.8 | 64.1±12.7 | |
| Range | 31–95 | 20–93 | |
| MDM2
polymorphism | | | 0.69a |
| T/T | 153 (20.1) | 152 (21.7) | |
| T/G | 379 (49.7) | 335 (47.9) | |
| G/G | 230 (30.2) | 213 (30.4) | |
| G allele
frequency | 0.551 | 0.544 | |
| PY |
| Mean ± SD | 36.4±37.2 | 26.6±32.7 | 0.001b |
| Range | 0–265 | 0–184 | |
| Histology |
| AD | 487 (63.9) | | |
| SQ | 182 (23.9) | | |
| Others | 82 (10.8) | | |
|
Un-differentiated | 11 (1.4) | | |
MDM2 and lung cancer risk
There was no overall association between c.309T>G
and the risk of lung cancer (Table
II). The adjusted OR for developing lung cancer was 1.18 (95%
CI, 0.76–1.80) for the G/G, compared to the T/T. The data was
further stratified by gender, cancer histology,
EGFR-mutation status of adenocarcinoma (AD) and
smoking-status subgroups. There were no associations among any
subgroup (Table II).
| Table IIGenotype frequencies of the
MDM2 309T>G polymorphism among controls and cases and
their association with lung cancer risk. |
Table II
Genotype frequencies of the
MDM2 309T>G polymorphism among controls and cases and
their association with lung cancer risk.
| | | | Adjusted OR (95%
CI)a |
|---|
| | | |
|
|---|
| Variable | No. | T/T (%) | T/G (%) | G/G (%) | T/T vs. G/G | T/T vs.
T/G+G/G | T/T+T/G vs.
G/G |
|---|
| Control | 700 | 152 (21.7) | 335 (47.9) | 213 (30.4) | 1.00
(Reference) | 1.00
(Reference) | 1.00
(Reference) |
| Case | 762 | 153 (20.1) | 379 (49.7) | 230 (30.2) | 1.18
(0.76–1.80) | 1.25
(0.87–1.81) | 0.98
(0.71–1.37) |
| Femaleb | 290 | 53 (18.3) | 143 (49.3) | 94 (32.4) | 1.31
(0.91–1.87) | 1.51
(0.83–2.75) | 1.34
(0.76–2.34) |
| Maleb | 472 | 100 (21.2) | 236 (50.0) | 136 (28.8) | 0.94
(0.55–1.60) | 1.13
(0.72–1.79) | 0.83
(0.55–1.24) |
| AD | 487 | 101 (20.7) | 233 (47.8) | 153 (31.4) | 1.05
(0.84–1.31) | 1.14
(0.77–1.67) | 1.02
(0.72–1.44) |
| SQ | 182 | 35 (19.2) | 98 (53.8) | 49 (26.9) | 1.06
(0.77–1.46) | 1.42
(0.80–2.49) | 0.87
(0.52–1.43) |
|
EGFR-WT-AD | 207 | 41 (19.8) | 102 (49.3) | 64 (30.9) | 1.09
(0.83–1.42) | 1.28
(0.80–2.05) | 1.01
(0.67–1.52) |
|
EGFR-Mt-AD | 175 | 39 (22.3) | 78 (44.6) | 58 (33.1) | 1.00
(0.75–1.35) | 0.97
(0.58–1.61) | 1.04
(0.66–1.64) |
| Never-smoker | 251 | 43 (17.1) | 129 (51.4) | 79 (31.5) | 1.07
(0.75–1.55) | 1.46
(0.78–2.73) | 0.89
(0.52–1.54) |
| Light smoker | 258 | 49 (19.0) | 127 (49.2) | 82 (31.8) | 1.09
(0.85–1.41) | 1.30
(0.83–2.03) | 1.00
(0.68–1.49) |
| Heavy smoker | 246 | 57 (23.2) | 120 (48.8) | 69 (28.0) | 1.00
(0.71–1.41) | 1.07
(0.60–1.92) | 0.95
(0.55–1.64) |
MDM2 and cigarette smoking
As smoking is a stressor and an established cause of
lung cancer, we evaluated whether an interaction existed between
the MDM2 polymorphism and smoking among lung cancer
patients. No significant associations were observed between the
various c.309T>G genotypes and cumulative smoking. (Table III). However, the G/G genotype
tended to be associated with a lower level of exposure to cigarette
smoke compared to the other genotype (P=0.07) among squamous cell
carcinoma (SQ) patients (Table
III).
| Table IIIComparison by cumulative smoking. |
Table III
Comparison by cumulative smoking.
| | T/T | T/G | G/G | |
|---|
| |
|
|
| |
|---|
| Variable | n | Mean ± SD | Mean ± SD | Mean ± SD | P-valuea (T/T+T/G vs. G/G) |
|---|
| Total | 755 | 39.9±36.5 | 36.5±38.7 | 34.1±35.0 | 0.35 |
| Female | 286 | 8.2±18.7 | 8.2±18.6 | 7.6±18.4 | 0.88 |
| Male | 469 | 55.9±32.6 | 53.6±37.6 | 52.5±31.9 | 0.70 |
| AD | 482 | 26.3±30.1 | 20.6±28.8 | 23.1±31.4 | 0.99 |
| SQ | 182 | 70.8±33.9 | 62.0±32.9 | 57.2±34.5 | 0.07 |
| SCLC | 52 | 58.8±34.9 | 67.5±56.7 | 59.2±24.8 | 0.93 |
MDM2 and age at diagnosis
The association between age at diagnosis and
c.309T>G in all the lung cancer patients was examined, as well
as in the gender, histological-subtype and smoking-status
subgroups. Kruskal-Wallis analysis indicated no association between
the various c.309T>G genotypes and age at onset in the study
population (Table IV).
| Table IVComparison by age at diagnosis. |
Table IV
Comparison by age at diagnosis.
| | T/T | T/G | G/G | |
|---|
| |
|
|
| |
|---|
| Variable | n | Mean ± SD | Mean ± SD | Mean ± SD | P-valuea (T/T+T/G vs. G/G) |
|---|
| Total | 761 | 67.4±9.6 | 68.9±9.7 | 68.2±10.0 | 0.54 |
| Female | 289 | 66.3±9.7 | 67.2±10.2 | 66.7±10.4 | 0.82 |
| Male | 472 | 68.0±9.6 | 69.9±9.3 | 69.2±9.5 | 0.69 |
| AD | 487 | 66.7±10.3 | 67.2±10.3 | 66.9±10.2 | 0.67 |
| SQ | 182 | 71.0±6.3 | 72.8±7.9 | 72.0±9.1 | 0.86 |
| SCLC | 52 | 64.9±9.9 | 69.3±7.8 | 70.8±8.9 | 0.27 |
| Smoker | 507 | 68.3±9.5 | 69.7±9.7 | 69.0±10.0 | 0.60 |
| Never smoker | 251 | 65.6±9.8 | 67.4±9.6 | 66.7±9.9 | 0.82 |
Discussion
In the present molecular epidemiological study, the
association of the genetic polymorphisms in MDM2 with the
risk of developing lung cancer in a Japanese population was
examined. The results obtained by analyzing 762 lung cancer
patients and 700 controls demonstrated that c.309T>G in the
MDM2 gene is not associated with lung cancer risk.
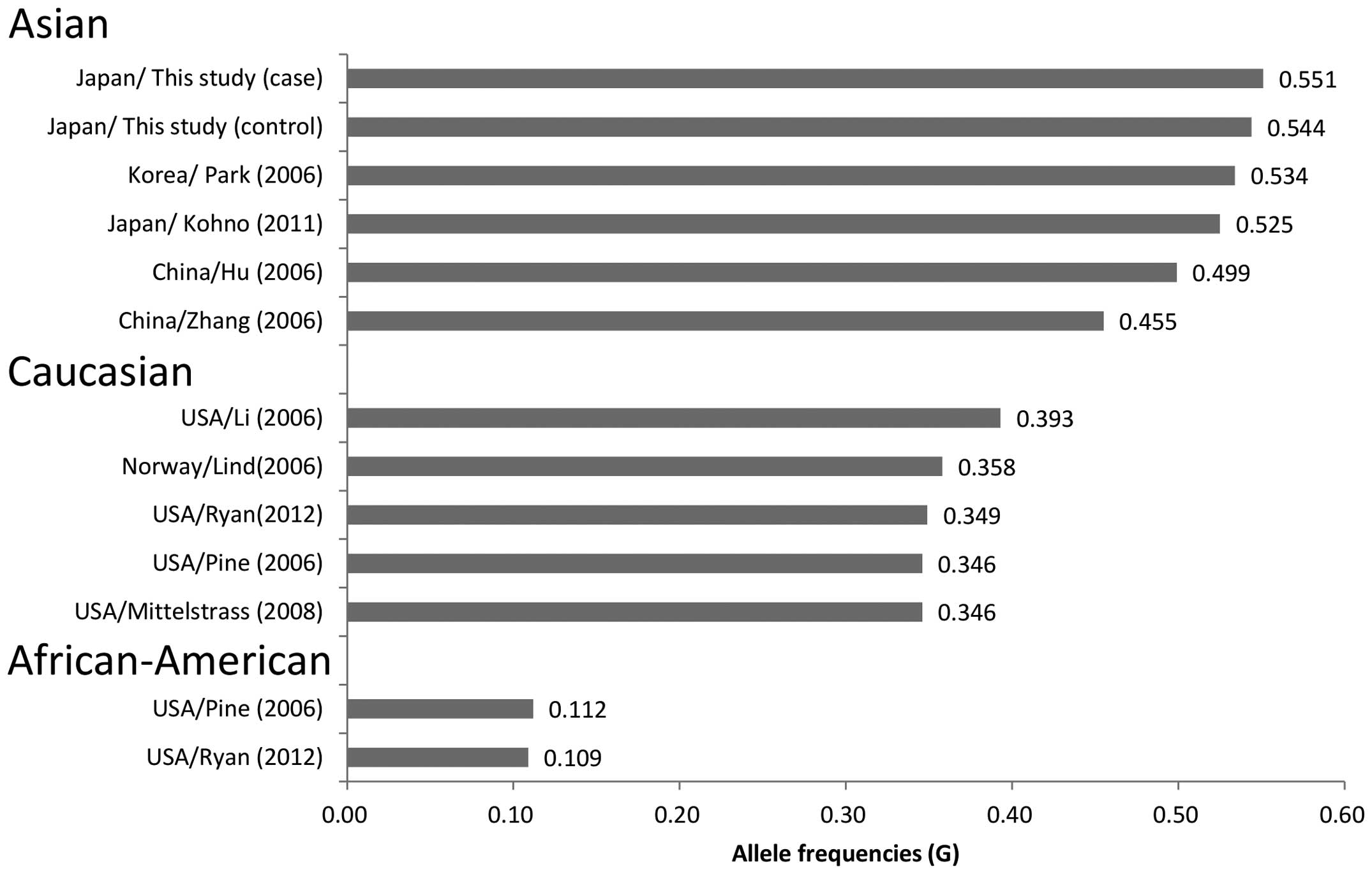
In the study, the frequency of the MDM2 309G
alleles among the controls was 0.544, which is almost identical to
the frequency observed in the Japanese (0.525) (20), Han Chinese of southeast China
(0.499) (14) and Korean (0.534)
(16) populations; but is
significantly higher compared to the Han Chinese of northeast China
(0.455) (15), Caucasian
(0.346–0.393) (11–13,18,38)
and African-American (0.109–0.112) (13,38)
populations (Fig. 1). There are
conflicting studies regarding the contribution of c.309T>G to
the lung cancer risk (11–19,21).
The differences in the allele frequencies among ethnic groups may
have contributed to the disparities among the previous studies.
Certain studies have linked the G allele with the
lung cancer risk among Caucasians (11) and Asians (15). Conversely, only one study linked the
309T allele with the risk in Caucasians, notably in SQ patients and
in males (12). The data of the
present study suggests that c.309T>G is not associated with the
lung cancer risk among the total population, which is in line with
numerous epidemiological studies conducted in Caucasians (13,17,18),
African-Americans (13) and Asians
(14,16,20). A
previous meta-analysis study (39)
concluded that the association between c.309T>G and lung cancer
was statistically significant in Asians, females and never-smokers,
but not in Caucasians, males, ever-smokers or among any of the
individual histological types.
Stratification by gender, histological subtype and
smoking status revealed no association between c.309T>G and lung
cancer susceptibility. Lind et al (11) reported a gender-specific
risk-disposing effect of the 309T allele of MDM2 SNP309 for
non-small cell lung cancer (NSCLC) patients. NSCLC patients were
investigated and it was found that female carriers of G/G had an OR
for lung cancer of 4.1, whereas male homozygotes had a
non-significant OR of 1.3. The data of the present study showed
corresponding ORs for females and males of 1.31 and 0.94,
respectively, which tended to confirm this finding, although the
ORs were much smaller and not significant. Bond et al
(40) showed that the effect of the
MDM2 G/G genotype was gender-specific and was increased in
females with active estrogen-signaling pathways, which may explain
the findings of the present study.
In terms of histological subtypes, Park et al
(16) and Ren et al
(21) reported that the T/T
genotype was associated with a decreased risk of AD. However, the
present study findings, as well as those of others (18,41),
did not show an interaction between c.309T>G and the
histological subtype.
Cigarette smoking may induce DNA damage, initiating
and promoting carcinogenesis, and is a major risk factor for NSCLC.
Park et al (16) and Zhang
et al (15) reported that
the T/T genotype was associated with a decreased risk among
ever-smokers and ever- and never-smokers, respectively. However,
the present study, as well as others (18,41),
did not show an interaction between c.309T>G in the MDM2
gene and smoking status. A tendency towards a lower level of
exposure to cigarette smoking was observed among the G/G SQ
patients compared with T allele carriers (T/T+T/G), but the
difference was not statistically significant. However, no
significant association between c.309T>G and the lung cancer
risk among smokers or SQ patients was observed. Therefore, it was
concluded that SNP309 did not contribute to smoking-related
tumors.
c.309T>G was reported to be associated with an
earlier onset of disease for Li-Fraumeni syndrome and sporadic
sarcoma (8). The present study did
not observe a lower age of diagnosis, and similar findings were
described in previous studies (13,14,18).
Although the reason for the differences in
MDM2 polymorphisms among different studies is unclear, it
may be due to differences in subjects, genetic backgrounds and/or
environmental factors (42) among
various populations. As an example of population heterogeneity, an
interaction of c.309T>G with c.285G>C in the MDM2 gene
was questionable (43), as it has
been previously reported to act as an antagonist by overriding the
effect of c.309T>G on Sp1-mediated transcription. However, the
study by Ryan et al (38)
recently reported that c.285G>C did not antagonize the effect of
c.309T>G in lung cancer. Furthermore, the differences in
frequencies of driver mutations, such as EGFR mutations
(44), may contribute to the
different effects of c.309T>G in various ethnic groups.
EGFR mutations are predominantly found in
female, non-smoking AD patients and in patients of East Asian
origin (45). A recent
meta-analysis study (39) reported
that the association between c.309T>G and lung cancer was
statistically significant, particularly in the Asian population,
female and never-smokers. No statistically significant association
was observed in males or ever-smokers. The AD patients were
stratified according to EGFR-mutation status, however, no
association was observed. To the best of our knowledge, there have
been no report in terms of analyzing the association between
c.309T>G in the MDM2 gene and lung cancer susceptibility
based on EGFR mutation status.
The limitations of the study include the
retrospective nature, and the patient populations may be biased.
Furthermore, the study was a hospital- and community-based
case-control study, which could not rule out possible selection
bias. However, by matching age, gender and PY of smoking, the
potential confounding effects should have been reduced. To further
elucidate the impact of c.309T>G on lung cancer susceptibility,
future investigations of large ethnically-diverse population-based
studies are warranted.
In conclusion, the present study is the first to
evaluate the overall lung cancer risk and c.309T>G in a Japanese
population. Considering the contradictory results across multiple
studies, conclusions from any single study must be interpreted with
caution. The results of the present study should be confirmed by
other prospective studies.
Acknowledgements
The present study was supported by Grant-in-Aid for
Scientific Research (C) (grant no. 22590516) from the Japan Society
for the Promotion of Science. The study was partially supported by
i) research grants for the RIKEN Omics Science Center from the
Japanese Ministry of Education, Culture, Sports, Science and
Technology (MEXT) to Y.H.; and ii) a research grant from the MEXT
to the RIKEN Center for Life Science Technologies. The funders had
no role in the study design, data collection and analysis, decision
to publish or preparation of the manuscript.
Abbreviations:
|
SNP
|
single-nucleotide polymorphism
|
|
OR
|
odds ratio
|
|
CI
|
confidence interval
|
|
PY
|
pack-year
|
|
AD
|
adenocarcinoma
|
|
SQ
|
squamous cell carcinoma
|
|
NSCLC
|
non-small cell lung cancer
|
References
|
1
|
Jemal A, Bray F, Center MM, Ferlay J, Ward
E and Forman D: Global cancer statistics. CA Cancer J Clin.
61:69–90. 2011. View Article : Google Scholar
|
|
2
|
Steliga MA and Dresler CM: Epidemiology of
lung cancer: smoking, secondhand smoke, and genetics. Surg Oncol
Clin N Am. 20:605–618. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Fucic A, Gamulin M, Ferencic Z, et al:
Lung cancer and environmental chemical exposure: a review of our
current state of knowledge with reference to the role of hormones
and hormone receptors as an increased risk factor for developing
lung cancer in man. Toxicol Pathol. 38:849–855. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yokota J, Shiraishi K and Kohno T: Genetic
basis for susceptibility to lung cancer: Recent progress and future
directions. Adv Cancer Res. 109:51–72. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Jin S and Levine AJ: The p53 functional
circuit. J Cell Sci. 114:4139–4140. 2001.PubMed/NCBI
|
|
6
|
Momand J, Zambetti GP, Olson DC, George D
and Levine AJ: The mdm-2 oncogene product forms a complex with the
p53 protein and inhibits p53-mediated transactivation. Cell.
69:1237–1245. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Thut CJ, Goodrich JA and Tjian R:
Repression of p53-mediated transcription by MDM2: a dual mechanism.
Genes Dev. 11:1974–1986. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Bond GL, Hu W, Bond EE, et al: A single
nucleotide polymorphism in the MDM2 promoter attenuates the p53
tumor suppressor pathway and accelerates tumor formation in humans.
Cell. 119:591–602. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Bond GL, Hu W and Levine A: A single
nucleotide polymorphism in the MDM2 gene: from a molecular and
cellular explanation to clinical effect. Cancer Res. 65:5481–5484.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Wo X, Han D, Sun H, et al: MDM2 SNP309
contributes to tumor susceptibility: a meta-analysis. J Genet
Genomics. 38:341–350. 2011.PubMed/NCBI
|
|
11
|
Lind H, Zienolddiny S, Ekstrøm PO, Skaug V
and Haugen A: Association of a functional polymorphism in the
promoter of the MDM2 gene with risk of nonsmall cell lung cancer.
Int J Cancer. 119:718–721. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Li G, Zhai X, Zhang Z, Chamberlain RM,
Spitz MR and Wei Q: MDM2 gene promoter polymorphisms and risk of
lung cancer: a case-control analysis. Carcinogenesis. 27:2028–2033.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Pine SR, Mechanic LE, Bowman ED, et al:
MDM2 SNP309 and SNP354 are not associated with lung cancer risk.
Cancer Epidemiol Biomarkers Prev. 15:1559–1561. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Hu Z, Ma H, Lu D, et al: Genetic variants
in the MDM2 promoter and lung cancer risk in a Chinese population.
Int J Cancer. 118:1275–1278. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Zhang X, Miao X, Guo Y, et al: Genetic
polymorphisms in cell cycle regulatory genes MDM2 and TP53 are
associated with susceptibility to lung cancer. Hum Mutat.
27:110–117. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Park SH, Choi JE, Kim EJ, et al: MDM2
309T>G polymorphism and risk of lung cancer in a Korean
population. Lung Cancer. 54:19–24. 2006.
|
|
17
|
Liu G, Wheatley-Price P, Zhou W, et al:
Genetic polymorphisms of MDM2, cumulative cigarette smoking and
nonsmall cell lung cancer risk. Int J Cancer. 122:915–918. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Mittelstrass K, Sauter W, Rosenberger A,
et al: Early onset lung cancer, cigarette smoking and the SNP309 of
the murine double minute-2 (MDM2) gene. BMC Cancer. 8:1132008.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Chua HW, Ng D, Choo S, et al: Effect of
MDM2 SNP309 and p53 codon 72 polymorphisms on lung cancer risk and
survival among non-smoking Chinese women in Singapore. BMC Cancer.
10:882010. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kohno T, Kunitoh H, Mimaki S, et al:
Contribution of the TP53, OGG1, CHRNA3, and HLA-DQA1 genes to the
risk for lung squamous cell carcinoma. J Thorac Oncol. 6:813–817.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ren YW, Yin ZH, Wan Y, et al: P53 Arg72Pro
and MDM2 SNP309 polymorphisms cooperate to increase lung
adenocarcinoma risk in Chinese female non-smokers: a case control
study. Asian Pac J Cancer Prev. 14:5415–5420. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Heist RS, Zhou W, Chirieac LR, et al: MDM2
polymorphism, survival, and histology in early-stage non-small-cell
lung cancer. J Clin Oncol. 25:2243–2247. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Han JY, Lee GK, Jang DH, Lee SY and Lee
JS: Association of p53 codon 72 polymorphism and MDM2 SNP309 with
clinical outcome of advanced nonsmall cell lung cancer. Cancer.
113:799–807. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Dong J, Ren B, Hu Z, et al: MDM2 SNP309
contributes to non-small cell lung cancer survival in Chinese. Mol
Carcinog. 50:433–438. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Zhuo W, Zhang L, Zhu B, Ling J and Chen Z:
Association of MDM2 SNP309 variation with lung cancer risk:
evidence from 7196 cases and 8456 controls. PLoS One. 7:e415462012.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Landi MT, Chatterjee N, Yu K, et al: A
genome-wide association study of lung cancer identifies a region of
chromosome 5p15 associated with risk for adenocarcinoma. Am J Hum
Genet. 85:679–691. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Hung RJ, McKay JD, Gaborieau V, et al: A
susceptibility locus for lung cancer maps to nicotinic
acetylcholine receptor subunit genes on 15q25. Nature. 452:633–637.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Wang Y, Broderick P, Webb E, et al: Common
5p15.33 and 6p21.33 variants influence lung cancer risk. Nat Genet.
40:1407–1409. 2008. View
Article : Google Scholar
|
|
29
|
Shi J, Chatterjee N, Rotunno M, et al:
Inherited variation at chromosome 12p13.33, including RAD52,
influences the risk of squamous cell lung carcinoma. Cancer Discov.
2:131–139. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Hosgood HD III, Wang WC, Hong YC, et al:
Genetic variant in TP63 on locus 3q28 is associated with risk of
lung adenocarcinoma among never-smoking females in Asia. Hum Genet.
131:1197–1203. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Ahn MJ, Won HH, Lee J, et al: The 18p11.22
locus is associated with never smoker non-small cell lung cancer
susceptibility in Korean populations. Hum Genet. 131:365–372. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Hu Z, Wu C, Shi Y, et al: A genome-wide
association study identifies two new lung cancer susceptibility
loci at 13q12.12 and 22q12.2 in Han Chinese. Nat Genet. 43:792–796.
2011. View
Article : Google Scholar : PubMed/NCBI
|
|
33
|
Shiraishi K, Kunitoh H, Daigo Y, et al: A
genome-wide association study identifies two new susceptibility
loci for lung adenocarcinoma in the Japanese population. Nat Genet.
44:900–903. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Lan Q, Hsiung CA, Matsuo K, et al:
Genome-wide association analysis identifies new lung cancer
susceptibility loci in never-smoking women in Asia. Nat Genet.
44:1330–1335. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Mitani Y, Lezhava A, Kawai Y, et al: Rapid
SNP diagnostics using asymmetric isothermal amplification and a new
mismatch-suppression technology. Nat Methods. 4:257–262. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Enokida Y, Shimizu K, Atsumi J, et al:
Rapid detection of SNP (c.309T>G) in the MDM2 gene by the Duplex
SmartAmp method. PLoS One. 8:e601512013. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Miyamae Y, Shimizu K, Mitani Y, et al:
Mutation detection of epidermal growth factor receptor and KRAS
genes using the smart amplification process version 2 from
formalin-fixed, paraffin-embedded lung cancer tissue. J Mol Diagn.
12:257–264. 2010. View Article : Google Scholar
|
|
38
|
Ryan BM, Calhoun KM, Pine SR, et al: MDM2
SNP285 does not antagonize the effect of SNP309 in lung cancer. Int
J Cancer. 131:2710–2716. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
He W, Long J, Xian L, et al: MDM2 SNP309
polymorphism is associated with lung cancer risk in women: A
meta-analysis using METAGEN. Exp Ther Med. 4:569–576.
2012.PubMed/NCBI
|
|
40
|
Bond GL, Hirshfield KM, Kirchhoff T, et
al: MDM2 SNP309 accelerates tumor formation in a gender-specific
and hormone-dependent manner. Cancer Res. 66:5104–5110. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Liu JN, Zhang XM, Guo YL, Sun T, Lin DX
and Wen T: Genetic polymorphism in MDM2 is associated with
susceptibility to colorectal cancer in a Chinese population.
Zhonghua Zhong Liu Za Zhi. 30:335–338. 2008.(In Chinese).
|
|
42
|
Alberg AJ, Ford JG and Samet JM; American
College of Chest Physicians. Epidemiology of lung cancer: ACCP
evidence-based clinical practice guidelines (2nd edition). Chest.
132(Suppl 3): 29S–55S. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Knappskog S, Bjørnslett M, Myklebust LM,
et al: The MDM2 promoter SNP285C/309G haplotype diminishes Sp1
transcription factor binding and reduces risk for breast and
ovarian cancer in Caucasians. Cancer Cell. 19:273–282. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Nana-Sinkam SP and Powell CA: Molecular
biology of lung cancer: diagnosis and management of lung cancer,
3rd ed: American College of Chest Physicians evidence-based
clinical practice guidelines. Chest. 143(5 Suppl): e30S–e39S. 2013.
View Article : Google Scholar
|
|
45
|
Mitsudomi T and Yatabe Y: Mutations of the
epidermal growth factor receptor gene and related genes as
determinants of epidermal growth factor receptor tyrosine kinase
inhibitors sensitivity in lung cancer. Cancer Sci. 98:1817–1824.
2007. View Article : Google Scholar : PubMed/NCBI
|